101 Meaningful Post Sixteen Special Education Activities for
Individuals Experiencing Profound and Multiple Learning Difficulties (IEPMLD)
 Sensory AstroPhysics Session
Sensory AstroPhysics Session
This page is dedicated to detailing a range of meaningful activities for young people experiencing Profound and Multiple Learning Difficulties in a post-school setting. While it is not claimed that every activity on this page will be suitable for all individuals, it is hoped that some may be tailored to the needs of someone in your care. Furthermore, while aiming to be comprehensive, it is not claimed that this page represents a full listings of all the meaningful activities possible for such a group of young people.
"Sensory cooking, sensory drama, sensory art, sensory garden, sensory room …. What does the word “sensory” written before the activity or place imply?" (Williams, 2010, page 23)
Not all activities are suitable for inclusion in any post-school curriculum on offer for Individuals Experiencing Profound and Multiple Learning Difficulties (hereafter the acronym IEPMLD will be used). As the cartoon suggests, simply placing the word 'sensory' in front of any activity does not, in and of itself, make it an appropriate curricula area; Sensory Russian (assuming the Learners are not Russian), Sensory Neurology, Sensory Welding, etc. are such examples. What then is appropriate and what right have others to decide what is or is not correct in this area of education? This page will attempt to address such issues.
Given that post school education for this group of young people is likely to be both short (one to three years) and expensive (running into tens of thousands of pounds), time should not be wasted on meaningless activities. The focus must be on things that will benefit individual future lives, enhance quality, and ensure a best transition route into a new adult world. This has been recognised for many years:
"Given the key characteristics of the students, what do they need to learn? In order to carry out this exercise successfully, you need to have a clear picture of what their lives are like now, and what they will be like in the future. What are the priorities? Remember that, although the students may have numerous gaps in their learning, you will only have them for two or three years. What are the things which will really
make a difference, even if they do not progress in the others?" (Griffiths & Tennyson, 1997, page 4)
Although specifically addressing schools, Richard Aird said the following in 2001:
"A pupil's school life is a brief affair, and the time in the classroom is a precious time that ought to be dedicated to minimising the handicapping affects of a pupil's disability and enabling the pupil to achieve maximum potential in a broad but relevant curriculum that is unique to the SLD sector and does not smack of the tokenism that has marred the history of the implementation of the National Curriculum in the SLD sector thus far." (Aird, 2001, page 14)
If school life is but a 'brief affair' then how many more constraints are placed on staff and student alike by an even shorter period of study in a post-school provision? Therefore, one might reasonably argue that there is an even greater need for this 'precious time' to have a specific focus as aptly indicated by Aird. Should this focus be different and distinct to that provided by an individual's school experience or should it be an allowance of further time (in some form of school extension) for Learners who, by definition, acquire knowledge at a very different rate to that of their peers?
What do IEPMLD at this time in their lives really need to learn? Do they really need to be continuing placing their hands in mixtures of ingredients (for example) in some form of sensory cookery session as they have presumably been doing throughout their school career? How is this assisting a better quality of life in the future? There may well be a really good rationale for so doing. However, it must be made explicit and all staff (inclusive of the supporting team) must be made aware of this rationale. Indeed, one might ask if IEPMLD are ever likely to be cooking for themselves at all? In which case, why is cookery a part of your curriculum? It might be argued that 'cooking for leisure' is something that an IEPMLD might enjoy and thus choose to do for fun. This might be an acceptable rationale for the provision of this area on the curriculum but should it be compulsory for all Learners? Perhaps Learners should be permitted to choose what they wish to undertake acting as agents making decisions about their own future. Can IEPMLD act as agents? If this is believed not to be the case, does it not follow that one possible curriculum option would be the empowerment of young people through the development of 'agentive' awareness and skills? How can one choose if you do not know how to choose? How can you learn how to choose if you are never given choice? If you are never given choice how can you be an agent?
"One of the reasons that students with disabilities have not succeeded once they leave school is that the educational process has not prepared students with special learning needs adequately to become self-determined young people."
(Wehmeyer & Schalock, 2001, page 2)
For activities to be appropriate for Individuals Experiencing PMLD at F.E. level they must fulfill most of the following criteria. They must show how they:
• are age appropriate within the confines of the ‘preference not deference’ rule;
• are delivered in a manner that is commensurate with the Learner’s cognitive ability;
• engage each Learner such that the Learner is active and not passive;
• empower the Learner through improvements in capability/coordination or through the use of available technology;
• empower the Learner through improvements in cognition and communication;
• relate to the possible future experiences and opportunities of the Learner;
• expand possible future experiences and opportunities for the Learner;
• enhance the Learner’s future Quality Of Life;
• are realistic but not pessimistic (self-fulfilling prophecy).
Thus, this page concerns itself with pragmatic and meaningful ideas for use in a post school environment for IEPMLD. You may not agree with all that is suggested but, hopefully, there will be some sections that you will find inspirational. We should look to new possibilities and better futures for this population and not impose unnecesary barriers and limitations and simply because their given 'label' has previously suggested them:
"the existence of learning difficulties so extreme as to present a major obstacle to participation in some of the most basic experiences in life, ought rather to generate educational aims concerned with enabling them to participate in those experiences. An aim which we might express as: 'enabling the child to participate in those experiences which are uniquely human'." (Ware, 1994, page 71)
"It should also become evident that people that may seem to be 'cognitively limited' nevertheless have a great deal of cognitive competence. You will see that without this competence simple things like pointing or eye gaze in a way that is appropriate to the context would not be possible. Such seemingly simple behaviours are still beyond the capabilities of very sophisticated computer simulations and could not occur without considerable knowledge of the world and how to solve problems in that world. (Anderson J. 1990). Hopefully, you will see that even 'cognitively limited' individuals are capable of more than most people think they are (Bray N. & Turner L. 1986, 1987). Facilitators can build on this cognitive base." (Bray N. 1990)
Furthermore, Learners may be better served if the greater part of continuing study had a focus on future activity rather on the development of isolated skills:
"Focusing on activities requires teachers therefore to move from a developmental, skill-based approach, to an ‘activity-based’ intervention approach that considers participation in activities in meaningful contexts as a basis for analysis of educational progress." (Magne Tellevik & Elmerskog, 2009)
"One critical feature of a ‘good’ assessment for this group is that it contributes to improving the individual’s quality of life, by helping teachers
to prioritise learning" (Ware & Donnelly, 2004, page 12).
If the reader feels that aspects of this page are inappropriate or ill-advised or wishes to suggest other areas of development, a contact form is provided at the bottom of the page. Please fell free to use it to contact TalkSense. If any such comment or idea is used on this page then appropriate acknowledgement and credit will be given.
Please Note: This page may be updated from time to time. TalkSense reserves the right to add to, amend or abrogate any section of this page at any time. Should the page change significantly TalkSense will update the 'date counter' such that readers will be alerted. This page was last updated on:
September 28th, 2018
This Page is currently in development. Talksense hopes to have it complete sometime soon. The page will change significantly over time. However you got here, while you are free to browse, please note that some sections are presently missing or incomplete, may alter considerably, and the number order may change. Constructive comments are welcome! (Use form provided at end of page before bibliography)
"Sensory cooking, sensory drama, sensory art, sensory garden, sensory room …. What does the word “sensory” written before the activity or place imply?" (Williams, 2010, page 23)
Not all activities are suitable for inclusion in any post-school curriculum on offer for Individuals Experiencing Profound and Multiple Learning Difficulties (hereafter the acronym IEPMLD will be used). As the cartoon suggests, simply placing the word 'sensory' in front of any activity does not, in and of itself, make it an appropriate curricula area; Sensory Russian (assuming the Learners are not Russian), Sensory Neurology, Sensory Welding, etc. are such examples. What then is appropriate and what right have others to decide what is or is not correct in this area of education? This page will attempt to address such issues.
Given that post school education for this group of young people is likely to be both short (one to three years) and expensive (running into tens of thousands of pounds), time should not be wasted on meaningless activities. The focus must be on things that will benefit individual future lives, enhance quality, and ensure a best transition route into a new adult world. This has been recognised for many years:
"Given the key characteristics of the students, what do they need to learn? In order to carry out this exercise successfully, you need to have a clear picture of what their lives are like now, and what they will be like in the future. What are the priorities? Remember that, although the students may have numerous gaps in their learning, you will only have them for two or three years. What are the things which will really
make a difference, even if they do not progress in the others?" (Griffiths & Tennyson, 1997, page 4)
Although specifically addressing schools, Richard Aird said the following in 2001:
"A pupil's school life is a brief affair, and the time in the classroom is a precious time that ought to be dedicated to minimising the handicapping affects of a pupil's disability and enabling the pupil to achieve maximum potential in a broad but relevant curriculum that is unique to the SLD sector and does not smack of the tokenism that has marred the history of the implementation of the National Curriculum in the SLD sector thus far." (Aird, 2001, page 14)
If school life is but a 'brief affair' then how many more constraints are placed on staff and student alike by an even shorter period of study in a post-school provision? Therefore, one might reasonably argue that there is an even greater need for this 'precious time' to have a specific focus as aptly indicated by Aird. Should this focus be different and distinct to that provided by an individual's school experience or should it be an allowance of further time (in some form of school extension) for Learners who, by definition, acquire knowledge at a very different rate to that of their peers?
What do IEPMLD at this time in their lives really need to learn? Do they really need to be continuing placing their hands in mixtures of ingredients (for example) in some form of sensory cookery session as they have presumably been doing throughout their school career? How is this assisting a better quality of life in the future? There may well be a really good rationale for so doing. However, it must be made explicit and all staff (inclusive of the supporting team) must be made aware of this rationale. Indeed, one might ask if IEPMLD are ever likely to be cooking for themselves at all? In which case, why is cookery a part of your curriculum? It might be argued that 'cooking for leisure' is something that an IEPMLD might enjoy and thus choose to do for fun. This might be an acceptable rationale for the provision of this area on the curriculum but should it be compulsory for all Learners? Perhaps Learners should be permitted to choose what they wish to undertake acting as agents making decisions about their own future. Can IEPMLD act as agents? If this is believed not to be the case, does it not follow that one possible curriculum option would be the empowerment of young people through the development of 'agentive' awareness and skills? How can one choose if you do not know how to choose? How can you learn how to choose if you are never given choice? If you are never given choice how can you be an agent?
"One of the reasons that students with disabilities have not succeeded once they leave school is that the educational process has not prepared students with special learning needs adequately to become self-determined young people."
(Wehmeyer & Schalock, 2001, page 2)
For activities to be appropriate for Individuals Experiencing PMLD at F.E. level they must fulfill most of the following criteria. They must show how they:
• are age appropriate within the confines of the ‘preference not deference’ rule;
• are delivered in a manner that is commensurate with the Learner’s cognitive ability;
• engage each Learner such that the Learner is active and not passive;
• empower the Learner through improvements in capability/coordination or through the use of available technology;
• empower the Learner through improvements in cognition and communication;
• relate to the possible future experiences and opportunities of the Learner;
• expand possible future experiences and opportunities for the Learner;
• enhance the Learner’s future Quality Of Life;
• are realistic but not pessimistic (self-fulfilling prophecy).
Thus, this page concerns itself with pragmatic and meaningful ideas for use in a post school environment for IEPMLD. You may not agree with all that is suggested but, hopefully, there will be some sections that you will find inspirational. We should look to new possibilities and better futures for this population and not impose unnecesary barriers and limitations and simply because their given 'label' has previously suggested them:
"the existence of learning difficulties so extreme as to present a major obstacle to participation in some of the most basic experiences in life, ought rather to generate educational aims concerned with enabling them to participate in those experiences. An aim which we might express as: 'enabling the child to participate in those experiences which are uniquely human'." (Ware, 1994, page 71)
"It should also become evident that people that may seem to be 'cognitively limited' nevertheless have a great deal of cognitive competence. You will see that without this competence simple things like pointing or eye gaze in a way that is appropriate to the context would not be possible. Such seemingly simple behaviours are still beyond the capabilities of very sophisticated computer simulations and could not occur without considerable knowledge of the world and how to solve problems in that world. (Anderson J. 1990). Hopefully, you will see that even 'cognitively limited' individuals are capable of more than most people think they are (Bray N. & Turner L. 1986, 1987). Facilitators can build on this cognitive base." (Bray N. 1990)
Furthermore, Learners may be better served if the greater part of continuing study had a focus on future activity rather on the development of isolated skills:
"Focusing on activities requires teachers therefore to move from a developmental, skill-based approach, to an ‘activity-based’ intervention approach that considers participation in activities in meaningful contexts as a basis for analysis of educational progress." (Magne Tellevik & Elmerskog, 2009)
"One critical feature of a ‘good’ assessment for this group is that it contributes to improving the individual’s quality of life, by helping teachers
to prioritise learning" (Ware & Donnelly, 2004, page 12).
If the reader feels that aspects of this page are inappropriate or ill-advised or wishes to suggest other areas of development, a contact form is provided at the bottom of the page. Please fell free to use it to contact TalkSense. If any such comment or idea is used on this page then appropriate acknowledgement and credit will be given.
Please Note: This page may be updated from time to time. TalkSense reserves the right to add to, amend or abrogate any section of this page at any time. Should the page change significantly TalkSense will update the 'date counter' such that readers will be alerted. This page was last updated on:
September 28th, 2018
This Page is currently in development. Talksense hopes to have it complete sometime soon. The page will change significantly over time. However you got here, while you are free to browse, please note that some sections are presently missing or incomplete, may alter considerably, and the number order may change. Constructive comments are welcome! (Use form provided at end of page before bibliography)
IEPMLD
What does IEPMLD stand for and why use this term? IEPMLD is an abbreviated form of either Individual Experiencing Profound and Multiple Learning Difficulties OR for its plural form Individuals Experiencing Profound and Multiple Learning Difficulties. The singular or plural form being suggested by context.
I is for Individual ... Everyone is unique. Everyone is an individual. The focus is on the individual, the ability, and not the disability.
E is for Experiencing ... TalkSense chose not to use the word 'with' as this implies some form of unchangeable condition; 'Once PMLD always PMLD'. However, the word 'experiencing' suggests a non-permanent situation and thus, 'Once PMLD but not always'. Experiencing suggests the current situation. However, it also implies a future beyond this state of being. Experiencing also suggests 'experience' in that PMLD is not something that such individuals posses but rather inherit as a result of their experience with the environment. As a parent with a pushchair may become 'handicapped' by a flight of stairs but enabled and included by entrances on one level, the environment in which we might find ourselves defines us. In H.G.Wells' 'The country of the blind' (1911) the sighted man is not king! Indeed, he is the handicapped person as he cannot make his way around in rooms devoid of light which the inhabitants do not require.
P is for Profound ... Profound is the most serious, the most complex, the concerning state of all. Such Individuals can be amongst the most challenging and yet the most rewarding with whom to work.
M is for Multiple... Such Individuals will be experiencing multiple challenges.
L is for Learning... Learning is the question and learning is the answer
D is for Difficulties... The Individual will be experiencing multiple difficulties arising from the present condition. These may include significant sensory impairments as well as additional physical disabilities.
There is no one stereotypical form of an IEPMLD; some are ambulant some are not, some respond readily, some do not, some may experience epilepsy while other may not. Definitions vary:
"Children and adults with profound and multiple learning disabilities have more than one disability, the most significant of which is a profound learning disability. All people who have profound and multiple learning disabilities will have great difficulty communicating. Many people will have additional sensory or physical disabilities, complex health needs or mental health difficulties. The combination of these needs and/or the lack of the right support may also affect behaviour. Some other people, such as those with autism and Down’s syndrome may also have profound and multiple learning disabilities. All children and adults with profound and multiple learning disabilities will need high levels of support with most aspects of daily life." (PMLD Network)
"People with profound intellectual and multiple disabilities are among the most disabled individuals in our community. They have a profound intellectual disability, which means that their intelligence quotient is estimated to be under 20 and therefore that they have severely limited understanding. In addition, they have multiple disabilities, which may include impairments of vision, hearing and movement as well as other problems like epilepsy and autism. Most people in this group are unable to walk unaided and many people have complex health needs requiring extensive help. People with profound intellectual and multiple disabilities have great difficulty communicating; they typically have very limited understanding and express themselves through non-verbal means, or at most through using a few words or symbols. They often show limited evidence of intention. Some people have, in addition, problems of challenging behaviour such as self-injury." (Mansell, 2010)
"People with profound intellectual and multiple disabilities, or profound and multiple learning disabilities (PMLD), can be some of the most
disabled individuals in our communities. They have a profound intellectual disability, which means that their intelligence quotient (IQ) is estimated to be under 20 and therefore they have severely limited understanding. In addition, they may have multiple disabilities, which can include impairments of vision, hearing and movement as well as other challenges such as epilepsy and autism. Most people in this group need support with mobility and many have complex health needs requiring extensive support. People with profound intellectual and multiple disabilities may have considerable difficulty communicating and characteristically have very limited understanding." (BILD 2016)
(Note: For an expanded definition of PMLD see Bellamy et al, 2010)
However PMLD is defined, there are some areas in which all might agree. Individuals Experiencing Profound and Multiple Learning Difficulties:
There are however those with dissenting views on such definitions of 'People with PMLD':
"In our view, describing children with PMLD primarily in terms of developmental deficits dehumanises them and potentially leads to their exclusion and degradation." (Simmons & Watson, page 25, 2014)
While taking on board the point being made here, I would doubt that the intention of the majority of individuals attempting a defintion of PMLD was in any way pejorative. Likewise, this section and, indeed, this page is not intended to be viewed in that light. The purpose is to illuminate practices that may deliver an amelioration of the experience (the E in IEPMLD) providing an increased quality of life. Thus, the question is, 'Can PMLD be ameliorated by input from varying professionals (and para-professionals) or is it a permanent unchangeable 'condition' at this moment in time'? In other words, once PMLD always PMLD? Talksense believes that all human beings are capable of learning given an approach adequately tailored to their needs.
All brains are now understood to be plastic:
"The adult brain, in short, retains much of the plasticity of the developing brain, including the power to repair damaged regions, to grow new neurons, to rezone regions that performed one task and have them assume a new task, to change the circuitry that weaves the neurons into the networks that allows us to remember, feel, suffer, think, imagine, and dream." (Begley, 2009, page 7)
"The effect of brain damage or lack of parts of the brain, by definition, will restrict the number of neurons present from the outset and, of course, also restrict the numbers of synapses that can develop. However, if we remember that synapses are formed throughout our lives (brain plasticity) there are always possibilities that people with PMLD can make new connections and learn new things just like typically developing people. Sensory stimulation, experiences with objects and new activities are just as important whatever the age of the learner." (Lacey, 2015, page 44)
Given advances in the therapies, medicine, care and education, it must be possible to harness the brain's plasticity to take an individual Learner from a state of pre-intentional responses to stimuli to one of intentionality, raising the individual's level of consciousness of the world to a point where the Learner can no longer be classified as having a profound cognitive condition. No claim is being made that any Learner will metamorphose from PLMD to Ph.D. rather that all Learners can continue to make progress given the appropriate environment, tools, and input. Will such progress guarantee each and every Learner a brighter future? That would be a foolhardy claim to make. However, it may be claimed that it increases the possibility of such a position.
In 2006 Ian Lamond said:
"I have where possible tried to avoid referring to anyone as disabled or as having a PMLD. This is at least in part because of my own belief that disability, whether physical disability or learning disability, is not something that a person has. My own view is that disability is something that is experienced or encountered as a result of the environment a person is in, or the people that are around them." (page 7)
Talksense likes to discuss people experiencing severe and profound learning difficulties using the phrase 'Stricken not Stupid' where 'stricken' denotes an impairment in cognitive functioning as a result of an (cerebral) injury or some agency, outside the control of the individual, impairing proper progression.
I is for Individual ... Everyone is unique. Everyone is an individual. The focus is on the individual, the ability, and not the disability.
E is for Experiencing ... TalkSense chose not to use the word 'with' as this implies some form of unchangeable condition; 'Once PMLD always PMLD'. However, the word 'experiencing' suggests a non-permanent situation and thus, 'Once PMLD but not always'. Experiencing suggests the current situation. However, it also implies a future beyond this state of being. Experiencing also suggests 'experience' in that PMLD is not something that such individuals posses but rather inherit as a result of their experience with the environment. As a parent with a pushchair may become 'handicapped' by a flight of stairs but enabled and included by entrances on one level, the environment in which we might find ourselves defines us. In H.G.Wells' 'The country of the blind' (1911) the sighted man is not king! Indeed, he is the handicapped person as he cannot make his way around in rooms devoid of light which the inhabitants do not require.
P is for Profound ... Profound is the most serious, the most complex, the concerning state of all. Such Individuals can be amongst the most challenging and yet the most rewarding with whom to work.
M is for Multiple... Such Individuals will be experiencing multiple challenges.
L is for Learning... Learning is the question and learning is the answer
D is for Difficulties... The Individual will be experiencing multiple difficulties arising from the present condition. These may include significant sensory impairments as well as additional physical disabilities.
There is no one stereotypical form of an IEPMLD; some are ambulant some are not, some respond readily, some do not, some may experience epilepsy while other may not. Definitions vary:
"Children and adults with profound and multiple learning disabilities have more than one disability, the most significant of which is a profound learning disability. All people who have profound and multiple learning disabilities will have great difficulty communicating. Many people will have additional sensory or physical disabilities, complex health needs or mental health difficulties. The combination of these needs and/or the lack of the right support may also affect behaviour. Some other people, such as those with autism and Down’s syndrome may also have profound and multiple learning disabilities. All children and adults with profound and multiple learning disabilities will need high levels of support with most aspects of daily life." (PMLD Network)
"People with profound intellectual and multiple disabilities are among the most disabled individuals in our community. They have a profound intellectual disability, which means that their intelligence quotient is estimated to be under 20 and therefore that they have severely limited understanding. In addition, they have multiple disabilities, which may include impairments of vision, hearing and movement as well as other problems like epilepsy and autism. Most people in this group are unable to walk unaided and many people have complex health needs requiring extensive help. People with profound intellectual and multiple disabilities have great difficulty communicating; they typically have very limited understanding and express themselves through non-verbal means, or at most through using a few words or symbols. They often show limited evidence of intention. Some people have, in addition, problems of challenging behaviour such as self-injury." (Mansell, 2010)
"People with profound intellectual and multiple disabilities, or profound and multiple learning disabilities (PMLD), can be some of the most
disabled individuals in our communities. They have a profound intellectual disability, which means that their intelligence quotient (IQ) is estimated to be under 20 and therefore they have severely limited understanding. In addition, they may have multiple disabilities, which can include impairments of vision, hearing and movement as well as other challenges such as epilepsy and autism. Most people in this group need support with mobility and many have complex health needs requiring extensive support. People with profound intellectual and multiple disabilities may have considerable difficulty communicating and characteristically have very limited understanding." (BILD 2016)
(Note: For an expanded definition of PMLD see Bellamy et al, 2010)
However PMLD is defined, there are some areas in which all might agree. Individuals Experiencing Profound and Multiple Learning Difficulties:
- typically have more than one disability;
- have a profound cognitive disability;
- have especial difficulty with communicating;
- require high levels of support with virtually every aspect of daily life;
- may have additional sensory or physical disabilities, complex health needs, or mental health difficulties;
- may exhibit behaviours that others find challenging.
There are however those with dissenting views on such definitions of 'People with PMLD':
"In our view, describing children with PMLD primarily in terms of developmental deficits dehumanises them and potentially leads to their exclusion and degradation." (Simmons & Watson, page 25, 2014)
While taking on board the point being made here, I would doubt that the intention of the majority of individuals attempting a defintion of PMLD was in any way pejorative. Likewise, this section and, indeed, this page is not intended to be viewed in that light. The purpose is to illuminate practices that may deliver an amelioration of the experience (the E in IEPMLD) providing an increased quality of life. Thus, the question is, 'Can PMLD be ameliorated by input from varying professionals (and para-professionals) or is it a permanent unchangeable 'condition' at this moment in time'? In other words, once PMLD always PMLD? Talksense believes that all human beings are capable of learning given an approach adequately tailored to their needs.
All brains are now understood to be plastic:
"The adult brain, in short, retains much of the plasticity of the developing brain, including the power to repair damaged regions, to grow new neurons, to rezone regions that performed one task and have them assume a new task, to change the circuitry that weaves the neurons into the networks that allows us to remember, feel, suffer, think, imagine, and dream." (Begley, 2009, page 7)
"The effect of brain damage or lack of parts of the brain, by definition, will restrict the number of neurons present from the outset and, of course, also restrict the numbers of synapses that can develop. However, if we remember that synapses are formed throughout our lives (brain plasticity) there are always possibilities that people with PMLD can make new connections and learn new things just like typically developing people. Sensory stimulation, experiences with objects and new activities are just as important whatever the age of the learner." (Lacey, 2015, page 44)
Given advances in the therapies, medicine, care and education, it must be possible to harness the brain's plasticity to take an individual Learner from a state of pre-intentional responses to stimuli to one of intentionality, raising the individual's level of consciousness of the world to a point where the Learner can no longer be classified as having a profound cognitive condition. No claim is being made that any Learner will metamorphose from PLMD to Ph.D. rather that all Learners can continue to make progress given the appropriate environment, tools, and input. Will such progress guarantee each and every Learner a brighter future? That would be a foolhardy claim to make. However, it may be claimed that it increases the possibility of such a position.
In 2006 Ian Lamond said:
"I have where possible tried to avoid referring to anyone as disabled or as having a PMLD. This is at least in part because of my own belief that disability, whether physical disability or learning disability, is not something that a person has. My own view is that disability is something that is experienced or encountered as a result of the environment a person is in, or the people that are around them." (page 7)
Talksense likes to discuss people experiencing severe and profound learning difficulties using the phrase 'Stricken not Stupid' where 'stricken' denotes an impairment in cognitive functioning as a result of an (cerebral) injury or some agency, outside the control of the individual, impairing proper progression.
1. School's Out

"School's out forever.
School's been blown to pieces"
The 1972 Alice Cooper hit 'School's Out' might be reinterpreted to infer the message of this section of the webpage, namely that Specialist Further Education in whatever form that takes (unit additional to school, residential college of specialist FE, unit in FE college, ...) is NOT school, should not be seen as school, and should have a very different look and feel to school. Whilst this might be difficult to achieve in an FE unit in actual school building there are certain fundamentals that are highly recommended nevertheless:
School's been blown to pieces"
The 1972 Alice Cooper hit 'School's Out' might be reinterpreted to infer the message of this section of the webpage, namely that Specialist Further Education in whatever form that takes (unit additional to school, residential college of specialist FE, unit in FE college, ...) is NOT school, should not be seen as school, and should have a very different look and feel to school. Whilst this might be difficult to achieve in an FE unit in actual school building there are certain fundamentals that are highly recommended nevertheless:
- The Learners have a new status as adults and should be treated as such even though they be operating at a level far below their chronological age;
- The system of time management in the FE setting does not have to follow that of school;
- As the your country's curriculum no longer is likely to apply, you may adopt a curriculum tailored to the specific needs of the Students;
- The dress code should be less formal and more individualistic;
- Age appropriate materials, supplies, and attitudes (see section on age appropriateness later on this page);
- Typically Further Education students do not stay in one classroom all day, they move from seminar room to seminar room;
- Typically Further Education students occupy a separate space to younger Learners;
- The language employed by staff should be different. For example, it is not uncommon to hear praise of the form 'Good boy/girl' in a school setting but this is strictly taboo in further education. Whilst you might use 'Good man/woman' in place of the former, 'Good work' might be even more appropriate or 'That's good <Name>' employing the Learner's first name instead or 'boy' or 'girl'. If you phrase all remarks as though you were talking to a (younger) colleague then you'll not go astray. Saying 'good boy' to a younger colleague would seem highly patronising and be totally inappropriate but 'That's brilliant Ben' or 'Fantastic Fiona' would be perfectly acceptable;
- The student body should have a 'voice' with management listening to learners and providing a framework for the students to
inform their own learning and adapt the provision were possible. This is a very challenging aspect of FE management when providing for IEPMLD; - Time in FE is likely to be short and therefore transition to possible appropriate future placements must be high on the agenda.
2. Begin the Begin
In the children's classic 'Alice in Wonderland' (Charles Lutwidge Dodgson) during the trial of the Knave of Hearts, the King says to the white rabbit when he asks where he should begin:
“Begin at the beginning," the King said, very gravely, "and go on till you come to the end: then stop.”
It may seem obvious that, in teaching Individuals Experiencing Profound and Multiple Learning Difficulties (IEPMLD), we need to begin at the beginning, carry on until we get to the place we intended for our session, and then stop but what does that actually mean in practice? Where is the beginning? How should we carry on? How do we know that we have reached 'the end'? How do we know that the IEPMLD have made that journey along with us?
"How to make the process meaningful and accessible to children with PMLD and the practicalities of sharing in a transparent manner is practically challenging." (Goodwin, 2013, page 24)
There will have been times in your life when you have been listening intently to an explanation but, as the explanation proceeded, somewhere along the way you lost the plot and failed to grasp what was being said. For example, when listening to theoretical physics at the quantum level I start out comprehending (at least I think I comprehend) what is being said but, as the explanation moves deeper and deeper, I find myself completely confused and not understanding. Can my understanding be improved? Can the structure of my brain be altered such that my intelligence is developed so that I can understand what is being said? Perhaps there are ways of achieving that but isn't there a much, much simpler solution? Rather than improve understanding why don't we improve the teaching? If the message was conveyed in a way which was commensurate with the level of my understanding then perhaps I might be able to move further along the pathway. It is therefore important that the teaching staff are aware of 'considered best practice' and the course that they should follow:
"A handicapped child represents a qualitatively different, unique type of development.... If a blind or deaf child achieves the same level of development as a normal child, then the child with a defect achieves this in another way, by another course, by other means; and, for the pedagogue, it is particularly important to know the uniqueness of the course along which he must lead the child. This uniqueness transforms the minus of the handicap into the plus of compensation." (Vygotsky, 1993)
In teaching IEPMLD we must obey at least eight fundamental rules:
Take the Trouble to start in the right place; that is with what the Learners already know and understand;
Explain using methodologies and terms that the Learners understand;
Appropriate Amounts: restrict the volume of new information delivered at any one time; single task - don't demand multi-tasking;
Clarity before accuracy:
Hold Heedfulness: ensure attention; show enthusiasm; inhibit interruptions;
Investigate comprehension: check for clues that confirm comprehension; evaluate understanding;
Number of repetitions: Not once but repeated over and over as many times as necessary; Take the Time;
Give Glee: Find Fun; Create Challenge but Suppress Stress; Learn to Love; Embrace the Enjoyable.
The above listing does not address 'what' should be taught but, rather, 'how'. The'what' can be found throughout the varying sections on this webpage and will therefore not be addressed here.
TEACHING requires that staff take the trouble to discover what the Learners already know and understand and build from there.
"When I'm working with people with PMLD, I always remind myself of the adage: 'start where the learners are and not where you think they should be……but you can't leave them there'. I know I must expect people with PMLD to learn how to think but I must also be realistic and build on what I can see is happening. I can't just give sensory experiences and hope that learning will take place. I need to know how many times to repeat the stimulus, what the likely reaction will be, how long it takes for that reaction to occur, where the best reactions take place, who gets the best reactions. It has to be very precise or I may not be 'where the learner is'. Typical learners can learn as long as the input/activity is roughly in the right cognitive area." (Lacey, 2015, page 46)
Too often materials are utilised in classrooms using concepts that are in advance of the current comprehension levels of the Learners: For example, some sensory stories Talksense have witnessed were about space and space flight. While the staff might have argued that the topic was irrelevant because the purchase was to have sensory experiences and to have fun (all well and good), if the topic is irrelevant then why not make it something that the Learners might already comprehend whilst still providing the sensory experiences and the fun (Giving Glee)? Of course, Talksense's view is that topics are not irrelevant and that they should always match the current level and needs of the individual Learners concerned. The question becomes, 'how can we ascertain what the Learners know and understand?'
Assessment of the current understanding of an IEPMLD is not a straightforward nor an easy task:
"Anyone who teaches pupils/ students with PMLD will be aware how difficult it is to assess the learning of the most disabled members of this group in a meaningful and holistic way". (Ware & Donnelly, 2004, page 12)
Routes to Learning (2006) offers a possible strategy for assessing the current level of knowledge of an IEPMLD. It is based on observations of an individuals behaviour when provided with varying forms of stimulation in controlled situations. It also emphasises that the starting point is 'a step you know they can already do':
"In order to use the chart to assess a pupil you start at a step you know they can already do, and work down through the steps until they do not respond. The routemap then shows a number of possible learning pathways to the next major ‘junction’. This encourages the adoption of problem solving approaches, for example when barriers to learning are encountered." (Ware & Donnelly, 2004, page 14)
However, even the Route Map has issues (even though Talksense has the greatest respect for the writings and works of Jean Ware)! For example, Route Map step 37 is 'communicates choice to attentive adult' for which its suggestion is to 'offer two items simultaneously. Observe the learner closely for obvious or increased attention to one of the items which communicates his/her preference'. The Route Map provides four observation criteria (smiling, eye pointing, reaching, and turning towards a preferred item) as apparent evidence of ability in this area. We can ask ourselves is 'smiling' in the presence of an object an indication of a preference? While it may be indicative in some circumstances and for some individuals it does not follow that it is necessarily an infallible and objective assessment of ability. Let's suppose that a learner reaches for an object; does this indicate that a choice has been made? Even this action is problematic! To analyse this extensively is beyond the scope of this page (see the choice page this web site for further explanation of this area). However, perhaps the Learner has a right side bias and will always select an item positioned in his/her right sensory field. Perhaps the Learner is attracted to 'light' and the item 'selected' just happened to glint in the sunlight a little more than the alternative. In either of these cases can we claim that the Learner is making a conscious choice? That is NOT to downplay the value of the Route Map nor to suggest it is not a good tool in the special education armoury, rather to challenge your thinking on what constitutes an effective assessment of ability in an IEPMLD.
"Eliminate all other factors, and the one which remains must be the truth" (Sherlock Holmes: The Sign of Four, 1890, Chapter 1, p. 92, Sir Arthur Conan Doyle)
In order to ascertain present understanding, we must scrutinise any response to a stimulus and, as Conan Doyle suggests (see quote above) 'eliminate all other factors' to discover any possible 'truth'. Thus, in reaching for an object, can we state that an individual has made a conscious choice if we have not (i) searched for alternative explanations and (ii) eliminated each in turn? It is when an observable behaviour can be explained by only one rationale (all others [including chance] being dismissed) that we might hypothesise that the behaviour B is as a result of an antecedent ability A of the Learner in question. To assume otherwise is to build castles from sand which might soon be washed away completely.
'Explain using methodologies and terms that the Learners understand' also provides us with a similar problem; that is, how do we know what the Learners understand?! If I am not sure of understanding unless evidenced by factors covered in the previous chapter then why would I utilise language, subject matter (topics), and or methodologies that are obviously beyond a Learners present level of cognition? Yet, I see this quite often in special education classrooms! For example, I hear stories being told of mythical creatures, space travel, even epic sea voyages which are beyond the every experiences of most if not all in the class no matter what sensory stimulation is being utilised to bring the story 'to life'. Why can't the stories concern experiences that the individuals in the group are likely to have encountered? Why not utilise everyday events using simple everyday language to provide the basis for learning and sensory stimulation?
Teachers tend to explain using the medium of language; there is a lot of it in any classroom that you visit. However, for IEPMLD language alone may not always be the best medium for information exchange. Indeed, language may have to be ruled out sometimes:
"It wasn't that I could not think anymore. I just didn't think in the same way. Communication with the external world was out. Language with linear processing was out. But thinking in pictures was in. Gathering glimpses of information, moment by moment, and then taking time to ponder the experience, was in." (Bolte Taylor, 2008, page 75)
Appropriate Amounts: restrict the volume of new information delivered at any one time; single task - don't demand multi-tasking
"Some may find difficulty in responding to stimuli through competing sensory channels, e.g. a learner may be unable to carry out a tactile search while listening to the teacher talking. In the early stages of development it may be appropriate to limit input to one sense only." (Northern Ireland Curriculum 2012)
"When it comes to information, it turns our that one can have too much of a good thing.,At a certain level of input, the law of diminishing returns takes effect; the glut of information no longer adds to our quality of life, but instead begins to cultivate stress, confusion, and even ignorance. Information overload threatens our ability to educate ourselves and leaves us more vulnerable as consumers and less cohesive as a society. For most of us, it actually diminishes our control over our own lives." (Shenk, 2003, page 395)
"The need to avoid an overload of sensory information has always been foremost in planning, and in some instances, it is the contrast between one section and the next which provides the stimulus to which pupils respond." (Henderson, 205, page 19)
"The trouble was that she (the teacher) gave me too many instructions. By the time I got to where I needed to be I had forgotten all but the last one and that didn’t make any sense on its own. So I hid." (Emma quoted in 'A Guide to Specific Learning Difficulties', 2017, page 4)
Almost everyone has heard the term 'information overload' which, in essence, means difficulty in (or a total lack of) comprehension as a result of too much information being provided at any one time. Information overload takes on more significance when the individual Learner concerned has a sensory processing disorder (see, for example, Koziol, Ely Budding, & Chidekel, 2011; May-Benson, 2011; Thye, Bednarz, Herringshaw, Sartin, & Kana, 2017). A sensory processing disorder may be defined as a failure to respond appropriately to the requirements of an environment as a result of inadequate processing and or integration (see the work of Jean Ayres, 1970, 1972, 1973, 1974 and see section on 'Sensory Integration' lower down on this webpage) of incoming sensory data (for a useful Sensory Processing Disorder checklist go here). In some cases, the Learner may be unable to screen out background sensory input from one or more of the sense organs such that the input becomes overwhelming:
"One of my sensory problems was hearing sensitivity, where certain loud noises, such as a school bell, hurt my ears. It sounded like a dentist drill going through my ears." (Grandin,1992)
"Some children with more severe sensory problems may withdraw further because the intrusion completely overloads their immature nervous system. They will often respond best to gentler teaching methods such as whispering softly to the child in a room free of florescent lights and visual distractions. Donna Williams (explained that forced eye contact caused her brain to shut down. She states when people spoke to her, their words become a mumble jumble, their voices a pattern of sounds. She can use only one sensory channel at a time. If Donna is listening to somebody talk, she is unable to perceive a cat jumping up on her lap. If she attends to the cat, then speech perception is blocked. She realized a black thing was on her lap, but she did not recognize it as a cat until she stopped listening to her friend talk." (Grandin,1996)
"Imagine driving a car that isn't working well. When you step on the gas the car sometimes lurches forward and sometimes doesn't respond. When you blow the horn it sounds blaring. The brakes sometimes slow the car, but not always. The blinkers work occasionally, the steering is erratic, and the speedometer is inaccurate. You are engaged in a constant struggle to keep the car on the road, and it is difficult to concentrate on anything else." (Greenspan, 1996)
"It was obvious that I perceived incoming stimulation as painful. Sound streaming in through my ears blasted my brain senseless so that when people spoke, I could not distinguish their voices from the underlying clatter of the environment." (Bolte Taylor, 2008, Page 72)
"At the most elementary level of information processing, stimulation is energy, and my brain needed to be protected, and isolated from obnoxious sensory stimulation, which it perceived as noise." (Bolte Taylor, 2008, Page 112)
"When people experience sensory overload or anxiety their behaviour may seem a little different to others, they aren't having a tantrum or being uncooperative they are simply overwhelmed and trying to cope best they can." ('A Guide to Specific Learning Difficulties', 2017, page 23)
In other cases, the information simply does not get through or gets scrambled along the way:
"The next thing you need to do is to control the rate and complexity of your communications with a child who has receptive language problems. A barrage of auditory input that overloads his 'wires' will result in lost bits of data. The child may remember some of it, but not all. What he does remember may be scrambled. Slow down your pace and give him a chance to absorb one thing before piling another on top of it." (Utley Adelizzi & Goss, 2001, page 111)
Thus, everything staff do together with IEPMLD should be simple. This includes the language used to convey information to Learners; it should be simple. The acronym ‘KISS’ (Keep It Short & Simple) should become a byword with staff avoiding ambiguity at all costs. Learners would be much better served if staff were to use the skills used by teachers of the deaf (Quigley S. & Kretchmer R. 1982, Wood D., Wood H. H., Griffiths A., & Howarth A. 1986):
Of course, the understanding of language itself may be problematic for many if not all of our Learners. However, ‘What is being said’, is far more than speech: It includes the staff member’s tone, facial expressions, gestures, and body language, as well as cues given from contextual information. Indeed, it has been demonstrated (Mehrabian & Ferris 1967) that, in presentations before groups of people, 55% of the impact is determined by body language, 38% by tone, and only 7% by the actual content of the presentation. As early as 1958, Bruce (Bruce D. 1958) showed that words used in a meaningful context is better understood than language used out of context. 'A meaningful context' can occur naturally (as in a park or a supermarket) or be 'engineered' by staff and both can be augmented with the addition of other sensory cues to aid comprehension:
"Children who are presented with information in a verbal medium (that is, the spoken or written word) frequently have greater difficulty in understanding or decoding the verbal input than they would have in understanding a nonverbal input(that is, a nonverbal event that is perceived visually or tactually)." (Milgram, N. 1973 page 167)
'Total communication' is a philosophy stressing the importance of multimodal forms of communication (which had its roots in the 1960s). Those supporting such an approach advocated the use of all appropriate means of input and output (for example, objects, pictures, symbols and signs in addition to speech) to facilitate communication and comprehension (see, for example, Denton,1970; Vernon,1972; Garretson,1976; Evans, 1982; Zangari, Lloyd, & Vicker, 1994). However, even here, there can be sensory overload!
Clarity before accuracy
While something can be completely accurate it can, at one and the same time, not be clear. An accurate depiction might involve too much information which, as the section above highlights, can be confusing while a simpler and shorter explanation might be better understood. Clarity is more likely to equate with understanding. If we teach clearly, our Learners are more likely to understand. This takes a great deal of effort, but when we speak in a 'language' that our Learners have a chance of understanding then there is hope of meaningful progression. It is important not to confuse the use of linguistic forms that are in advance of Learner's level of understanding with accuracy when their use will simply confuse the Learners. Translating and transforming more advanced terminology into simpler, comprehensible methodological approaches will help provide clarity.
"Sometimes in this sea of information we lose sight of the fact that there is another way to sharpen teaching and strengthen the educational impact of our institutions—improving the clarity and organization of our classes. Although this may not sound as transformative or exciting as some of the pedagogies and high-impact practices described above, it turns out to be very important for student learning, and it can pay dividends regardless of whether it is applied with these innovative pedagogies and practices or used on its own." (Blaich, Wise, Pascarella, & Roksa, 2016, page 6)
"Because it was very difficult for my ears to distinguish a single voice from background noise, I needed the question to be repeated slowly and enunciated clearly. I needed calm , clear communication. I may have had a dense expression on my face and appeared ignorant, but my mind was very busy concentrating on the acquisition of new information. My responses came slowly. Much too slowly for the real world ." (Bolte Taylor, 2008, page 76)
Hold Heedfulness
"Considerable evidence gathered over several decades highlights the importance of maximising the arousal and connectivity of individuals in this group, who are typically affected by a myriad of intrapersonal complications including sensory, intellectual and physical challenges." (Arthur-Kelly, Foreman, Bennett & Pascoe, 2008, page 162)
"An important focus of attention in the learning process is the alertness and attention of people with PMD. In research, these characteristics
are put forward as an essential basis for learning and developing (Arthur, 2003, 2004; Foreman, Arthur-Kelly, Pascoe, & King, 2004; Guess, Roberts, & Rues, 2002)." (Petry et al, 2007c, page 133)
To hold heedfulness is to assure attention. How do we hold heedfulness by assuring attention? There are a number of factors that can affect the attentiveness of an individual Learner in any group: Specific 'aspects' that can creep into any session have the ability to affect desirable outcomes. There may be several such 'aspects' but, here, we will deal with just two: waiting and distractions. It should be noted that it is common to find occurrences of self stimulatory behaviour amongst the population of Individuals Experiencing Profound and Multiple Learning Difficulties. The aetiology of such behaviours is complex but one causal factor is a lack of extrinsic stimulation. As such, Individuals who are sitting idle and spending periods waiting will tend to self stimulate. We should seek to extinguish Self Stimulatory Behaviours (See, for example, Rincover, A. 1978).
"when engaged in these behaviors, the children were particularly hard to 'reach' socially and difficult to teach.Their attention seemed to focus exclusively on their own behaviors, making them oblivious to all but the strongest external stimuli." (Lovaas, Newsom, & Hickman 1987 page 46)
While some Learners may self stimulate, others may fall asleep and some may even resort to behaviours that others may find challenging perhaps in an attempt to gain attention. None of these are desirable and, thus, periods of idleness need to be reduced to a minimum. Behaviours that others may find challenging may also act as a distraction from the goals of any particular session. If Learners are focused elsewhere, they are unlikely to be attending to a specific aspect of the session as well. As such staff should plan to try to reduce all external distractions: for example, you might put a 'do not disturb' sign on the door handle outside the room to notify others that, unless it is an emergency, they should not enter. As any aspect of a session is likely to be illustrated through the differing senses, all competing sensory input from other sources needs to be attenuated: you will want a quiet place to work in which you can control the ambiance as much as is possible: can you control the light, the sound, and the smells? It might be unwise therefore to consider delivering a Sensory Story (for example) in the classroom next to the dining hall in the period before lunch when the kitchen noises and smells are still pervasive even with a closed door.
Investigate comprehension
"Much of the checking for understanding done in schools is ineffective." (Fisher & Frey, 2014, page 1)
Investigating comprehension is not quite the same thing as an assessment of present understanding and, thus, starting in the right place. It involves means of checking as to whether what is currently being taught is making sense to the Learner, is understood and, thus, the Learner is making progress. Indeed, there is little point in preparing the most fantastic all singing and dancing sessions if the Learner is sitting there oblivious to it all throughout, and the session would have had as much impact if one staff member had just sat with the Learner and watched a recording of a documentary on quantum physics with very little interaction!
As any session proceeds, it is important that we investigate the comprehension of the Learner(s). The question now becomes just exactly how do we do that?
"Checking for understanding is an important step in the teaching and learning process. The background knowledge that students bring into the classroom influences how they understand the material you share and the lessons or learning opportunities you provide. Unless you check for understanding, it is difficult to know exactly what students are getting out of the lesson. In fact, checking for understanding is part of a formative assessment system in which teachers identify learning goals, provide students feedback, and then plan instruction based on students’ errors and misconceptions." (Fisher & Frey, 2014, page 2)
Controlling comprehension will involve 'holding heedfulness' as highlighted in the prior section as, if the Learner is not attending, it is very unlikely s/he is comprehending the purpose of the session at that point in time. However, attention, although very important, does not in and of itself, guarantee comprehension; we can attend very careful to a lecture on a difficult subject and yet leave the lecture hall completely confused! That then brings us full circle back to some of the other other issues detailed in the sections of 'TEACHING' detailed both above and below such as ensuring we are providing just the right amount of information, at the right level for the Learners, and making it fun and memorable. Even then, given the aforementioned items, how do we know if an individual has 'taken in' the purpose (objectives) of the session?
The use of a 'Total Communication' approach may be enlisted better to improve Learner comprehension:
"Consultation approaches with children with learning disabilities increasingly use total communication methods in order to ensure as
far as possible that meaning is understood by the child and the caregiver. However, many PMLD children who communicate pre-intentionally
may not have been listened to due to perceived issues of their capacity and the validity and ethicality of such approaches." (Goodwin, 2013, page 21)
However, while such an approach makes significant use of multiple modalities in conveying information with the aim of improving comprehension, it does not guarantee it nor does it check for it. While interpretations of Learner behaviours by Significant Others during sessions utilising Total Communication may suggest understanding, it is easier to assume a positive when you have a significant emotional investment in the outcome:
"Those who are most familiar with an individual and most likely to interpret their reactions appropriately are also likely to be those with the highest degree of emotional involvement." (Ware, 2004, page 32)
While it does not follow that Significant Others are always wrong in their 'assumptions of understanding' of Learners in their charge, their assumptions are still assumptions and not objectively verifiable facts. Is it possible to acquire objectively verifiable facts in the teaching and learning process with IEPMLD? While not as straightforward a process as with the assessment more able peers, there are some things which might indicate understanding in IEPMLD:
In the example above (a real life case) what can we claim about 'A's comprehension? Can we claim cause and effect skills (contingency awareness)? If so, why? As quoted earlier, Sherlock Homes said:
"Eliminate all other factors, and the one which remains must be the truth" (Sherlock Holmes: The Sign of Four, 1890, Chapter 1, p. 92, Sir Arthur Conan Doyle)
As we are claiming that the use of the switch to activate the video is evidence of contingency awareness comprehension in student 'A' what other possible explanations for the behaviour exist and can these be eliminated?
Number of repetitions
In the USA there is hardly a house to be found that doesn’t have a basketball hoop fixed to its wall and a child practising the necessary skills to become proficient at the game. The same is true of soccer in the U.K. We think nothing of a child spending hundreds of hours in such practice. Touch typists require approximately 200 hours of practice. Practice requires a number of repetitions; repetitions that provide an opportunity for the Individual to grasp the essence of that which is being conveyed or to begin to master a skill. Remember, IEPMLD require repetitions really regularly!
"Constant repetition and a great deal of support will be needed to generalise learning into new situations." (MENCAP, 2008, Page 4)
" Essentially, I had to completely inhabit the level of ability that I could achieve before it was time to take the next step. In order to atain a new ability, I had to be able to repeat that effort with grace and control before taking the next step." (Bolte Taylor, 2008, page 90)
"I needed my caregivers to teach me with patience. Sometimes I needed them to show me something over and over again., until my body and brain could figure out what I was learning" (Bolte Taylor, 2008, page 119)
"Repetition provides rehearsal and consolidation of known games and activities, and a continuous secure base and reference points. Through repetition variations occur, leading to new games and activities." (Quest For Learning, 2009, page 41)
"In order to meet their specific learning needs, a curriculum designed for pupils with MSI must provide frequent repetition and redundancy of information" (Murdoch et al, 2009, page 12)
"Remember that short, daily repetition is more valuable than longer, weekly sessions" (Association of Teachers and Lecturers, 2013, page 4)
"Focused on repeating sequences of sensory storytelling with the same three stories told every week for six weeks and then another three stories. The would allow for,the development of a pattern of sensory experiences using voice and body, and words and multi sensory objects." (Dowling, 2011, page 29)
"The student that I had the most progress with, was the student that I had every day, was seeing the symbols every day, over and over and over again." (Bruce, Trief, and Cascella, 2011)
"The more you bring a memory back to mind, the stronger it becomes. Boring but true. At the neural level, with each repetition you are strengthening the synaptic connections underlying the memory, allowing it to resist interference from other memories or general degradation. Repetition engages the neural networks related to our attention system; in other words, we tend to remember what we pay attention to." (Suzuki, 2015, page 75)
"So if people with PMLD have such difficulties with memory, how can they learn? As was suggested earlier in this article, sheer repetition is likely to be the answer. If John can learn to open his mouth to anticipate food on the spoon, then he can learn to anticipate other things,
but not without a tremendous amount of repetition. In my experience we do not repeat activities sufficiently. We want to give learners with PMLD an interesting life with lots of different sensory experiences, where perhaps we should be concentrating on a few that are repeated
many times." (Lacey, 2015, page 44)
The Murdoch et al quote (2009) above notes that IEPMLD curricula should contain 'redundancy'. Redundancy implies that the teaching should contain restatements of bits of information in slightly varying form so that each statement builds slowly on the preceding one (The orange needs to be cut; a knife is good for cutting an orange; let's get a knife to cut the orange; cut the orange with the knife)(see Blank and Marquis 1987). This leads to a re-formulation of the point made earlier on this page recommending the use of short sentences: it now becomes 'use short sentences but build in considerable redundancy such that each sentence builds into the next and helps to ease Learner comprehension':
"The alteration in the teacher's pattern of language has definite advantages for language disabled children. As noted above, the expanded verbalization is largely redundant. As a result, if children attend, they have the opportunity to have the information reinforced. By contrast, if their attention wavers, they still have the opportunity to hear the message that might have been missed. In addition, the expanded messages provide children with more time between questions, thereby meeting their needs to have longer periods in which to process information. Finally, in making the implicit explicit, the demands for inferential reasoning on the children's part are reduced, thereby bringing the conversation within manageable proportions." (Blank and Marquis. 1987)
Redundancy aids interaction between the Staff and the Learner. It eases the mental effort required by the Learner to comprehend the narrative. Consider the following two texts:
The second text example holds considerable redundancy but only increases the text by about 10 words. No assumption is made of 'carry-over' and intra-phrasal comprehension. The concepts are made explicit in each phrase. Each phrase builds on the next. By building redundancy into communication interactions with Learners in any presentation, staff assist comprehension, which should never be taken for granted.
Give Glee; Suppress Stress, Learn to Love and Find the Fun
"One of Sue’s most fundamental signals, and the basis of her style of celebrating his behaviour, is that she is really having a good time. She is not pretending to have fun for his sake, she isn’t shaping and styling her behaviour purely for his benefit, she is literally, unequivocally, unashamedly having a great time and indulging her own needs for enjoyment." (Nind, & Hewett, 1994 page 49)
If it is not fun for you or it is not fun for the user or for both of you, then:
Long term stress is toxic to the developing brain and, indeed, to all brains (Gunnar & Vazquez, 2006; Gunnar & Quevedo, 2007; Lupien, McEwen, Gunnar, & Heim 2009, Shonkoff, 2011; McEwen, 2012; Eiland & Romeo 2013; National Scientific Council on the Developing Child, 2014). Schools and Colleges should not be stressful environments: not for staff and not for students. We should do everything in our power to suppress the stress, find the fun and give glee. While short term stress (such as the school inspectors coming in?!) might be, on limited occasions, beneficial these should not be turned into long term stressors:
"Studies indicate that toxic stress can have an adverse impact on brain architecture. In the extreme, such as in cases of severe, chronic
abuse, especially during early, sensitive periods of brain development, the regions of the brain involved in fear, anxiety, and impulsive responses may overproduce neural connections while those regions dedicated to reasoning, planning, and behavioral control may produce fewer neural connections. Extreme exposure to toxic stress can change the stress system so that it responds at lower thresholds to events that might not be stressful to others, and, therefore, the stress response system activates more frequently and for longer periods than is necessary, like revving a car engine for hours every day. This wear and tear increases the risk of stress-related physical and mental illness later in life." (National Scientific Council on the Developing Child, 2005/2014)
"Although they are necessary for survival, frequent neurobiological stress responses increase the risk of physical and mental health problems, perhaps particularly when experienced during periods of rapid brain development." (Gunnar & Quevedo, 2007)
"Based on these bourgeoning lines of research, it appears that many factors converge during adolescence that may make this stage of development a particularly sensitive period to stressors, particularly in regard to neurobiological processes." (Eiland & Romeo 2013)
Finally, in this section, is the notion 'learning to love'; not just learning to love what you do although that plays a big part in achieving much of the above but, also, adding love and care to your interactions with others:
"I realised that morning that a hospital's number one responsibility should be protecting its patients' energy levels. This young girl was an energy vampire. She wanted to take something from me despite my fragile condition, and she had nothing to give me in return, She was rushing against a clock and obviously losing the race. In her haste, she was rough in the way she handled me and I felt like a detail that had fallen through someone's crack. She spoke a million miles a minute and hollered at me as if I were deaf. I sat and observed her absurdity and ignorance. She was I a hurry and I was a stroke survivor - not a natural match! She might have gotten something more from me had she come to me gently with patience and kindness, but because she insisted that I come to her in her time and at her pace, it was not satisfying for either of us. Her demands were annoying and I felt weary from the encounter." (Bolte Taylor, 2008, page 81)
In the 24th Annual Benjamin Ide Wheeler Society Lecture (2011), Professor Marian Diamond list five factors that her research highlighted as important for the enrichment of brains, one of which was 'love' (the other four will be covered elsewhere on this webpage. However, if you cannot wait to discover what they are watch the lecture yourself on YouTube by following the link above). Diamonds research showed that the love care and attention she payed to the research animals in her care the greater their cerebral cortex:
"She said she stumbled upon the fifth factor while performing her experiments with lab rats, which weren’t living long enough for her to study their brains in old age. Although the cages were well cleaned, many of the rats were dying after about 600 days, or roughly 60 years in a human time span. But some were living much longer. The difference, she found, was touch. By holding the lab rats against her lab coat and petting them each day, she found that she could increase their life span — and found that these rats generally had thicker cerebral cortices."
(Harrison Smith, 2016, The Washington Post, Obituary of Marian Diamond)
In other words, those animals who had more loving care had better developed brains and, thus, she added 'love' as a factor to her talks on the enrichment of the neural structure of the cerebrum.
“Begin at the beginning," the King said, very gravely, "and go on till you come to the end: then stop.”
It may seem obvious that, in teaching Individuals Experiencing Profound and Multiple Learning Difficulties (IEPMLD), we need to begin at the beginning, carry on until we get to the place we intended for our session, and then stop but what does that actually mean in practice? Where is the beginning? How should we carry on? How do we know that we have reached 'the end'? How do we know that the IEPMLD have made that journey along with us?
"How to make the process meaningful and accessible to children with PMLD and the practicalities of sharing in a transparent manner is practically challenging." (Goodwin, 2013, page 24)
There will have been times in your life when you have been listening intently to an explanation but, as the explanation proceeded, somewhere along the way you lost the plot and failed to grasp what was being said. For example, when listening to theoretical physics at the quantum level I start out comprehending (at least I think I comprehend) what is being said but, as the explanation moves deeper and deeper, I find myself completely confused and not understanding. Can my understanding be improved? Can the structure of my brain be altered such that my intelligence is developed so that I can understand what is being said? Perhaps there are ways of achieving that but isn't there a much, much simpler solution? Rather than improve understanding why don't we improve the teaching? If the message was conveyed in a way which was commensurate with the level of my understanding then perhaps I might be able to move further along the pathway. It is therefore important that the teaching staff are aware of 'considered best practice' and the course that they should follow:
"A handicapped child represents a qualitatively different, unique type of development.... If a blind or deaf child achieves the same level of development as a normal child, then the child with a defect achieves this in another way, by another course, by other means; and, for the pedagogue, it is particularly important to know the uniqueness of the course along which he must lead the child. This uniqueness transforms the minus of the handicap into the plus of compensation." (Vygotsky, 1993)
In teaching IEPMLD we must obey at least eight fundamental rules:
Take the Trouble to start in the right place; that is with what the Learners already know and understand;
Explain using methodologies and terms that the Learners understand;
Appropriate Amounts: restrict the volume of new information delivered at any one time; single task - don't demand multi-tasking;
Clarity before accuracy:
Hold Heedfulness: ensure attention; show enthusiasm; inhibit interruptions;
Investigate comprehension: check for clues that confirm comprehension; evaluate understanding;
Number of repetitions: Not once but repeated over and over as many times as necessary; Take the Time;
Give Glee: Find Fun; Create Challenge but Suppress Stress; Learn to Love; Embrace the Enjoyable.
The above listing does not address 'what' should be taught but, rather, 'how'. The'what' can be found throughout the varying sections on this webpage and will therefore not be addressed here.
TEACHING requires that staff take the trouble to discover what the Learners already know and understand and build from there.
"When I'm working with people with PMLD, I always remind myself of the adage: 'start where the learners are and not where you think they should be……but you can't leave them there'. I know I must expect people with PMLD to learn how to think but I must also be realistic and build on what I can see is happening. I can't just give sensory experiences and hope that learning will take place. I need to know how many times to repeat the stimulus, what the likely reaction will be, how long it takes for that reaction to occur, where the best reactions take place, who gets the best reactions. It has to be very precise or I may not be 'where the learner is'. Typical learners can learn as long as the input/activity is roughly in the right cognitive area." (Lacey, 2015, page 46)
Too often materials are utilised in classrooms using concepts that are in advance of the current comprehension levels of the Learners: For example, some sensory stories Talksense have witnessed were about space and space flight. While the staff might have argued that the topic was irrelevant because the purchase was to have sensory experiences and to have fun (all well and good), if the topic is irrelevant then why not make it something that the Learners might already comprehend whilst still providing the sensory experiences and the fun (Giving Glee)? Of course, Talksense's view is that topics are not irrelevant and that they should always match the current level and needs of the individual Learners concerned. The question becomes, 'how can we ascertain what the Learners know and understand?'
Assessment of the current understanding of an IEPMLD is not a straightforward nor an easy task:
"Anyone who teaches pupils/ students with PMLD will be aware how difficult it is to assess the learning of the most disabled members of this group in a meaningful and holistic way". (Ware & Donnelly, 2004, page 12)
Routes to Learning (2006) offers a possible strategy for assessing the current level of knowledge of an IEPMLD. It is based on observations of an individuals behaviour when provided with varying forms of stimulation in controlled situations. It also emphasises that the starting point is 'a step you know they can already do':
"In order to use the chart to assess a pupil you start at a step you know they can already do, and work down through the steps until they do not respond. The routemap then shows a number of possible learning pathways to the next major ‘junction’. This encourages the adoption of problem solving approaches, for example when barriers to learning are encountered." (Ware & Donnelly, 2004, page 14)
However, even the Route Map has issues (even though Talksense has the greatest respect for the writings and works of Jean Ware)! For example, Route Map step 37 is 'communicates choice to attentive adult' for which its suggestion is to 'offer two items simultaneously. Observe the learner closely for obvious or increased attention to one of the items which communicates his/her preference'. The Route Map provides four observation criteria (smiling, eye pointing, reaching, and turning towards a preferred item) as apparent evidence of ability in this area. We can ask ourselves is 'smiling' in the presence of an object an indication of a preference? While it may be indicative in some circumstances and for some individuals it does not follow that it is necessarily an infallible and objective assessment of ability. Let's suppose that a learner reaches for an object; does this indicate that a choice has been made? Even this action is problematic! To analyse this extensively is beyond the scope of this page (see the choice page this web site for further explanation of this area). However, perhaps the Learner has a right side bias and will always select an item positioned in his/her right sensory field. Perhaps the Learner is attracted to 'light' and the item 'selected' just happened to glint in the sunlight a little more than the alternative. In either of these cases can we claim that the Learner is making a conscious choice? That is NOT to downplay the value of the Route Map nor to suggest it is not a good tool in the special education armoury, rather to challenge your thinking on what constitutes an effective assessment of ability in an IEPMLD.
"Eliminate all other factors, and the one which remains must be the truth" (Sherlock Holmes: The Sign of Four, 1890, Chapter 1, p. 92, Sir Arthur Conan Doyle)
In order to ascertain present understanding, we must scrutinise any response to a stimulus and, as Conan Doyle suggests (see quote above) 'eliminate all other factors' to discover any possible 'truth'. Thus, in reaching for an object, can we state that an individual has made a conscious choice if we have not (i) searched for alternative explanations and (ii) eliminated each in turn? It is when an observable behaviour can be explained by only one rationale (all others [including chance] being dismissed) that we might hypothesise that the behaviour B is as a result of an antecedent ability A of the Learner in question. To assume otherwise is to build castles from sand which might soon be washed away completely.
'Explain using methodologies and terms that the Learners understand' also provides us with a similar problem; that is, how do we know what the Learners understand?! If I am not sure of understanding unless evidenced by factors covered in the previous chapter then why would I utilise language, subject matter (topics), and or methodologies that are obviously beyond a Learners present level of cognition? Yet, I see this quite often in special education classrooms! For example, I hear stories being told of mythical creatures, space travel, even epic sea voyages which are beyond the every experiences of most if not all in the class no matter what sensory stimulation is being utilised to bring the story 'to life'. Why can't the stories concern experiences that the individuals in the group are likely to have encountered? Why not utilise everyday events using simple everyday language to provide the basis for learning and sensory stimulation?
Teachers tend to explain using the medium of language; there is a lot of it in any classroom that you visit. However, for IEPMLD language alone may not always be the best medium for information exchange. Indeed, language may have to be ruled out sometimes:
"It wasn't that I could not think anymore. I just didn't think in the same way. Communication with the external world was out. Language with linear processing was out. But thinking in pictures was in. Gathering glimpses of information, moment by moment, and then taking time to ponder the experience, was in." (Bolte Taylor, 2008, page 75)
Appropriate Amounts: restrict the volume of new information delivered at any one time; single task - don't demand multi-tasking
"Some may find difficulty in responding to stimuli through competing sensory channels, e.g. a learner may be unable to carry out a tactile search while listening to the teacher talking. In the early stages of development it may be appropriate to limit input to one sense only." (Northern Ireland Curriculum 2012)
"When it comes to information, it turns our that one can have too much of a good thing.,At a certain level of input, the law of diminishing returns takes effect; the glut of information no longer adds to our quality of life, but instead begins to cultivate stress, confusion, and even ignorance. Information overload threatens our ability to educate ourselves and leaves us more vulnerable as consumers and less cohesive as a society. For most of us, it actually diminishes our control over our own lives." (Shenk, 2003, page 395)
"The need to avoid an overload of sensory information has always been foremost in planning, and in some instances, it is the contrast between one section and the next which provides the stimulus to which pupils respond." (Henderson, 205, page 19)
"The trouble was that she (the teacher) gave me too many instructions. By the time I got to where I needed to be I had forgotten all but the last one and that didn’t make any sense on its own. So I hid." (Emma quoted in 'A Guide to Specific Learning Difficulties', 2017, page 4)
Almost everyone has heard the term 'information overload' which, in essence, means difficulty in (or a total lack of) comprehension as a result of too much information being provided at any one time. Information overload takes on more significance when the individual Learner concerned has a sensory processing disorder (see, for example, Koziol, Ely Budding, & Chidekel, 2011; May-Benson, 2011; Thye, Bednarz, Herringshaw, Sartin, & Kana, 2017). A sensory processing disorder may be defined as a failure to respond appropriately to the requirements of an environment as a result of inadequate processing and or integration (see the work of Jean Ayres, 1970, 1972, 1973, 1974 and see section on 'Sensory Integration' lower down on this webpage) of incoming sensory data (for a useful Sensory Processing Disorder checklist go here). In some cases, the Learner may be unable to screen out background sensory input from one or more of the sense organs such that the input becomes overwhelming:
"One of my sensory problems was hearing sensitivity, where certain loud noises, such as a school bell, hurt my ears. It sounded like a dentist drill going through my ears." (Grandin,1992)
"Some children with more severe sensory problems may withdraw further because the intrusion completely overloads their immature nervous system. They will often respond best to gentler teaching methods such as whispering softly to the child in a room free of florescent lights and visual distractions. Donna Williams (explained that forced eye contact caused her brain to shut down. She states when people spoke to her, their words become a mumble jumble, their voices a pattern of sounds. She can use only one sensory channel at a time. If Donna is listening to somebody talk, she is unable to perceive a cat jumping up on her lap. If she attends to the cat, then speech perception is blocked. She realized a black thing was on her lap, but she did not recognize it as a cat until she stopped listening to her friend talk." (Grandin,1996)
"Imagine driving a car that isn't working well. When you step on the gas the car sometimes lurches forward and sometimes doesn't respond. When you blow the horn it sounds blaring. The brakes sometimes slow the car, but not always. The blinkers work occasionally, the steering is erratic, and the speedometer is inaccurate. You are engaged in a constant struggle to keep the car on the road, and it is difficult to concentrate on anything else." (Greenspan, 1996)
"It was obvious that I perceived incoming stimulation as painful. Sound streaming in through my ears blasted my brain senseless so that when people spoke, I could not distinguish their voices from the underlying clatter of the environment." (Bolte Taylor, 2008, Page 72)
"At the most elementary level of information processing, stimulation is energy, and my brain needed to be protected, and isolated from obnoxious sensory stimulation, which it perceived as noise." (Bolte Taylor, 2008, Page 112)
"When people experience sensory overload or anxiety their behaviour may seem a little different to others, they aren't having a tantrum or being uncooperative they are simply overwhelmed and trying to cope best they can." ('A Guide to Specific Learning Difficulties', 2017, page 23)
In other cases, the information simply does not get through or gets scrambled along the way:
"The next thing you need to do is to control the rate and complexity of your communications with a child who has receptive language problems. A barrage of auditory input that overloads his 'wires' will result in lost bits of data. The child may remember some of it, but not all. What he does remember may be scrambled. Slow down your pace and give him a chance to absorb one thing before piling another on top of it." (Utley Adelizzi & Goss, 2001, page 111)
Thus, everything staff do together with IEPMLD should be simple. This includes the language used to convey information to Learners; it should be simple. The acronym ‘KISS’ (Keep It Short & Simple) should become a byword with staff avoiding ambiguity at all costs. Learners would be much better served if staff were to use the skills used by teachers of the deaf (Quigley S. & Kretchmer R. 1982, Wood D., Wood H. H., Griffiths A., & Howarth A. 1986):
- use short sentences;
- avoid unnecessary words;
- choice of concrete rather than abstract words;
- use of straightforward language (not ‘what purpose does it serve?’ but ‘what is the use of?’);
- avoid words or phrases which may have a double meaning (overall, employed, I haven’t got a sausage, a close shave, .....);
- avoid metaphors (kick the bucket, pull your socks up);
- avoid unusual words;
- avoid double negatives (He won’t get none);
- avoid advanced grammatical forms. Use the active rather than the passive form;
- slow down speech slightly, but do not highlight every word: ‘A - dog - is - a - sort - of - animal’;
- do not shout;
- talk to the Learner; do not ‘dance’ around the environment whilst speaking; do not talk with your back to the Learner, for example, while writing or drawing on a board;
- look at the Learner whilst talking; gain eye contact; wait until you have attention;
- try to speak at the Learner’s own physical level; sit down opposite the Learner if possible - it will be much easier to follow what you are saying;
- patience is a virtue; repeat ideas and concepts using several differing modalities (signing, with object cues, with picture or other sensory cues, etc); check the concept;
- although you may have a mixed ability classroom and some, 'more advanced' Learners may use deviant language forms or have a delayed language structure, do not adopt these as patterns for teaching; staff should use very simple but correct syntax;
- do not assume comprehension; do not assume that people understand even when they might appear to indicate they do (by smiling for example); do not ask the question "Do you understand?”, rather, test for comprehension.
Of course, the understanding of language itself may be problematic for many if not all of our Learners. However, ‘What is being said’, is far more than speech: It includes the staff member’s tone, facial expressions, gestures, and body language, as well as cues given from contextual information. Indeed, it has been demonstrated (Mehrabian & Ferris 1967) that, in presentations before groups of people, 55% of the impact is determined by body language, 38% by tone, and only 7% by the actual content of the presentation. As early as 1958, Bruce (Bruce D. 1958) showed that words used in a meaningful context is better understood than language used out of context. 'A meaningful context' can occur naturally (as in a park or a supermarket) or be 'engineered' by staff and both can be augmented with the addition of other sensory cues to aid comprehension:
"Children who are presented with information in a verbal medium (that is, the spoken or written word) frequently have greater difficulty in understanding or decoding the verbal input than they would have in understanding a nonverbal input(that is, a nonverbal event that is perceived visually or tactually)." (Milgram, N. 1973 page 167)
'Total communication' is a philosophy stressing the importance of multimodal forms of communication (which had its roots in the 1960s). Those supporting such an approach advocated the use of all appropriate means of input and output (for example, objects, pictures, symbols and signs in addition to speech) to facilitate communication and comprehension (see, for example, Denton,1970; Vernon,1972; Garretson,1976; Evans, 1982; Zangari, Lloyd, & Vicker, 1994). However, even here, there can be sensory overload!
Clarity before accuracy
While something can be completely accurate it can, at one and the same time, not be clear. An accurate depiction might involve too much information which, as the section above highlights, can be confusing while a simpler and shorter explanation might be better understood. Clarity is more likely to equate with understanding. If we teach clearly, our Learners are more likely to understand. This takes a great deal of effort, but when we speak in a 'language' that our Learners have a chance of understanding then there is hope of meaningful progression. It is important not to confuse the use of linguistic forms that are in advance of Learner's level of understanding with accuracy when their use will simply confuse the Learners. Translating and transforming more advanced terminology into simpler, comprehensible methodological approaches will help provide clarity.
"Sometimes in this sea of information we lose sight of the fact that there is another way to sharpen teaching and strengthen the educational impact of our institutions—improving the clarity and organization of our classes. Although this may not sound as transformative or exciting as some of the pedagogies and high-impact practices described above, it turns out to be very important for student learning, and it can pay dividends regardless of whether it is applied with these innovative pedagogies and practices or used on its own." (Blaich, Wise, Pascarella, & Roksa, 2016, page 6)
"Because it was very difficult for my ears to distinguish a single voice from background noise, I needed the question to be repeated slowly and enunciated clearly. I needed calm , clear communication. I may have had a dense expression on my face and appeared ignorant, but my mind was very busy concentrating on the acquisition of new information. My responses came slowly. Much too slowly for the real world ." (Bolte Taylor, 2008, page 76)
Hold Heedfulness
"Considerable evidence gathered over several decades highlights the importance of maximising the arousal and connectivity of individuals in this group, who are typically affected by a myriad of intrapersonal complications including sensory, intellectual and physical challenges." (Arthur-Kelly, Foreman, Bennett & Pascoe, 2008, page 162)
"An important focus of attention in the learning process is the alertness and attention of people with PMD. In research, these characteristics
are put forward as an essential basis for learning and developing (Arthur, 2003, 2004; Foreman, Arthur-Kelly, Pascoe, & King, 2004; Guess, Roberts, & Rues, 2002)." (Petry et al, 2007c, page 133)
To hold heedfulness is to assure attention. How do we hold heedfulness by assuring attention? There are a number of factors that can affect the attentiveness of an individual Learner in any group: Specific 'aspects' that can creep into any session have the ability to affect desirable outcomes. There may be several such 'aspects' but, here, we will deal with just two: waiting and distractions. It should be noted that it is common to find occurrences of self stimulatory behaviour amongst the population of Individuals Experiencing Profound and Multiple Learning Difficulties. The aetiology of such behaviours is complex but one causal factor is a lack of extrinsic stimulation. As such, Individuals who are sitting idle and spending periods waiting will tend to self stimulate. We should seek to extinguish Self Stimulatory Behaviours (See, for example, Rincover, A. 1978).
"when engaged in these behaviors, the children were particularly hard to 'reach' socially and difficult to teach.Their attention seemed to focus exclusively on their own behaviors, making them oblivious to all but the strongest external stimuli." (Lovaas, Newsom, & Hickman 1987 page 46)
While some Learners may self stimulate, others may fall asleep and some may even resort to behaviours that others may find challenging perhaps in an attempt to gain attention. None of these are desirable and, thus, periods of idleness need to be reduced to a minimum. Behaviours that others may find challenging may also act as a distraction from the goals of any particular session. If Learners are focused elsewhere, they are unlikely to be attending to a specific aspect of the session as well. As such staff should plan to try to reduce all external distractions: for example, you might put a 'do not disturb' sign on the door handle outside the room to notify others that, unless it is an emergency, they should not enter. As any aspect of a session is likely to be illustrated through the differing senses, all competing sensory input from other sources needs to be attenuated: you will want a quiet place to work in which you can control the ambiance as much as is possible: can you control the light, the sound, and the smells? It might be unwise therefore to consider delivering a Sensory Story (for example) in the classroom next to the dining hall in the period before lunch when the kitchen noises and smells are still pervasive even with a closed door.
Investigate comprehension
"Much of the checking for understanding done in schools is ineffective." (Fisher & Frey, 2014, page 1)
Investigating comprehension is not quite the same thing as an assessment of present understanding and, thus, starting in the right place. It involves means of checking as to whether what is currently being taught is making sense to the Learner, is understood and, thus, the Learner is making progress. Indeed, there is little point in preparing the most fantastic all singing and dancing sessions if the Learner is sitting there oblivious to it all throughout, and the session would have had as much impact if one staff member had just sat with the Learner and watched a recording of a documentary on quantum physics with very little interaction!
As any session proceeds, it is important that we investigate the comprehension of the Learner(s). The question now becomes just exactly how do we do that?
"Checking for understanding is an important step in the teaching and learning process. The background knowledge that students bring into the classroom influences how they understand the material you share and the lessons or learning opportunities you provide. Unless you check for understanding, it is difficult to know exactly what students are getting out of the lesson. In fact, checking for understanding is part of a formative assessment system in which teachers identify learning goals, provide students feedback, and then plan instruction based on students’ errors and misconceptions." (Fisher & Frey, 2014, page 2)
Controlling comprehension will involve 'holding heedfulness' as highlighted in the prior section as, if the Learner is not attending, it is very unlikely s/he is comprehending the purpose of the session at that point in time. However, attention, although very important, does not in and of itself, guarantee comprehension; we can attend very careful to a lecture on a difficult subject and yet leave the lecture hall completely confused! That then brings us full circle back to some of the other other issues detailed in the sections of 'TEACHING' detailed both above and below such as ensuring we are providing just the right amount of information, at the right level for the Learners, and making it fun and memorable. Even then, given the aforementioned items, how do we know if an individual has 'taken in' the purpose (objectives) of the session?
The use of a 'Total Communication' approach may be enlisted better to improve Learner comprehension:
"Consultation approaches with children with learning disabilities increasingly use total communication methods in order to ensure as
far as possible that meaning is understood by the child and the caregiver. However, many PMLD children who communicate pre-intentionally
may not have been listened to due to perceived issues of their capacity and the validity and ethicality of such approaches." (Goodwin, 2013, page 21)
However, while such an approach makes significant use of multiple modalities in conveying information with the aim of improving comprehension, it does not guarantee it nor does it check for it. While interpretations of Learner behaviours by Significant Others during sessions utilising Total Communication may suggest understanding, it is easier to assume a positive when you have a significant emotional investment in the outcome:
"Those who are most familiar with an individual and most likely to interpret their reactions appropriately are also likely to be those with the highest degree of emotional involvement." (Ware, 2004, page 32)
While it does not follow that Significant Others are always wrong in their 'assumptions of understanding' of Learners in their charge, their assumptions are still assumptions and not objectively verifiable facts. Is it possible to acquire objectively verifiable facts in the teaching and learning process with IEPMLD? While not as straightforward a process as with the assessment more able peers, there are some things which might indicate understanding in IEPMLD:
- Performance;
- Reaction and Response.
In the example above (a real life case) what can we claim about 'A's comprehension? Can we claim cause and effect skills (contingency awareness)? If so, why? As quoted earlier, Sherlock Homes said:
"Eliminate all other factors, and the one which remains must be the truth" (Sherlock Holmes: The Sign of Four, 1890, Chapter 1, p. 92, Sir Arthur Conan Doyle)
As we are claiming that the use of the switch to activate the video is evidence of contingency awareness comprehension in student 'A' what other possible explanations for the behaviour exist and can these be eliminated?
- A is simply activating the switch randomly - This is not true as A only activates the switch when the music stops;
- A likes the sensory feedback provided by the switch - while that may or may not be true it does not account for the fact that A will only activate the switch under very specific circumstances (namely the video and music terminating);
- A is simply activating the switch by accident - Again, this is not true as A does not accidentally activate the switch while the video is playing.
- A is being prompted by some other agent to activate the switch appropriately - A will activate the switch appropriately when no other person is around even when s/he is unaware of being observed..
- A is activating the switch because of the silence at the end of the video. A does not understand it will repeat the favoured music - A will activate the switch at the end even in a noisy classroom and even if there is music coming from another source for another student in the room. Furthermore, if this were true, does this not demonstrate an understanding that the switch provides a source of 'non-silence' which, itself, is evidence of cause and effect.
- One final point, for which it is difficult to account, is A's repeated attempts to activate the switch when s/he targets and misses, then ceasing all further attempts (once successful) until the video and music stops once again.
Number of repetitions
In the USA there is hardly a house to be found that doesn’t have a basketball hoop fixed to its wall and a child practising the necessary skills to become proficient at the game. The same is true of soccer in the U.K. We think nothing of a child spending hundreds of hours in such practice. Touch typists require approximately 200 hours of practice. Practice requires a number of repetitions; repetitions that provide an opportunity for the Individual to grasp the essence of that which is being conveyed or to begin to master a skill. Remember, IEPMLD require repetitions really regularly!
"Constant repetition and a great deal of support will be needed to generalise learning into new situations." (MENCAP, 2008, Page 4)
" Essentially, I had to completely inhabit the level of ability that I could achieve before it was time to take the next step. In order to atain a new ability, I had to be able to repeat that effort with grace and control before taking the next step." (Bolte Taylor, 2008, page 90)
"I needed my caregivers to teach me with patience. Sometimes I needed them to show me something over and over again., until my body and brain could figure out what I was learning" (Bolte Taylor, 2008, page 119)
"Repetition provides rehearsal and consolidation of known games and activities, and a continuous secure base and reference points. Through repetition variations occur, leading to new games and activities." (Quest For Learning, 2009, page 41)
"In order to meet their specific learning needs, a curriculum designed for pupils with MSI must provide frequent repetition and redundancy of information" (Murdoch et al, 2009, page 12)
"Remember that short, daily repetition is more valuable than longer, weekly sessions" (Association of Teachers and Lecturers, 2013, page 4)
"Focused on repeating sequences of sensory storytelling with the same three stories told every week for six weeks and then another three stories. The would allow for,the development of a pattern of sensory experiences using voice and body, and words and multi sensory objects." (Dowling, 2011, page 29)
"The student that I had the most progress with, was the student that I had every day, was seeing the symbols every day, over and over and over again." (Bruce, Trief, and Cascella, 2011)
"The more you bring a memory back to mind, the stronger it becomes. Boring but true. At the neural level, with each repetition you are strengthening the synaptic connections underlying the memory, allowing it to resist interference from other memories or general degradation. Repetition engages the neural networks related to our attention system; in other words, we tend to remember what we pay attention to." (Suzuki, 2015, page 75)
"So if people with PMLD have such difficulties with memory, how can they learn? As was suggested earlier in this article, sheer repetition is likely to be the answer. If John can learn to open his mouth to anticipate food on the spoon, then he can learn to anticipate other things,
but not without a tremendous amount of repetition. In my experience we do not repeat activities sufficiently. We want to give learners with PMLD an interesting life with lots of different sensory experiences, where perhaps we should be concentrating on a few that are repeated
many times." (Lacey, 2015, page 44)
The Murdoch et al quote (2009) above notes that IEPMLD curricula should contain 'redundancy'. Redundancy implies that the teaching should contain restatements of bits of information in slightly varying form so that each statement builds slowly on the preceding one (The orange needs to be cut; a knife is good for cutting an orange; let's get a knife to cut the orange; cut the orange with the knife)(see Blank and Marquis 1987). This leads to a re-formulation of the point made earlier on this page recommending the use of short sentences: it now becomes 'use short sentences but build in considerable redundancy such that each sentence builds into the next and helps to ease Learner comprehension':
"The alteration in the teacher's pattern of language has definite advantages for language disabled children. As noted above, the expanded verbalization is largely redundant. As a result, if children attend, they have the opportunity to have the information reinforced. By contrast, if their attention wavers, they still have the opportunity to hear the message that might have been missed. In addition, the expanded messages provide children with more time between questions, thereby meeting their needs to have longer periods in which to process information. Finally, in making the implicit explicit, the demands for inferential reasoning on the children's part are reduced, thereby bringing the conversation within manageable proportions." (Blank and Marquis. 1987)
Redundancy aids interaction between the Staff and the Learner. It eases the mental effort required by the Learner to comprehend the narrative. Consider the following two texts:
- 'I have put lots of things on the table today. They are all sorts of fruit. As we have not done it before, that is what we are going to work with today.'
- 'Look at the table. I have put lots of things on the table today. The things on the table are all sorts of fruit. We have not had a story about fruit before. We are going to have a story about fruit today.'
The second text example holds considerable redundancy but only increases the text by about 10 words. No assumption is made of 'carry-over' and intra-phrasal comprehension. The concepts are made explicit in each phrase. Each phrase builds on the next. By building redundancy into communication interactions with Learners in any presentation, staff assist comprehension, which should never be taken for granted.
Give Glee; Suppress Stress, Learn to Love and Find the Fun
"One of Sue’s most fundamental signals, and the basis of her style of celebrating his behaviour, is that she is really having a good time. She is not pretending to have fun for his sake, she isn’t shaping and styling her behaviour purely for his benefit, she is literally, unequivocally, unashamedly having a great time and indulging her own needs for enjoyment." (Nind, & Hewett, 1994 page 49)
If it is not fun for you or it is not fun for the user or for both of you, then:
- it will not be successful;
- something is wrong.
Long term stress is toxic to the developing brain and, indeed, to all brains (Gunnar & Vazquez, 2006; Gunnar & Quevedo, 2007; Lupien, McEwen, Gunnar, & Heim 2009, Shonkoff, 2011; McEwen, 2012; Eiland & Romeo 2013; National Scientific Council on the Developing Child, 2014). Schools and Colleges should not be stressful environments: not for staff and not for students. We should do everything in our power to suppress the stress, find the fun and give glee. While short term stress (such as the school inspectors coming in?!) might be, on limited occasions, beneficial these should not be turned into long term stressors:
"Studies indicate that toxic stress can have an adverse impact on brain architecture. In the extreme, such as in cases of severe, chronic
abuse, especially during early, sensitive periods of brain development, the regions of the brain involved in fear, anxiety, and impulsive responses may overproduce neural connections while those regions dedicated to reasoning, planning, and behavioral control may produce fewer neural connections. Extreme exposure to toxic stress can change the stress system so that it responds at lower thresholds to events that might not be stressful to others, and, therefore, the stress response system activates more frequently and for longer periods than is necessary, like revving a car engine for hours every day. This wear and tear increases the risk of stress-related physical and mental illness later in life." (National Scientific Council on the Developing Child, 2005/2014)
"Although they are necessary for survival, frequent neurobiological stress responses increase the risk of physical and mental health problems, perhaps particularly when experienced during periods of rapid brain development." (Gunnar & Quevedo, 2007)
"Based on these bourgeoning lines of research, it appears that many factors converge during adolescence that may make this stage of development a particularly sensitive period to stressors, particularly in regard to neurobiological processes." (Eiland & Romeo 2013)
Finally, in this section, is the notion 'learning to love'; not just learning to love what you do although that plays a big part in achieving much of the above but, also, adding love and care to your interactions with others:
"I realised that morning that a hospital's number one responsibility should be protecting its patients' energy levels. This young girl was an energy vampire. She wanted to take something from me despite my fragile condition, and she had nothing to give me in return, She was rushing against a clock and obviously losing the race. In her haste, she was rough in the way she handled me and I felt like a detail that had fallen through someone's crack. She spoke a million miles a minute and hollered at me as if I were deaf. I sat and observed her absurdity and ignorance. She was I a hurry and I was a stroke survivor - not a natural match! She might have gotten something more from me had she come to me gently with patience and kindness, but because she insisted that I come to her in her time and at her pace, it was not satisfying for either of us. Her demands were annoying and I felt weary from the encounter." (Bolte Taylor, 2008, page 81)
In the 24th Annual Benjamin Ide Wheeler Society Lecture (2011), Professor Marian Diamond list five factors that her research highlighted as important for the enrichment of brains, one of which was 'love' (the other four will be covered elsewhere on this webpage. However, if you cannot wait to discover what they are watch the lecture yourself on YouTube by following the link above). Diamonds research showed that the love care and attention she payed to the research animals in her care the greater their cerebral cortex:
"She said she stumbled upon the fifth factor while performing her experiments with lab rats, which weren’t living long enough for her to study their brains in old age. Although the cages were well cleaned, many of the rats were dying after about 600 days, or roughly 60 years in a human time span. But some were living much longer. The difference, she found, was touch. By holding the lab rats against her lab coat and petting them each day, she found that she could increase their life span — and found that these rats generally had thicker cerebral cortices."
(Harrison Smith, 2016, The Washington Post, Obituary of Marian Diamond)
In other words, those animals who had more loving care had better developed brains and, thus, she added 'love' as a factor to her talks on the enrichment of the neural structure of the cerebrum.
3. The Goal is Control

"There is a real danger that any sense of the identity of a person with learning difficulties is subsumed beneath a prevailing desire to label, to pigeon-hole, to file and thereby to control."
(Gray and Ridden 1999)
"People with disabilities are more visible and more vocal than ever before, and they are increasingly demanding more control and choice in their lives."
(Field, Martin, Miller, Ward, & Wehmeyer 1998 page 11)
"Students become empowered by taking control of their own learning." (Sutcliffe 1990 page 13)
"Good quality support is to do with giving people power."
(Virginia Moffat 1996 page 37)
"a high quality of life is one in which people receive individually tailored support to become full participants in the life of the community, develop skills and independence, be given appropriate choice and control over their lives, be treated with respect in a safe and secure environment”. (Emerson et al 1996)
"Empowerment occurs when control, or power, is passed to an individual or group. In rehabilitation, medicine, social work, psychology, education, and many allied disciplines, it is gradually becoming recognized that the healthiest and most effective individuals have personal control and make decisions for themselves with advice and input from others. The belief here is that, for best results overall, final decisions should be made by the individuals who are most closely affected by the decisions." (Brown and Brown 2003 page 227)
"Independence for this specific group of children means providing them with the opportunity to exercise more control over their own existence, over their environment and over the things that happen to each individual child." (van der Putten, 2005, page 49)
"... with profound multiple disabilities, because of their prevailing disabilities, are totally dependent on their direct support persons in all daily tasks. Therefore, activities offered to children with PMD should be aimed at enhancing their independence and control over their own lives."
(Van der Putten et al, 2005b)
"Choice can be viewed as a key component of empowerment where individuals maintain control over their own lives and as such increase their ability to influence their future goals and ideals." (Bradley 2012)
Generally speaking, the more independent people are and the less external control they receive from others, the more satisfied they are (higher quality of life) (See Legault 1992).Thus, a fundamental goal of all special education should be equipping Learners to live as independent a life as possible. This has long been recognised:
"... citizens with a mental retardation have a right to receive such individual habilitation as will give each of them a realistic opportunity to lead a more useful and meaningful life and to return to society." (Bannerman, Sheldon, Sherman, & Harchik 1990)
"even children with profound learning difficulties , given suitable conditions provided by modern technology, can make choices; in this case between sounds, voices, and rhymes provided on speakers. Moreover, they show enjoyment while so occupied and are motivated to further choice making. At the beginning of this chapter, the opinion was expressed that every step on the way to having more control over our lives is worth taking. In the case of these children, opportunity to exert control, however limited, appears to be leading to increased motivation and increasing self-regulation." (Beryl Smith 1994)(Page 5)
"From her work, Glenn (1987) suggests that if learners with PMLD are not given opportunities to act on their environment, because of their multiple difficulties, they will be severely restricted in their cognitive development." (Lacey 2015b)
In most countries, where post-school education is available for IEPMLD, only a limited period is available (typically one to three years) for study. In some places there is discrimination between what is available to young people who have no such learning disability and those who do: for example, an IEPMLD may only be funded in F.E. for a single year at a time whereas any other 'student' may be following a particular course that requires three or more years of work and funding. While such funding may be on some form of governmental 'loan' basis to be repaid as and when the student gains employment and reaches a specified salary level, why should an IEPMLD not be given the same access to funding on the same terms? While it is undoubtedly true that the funding required for an IEPMLD per annum is greater than that of a 'standard' student (if such a person exists) it only means there is more for the student to repay should the student obtain employment and achieve the threshold salary. While one law for one person and a different law for another is, by definition, discriminatory, some might reasonably argue that the standard student cannot access the amount of funding demanded by the IEPMLD curriculum and, thus, such a system actually favours the IEPMLD Learner.
Of course, by definition, an IEPMLD (post school age) is extremely unlikely to be following a vocational pathway nor is it at all likely that this Learner will be taking a higher academic route. What is the likely outcome for an IEPMLD following a course of post-school educational provision? Typically this will involve one or more of the following:
Many years ago I began to use the term 'POSE' to refer to the 'Politics Of Special Education'. There is typically a current POSE in vogue in any country, each with (at least) a slight variation on that of others. Countries may look to the POSEs of others as a source of inspiration and guidance. Such POSEs evolve over time, with one superseding the previous incarnation and each is usually accompanied by its own form of acceptable 'politically correct' vernacular. However, whatever POSE happens to be fashionable, good educational practice tends to remain fairly constant: The underlying targets and objectives of the education of IEPMLD at Further Education (since the period when FE became available for this group of Learners) have always been a focus on preparation for future life. For TalkSense, that has long invoked an understanding that 'the Goal is Control'.
The Goal is Control does not relate to control of Learners by Significant Others (Family, teachers, Therapists, etc) but rather of control by Learners over:
Thus, the goal of further education, with reference to the IEPMLD, is to provide a learning environment that will promote the development of greater Learner control. A greater ability to control one's life is directly proportional to a higher quality of life (see the work of Michael Wehmeyer on self determinism and Learning Difficulty, for example). If we were to watch a film in which a person lacks control over each and every aspect of their life with all control being in the hands of an other (or others) then we would undoubtedly surmise it was a film about a totalitarian state, or a prisoner, or some equally undesirable situation. It is unlikely that it would be considered to be a good state of affairs if someone else decided when and what another can eat, when another must sleep and rise in the morning, what another will be allowed to wear, and what another may and may not do each and every day. Thus, the more control we can exert over what we do and how we do it is a primary factor in how we value our existence:
"... for we know that young people with disabilities who are more self-determined achieve better employment and independent living outcomes and report a higher quality of life." (Wehmeyer M.L. 2014, page 183)
It should be noted that Wehmeyer does not see self-determinism as equating with control (see for example: https://www.youtube.com/watch?v=l5-IxjBA0TQ )
(Gray and Ridden 1999)
"People with disabilities are more visible and more vocal than ever before, and they are increasingly demanding more control and choice in their lives."
(Field, Martin, Miller, Ward, & Wehmeyer 1998 page 11)
"Students become empowered by taking control of their own learning." (Sutcliffe 1990 page 13)
"Good quality support is to do with giving people power."
(Virginia Moffat 1996 page 37)
"a high quality of life is one in which people receive individually tailored support to become full participants in the life of the community, develop skills and independence, be given appropriate choice and control over their lives, be treated with respect in a safe and secure environment”. (Emerson et al 1996)
"Empowerment occurs when control, or power, is passed to an individual or group. In rehabilitation, medicine, social work, psychology, education, and many allied disciplines, it is gradually becoming recognized that the healthiest and most effective individuals have personal control and make decisions for themselves with advice and input from others. The belief here is that, for best results overall, final decisions should be made by the individuals who are most closely affected by the decisions." (Brown and Brown 2003 page 227)
"Independence for this specific group of children means providing them with the opportunity to exercise more control over their own existence, over their environment and over the things that happen to each individual child." (van der Putten, 2005, page 49)
"... with profound multiple disabilities, because of their prevailing disabilities, are totally dependent on their direct support persons in all daily tasks. Therefore, activities offered to children with PMD should be aimed at enhancing their independence and control over their own lives."
(Van der Putten et al, 2005b)
"Choice can be viewed as a key component of empowerment where individuals maintain control over their own lives and as such increase their ability to influence their future goals and ideals." (Bradley 2012)
Generally speaking, the more independent people are and the less external control they receive from others, the more satisfied they are (higher quality of life) (See Legault 1992).Thus, a fundamental goal of all special education should be equipping Learners to live as independent a life as possible. This has long been recognised:
"... citizens with a mental retardation have a right to receive such individual habilitation as will give each of them a realistic opportunity to lead a more useful and meaningful life and to return to society." (Bannerman, Sheldon, Sherman, & Harchik 1990)
"even children with profound learning difficulties , given suitable conditions provided by modern technology, can make choices; in this case between sounds, voices, and rhymes provided on speakers. Moreover, they show enjoyment while so occupied and are motivated to further choice making. At the beginning of this chapter, the opinion was expressed that every step on the way to having more control over our lives is worth taking. In the case of these children, opportunity to exert control, however limited, appears to be leading to increased motivation and increasing self-regulation." (Beryl Smith 1994)(Page 5)
"From her work, Glenn (1987) suggests that if learners with PMLD are not given opportunities to act on their environment, because of their multiple difficulties, they will be severely restricted in their cognitive development." (Lacey 2015b)
In most countries, where post-school education is available for IEPMLD, only a limited period is available (typically one to three years) for study. In some places there is discrimination between what is available to young people who have no such learning disability and those who do: for example, an IEPMLD may only be funded in F.E. for a single year at a time whereas any other 'student' may be following a particular course that requires three or more years of work and funding. While such funding may be on some form of governmental 'loan' basis to be repaid as and when the student gains employment and reaches a specified salary level, why should an IEPMLD not be given the same access to funding on the same terms? While it is undoubtedly true that the funding required for an IEPMLD per annum is greater than that of a 'standard' student (if such a person exists) it only means there is more for the student to repay should the student obtain employment and achieve the threshold salary. While one law for one person and a different law for another is, by definition, discriminatory, some might reasonably argue that the standard student cannot access the amount of funding demanded by the IEPMLD curriculum and, thus, such a system actually favours the IEPMLD Learner.
Of course, by definition, an IEPMLD (post school age) is extremely unlikely to be following a vocational pathway nor is it at all likely that this Learner will be taking a higher academic route. What is the likely outcome for an IEPMLD following a course of post-school educational provision? Typically this will involve one or more of the following:
- Living at home with family;
- Living in specialist provision with 'round-the-clock' care and support;
- Occasional periods of respite care;
- Regular (or irregular) visits for therapy provision (Physiotherapy, occupational therapy, speech and language therapy, hydrotherapy, rebound therapy, other);
- Regular (or irregular) visits for health and welfare support (nurse, doctor, clinic, hospital, consultant, psychologist, other);
- Accessing specialist provision during the day provided by the local authority or a charity for a number of days during any week;
- Supported access to the local community where provision can accommodate the specific requirements of the Individual;
- Supported access to leisure activities where such provision can accommodate the specific requirements of the Individual;
- Occasional variations on the above as the Individual 'transitions' through placements as a result of a change in circumstances, funding, health and welfare issues, etc.
- Occasional variations on above as the individual moves locations (family may move home, Individual may go on a 'holiday' or have to go into hospital, a regular provision may no longer be available, etc.)
- Funding for the above provided through private (family?), charitable, or official (governmental) sources.
Many years ago I began to use the term 'POSE' to refer to the 'Politics Of Special Education'. There is typically a current POSE in vogue in any country, each with (at least) a slight variation on that of others. Countries may look to the POSEs of others as a source of inspiration and guidance. Such POSEs evolve over time, with one superseding the previous incarnation and each is usually accompanied by its own form of acceptable 'politically correct' vernacular. However, whatever POSE happens to be fashionable, good educational practice tends to remain fairly constant: The underlying targets and objectives of the education of IEPMLD at Further Education (since the period when FE became available for this group of Learners) have always been a focus on preparation for future life. For TalkSense, that has long invoked an understanding that 'the Goal is Control'.
The Goal is Control does not relate to control of Learners by Significant Others (Family, teachers, Therapists, etc) but rather of control by Learners over:
- Choice (choosing what to wear, what to eat and drink, where to go, what to do ...)
- Others (letting others know what I want);
- N-vironment (environment - having some independent control over the environment through the use of modern technology)
- Timing (when to do something and for how long);
- Routine (Controlling how often something is repeated for example);
- Own Objectives (I set my own objectives they are not always selected for me by others in my 'best interest');
- Leisure (This is what I like and this is how I like to do it).
Thus, the goal of further education, with reference to the IEPMLD, is to provide a learning environment that will promote the development of greater Learner control. A greater ability to control one's life is directly proportional to a higher quality of life (see the work of Michael Wehmeyer on self determinism and Learning Difficulty, for example). If we were to watch a film in which a person lacks control over each and every aspect of their life with all control being in the hands of an other (or others) then we would undoubtedly surmise it was a film about a totalitarian state, or a prisoner, or some equally undesirable situation. It is unlikely that it would be considered to be a good state of affairs if someone else decided when and what another can eat, when another must sleep and rise in the morning, what another will be allowed to wear, and what another may and may not do each and every day. Thus, the more control we can exert over what we do and how we do it is a primary factor in how we value our existence:
"... for we know that young people with disabilities who are more self-determined achieve better employment and independent living outcomes and report a higher quality of life." (Wehmeyer M.L. 2014, page 183)
It should be noted that Wehmeyer does not see self-determinism as equating with control (see for example: https://www.youtube.com/watch?v=l5-IxjBA0TQ )
"Self-determined people are, in essence, actors in their own lives, rather than being acted upon." (Wehmeyer & Abery 2013, page 399)
Wehmeyer sees self determinism as something more specific than control although, I think he would agree it is a fundamental feature such that, while a person can be said to possess self-determinism but not be fully in control, it could never be said that a person could be fully in control without possessing self-determinism. It would not serve any purpose to go into a debate here on semantics. However, if we accept Wehmeyer's assertion that self-determinism is something different from that of control, it does not follow that the goal is altered: The goal remains control. Then, in order to move towards the goal, we must necessarily see self-determinism as a milestone marking a significant achievement along the route. Will control ever be a feature of the life of an IEPMLD? Almost by definition, a person having such a level of control could not be classified as experiencing PMLD. However, simply because the goal is lofty does not make it inappropriate; it remains something towards which we should continue to strive, constantly improving the quality of life for those individuals experiencing significant learning difficulties.
Control should not be confused with an ability to do it yourself which, for perhaps a large number of IEPMLD, may not be possible because of associated physical disabilities (to cite just one reason):
"When self-determination is interpreted strictly to mean ‘doing it yourself’, there is an obvious problem for people with significant disabilities,many of whom may have limits to the number and types of activities they can perform independently."
Michael Wehmeyer (1998 page 65)
Control can mean pointing out to others (by any means available) what is wanted such that the 'others' act, at your behest, on your behalf, rather than acting in what they assume to be in the best interest of the individual, or in the interests of some externally imposed curriculum or agenda.
The promotion of control in young people with disabilities should be seen as best practice in both secondary education, further education, and any transitional service (Field, Martin, Miller, Ward, & Wehmeyer, 1998; Wehmeyer, Abery, Mithaug, & Stancliffe, 2003; Wehmeyer et al., 2007). The development of control may be viewed as best practice because it is directly related to:
What does 'control' mean if we accept that it is the goal? In gradually relinquishing control to Learners staff need to 'sail the seven seas' (or, in this case, the seven C's), that is, control can be broken down into target areas, each of which plays its part in the provision of a higher quality of life. The seven C's are as illustrated below:
Wehmeyer sees self determinism as something more specific than control although, I think he would agree it is a fundamental feature such that, while a person can be said to possess self-determinism but not be fully in control, it could never be said that a person could be fully in control without possessing self-determinism. It would not serve any purpose to go into a debate here on semantics. However, if we accept Wehmeyer's assertion that self-determinism is something different from that of control, it does not follow that the goal is altered: The goal remains control. Then, in order to move towards the goal, we must necessarily see self-determinism as a milestone marking a significant achievement along the route. Will control ever be a feature of the life of an IEPMLD? Almost by definition, a person having such a level of control could not be classified as experiencing PMLD. However, simply because the goal is lofty does not make it inappropriate; it remains something towards which we should continue to strive, constantly improving the quality of life for those individuals experiencing significant learning difficulties.
Control should not be confused with an ability to do it yourself which, for perhaps a large number of IEPMLD, may not be possible because of associated physical disabilities (to cite just one reason):
"When self-determination is interpreted strictly to mean ‘doing it yourself’, there is an obvious problem for people with significant disabilities,many of whom may have limits to the number and types of activities they can perform independently."
Michael Wehmeyer (1998 page 65)
Control can mean pointing out to others (by any means available) what is wanted such that the 'others' act, at your behest, on your behalf, rather than acting in what they assume to be in the best interest of the individual, or in the interests of some externally imposed curriculum or agenda.
The promotion of control in young people with disabilities should be seen as best practice in both secondary education, further education, and any transitional service (Field, Martin, Miller, Ward, & Wehmeyer, 1998; Wehmeyer, Abery, Mithaug, & Stancliffe, 2003; Wehmeyer et al., 2007). The development of control may be viewed as best practice because it is directly related to:
- the attainment of enhanced academic and transition outcomes (Fowler, Konrad, Walker, Test, & Wood, 2007; Konrad, Fowler, Walker, Test, & Wood, 2007; Lee, Wehmeyer, Soukup, & Palmer, 2010);
- more positive employment and independent living (Martorell, Gutierrez-Recacha, Pereda, & Ayuso-Mateos, 2008; Wehmeyer & Palmer, 2003; Wehmeyer & Schwartz, 1997);
- improved recreation and leisure outcomes (McGuire & McDonnell, 2008);
- greater quality of life and life satisfaction (Wehmeyer & Schwartz, 1998; Lachapelle et al., 2005; Shogren, Lopez, Wehmeyer, Little, & Pressgrove, 2006; Nota, Ferrari, Soresi, & Wehmeyer, 2007; Schalock and Verdugo 2002, 2012 ).
What does 'control' mean if we accept that it is the goal? In gradually relinquishing control to Learners staff need to 'sail the seven seas' (or, in this case, the seven C's), that is, control can be broken down into target areas, each of which plays its part in the provision of a higher quality of life. The seven C's are as illustrated below:
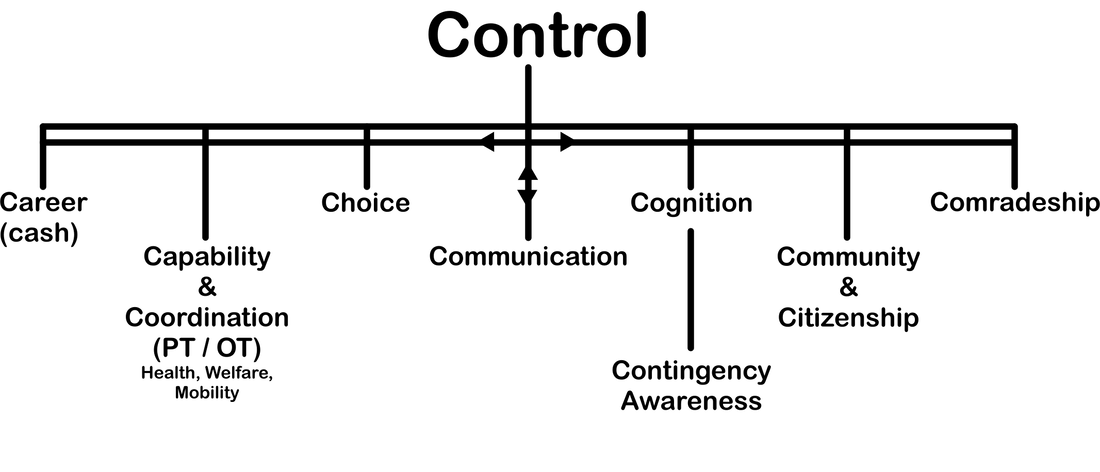
Career
Career does not necessarily equate to employment; indeed, it is unlikely that IEPMLD will move on to paid employment. However, here 'career' refers to a possible future direction. Having some control over that direction is important: When others decide on such matters on your behalf it is their idea of what a good life should be for someone like you, it is not necessarily what you might decide for yourself given some control. Career also refers to some control over cash. Typically those with primary responsibility for individuals (parents, close relatives, significant others, ...) don't always pay (control the finance) for necessary service provision (this may come directly out of other budgets such as local councils or government agencies). If you are paying for a service directly you are controlling it, you have a better say in the quality of provision for, if you find that wanting, you can stop paying. Whereas, if the payment come directly from government or some other source, once a decision on service provision has been made it is more difficult for primary carers to influence the standard. If governments were to provide funding for primary carers and primary carers made decisions on provision in the best interest of their family member:
Capability and Coordination
Typically this refers to the services provided by the therapy departments; the Physiotherapists, the Occupational Therapists and the Speech and Language Therapists. However, in addition to the therapy services, there is much that can be done by teaching and support staff in improving both an individual's capability (in one or more areas) and coordination. These areas will be addressed in other sections on this webpage. Also included under the banner of capability and coordination are the areas of health, welfare, and mobility.
Choice
Choice is a voice. As such, it is a fundamental feature in exerting control. Choice is a fundamental human right. Aspects of choice will feature significantly on this webpage.
"... often have very little opportunity of exercising any choice in their life-style; it is very easy for an adult to govern their lives completely. We choose to feed them when we consider that they should be hungry; we put them to rest when we consider that they should be tired; we place them in front of the television and expect them to watch what we choose for them." (Clark, 1991, page 18)
"The more opportunities there are for individuals to make meaningful choices, the more control they will experience." (Agran et al, 2010)(See also Mithaug & Mithaug 2003).
Communication
Communication is at the heart of the diagram for a reason; it is a foundational feature in creating control. Thus, post-sixteen education should be doing all it can to develop communicative abilities in IEPMLD. Aspects of communication practice will feature throughout this webpage.
Cognition (including Contingency Awareness)
Improving awareness of self and of the world immediately surrounding and impacting on the self is fundamental to a person taking some control. The more that can be done to ameliorate the cognitive condition of the Learner the more able the Learner will be to comprehend and control events as they occur.
"If we have discovered the learner with PMLD is beginning to learn about 'contingency awareness' then that should become central to all their learning. School children may be working on a range of curriculum activities and adult learners are likely to be involved in a range of community activities but what is required for all at this stage is for teachers and supporters to provide as many opportunities as possible to practice contingency awareness. This should be done throughout the day, preferably with a range of different resources so the person can learn to generalise his/her understanding in many different situations." (Lacey, 2015, page 45)
Community and Citizenship
IEPMLD should not be shut way from their community, they should be part of it. The IEPMLD will benefit from access to the community and the community will benefit from such access. Those experiencing PMLD should be able to take advantage of all that their community has to offer to make the most of their leisure time. They should not be shut away in some hide away establishment but seen out and about enjoying the services and provisions of their local community. Likewise the local community should get to know and understand the abilities, needs and requirements of IEPMLD; it is a reciprocal relationship. IEPMLD should be citizens of their community, championed and respected by all people.
Comradeship
Friendship is important to us all: Some might say it is the most important part of our lives. Should black people only associate with black people? Should Catholics only associate with Catholics? Hindus with Hindus? Muslims with Muslims? Women with women? Of course not! Then why should IEPMLD only associate with IEPMLD? Friendship should transcend colour, race, religion, sex, and cognitive ability. Marginalising those that are somehow perceived as different only serves to reinforce stereotypes and distrust. IEMPLD need friends too and not just other people who may happen to have a learning difficulty but friends from all walks of life. However, being 'ghettoed' in daily provision that only allows for meetings with like people (and their supporting staff) does not necessarily permit the blossoming of such frienships unless such establishments actively work to to prevent social isolation of this group of people.
Control is important:
"Researchers arranged for student volunteers to pay regular visits to nursing-home residents. Residents in the high-control group were allowed to control the timing and duration of the student's visits ("Please come visit me next Thursday for an hour'), and residents in the low-control group were not (I'll come vist you next Thursday for an hour"). After two months, residents in the high-control group were happier, healthier, more active, and taking fewer medications than those in the low-control group." (Gilbert 2006 detailing Schulz & Hanusa's 1978 study)
To be completed .... XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
Career does not necessarily equate to employment; indeed, it is unlikely that IEPMLD will move on to paid employment. However, here 'career' refers to a possible future direction. Having some control over that direction is important: When others decide on such matters on your behalf it is their idea of what a good life should be for someone like you, it is not necessarily what you might decide for yourself given some control. Career also refers to some control over cash. Typically those with primary responsibility for individuals (parents, close relatives, significant others, ...) don't always pay (control the finance) for necessary service provision (this may come directly out of other budgets such as local councils or government agencies). If you are paying for a service directly you are controlling it, you have a better say in the quality of provision for, if you find that wanting, you can stop paying. Whereas, if the payment come directly from government or some other source, once a decision on service provision has been made it is more difficult for primary carers to influence the standard. If governments were to provide funding for primary carers and primary carers made decisions on provision in the best interest of their family member:
- primary carers would ensure standards (or remove funding from the chosen establishment);
- Government would save money because it would not have to employ inspectors to ensure quality of provision;
- provision would have to work to attract potential clients to their service.
- good provision would be profitable, poor provision would go out of business.
Capability and Coordination
Typically this refers to the services provided by the therapy departments; the Physiotherapists, the Occupational Therapists and the Speech and Language Therapists. However, in addition to the therapy services, there is much that can be done by teaching and support staff in improving both an individual's capability (in one or more areas) and coordination. These areas will be addressed in other sections on this webpage. Also included under the banner of capability and coordination are the areas of health, welfare, and mobility.
Choice
Choice is a voice. As such, it is a fundamental feature in exerting control. Choice is a fundamental human right. Aspects of choice will feature significantly on this webpage.
"... often have very little opportunity of exercising any choice in their life-style; it is very easy for an adult to govern their lives completely. We choose to feed them when we consider that they should be hungry; we put them to rest when we consider that they should be tired; we place them in front of the television and expect them to watch what we choose for them." (Clark, 1991, page 18)
"The more opportunities there are for individuals to make meaningful choices, the more control they will experience." (Agran et al, 2010)(See also Mithaug & Mithaug 2003).
Communication
Communication is at the heart of the diagram for a reason; it is a foundational feature in creating control. Thus, post-sixteen education should be doing all it can to develop communicative abilities in IEPMLD. Aspects of communication practice will feature throughout this webpage.
Cognition (including Contingency Awareness)
Improving awareness of self and of the world immediately surrounding and impacting on the self is fundamental to a person taking some control. The more that can be done to ameliorate the cognitive condition of the Learner the more able the Learner will be to comprehend and control events as they occur.
"If we have discovered the learner with PMLD is beginning to learn about 'contingency awareness' then that should become central to all their learning. School children may be working on a range of curriculum activities and adult learners are likely to be involved in a range of community activities but what is required for all at this stage is for teachers and supporters to provide as many opportunities as possible to practice contingency awareness. This should be done throughout the day, preferably with a range of different resources so the person can learn to generalise his/her understanding in many different situations." (Lacey, 2015, page 45)
Community and Citizenship
IEPMLD should not be shut way from their community, they should be part of it. The IEPMLD will benefit from access to the community and the community will benefit from such access. Those experiencing PMLD should be able to take advantage of all that their community has to offer to make the most of their leisure time. They should not be shut away in some hide away establishment but seen out and about enjoying the services and provisions of their local community. Likewise the local community should get to know and understand the abilities, needs and requirements of IEPMLD; it is a reciprocal relationship. IEPMLD should be citizens of their community, championed and respected by all people.
Comradeship
Friendship is important to us all: Some might say it is the most important part of our lives. Should black people only associate with black people? Should Catholics only associate with Catholics? Hindus with Hindus? Muslims with Muslims? Women with women? Of course not! Then why should IEPMLD only associate with IEPMLD? Friendship should transcend colour, race, religion, sex, and cognitive ability. Marginalising those that are somehow perceived as different only serves to reinforce stereotypes and distrust. IEMPLD need friends too and not just other people who may happen to have a learning difficulty but friends from all walks of life. However, being 'ghettoed' in daily provision that only allows for meetings with like people (and their supporting staff) does not necessarily permit the blossoming of such frienships unless such establishments actively work to to prevent social isolation of this group of people.
Control is important:
"Researchers arranged for student volunteers to pay regular visits to nursing-home residents. Residents in the high-control group were allowed to control the timing and duration of the student's visits ("Please come visit me next Thursday for an hour'), and residents in the low-control group were not (I'll come vist you next Thursday for an hour"). After two months, residents in the high-control group were happier, healthier, more active, and taking fewer medications than those in the low-control group." (Gilbert 2006 detailing Schulz & Hanusa's 1978 study)
To be completed .... XXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXXX
- choice-making skills;
- decision-making skills;
- goal setting and attainment skills;
- self-advocacy skills;
- problem-solving skills;
- self-awareness skills.
4. Consistency, Clarity, Cooperation, Calm, Care, Caution, Challenge, Checks, Chuckles, and Carrots, ... in the Curriculum

While the above section deals with Control and the Seven C's, there are of course many more C's to take into consideration. The difference is perhaps that these C's are not curricular areas but rather characteristics of good practice flowing through all areas of the curriculum. While most are self- explanatory, it may be worthwhile taking a little time and web space to cover a few here. They are covered in alphabetical order:
Calm
I don't know about you but I require a very peaceful atmosphere in order just to be able to read. If there is loud music playing or someone is running about wildly it is so distracting that I find I am reading the same line over and over again and still not taking it in. If this is true for me then it must hold a greater truth for IEPMLD. People working in cramped (too near too other Learners), noisy, extremely busy (lots of distractions), and frequently interrupted sessions are not placed in the best position to be able to learn. Seek and provide calm!
Care
Carrots
Carrots here is used to refer to motivational items for individual Learners. Each Learner will have at least one BEST (Best Ever Stimulating Thing) that may be used as an incentive in the classroom and beyond. BESTs are address in a separate area on this webpage.
Caution
Challenge
Checks
Chuckles
Clarity
Consistency, Constancy, and Continuity
"For people who have severe learning difficulties, consistency and continuity of approach is necessary." (Aitken & Buultjens, 1992, page 49).
"Learners with PMLD are likely to have great difficulty with memory, with perhaps some having virtually no memory at all, meaning every person and activity they experience is as if for the first time, every time. Thus learners with PMLD require an enormous amount of repetition to learn." (Lacey, 2009, page 18)
Consistency, Constancy (in the example above, repetition), and Continuity are vitally important in this area of education. For example, in order that an Objects Of Reference scheme should provide the greatest level of support for learning, the approach must be repeatedly applied, in a consistent manner, over a long period of time.
Cooperation
Teachers, Speech and Language Therapists, Occupational Therapists, Physiotherapists, Psychologists and other professional bodies of people all meet together within special education and yet they may not all 'come together'. While they may all have particular specialisms, to be told that a particular aspect of learning/provision is the role of a particular person on the team, and should not be addressed by others, is counter productive. We need to cooperate, working together such that every one is a physiotherapist, everyone is a teacher, everyone is a speech therapist,... (or, at least, a physiotherapy assistant, a teaching assistant, a SLT assistant ...).
"Where specialist therapies are in use, it may be difficult to see beyond the therapy. Even though only a few simple changes may be required to working practices, in order for that therapy to be integrated into a wider sphere of objectives." (Aitken & Buultjens 1992, page 49)
Such practice (cooperation) should not be seen as 'challenging' to the therapists or the teachers but, rather, empowering: it is not aiming to 'do away' with need for the professionals nor indeed to devalue their contribution in any way. On the contrary, it seeks to empower this group by providing them with control over a team of para-professionals who can be directed and learn from them to the benefit of all in their charge:
"As someone who leads a team, you’ll be used to being the decision-maker, problem-solver, planner, manager and instructor. In short, you’re normally the one who’s in control. So, empowering others is no doubt very different from what you are used to doing. It means handing over much of this control, along with many associated responsibilities, to your team. If you’re new to empowerment, it’s only natural to feel a little anxious about this. You might feel that your role will become redundant. In fact, it’s quite the opposite – your team needs you more than ever!
You may have handed over a great deal of control, but you’re still ultimately responsible for the work of the team. Just because you’ve given power to others doesn’t mean that you’ve lost it yourself. You’re still the one who defines the goals and boundaries, and your team will still look to you for support, guidance and encouragement. In fact, empowering your team will leave you free to concentrate on new and exciting responsibilities ..." (University of Aberdeen, 2017, https://www.abdn.ac.uk/develop/managers/empowering-your-team-307.php)
Calm
I don't know about you but I require a very peaceful atmosphere in order just to be able to read. If there is loud music playing or someone is running about wildly it is so distracting that I find I am reading the same line over and over again and still not taking it in. If this is true for me then it must hold a greater truth for IEPMLD. People working in cramped (too near too other Learners), noisy, extremely busy (lots of distractions), and frequently interrupted sessions are not placed in the best position to be able to learn. Seek and provide calm!
Care
Carrots
Carrots here is used to refer to motivational items for individual Learners. Each Learner will have at least one BEST (Best Ever Stimulating Thing) that may be used as an incentive in the classroom and beyond. BESTs are address in a separate area on this webpage.
Caution
Challenge
Checks
Chuckles
Clarity
Consistency, Constancy, and Continuity
"For people who have severe learning difficulties, consistency and continuity of approach is necessary." (Aitken & Buultjens, 1992, page 49).
"Learners with PMLD are likely to have great difficulty with memory, with perhaps some having virtually no memory at all, meaning every person and activity they experience is as if for the first time, every time. Thus learners with PMLD require an enormous amount of repetition to learn." (Lacey, 2009, page 18)
Consistency, Constancy (in the example above, repetition), and Continuity are vitally important in this area of education. For example, in order that an Objects Of Reference scheme should provide the greatest level of support for learning, the approach must be repeatedly applied, in a consistent manner, over a long period of time.
Cooperation
Teachers, Speech and Language Therapists, Occupational Therapists, Physiotherapists, Psychologists and other professional bodies of people all meet together within special education and yet they may not all 'come together'. While they may all have particular specialisms, to be told that a particular aspect of learning/provision is the role of a particular person on the team, and should not be addressed by others, is counter productive. We need to cooperate, working together such that every one is a physiotherapist, everyone is a teacher, everyone is a speech therapist,... (or, at least, a physiotherapy assistant, a teaching assistant, a SLT assistant ...).
"Where specialist therapies are in use, it may be difficult to see beyond the therapy. Even though only a few simple changes may be required to working practices, in order for that therapy to be integrated into a wider sphere of objectives." (Aitken & Buultjens 1992, page 49)
Such practice (cooperation) should not be seen as 'challenging' to the therapists or the teachers but, rather, empowering: it is not aiming to 'do away' with need for the professionals nor indeed to devalue their contribution in any way. On the contrary, it seeks to empower this group by providing them with control over a team of para-professionals who can be directed and learn from them to the benefit of all in their charge:
"As someone who leads a team, you’ll be used to being the decision-maker, problem-solver, planner, manager and instructor. In short, you’re normally the one who’s in control. So, empowering others is no doubt very different from what you are used to doing. It means handing over much of this control, along with many associated responsibilities, to your team. If you’re new to empowerment, it’s only natural to feel a little anxious about this. You might feel that your role will become redundant. In fact, it’s quite the opposite – your team needs you more than ever!
You may have handed over a great deal of control, but you’re still ultimately responsible for the work of the team. Just because you’ve given power to others doesn’t mean that you’ve lost it yourself. You’re still the one who defines the goals and boundaries, and your team will still look to you for support, guidance and encouragement. In fact, empowering your team will leave you free to concentrate on new and exciting responsibilities ..." (University of Aberdeen, 2017, https://www.abdn.ac.uk/develop/managers/empowering-your-team-307.php)
5. Preference Not Deference: Age Appropriateness

"Whatever level of involvement we are considering, it is important to recall that normalization philosophy has emphasized that the activities in which we engage people should be seen to be appropriate to their age. However, since choice is at the heart of leisure, many will be aware that our judgement of age-appropriateness may on occasion clash with a person's choice of activity. Some professionals in this situation, whose commitment to normalization is paramount, would urge that ensuring age-appropriateness should take priority over choice, and an activity should be denied or substituted with a less preferred but age-appropriate one." (Hogg, 1995, page 45)
Choice is not an option (see section below) and therefore cannot be overruled by age-appropriateness as noted by Hogg (op.cit.) above. A good guide to best practice in this area is the use of the mnemonic 'preference not deference'
"While age-appropriateness and developmental appropriateness are both important concerns, maybe we should concentrate more on what is ‘person-appropriate’" (Smith, 1996, page 79).
" ... stating that of course the chronological age of a person is one of the aspects of the person to be addressed in our education and care. However, we must not allow this issue to become paramount over the need to give regard to where the person is ‘at’ developmentally, psychologically, emotionally and communicatively. Additionally, people of whatever age can want or need physical stimulation and support." (Hewett, 2007, page 121)
"The storytelling has generated much discussion on what is age-appropriate material - for example, at what age, if any, do fairy tales become inappropriate?" (Birch et al., 2000, page 4)
"A principle operating in services throughout Australia, the UK, and the USA is that of age-appropriateness. The principle of age-appropriateness is widespread throughout government policy and non-government practice guidelines, but the exact meaning of the term is rarely defined. It is commonly assumed to mean activities and approaches commensurate with an individual’s chronological age. Dress, furnishing, object selection, and the style of interactions, are all supposed to be age-appropriate, according to many policies. However, when this principle is applied to people with profound intellectual and multiple disabilities, I argue that instead of promoting a good life, the principle contributes to practices that compromise individuals’ health, well-being, quality of life, and their human rights." (Forster, 2010, page 129)
Everyone reading this webpage probably has something that they like to do which is not particularly age appropriate. For example, I must admit to both watching and enjoying 'Sponge Bob Square Pants' from time to time. A friend admits to taking a pink rabbit with her to bed. The issue is that we chose to like doing these things, they are our preferences. We did not defer to some other person's choice on our behalf (deference). Had I been given no choice and had to learn Mandarin from staff utilising Sponge Bob cartoons when I had never seen him before or had my friend been lectured on the curriculum in special education by use of a pink rabbit then we might have questioned the (age) appropriateness. Actually, while working in Taiwan and trying to learn some Mandarin, I did watch children's cartoons because I thought that the language might be simpler for me to understand. However, again, it was by my choice and my preference. There have been several studies and many papers concerning the use of dolls as therapy with older people with dementia that highlight the positive outcomes of such an approach and which reflect and reinforce the notions made in the quote by Forster above (for a review of doll therapy see Turner and Shepherd 2014). However, the dolls are not imposed on the individuals. Indeed, Ellingford et al. (2007) argue that dolls should be introduced indirectly by leaving dolls in communal areas and on chairs, to allow for freedom of choice and free interaction.
In relation to best practice therefore, the use of supporting resources should relate to Learner preferences: Learners should not have to defer to another's choice that is not age appropriate. Thus, for example, a Sensory Story told to a young adult might involve a doll (as in the cartoon) if that person has a preference for dolls. As dolls are this particular Learner's B.E.S.T. (Best Ever Stimulating Thing) their use in the Sensory Story might help to captivate and engage the Learner in the process. B.E.S.T. practice, by definition, is highly motivating and may therefore be used to illustrate a story without fear of accusations of age inappropriateness (although unenlightened individuals might claim otherwise!).
'Preference not deference' therefore relates to an individual's free choice of materials in use in an educational setting. Items that are Learner preference (and not imposed by deference to a staff member) should not be seen to be age inappropriate.
Choice is not an option (see section below) and therefore cannot be overruled by age-appropriateness as noted by Hogg (op.cit.) above. A good guide to best practice in this area is the use of the mnemonic 'preference not deference'
"While age-appropriateness and developmental appropriateness are both important concerns, maybe we should concentrate more on what is ‘person-appropriate’" (Smith, 1996, page 79).
" ... stating that of course the chronological age of a person is one of the aspects of the person to be addressed in our education and care. However, we must not allow this issue to become paramount over the need to give regard to where the person is ‘at’ developmentally, psychologically, emotionally and communicatively. Additionally, people of whatever age can want or need physical stimulation and support." (Hewett, 2007, page 121)
"The storytelling has generated much discussion on what is age-appropriate material - for example, at what age, if any, do fairy tales become inappropriate?" (Birch et al., 2000, page 4)
"A principle operating in services throughout Australia, the UK, and the USA is that of age-appropriateness. The principle of age-appropriateness is widespread throughout government policy and non-government practice guidelines, but the exact meaning of the term is rarely defined. It is commonly assumed to mean activities and approaches commensurate with an individual’s chronological age. Dress, furnishing, object selection, and the style of interactions, are all supposed to be age-appropriate, according to many policies. However, when this principle is applied to people with profound intellectual and multiple disabilities, I argue that instead of promoting a good life, the principle contributes to practices that compromise individuals’ health, well-being, quality of life, and their human rights." (Forster, 2010, page 129)
Everyone reading this webpage probably has something that they like to do which is not particularly age appropriate. For example, I must admit to both watching and enjoying 'Sponge Bob Square Pants' from time to time. A friend admits to taking a pink rabbit with her to bed. The issue is that we chose to like doing these things, they are our preferences. We did not defer to some other person's choice on our behalf (deference). Had I been given no choice and had to learn Mandarin from staff utilising Sponge Bob cartoons when I had never seen him before or had my friend been lectured on the curriculum in special education by use of a pink rabbit then we might have questioned the (age) appropriateness. Actually, while working in Taiwan and trying to learn some Mandarin, I did watch children's cartoons because I thought that the language might be simpler for me to understand. However, again, it was by my choice and my preference. There have been several studies and many papers concerning the use of dolls as therapy with older people with dementia that highlight the positive outcomes of such an approach and which reflect and reinforce the notions made in the quote by Forster above (for a review of doll therapy see Turner and Shepherd 2014). However, the dolls are not imposed on the individuals. Indeed, Ellingford et al. (2007) argue that dolls should be introduced indirectly by leaving dolls in communal areas and on chairs, to allow for freedom of choice and free interaction.
In relation to best practice therefore, the use of supporting resources should relate to Learner preferences: Learners should not have to defer to another's choice that is not age appropriate. Thus, for example, a Sensory Story told to a young adult might involve a doll (as in the cartoon) if that person has a preference for dolls. As dolls are this particular Learner's B.E.S.T. (Best Ever Stimulating Thing) their use in the Sensory Story might help to captivate and engage the Learner in the process. B.E.S.T. practice, by definition, is highly motivating and may therefore be used to illustrate a story without fear of accusations of age inappropriateness (although unenlightened individuals might claim otherwise!).
'Preference not deference' therefore relates to an individual's free choice of materials in use in an educational setting. Items that are Learner preference (and not imposed by deference to a staff member) should not be seen to be age inappropriate.
6. Choice is not an option
"A third problem involves the limited opportunities for choice. Several studies have demonstrated that people with PIMD lack control over their life situation (Carnaby & Cambridge, 2002; De Waele & Van Hove, 2005; Seifert, 2002), and have few opportunities to make choices regarding everyday activities and major life events." (Maes et al, 2007, page 164)
"The basic human right to choice is mandatory according to the CRPD which was adopted by the United Nations in 2006 and came into force internationally in 2008. To date, 153 nations have signed the Convention and 119 have ratified it. Ratifying nations commit themselves to implement all obligations of the Convention. The CRPD is the first disability-specific international treaty and the first treaty to adopt the human rights approach to disability. Specifically, the CRPD promotes freedom of choice and autonomy, non-discrimination, full participation and inclusiveness in society, respect for the differences evident in persons with disabilities, equality of opportunity, accessibility to core social goods and services, and the identification and removal of barriers."
(Werner, S. 2012. Page 3)
The United Nations Convention on the Rights of People with Disabilities came into force in 2008. It has been signed and ratified by 119 nations including Australia, Canada, New Zealand, and the United Kingdom but, although signed, it has still not been ratified by the USA or Ireland.
In the UK, the CRPD builds further on the MCA (Mental Capacity Act 2005) which came into force in 2007:
"The Mental Capacity Act 2005 is the first piece of legislation to clearly state that people can no longer make decisions on behalf of others without following a process." (Fulton, Woodley, & Sanderson 2008 page 5)
Thus, Choice is not an option, it is mandated by law. However, regrettably, research shows us that there is an inverse relationship between level of disability and the amount of choice provided; that is, the greater the disability the less the choice (Wehmeyer & Garner, 2003; Smith, Morgan & Davidson, 2005; Neely-Barnes, Marcenko, & Weber, 2008).
How should choice for IEPMLD be provided? What does it look like? This section begins to address these questions and further sections to follow later on this page will expand on specific aspects of choice provision as a meaningful activity. Choice is also covered in some depth on its own webpage on this site. Click here to move to the choice page.
When defining choice people typically use words like decide, elect, opt, pick, prefer, and select but these words are simply alternative forms of vocabulary for choice. Thus, the definition becomes something of a tautology: choice equals choice! Defining choice without using words that simply mean choice is not easy. However, TalkSense defines choice as:
"The independent knowledge (understanding, consciousness) that a particular behaviour (action, vocalisation, physical movement, indicating strategy) will lead to (result in, be commensurate with) a specific (desired) result (goal, need fulfillment, attainment) when presented with a set of recognised (known, comprehended), whole (not selecting for a part of or an attribute of), alternatives at a particular point in time."
Here, choice is regarded as a specific observable independent behaviour which has a particular consequence in response to a given range of currently available alternate stimuli. The notion of individual consciousness of the behaviour plays an important role in all aspects of this. The Learner has to be conscious of the:
All of this from an individual whose understanding of the world is limited as a result of his/her condition. The Learner therefore has to be conscious of the situation, each of the alternatives, what is being (t)asked of him/her, his/her response strategy, others understanding of his/her response strategy (theory of mind). Is this really feasible from an Individual Experiencing PMLD?
When a staff member states that a particular individual has 'made a choice', are they really implying all of the above? Are they aware of all of the above and does anyone ever ask them to qualify their statement? What they are likely to be stating is a specific Learner appeared to indicate (in some manner appropriate to the Learner's physical abilities) an item from a range of other items. However, is this a choice?
Knowing what choice means (having a definition) is a way of deciding what issues need to be addressed in teaching Learners to make choices. The clearer the definition the clearer the pathway to the goal. Choice is not just something that happens, it is something that needs to be taught once we are clear exactly what that entails. Choice can be taught:
"As has often been the case, individuals with intellectual or developmental disabilities have not been provided opportunities to make choices and decisions based on their own preferences. Because of this, many individuals do not know how to make choices and need targeted, systematic instruction on this skill. Consequently, much of the choice-making literature has involved demonstrations that individuals with intellectual and severe intellectual disabilities do have preferences and can be taught to make choices based on these preferences." (Agran et al, 2010)
"The positive self esteem that people with PIMD feel, is also linked to the degree of self determination they have. It is of great importance for people with PIMD to feel that they influence and control their life and environment and that they can make choices. Research has demonstrated that people with PIMD are able to make choices (Lancioni, O’Reilly, & Emerson, 1996; Saunders et al., 2005). Support staff is expected to adequately build in options in the daily context and to contingently take advantage of preferences (Browder, Cooper, & Lim, 1998; Cannella, O’Reilly & Lancioni, 2005; Green, Middleton, & Reid, 2000). As a result of the opportunity to make choices the person takes more initiatives and is more actively involved in activities (Cannella, O’Reilly & Lancioni, 2005; Cole & Levinson, 2002; Lancioni, O’Reilly & Emerson, 1996) and problem behavior is reduced (Cannella, O’Reilly & Lancioni, 2005; Lohrmann-O’Rourke, & Yurman, 2001)." (Petry, Maes, & Vlaskamp, 2007c)
"The basic human right to choice is mandatory according to the CRPD which was adopted by the United Nations in 2006 and came into force internationally in 2008. To date, 153 nations have signed the Convention and 119 have ratified it. Ratifying nations commit themselves to implement all obligations of the Convention. The CRPD is the first disability-specific international treaty and the first treaty to adopt the human rights approach to disability. Specifically, the CRPD promotes freedom of choice and autonomy, non-discrimination, full participation and inclusiveness in society, respect for the differences evident in persons with disabilities, equality of opportunity, accessibility to core social goods and services, and the identification and removal of barriers."
(Werner, S. 2012. Page 3)
The United Nations Convention on the Rights of People with Disabilities came into force in 2008. It has been signed and ratified by 119 nations including Australia, Canada, New Zealand, and the United Kingdom but, although signed, it has still not been ratified by the USA or Ireland.
In the UK, the CRPD builds further on the MCA (Mental Capacity Act 2005) which came into force in 2007:
"The Mental Capacity Act 2005 is the first piece of legislation to clearly state that people can no longer make decisions on behalf of others without following a process." (Fulton, Woodley, & Sanderson 2008 page 5)
Thus, Choice is not an option, it is mandated by law. However, regrettably, research shows us that there is an inverse relationship between level of disability and the amount of choice provided; that is, the greater the disability the less the choice (Wehmeyer & Garner, 2003; Smith, Morgan & Davidson, 2005; Neely-Barnes, Marcenko, & Weber, 2008).
How should choice for IEPMLD be provided? What does it look like? This section begins to address these questions and further sections to follow later on this page will expand on specific aspects of choice provision as a meaningful activity. Choice is also covered in some depth on its own webpage on this site. Click here to move to the choice page.
When defining choice people typically use words like decide, elect, opt, pick, prefer, and select but these words are simply alternative forms of vocabulary for choice. Thus, the definition becomes something of a tautology: choice equals choice! Defining choice without using words that simply mean choice is not easy. However, TalkSense defines choice as:
"The independent knowledge (understanding, consciousness) that a particular behaviour (action, vocalisation, physical movement, indicating strategy) will lead to (result in, be commensurate with) a specific (desired) result (goal, need fulfillment, attainment) when presented with a set of recognised (known, comprehended), whole (not selecting for a part of or an attribute of), alternatives at a particular point in time."
Here, choice is regarded as a specific observable independent behaviour which has a particular consequence in response to a given range of currently available alternate stimuli. The notion of individual consciousness of the behaviour plays an important role in all aspects of this. The Learner has to be conscious of the:
- stimuli (alternatives);
- the situation (that a specific action on his/her part will result in one particular response. The other alternative will no longer be available);
- whole (that is the Learner is not selecting on the basis of a portion or characteristic of the whole such as [for example] the colour rather than the drink);
- his/her behaviour and how it will effect an outcome.
All of this from an individual whose understanding of the world is limited as a result of his/her condition. The Learner therefore has to be conscious of the situation, each of the alternatives, what is being (t)asked of him/her, his/her response strategy, others understanding of his/her response strategy (theory of mind). Is this really feasible from an Individual Experiencing PMLD?
When a staff member states that a particular individual has 'made a choice', are they really implying all of the above? Are they aware of all of the above and does anyone ever ask them to qualify their statement? What they are likely to be stating is a specific Learner appeared to indicate (in some manner appropriate to the Learner's physical abilities) an item from a range of other items. However, is this a choice?
Knowing what choice means (having a definition) is a way of deciding what issues need to be addressed in teaching Learners to make choices. The clearer the definition the clearer the pathway to the goal. Choice is not just something that happens, it is something that needs to be taught once we are clear exactly what that entails. Choice can be taught:
"As has often been the case, individuals with intellectual or developmental disabilities have not been provided opportunities to make choices and decisions based on their own preferences. Because of this, many individuals do not know how to make choices and need targeted, systematic instruction on this skill. Consequently, much of the choice-making literature has involved demonstrations that individuals with intellectual and severe intellectual disabilities do have preferences and can be taught to make choices based on these preferences." (Agran et al, 2010)
"The positive self esteem that people with PIMD feel, is also linked to the degree of self determination they have. It is of great importance for people with PIMD to feel that they influence and control their life and environment and that they can make choices. Research has demonstrated that people with PIMD are able to make choices (Lancioni, O’Reilly, & Emerson, 1996; Saunders et al., 2005). Support staff is expected to adequately build in options in the daily context and to contingently take advantage of preferences (Browder, Cooper, & Lim, 1998; Cannella, O’Reilly & Lancioni, 2005; Green, Middleton, & Reid, 2000). As a result of the opportunity to make choices the person takes more initiatives and is more actively involved in activities (Cannella, O’Reilly & Lancioni, 2005; Cole & Levinson, 2002; Lancioni, O’Reilly & Emerson, 1996) and problem behavior is reduced (Cannella, O’Reilly & Lancioni, 2005; Lohrmann-O’Rourke, & Yurman, 2001)." (Petry, Maes, & Vlaskamp, 2007c)
7. Breaking Choice
All special needs establishments take breaks during the day to provide a chance for Learners to access personal care areas and to take a drink. However, not all are treating this period of time as an educational opportunity. Indeed, in terms of IEPMLD, there is no period of time during such an establishment's day that should not be seen as an opportunity to develop skills.
The whole process of break time should be delivered as consistently as is possible such that each Learner begins to anticipate the coming events as they unfold. This recommends (although doesn't necessarily necessitate) a consistency of staff support with each team member fully aware of their role and the provision to be made. Colleges and other establishments may wish to develop their own policy and procedure documentation covering this aspect of the day.
Good practice during break times would dictate that, at least, the following practices are in place:
In order to illustrate such practice let's assume a Learner called James who is an IEPMLD currently working in a Sensory Art session somewhere in a College. James is not ambulant and uses a manual wheelchair to move around the building. James has some hand function but it is inconsistent. When James is motivated it appears his hand function is reasonably good. James does not have any known visual problems. Although James requires a hearing aid he will not tolerate it and simply pulls it out. He displays behaviours that staff find challenging if anyone tries to replace it. However, James does respond to sound; he will turn his head to a sudden sound and will move his body to music.
The time approaches for a break. A staff member (Alice), with responsibilty for James, approaches and takes James' OOR bag from his wheelchair. Opening the bag, she locates the Object of Reference for breaktime (in this instance a blue plastic beaker). Alice places the beaker in the mouth of the bag and crouches down in front of James and attempts to get eye contact.
"James", she says clearly, trying to engage his attention. "James, it is time for a drink now".
Alice uses the same words at every break time. She does not vary them. She also signs 'drink time' using Makaton.
She holds the bag up such that James can easily take the beaker from the bag. There is no chance that James can get hold of any other object by accident or intention. James makes eye contact but does not take the object. Alice moves the object closer to James's right hand. James reaches for it, takes it and Alice removes the bag.
"James, we are going for a drink now. You have the cup. Well done James. Let's go for a drink." Alice signs using Makaton for the words 'go' and 'drink' as she speaks.
James drops the cup on the floor. Alice says nothing. She reaches down and retrieves the cup and gives it back to James.
"James, we are going for a drink now". Alice moves James though the door of the classroom and into the corridoor. James once again drops the cup. Alice picks it up and uses the opportunity to provide James with directions to the Break area:
"James we are going for a drink now". Alice shows him the cup. "Do you know which way we go?" Alice smiles at James and gains eye contact before turning her head and eyes slowly to the right hopefully indicating the direction to be travelled. Alice points and says, "We have to go this way for a drink." Alice returns the cup to James and resumes assisting him to move towards the drinks area. While James has some hand function he does not self propel his wheelchair, he relies on stafff to transport him around the College.
The whole process of break time should be delivered as consistently as is possible such that each Learner begins to anticipate the coming events as they unfold. This recommends (although doesn't necessarily necessitate) a consistency of staff support with each team member fully aware of their role and the provision to be made. Colleges and other establishments may wish to develop their own policy and procedure documentation covering this aspect of the day.
Good practice during break times would dictate that, at least, the following practices are in place:
- Use of Makaton signing with all communication from staff;
- if Personal Care is to be addressed then, presentation of OOR for this POLE (Person Object Location Event);
- Object of Reference presented during session immediately prior to break indicating that it is break time and there will be a move to a new area;
- Movement to Personal Care area / Break area is NOT staff directed but rather a Learner focus (see the research by Trief 2015)
- D-oor-ways to mark the Personal Care areas;
- Sensory Cue to mark the Personal Care area;
- Consistency of approach in Personal Care;
- At end of Personal Care, Object Of Reference presented for break time;
- Symbol use to indicate directions to travel and to mark the break time area;
- D-oor-ways to mark the entrance to the break area;
- Sensory Cue(s) to mark the break location/event;
- Consistency of approach;
- Micro-management of events;
- Choice of drinks available;
- Choice of entertainment available (Symbolic and/or Object choice);
- Symbolic representation of drinks choice for some Learners (both personal choice boards and visual menu displays);
- Object representation (Sensory Cueing) of drinks choice for some Learners;
- At end of break, Learner presented with Object Of Reference for next session.
In order to illustrate such practice let's assume a Learner called James who is an IEPMLD currently working in a Sensory Art session somewhere in a College. James is not ambulant and uses a manual wheelchair to move around the building. James has some hand function but it is inconsistent. When James is motivated it appears his hand function is reasonably good. James does not have any known visual problems. Although James requires a hearing aid he will not tolerate it and simply pulls it out. He displays behaviours that staff find challenging if anyone tries to replace it. However, James does respond to sound; he will turn his head to a sudden sound and will move his body to music.
The time approaches for a break. A staff member (Alice), with responsibilty for James, approaches and takes James' OOR bag from his wheelchair. Opening the bag, she locates the Object of Reference for breaktime (in this instance a blue plastic beaker). Alice places the beaker in the mouth of the bag and crouches down in front of James and attempts to get eye contact.
"James", she says clearly, trying to engage his attention. "James, it is time for a drink now".
Alice uses the same words at every break time. She does not vary them. She also signs 'drink time' using Makaton.
She holds the bag up such that James can easily take the beaker from the bag. There is no chance that James can get hold of any other object by accident or intention. James makes eye contact but does not take the object. Alice moves the object closer to James's right hand. James reaches for it, takes it and Alice removes the bag.
"James, we are going for a drink now. You have the cup. Well done James. Let's go for a drink." Alice signs using Makaton for the words 'go' and 'drink' as she speaks.
James drops the cup on the floor. Alice says nothing. She reaches down and retrieves the cup and gives it back to James.
"James, we are going for a drink now". Alice moves James though the door of the classroom and into the corridoor. James once again drops the cup. Alice picks it up and uses the opportunity to provide James with directions to the Break area:
"James we are going for a drink now". Alice shows him the cup. "Do you know which way we go?" Alice smiles at James and gains eye contact before turning her head and eyes slowly to the right hopefully indicating the direction to be travelled. Alice points and says, "We have to go this way for a drink." Alice returns the cup to James and resumes assisting him to move towards the drinks area. While James has some hand function he does not self propel his wheelchair, he relies on stafff to transport him around the College.
The drinks area is in the College Hall which also serves as the dining room and functions as a sports hall in inclement weather. On the door to the hall is a d-oor-way, an Object Of Reference holder which states the current function of the hall. Already slid into this holder is an identical blue plastic beaker to the one that James is carrying although it has been cut in half and mounted on a slider plate that fits inside the d-oor-way. Alice points to the d-oor-way and says, "James, look, drink time". She signs 'drink time' again for James. Alice removes the slider from its housing on the door. She puts the slider next to the beaker James still has in his lap and holds both up for him to see. "Same", Alice says and, putting both onto his lap, signs 'same'. Alice replaces the slider into its housing and moves through the doorway into the hall.
In the hall, a drinks trolley (which is kept is in permanent storage) has been readied by catering staff. It is positioned alongside a permanent wall dispaly of the drinks available. The same drinks are available at every break. It does not vary. There are five drinks but six options (one option being to choose not to have a drink)
In the hall, a drinks trolley (which is kept is in permanent storage) has been readied by catering staff. It is positioned alongside a permanent wall dispaly of the drinks available. The same drinks are available at every break. It does not vary. There are five drinks but six options (one option being to choose not to have a drink)
no drink apple juice orange juice blackcurrant water milk


In addition to the wall menu there are:
Staff do not have to go searching for the resources, the College has micro-managed the entire break experience such that everything is ready to go at each break time. Some things are kept permanently on display others are permanent but put into storage at the end of each break session and brought out for the next break time.
Alice took James over to the drinks. "We are here here James", she said. "Let's put the blue beaker back in your bag". She carefully took the Objects Of Reference bag from the back of James' chair and held it open for him. James looked at her and the bag but did not put the beaker back inside. Instead, he tried to put his hand inside. Alice knew to move the bag away if he did that but not to say anything. She knew if he managed to take another object out of the bag they would have to treat that as a choice by James and go to that place. So she withdrew the bag and made sure James was holding the beaker before trying once again to get him to put it into the bag. This time he put the beaker in the bag. Alice smiled and said, "Well, done James."
Alice went over to the drinks trolley and selected two BIGmacks; One for orange which Alice knew James liked and one for water which she knew he would drink but assumed would rather have orange. She placed them on a portable trolley together with the appropriate drinks containers and the correct coloured drinks beakers and positioned the trolley in front of James. The items were arranged in two groupings: the items representing water on one side and the items representing orange on the other. Alice knew James had a right side positional preference and so she often put the water items there although, originally, she had always maintained the orange items in the right position in the simple choice such that he might start to associate the 'orange items' with receiving the orange drink. James needed a simple choice. The wall display was too much for him, and three items was not yet working in the classroom. He could cope with two items but didn't always select the one that was correct when assessed with the choice making kit they had purchased for that purpose. They continued to work on it however and break times was just another opportunity to address and develop those particular skills.
James reached out and took a hold of the clear beaker and raised it to his lips even though it was empty. Alice was disappointed that he hadn't gone for the orange she had placed in his non-preferred position but she did not say or do anything to show it. Alice knew that she must always provide every student with the option dictated by what they had 'chosen'. If they looked at, touched, or otherwise indicated a particular object then that was the item to which the staff must respond as though it were a deliberate and considered choice. Alice had witnessed staff who ignored the rules and said things such as, "Oh you didn't mean that, I know what you mean. I'll get you a ..." Alice knew that was not good practice and that it undermined everything that the College was trying to achieve and always spoke up and corrected other staff when she saw or heard them doing that. She knew that the staff were simply trying to be kind and were well intentioned but she also knew that good intentions was not the same as good practice and would not lead to good progress. So, although Alice wasn't sure that James had really chosen water she nevertheless treated his 'selection' as though he had and said and signed "water? Right away sir!". She removed the portable trolley display and went to the drinks trolley and poured James a beaker of water into a clear plastic beaker and gave it to him. James drank it down greedily in almost one go. While he was doing that, Alice replaced everything on the drinks trolley such that other staff could make use of them and they wouldn't go missing.
Alice noticed a staff member pouring orange into a green beaker. "No, that's wrong, you need to use an orange beaker for the orange juice'" she said helpfully. "What does it matter/" the staff member replied, "A beaker is a beaker and Susan can't see it anyway." Alice scowled and said strongly, "It does matter. We have to do it properly every time otherwise we might as well not do it at all. You don't know if Susan can't see but, even if if you are right about that, the other students can see and it is just confusing for everyone. Use the correct colour." The staff member looked a little embarrassed and complied with Alice's demand. Alice thought that the college would have no chance to succeed if staff just ignored what they had been told during training and did their own thing for an easier life and made a mental note to keep an eye on that staff member's practice in future.
James had finished his water and dropped the empty beaker on the ground. However, that was progress; in the past he had thrown it across the room half-filled with drink and made something of a mess. These days Alice could leave him to drink in peace and not have to stand watching him every second of the process. Alice picked up the empty beaker and gave it to James, "Where do empty cups go?" she said (signing 'where' and 'cup') taking James to another trolley that container big plastic containers for used items. "Put the cup in" she said and signed pointing to the place James was to put the beaker. Staff were told not to use the word 'beaker' as 'cup' was a simpler form that students might begin to understand in time. James put the beaker into the container and Alice said, "Well done James, good work." She made the signs for good work and gave James a really big smile.
"James, there's no music" Alice said and signed. She took James over to the switch mounted on the wall of the hall that turned on the music. Each time it was activated it changed the track playing and there was a choice of several items from quiet classical to somewhat noisy rock. "Do you want some music/" Alice signed 'music' and waited. She looked at James and then at the big red switch with the music symbol on the wall and then back at James once again. She repeated this three times. James had done it previously so she knew he could do it. She was just thinking,'perhaps he doesn't want any music' when James reached out and hit the switch. Music started almost instantly. It played for just a couple of seconds before James hit the switch once again and the music changed. "You did not want that music?" Alice said hoping James had really made a conscious choice to change the track but secretly believing that he had simply hit the switch twice for some other reason. However, she knew that if he did it often enough, he might just latch on to the fact that the switch changed the music as well as just turning it on. Alice looked forward to that day. She knew it would come given time.
- laminated sheet drink menus of the same drinks options kept on the trolley that staff can either give to, hold for, or hold and scan for, the Learner to be able to make a choice.
- single options available, each as an A4 laminated sheet such that staff can simplfy the choice and (for example) just hold up two options from which a Learner may select (orange or apple, for example).
- single options available ready mounted on a velcro-friendly trifold flip board. To simplify choices, the symbols can be flipped over such that any combination can easily be displaid.
- tactile symbols each mounted on strong card which can be arranged in any order and from which a Learner may select. The tactile symbols were formed using simple processes. For example: a glue gun to create the simple outline shape of an apple which was then in-filled with a sensory surface using apple pips; an orange coloured peg board cut into a circle; a set of purple beads arranged as a letter 'B'; strips of sponge forming a letter 'W'; and milk container screw tops (each white) glued in formation to make the letter M. Each tactile symbol could be positioned on an appropriate BIGmack if an auditory output was desired.
- a complete set of plastic bottle and containers that are permanently sealed. There is a bottle of water to represent water, a sealed carton of milk, a bottle of blackcurrant juice, a carton of apple juice and a carton of orange juice. Each was chosen specifically to be as distinct from the other options available to enable a choice to be made readily.
- A set of BIGmacks mounted under each option on the wall such that can select by activating any surface. The BIGmacks are mounted such that they can easily be removed if necessary (to replace batteries for example). As there are only four (red, blue, green, and yellow) colours available for BIGmack tops, colours are provided by appropriate labels attached to their surface held in place by snap caps.
- A further set of identical BIGmacks on the trolley for use by any student.
- A single large Step By Step that has been pre-recorded with the options: apple juice, orange juice, blackcurrant juice, water, milk, and nothing through which a Learner can step over and over until s/he stops at one and indicates by vocalisation, sign, gesture, or body language 'this is the one that I want'.
- sets of coloured beakers. Each beaker represents a different drink option: A green beaker for apple juice, an orange beaker for orange juice, a purple beaker for blackcurrant juice, a clear beaker for water, and a white beaker for milk. These are always used consistently to provide the drinks for those Learners that can manage to hold a beaker to drink. If a Learner requires a special drinking vessel they get the vessel with their chosen drink and the empty coloured plastic beaker representing what they have chosen.
Staff do not have to go searching for the resources, the College has micro-managed the entire break experience such that everything is ready to go at each break time. Some things are kept permanently on display others are permanent but put into storage at the end of each break session and brought out for the next break time.
Alice took James over to the drinks. "We are here here James", she said. "Let's put the blue beaker back in your bag". She carefully took the Objects Of Reference bag from the back of James' chair and held it open for him. James looked at her and the bag but did not put the beaker back inside. Instead, he tried to put his hand inside. Alice knew to move the bag away if he did that but not to say anything. She knew if he managed to take another object out of the bag they would have to treat that as a choice by James and go to that place. So she withdrew the bag and made sure James was holding the beaker before trying once again to get him to put it into the bag. This time he put the beaker in the bag. Alice smiled and said, "Well, done James."
Alice went over to the drinks trolley and selected two BIGmacks; One for orange which Alice knew James liked and one for water which she knew he would drink but assumed would rather have orange. She placed them on a portable trolley together with the appropriate drinks containers and the correct coloured drinks beakers and positioned the trolley in front of James. The items were arranged in two groupings: the items representing water on one side and the items representing orange on the other. Alice knew James had a right side positional preference and so she often put the water items there although, originally, she had always maintained the orange items in the right position in the simple choice such that he might start to associate the 'orange items' with receiving the orange drink. James needed a simple choice. The wall display was too much for him, and three items was not yet working in the classroom. He could cope with two items but didn't always select the one that was correct when assessed with the choice making kit they had purchased for that purpose. They continued to work on it however and break times was just another opportunity to address and develop those particular skills.
James reached out and took a hold of the clear beaker and raised it to his lips even though it was empty. Alice was disappointed that he hadn't gone for the orange she had placed in his non-preferred position but she did not say or do anything to show it. Alice knew that she must always provide every student with the option dictated by what they had 'chosen'. If they looked at, touched, or otherwise indicated a particular object then that was the item to which the staff must respond as though it were a deliberate and considered choice. Alice had witnessed staff who ignored the rules and said things such as, "Oh you didn't mean that, I know what you mean. I'll get you a ..." Alice knew that was not good practice and that it undermined everything that the College was trying to achieve and always spoke up and corrected other staff when she saw or heard them doing that. She knew that the staff were simply trying to be kind and were well intentioned but she also knew that good intentions was not the same as good practice and would not lead to good progress. So, although Alice wasn't sure that James had really chosen water she nevertheless treated his 'selection' as though he had and said and signed "water? Right away sir!". She removed the portable trolley display and went to the drinks trolley and poured James a beaker of water into a clear plastic beaker and gave it to him. James drank it down greedily in almost one go. While he was doing that, Alice replaced everything on the drinks trolley such that other staff could make use of them and they wouldn't go missing.
Alice noticed a staff member pouring orange into a green beaker. "No, that's wrong, you need to use an orange beaker for the orange juice'" she said helpfully. "What does it matter/" the staff member replied, "A beaker is a beaker and Susan can't see it anyway." Alice scowled and said strongly, "It does matter. We have to do it properly every time otherwise we might as well not do it at all. You don't know if Susan can't see but, even if if you are right about that, the other students can see and it is just confusing for everyone. Use the correct colour." The staff member looked a little embarrassed and complied with Alice's demand. Alice thought that the college would have no chance to succeed if staff just ignored what they had been told during training and did their own thing for an easier life and made a mental note to keep an eye on that staff member's practice in future.
James had finished his water and dropped the empty beaker on the ground. However, that was progress; in the past he had thrown it across the room half-filled with drink and made something of a mess. These days Alice could leave him to drink in peace and not have to stand watching him every second of the process. Alice picked up the empty beaker and gave it to James, "Where do empty cups go?" she said (signing 'where' and 'cup') taking James to another trolley that container big plastic containers for used items. "Put the cup in" she said and signed pointing to the place James was to put the beaker. Staff were told not to use the word 'beaker' as 'cup' was a simpler form that students might begin to understand in time. James put the beaker into the container and Alice said, "Well done James, good work." She made the signs for good work and gave James a really big smile.
"James, there's no music" Alice said and signed. She took James over to the switch mounted on the wall of the hall that turned on the music. Each time it was activated it changed the track playing and there was a choice of several items from quiet classical to somewhat noisy rock. "Do you want some music/" Alice signed 'music' and waited. She looked at James and then at the big red switch with the music symbol on the wall and then back at James once again. She repeated this three times. James had done it previously so she knew he could do it. She was just thinking,'perhaps he doesn't want any music' when James reached out and hit the switch. Music started almost instantly. It played for just a couple of seconds before James hit the switch once again and the music changed. "You did not want that music?" Alice said hoping James had really made a conscious choice to change the track but secretly believing that he had simply hit the switch twice for some other reason. However, she knew that if he did it often enough, he might just latch on to the fact that the switch changed the music as well as just turning it on. Alice looked forward to that day. She knew it would come given time.
8. Supporting Communication
It is extremely rare for any conscious person to be completely unable to communicate by, at the very least, behaviour, body language, facial expression, etc:
"They are all too often defined by what they cannot do and language problem are often listed among their deficits. However, I have yet to meet a child who does not communicate in some way." (Knight, 1992)
"Babies no older than an hour of age communicate - perhaps not intentionally, though try telling that to most parents of new infants, and you'll run into an argument - but certainly, they are doing things that we recognise as communicative and that cause us to act as though we are being communicated to. Thus, we realize that everyone can communicate, and, in fact, everyone does communicate in some way, somehow, if there is something important to say. In other words, communication is neither a right nor something that has to be learned - it is an inevitability: people cannot not communicate (Watzlawick P., Beavin J., & Jackson D. 1967). ... communication has only one prerequisite ... breathing is the only prerequisite that is relevant to communication." (Mirenda,1993, page 4)
However, body language (etc), although important, is not sufficient to make all needs explicit and interact fully with other people; for these things (and more) we require some form of (probably augmentative and alternative) communication. Such communication skills need to be developed and, thus, taught and yet there usually is no 'communication' as a subject to be found on the curriculum:
"Language is often undervalued because it is not a curriculum subject. This situation worsens as the child moves to secondary education where there is a great deal of subject compartmentalisation. Each subject in the curriculum is thought to be a group of skills that can be taught apart from language." (Beveridge & Conti-Ramsden, 1987)
Further, it is really important that all staff working within any establishment who come into any contact with IEPMLD should have positive mental attitudes:
"Until now the indirect speech and language therapy of individuals with PMLD has mostly been predicated on teaching staff new communication practices. However, then the question arises whether the sole emphasis on training the communication practices of the staff is enough to ensure effective communication. Ager and O’May (2001) noted that a change in staff behaviour requires a change in the staff members’ thinking habits. This means that in addition to learning new communication strategies, the staff should have opportunity to focus on an awareness of the assumptions they have about the communication abilities of individuals with PMLD. Furthermore, the scholars in the field of indirect speech and language therapy seem to have neglected the fact that the values and practices of the organisation in which the clients and staff members interact affects the nature and effectiveness of those interactions. The practices of the organisation thus have
an impact on how the staff members encounter their clients." (Koski, 2014, page 16)
Language and communication skills are important:
"Lacking a language the child is crippled in mind and personality. He is condemned to an intellectual silence and an emotional solitude too distressing to contemplate." (Sheridan, 1964)
"Without adequate communication social life, even at a most elementary level, is impossible. But with adequate communication the effects of even a very severe physical handicap can be alleviated very greatly in many ways." (Fisch 1969)
"Through language he makes the present comprehensible, the past available, the future conceivable." (Creber, 1972)
"Learning to communicate is at the heart of education" (Barnes,1976)
"No one in this day and age can possibly underestimate the importance of language. We are surrounded by talking." (Jeffree. & McConkey, 1976)
"Cerebral palsied children have a multiplicity of problems: depending on the extent of their brain damage, there may be intellectual deficit and sensory loss in addition to motor disability. These together with psychosocial factors will influence communicative ability. Maximum development of a child's communication should be the principal goal for everyone concerned." (Coombes, 1986)
"Speech is the most important thing we have. It makes us a person and not a thing. No one should ever have to be a 'thing'." (Joseph, 1986, page 8)
"The ability to communicate, that is, to interact socially and to make needs and wants known, is central to the determination of an individual's quality of life. The power of communication is especially important for the severely handicapped .... these individuals face a lifetime of substantial, if not total dependence on others; hence, their ability to communicate and establish some control over their environment must be recognized as a priority in their programming." (Light, McNaughton, & Parnes, 1986)
"In addition, it is thought that language interacts with the child's learning and ability to cope with the demands of the classroom. Thus those children with language difficulties do not have a discrete, contained problem. They have a problem which affects their whole school career."(Beveridge & Conti-Ramsden, 1987)
"If you want to know what it is like to be unable to speak, there is a way. Go to a party and don't talk. Play mute. Use your hands if you wish but don=t use paper and pencil. Paper and pencil are not always handy for a mute person. Here is what you will find: people talking; talking behind, beside, around, over, under, through, and even for you. But never with you. You are ignored until finally you feel like a piece of furniture." (Rick Creech quoted in Musselwhite. & St. Louis, 1988, page 104)
"And to be defective in language, for a human being, is one of the most desperate of calamities, for it is only through language that we enter fully into our human estate and culture, communicate freely with our fellows, acquire and share information. If we cannot do this, we will be bizarrely disabled and cut off - whatever our desires, or endeavours, or native capacities. And indeed, we may be so little able to realize our intellectual capacities as to appear mentally defective." (Sacks, 1989)
"To fully participate in an educational environment, an individual must have the tools to interact. Oral communication which is now possible through the development of voice output communication aids, will only enhance the involvement and participation of AAC communicators in the classroom. Every child should have the tools necessary to help him maximize his talents and to benefit from educational opportunities."(March, 1990, page 96)
"A communication handicap is quite different from other handicaps. It affects the manner in which you relate to other people and how they relate to you, it pervades everything you do." (Oakley, 1991)
"Freedom of expression is both a necessity and a highly prized right in our country. In its absence Americans with significant speech disabilities routinely experience isolation, discrimination, segregation, illiteracy, institutionalization, unemployment, poverty, and despair. Due to the lack of understandable speech, these individuals are perceived to be unable to direct their own lives; a perception that often leads to an erosion or outright deprivation of their most basic civil rights and liberties. The 'cloak of incompetence' is the heaviest burden Americans with significant speech disabilities have always faced in our country, and now is the time to cast off this cloak once and for all." (United Cerebral Palsy Associations, 1992)
"Denying these individuals a voice has also had the effect of further cementing the tiles in the mosaic - since, if they could not communicate, there was no way they could tell us whether or not they liked the lives we designed for them. So we assumed they did and continued to design them." (Mirenda, 1993, page 4)
"Where there is failure to develop language or where speech is rendered unintelligible through neurological or other organic disorder, lack of verbal communication with others can have far-reaching effects on many aspects of a child's development. Reduced ability to comprehend and use language will hinder cognitive and social development and there is known to be a high incidence of emotional and behavioural problems among such children." (Dalton,1994, Page 2)
"What we do know is that the outcome for children with speech and language problems is very poor. In middle childhood about 50 per cent of children with language difficulties will have related emotional difficulties." (Goodyer,1995, page 13)
"I mean if a person cannot communicate his/her thoughts, others will do it for the person and assume they know what the person means and what's best for the person. Their intentions are well meant, however, the whole concept is... Bull!" (Kitch,1995, page 4)
"The emergence and development of the ability to communicate through speech and the ability to move beyond the here-and-now through thinking are among the most striking achievements of childhood - for they are not only the most distinctly human capacities, but are also at the very centre of psychological development." (Lee & Das Gupta,1995, page vii)
"'Do you mean the national curriculum, Charles?' I asked, fascinated that a centenarian, retired from teaching for some 40 years, should still want to know about his former profession. 'I don't know', he replied, 'I keep hearing about this new curriculum on the radio. What is it?' I described it briefly and neutrally so as not to raise his blood pressure unduly. 'Is there anything about communication in it?', he asked, 'that's what's important for children, you know.'" (Wragg, 1996, page 64, talking with Charles Warrell)
If, as Charles Warrell suggests (op.cit.), communication is fundamental then how should it be addressed for IEPMLD? While it is very unlikely that such Learners will ever gain the power of speech via 'natural' means, there are a number of Augmentative and Alternative Communication methodologies (AAC) that can be explored. It is beyond the scope of this webpage to cover them all as it would take several web pages to even begin to address the topic. However, many of these systems have already been addressed elsewhere on this website; simply click on the links to find out more (links open other pages on this website or open other sites with relevant information):
"They are all too often defined by what they cannot do and language problem are often listed among their deficits. However, I have yet to meet a child who does not communicate in some way." (Knight, 1992)
"Babies no older than an hour of age communicate - perhaps not intentionally, though try telling that to most parents of new infants, and you'll run into an argument - but certainly, they are doing things that we recognise as communicative and that cause us to act as though we are being communicated to. Thus, we realize that everyone can communicate, and, in fact, everyone does communicate in some way, somehow, if there is something important to say. In other words, communication is neither a right nor something that has to be learned - it is an inevitability: people cannot not communicate (Watzlawick P., Beavin J., & Jackson D. 1967). ... communication has only one prerequisite ... breathing is the only prerequisite that is relevant to communication." (Mirenda,1993, page 4)
However, body language (etc), although important, is not sufficient to make all needs explicit and interact fully with other people; for these things (and more) we require some form of (probably augmentative and alternative) communication. Such communication skills need to be developed and, thus, taught and yet there usually is no 'communication' as a subject to be found on the curriculum:
"Language is often undervalued because it is not a curriculum subject. This situation worsens as the child moves to secondary education where there is a great deal of subject compartmentalisation. Each subject in the curriculum is thought to be a group of skills that can be taught apart from language." (Beveridge & Conti-Ramsden, 1987)
Further, it is really important that all staff working within any establishment who come into any contact with IEPMLD should have positive mental attitudes:
"Until now the indirect speech and language therapy of individuals with PMLD has mostly been predicated on teaching staff new communication practices. However, then the question arises whether the sole emphasis on training the communication practices of the staff is enough to ensure effective communication. Ager and O’May (2001) noted that a change in staff behaviour requires a change in the staff members’ thinking habits. This means that in addition to learning new communication strategies, the staff should have opportunity to focus on an awareness of the assumptions they have about the communication abilities of individuals with PMLD. Furthermore, the scholars in the field of indirect speech and language therapy seem to have neglected the fact that the values and practices of the organisation in which the clients and staff members interact affects the nature and effectiveness of those interactions. The practices of the organisation thus have
an impact on how the staff members encounter their clients." (Koski, 2014, page 16)
Language and communication skills are important:
"Lacking a language the child is crippled in mind and personality. He is condemned to an intellectual silence and an emotional solitude too distressing to contemplate." (Sheridan, 1964)
"Without adequate communication social life, even at a most elementary level, is impossible. But with adequate communication the effects of even a very severe physical handicap can be alleviated very greatly in many ways." (Fisch 1969)
"Through language he makes the present comprehensible, the past available, the future conceivable." (Creber, 1972)
"Learning to communicate is at the heart of education" (Barnes,1976)
"No one in this day and age can possibly underestimate the importance of language. We are surrounded by talking." (Jeffree. & McConkey, 1976)
"Cerebral palsied children have a multiplicity of problems: depending on the extent of their brain damage, there may be intellectual deficit and sensory loss in addition to motor disability. These together with psychosocial factors will influence communicative ability. Maximum development of a child's communication should be the principal goal for everyone concerned." (Coombes, 1986)
"Speech is the most important thing we have. It makes us a person and not a thing. No one should ever have to be a 'thing'." (Joseph, 1986, page 8)
"The ability to communicate, that is, to interact socially and to make needs and wants known, is central to the determination of an individual's quality of life. The power of communication is especially important for the severely handicapped .... these individuals face a lifetime of substantial, if not total dependence on others; hence, their ability to communicate and establish some control over their environment must be recognized as a priority in their programming." (Light, McNaughton, & Parnes, 1986)
"In addition, it is thought that language interacts with the child's learning and ability to cope with the demands of the classroom. Thus those children with language difficulties do not have a discrete, contained problem. They have a problem which affects their whole school career."(Beveridge & Conti-Ramsden, 1987)
"If you want to know what it is like to be unable to speak, there is a way. Go to a party and don't talk. Play mute. Use your hands if you wish but don=t use paper and pencil. Paper and pencil are not always handy for a mute person. Here is what you will find: people talking; talking behind, beside, around, over, under, through, and even for you. But never with you. You are ignored until finally you feel like a piece of furniture." (Rick Creech quoted in Musselwhite. & St. Louis, 1988, page 104)
"And to be defective in language, for a human being, is one of the most desperate of calamities, for it is only through language that we enter fully into our human estate and culture, communicate freely with our fellows, acquire and share information. If we cannot do this, we will be bizarrely disabled and cut off - whatever our desires, or endeavours, or native capacities. And indeed, we may be so little able to realize our intellectual capacities as to appear mentally defective." (Sacks, 1989)
"To fully participate in an educational environment, an individual must have the tools to interact. Oral communication which is now possible through the development of voice output communication aids, will only enhance the involvement and participation of AAC communicators in the classroom. Every child should have the tools necessary to help him maximize his talents and to benefit from educational opportunities."(March, 1990, page 96)
"A communication handicap is quite different from other handicaps. It affects the manner in which you relate to other people and how they relate to you, it pervades everything you do." (Oakley, 1991)
"Freedom of expression is both a necessity and a highly prized right in our country. In its absence Americans with significant speech disabilities routinely experience isolation, discrimination, segregation, illiteracy, institutionalization, unemployment, poverty, and despair. Due to the lack of understandable speech, these individuals are perceived to be unable to direct their own lives; a perception that often leads to an erosion or outright deprivation of their most basic civil rights and liberties. The 'cloak of incompetence' is the heaviest burden Americans with significant speech disabilities have always faced in our country, and now is the time to cast off this cloak once and for all." (United Cerebral Palsy Associations, 1992)
"Denying these individuals a voice has also had the effect of further cementing the tiles in the mosaic - since, if they could not communicate, there was no way they could tell us whether or not they liked the lives we designed for them. So we assumed they did and continued to design them." (Mirenda, 1993, page 4)
"Where there is failure to develop language or where speech is rendered unintelligible through neurological or other organic disorder, lack of verbal communication with others can have far-reaching effects on many aspects of a child's development. Reduced ability to comprehend and use language will hinder cognitive and social development and there is known to be a high incidence of emotional and behavioural problems among such children." (Dalton,1994, Page 2)
"What we do know is that the outcome for children with speech and language problems is very poor. In middle childhood about 50 per cent of children with language difficulties will have related emotional difficulties." (Goodyer,1995, page 13)
"I mean if a person cannot communicate his/her thoughts, others will do it for the person and assume they know what the person means and what's best for the person. Their intentions are well meant, however, the whole concept is... Bull!" (Kitch,1995, page 4)
"The emergence and development of the ability to communicate through speech and the ability to move beyond the here-and-now through thinking are among the most striking achievements of childhood - for they are not only the most distinctly human capacities, but are also at the very centre of psychological development." (Lee & Das Gupta,1995, page vii)
"'Do you mean the national curriculum, Charles?' I asked, fascinated that a centenarian, retired from teaching for some 40 years, should still want to know about his former profession. 'I don't know', he replied, 'I keep hearing about this new curriculum on the radio. What is it?' I described it briefly and neutrally so as not to raise his blood pressure unduly. 'Is there anything about communication in it?', he asked, 'that's what's important for children, you know.'" (Wragg, 1996, page 64, talking with Charles Warrell)
If, as Charles Warrell suggests (op.cit.), communication is fundamental then how should it be addressed for IEPMLD? While it is very unlikely that such Learners will ever gain the power of speech via 'natural' means, there are a number of Augmentative and Alternative Communication methodologies (AAC) that can be explored. It is beyond the scope of this webpage to cover them all as it would take several web pages to even begin to address the topic. However, many of these systems have already been addressed elsewhere on this website; simply click on the links to find out more (links open other pages on this website or open other sites with relevant information):
- Sign Language: There are several sign language systems available although most notable amongst these with respect to IEPMLD are Makaton and Signalong.
- Tactile Sign Language. For example: Moon; Block; Hands-on-signing; Pro-tactile signing; Tassels; Canaan Barrie; Body signing;
- Tadoma.
- Objects Of Reference.
- Choice is a voice: See the choice section above, this webpage and also the choice page on this website.
- Picture Exchange Communication System (PECS).
- Communication Passports.
- BIGmacks, BIGsteps, and other single messaging communication aids. A number of companies offer alternative single messaging and simple communication aids. As these vary depending on your country, a simple internet search for single messaging communication aids should provide further information on current devices available or go here for a great resource.
- Simple AAC systems. Go here for a free chart on uses for simple AAC systems.
- Symbol systems for AAC. There are more of these systems available than you might imagine. Go here for a comprehensive list.
- Intensive Interaction (see Intensive Interaction section this web page [below] for further information.)
- Other? If there is a further communication system suitable for IEPMLD that is not included in the listing above please contact TalkSense ([email protected]) and let us know such that it may be added to the list for everyone's benefit. Thank you.
9. SELF control
"Whenever possible let the learner lead. Allow her to show what she wants to do and follow and encourage her in these activities, giving time for her to explore." (Aiken & Buultjens 1992, page 47)
"Today our clients can influence what we do. We have in our weekly schedule a choice in the opportunities we can give. Obviously we cannot give limitless choice. But earlier, everyone painted today and made puzzles tomorrow. However, now [following OIVA training] individuals can have their say [in the daily routine]." (Koski, 2014, page 54)
SELF Control is a curriculum that puts the Learner at it's centre and allows the Learner to choose what s/he wants to do and when. SELF stands for Student Enabled Learning Focus and 'control' refers to the goal of the scheme (The goal is control) putting the Learner in control. In such a curriculum Learners would be free to select the activities they follow during a portion of the day (for example, the morning). Such learning would have an individual focus rather than a group dynamic with Learners coming together for group sessions during the afternoon (for example) for such things as TASCS (See Idea XXX).
SELF Control assumes at least a two year program of study:
Year 1: Promoting Awareness
Year 2: Controlled Experience
SELF Control is an enhanced Objects of Reference (OOR) System supported through Multi-Sensory Referencing (MSR) techniques. As these aspects are covered in depth elsewhere on this website they will not be detailed further here. Initially, in (at least) year one, the system is staff controlled in order to promote awareness in the students of the relationship between an object (alternatively sensory surface or symbol if appropriate) and its referent (the activity). This follows the typical OOR methodologies outlined on the Multi-Sensory Referencing Page (This website).
Once a basic awareness of a relationship between objects and activities (POLE - Person Object Location Event) has been established, the staff begin to relinquish control to the students themselves allowing the students to choose the activity to follow. It does not not follow that the students need now be fluent in the comprehension of all objects utilised in the scheme, nor does it follow that student learning is complete; indeed, phase two is predicated on raising further student awareness.
During Phase Two (which may or may not be year two) each staff member begins to offer the Learners a choice of (meaningful) activities. This is repeated several times during a set period of time (the morning for example). The Learner is presented with an array of objects from which to choose. Each object is representative of an activity (awareness of which has been developed in phase one). On Learner selection of an object from an array, the staff member facilitates study on the area associated with the object for a period of at least ten minutes. Should the Learner be actively engaged, the activity might continue for longer until either the Learner 'indicates' (shows signs of flagging interest, gets up and walks away, behaviour changes, etc) it is time for a change or a maximum threshold of time is reached (one hour?). Following the first learning session, a further range of options for learning (OOR) are then offered to the Learner with staff withholding the object for the session previously selected (although this could again be re-offered for the next session). If more than an hour had passed by, the options on offer could include a drink break, personal care, etc. This would mean that the Learner could elect to take a break at a time of his/her choosing (the Learner acting as agent) rather than conforming to rigorously externally prescribed patterns. While this might mean that Learners are taking breaks at different times, in reality, such options would tend to be provided after at least one hour of study and, thus, most students would be electing to take their break during a similar time period. The same system might hold for the lunch break although canteen systems tend to work to a fixed schedule and, thus, there would be external constraints on the flexibility of such an approach (unless the student was to select and control the preparation of his/her own meal?).
The goal of such a scheme is to empower the Learner such that the Learner gets to choose what activities are done, in what order and, for how long (for a significant portion of the day). By definition, IEPMLD require one to one support and so staffing such a scheme should not be problematic. However, there may be some areas that require a two to one ratio (personal care, in some instances, for example) and this might not allow for continuing one to one support for all members of the student body. Resolving such issues must be a part of the planning for the scheme.
The approach requires that a number of activities are available from which a Learner may choose. As such, each activity must be prepared in advance. With resource boxes ready to go, and each staff member familiar with their use, staff can quickly accommodate any student selection. Ideally, the session tutor is freed to move from Learner to Learner, supporting the staff, ensuring correct use of the resources, and noting any significant progression. The session tutor, being 'free' in this way, could also help to resolve the aforementioned issue of an occasional requirement for two to one support for small periods of the day, stepping in to provide temporary cover until the staff member is able to return and allow the tutor to move between all Learners once again.
That's crazy! My students cannot make such choices.
That's the point! Unless we provide options and teach choice, how is the Learner ever going to come to understand that s/he has control over their own learning? The scheme does not demand that all Learners have prerequisite cognitive and physical skills, rather it provides a methodology through which such skills might emerge. If two or three objects are placed in front of a Learner it is fairly likely that s/he will reach out and interact with one (or look at one). If this is taken to be a choice (see Jean Ware 2003), even though it may not be any such thing, the Learner may eventually come to associate the object with the activity that follows. The Learner makes a 'choice', an activity (the activity associated with the object) follows. If the Learner doesn't settle with this activity (which may indicate that the Learner has not yet associated the object with the activity and did not intend to select it to follow) staff should take this to mean 'I have finished with this now, let me choose again'. Staff can then re-present the same range of activity objects minus the one that has already been 'chosen'.
What if the Learner chooses the same activity over and over again?
The Learner has chosen: Isn't that a good thing? Doesn't it also tell us something about the Learner's ability to recognise a particular object even when it is presented in different positions (Note: some Learners will have a positional bias and may always select the rightmost object {for example} presented. Therefore it is good practice to vary the position of objects in any array each time they are presented)? However, the selection of the same activity over and over is made impossible if the object relating to that activity is withdrawn from the options following the activity.
That's stupid! My Learners would not associate an object with an activity. How would they know what the objects meant?
They have had phase one to begin to make this association. However, the scheme does not assume that they know! Rather, by consistently following the choice of a particular object with a particular activity, it is hoped the Learner will come to comprehend the relationship and be empowered to make meaningful choices at some future time.
One of my students would grab all of the items on display at the same time. How could that be a choice?
Then you might need to limit the choice to two items and space them far enough apart to prevent your student from easily getting at them at the same time. Alternatively, if s/he takes them all, does s/he 'play with'/'focus on' one of them more than the others?
That might take months or even years.
Yes, it might. It certainly will not happen over night. However, isn't it a meaningful thing to attempt to do? Isn't it empowering? Doesn't it fulfill the goal (control)? Furthermore, don't the Learners get one one to one support on meaningful activities regardless of whether they understand the choice that they have made from the onset? How does that differ from simply bringing them into a classroom and staff deciding what is delivered which is what is common practice presently? It is not that the system doesn't provide meaningful activities (you may elect to use some of the meaningful activities presented on this page). It's not that the system does not provide the necessary support. However, the system does permit the development of the Learner as 'agent', controlling his/her life.
The student might select items but continually miss out on one that would be important for him such as physiotherapy which s/he does not like.
If physio was a necessary part of the Learner's daily schedule then perhaps the choices during one option of the morning session could be between two or three different physiotherapy options for example: walking, stretching exercises on a floor mat, ball play, balancing ... Obviously, each of these activities would be designed and overseen by a qualified physiotherapist (and tailored to the specific requirement of the individual) but not necessarily delivered by him or her.
Wouldn't that mean the student would be stuck with the same staff member each and every day?
No, not really. Staff members could revolve around a small group of Learners changing each day. Furthermore, there are benefits to staff members getting to know a Learner extremely well and for Learners to be working with a small group of staff with whom they are familiar. Furthermore, the options are not for the whole day; a portion of the day would be set aside for group activities.
What happens if a staff member is absent and the establishment can no longer provide one to one support?
Such issues need contingency planning under any curriculum. It may be that the option process is temporarily suspended in favour of a group dynamic. It may be that one member of staff takes on two students and works on choices with both allowing each a turn at selecting. It may be that one student is capable of working on his/her own for a short period (watching TV, playing on a computer) providing there is covering support available in the same room.
Watching TV? Playing on a computer? They are not meaningful activities!
Yes they are! Providing the Learner has chosen to do this then they are meaningful. Is it likely that these activities will form any part of the future daily routine of the Learner in the future? Of course; they are an almost certain bet! Wouldn't it be great if the Learner could control the TV, change the channel, replay a video, select a YouTube item to watch, ... Isn't this empowering? Empowering the Learner in activities that are going to play an important part of the future life of any Learner should be a major part of the curriculum on offer.
I don't want to my student to spend all day watching TV.
Neither does Talksense and the system does not allow for that. However, even if it did, it would be the Learner's choice so to do.
What if the activity requires the need for transport to a place outside of the establishment?
If the activity requires a visit to a sensory garden or the local park and it is possible to move there without transport there is not an issue. Thus, not all external activities create problems. If the request is for something such as swimming where there would be a need for transport to a pool not within walking distance then this need cannot obviously easily be met. Thus, such options should not be available as part of the SELF control section of the timetable. However, it does not follow that swimming would not take place as a meaningful group activity within that section of the curriculum. The same would apply to bowling, horse-riding, etc. If any of these activities could be provided locally by a single member of staff in a safe manner then they could form part of the SELF control curriculum.
What if the request is to use the College hydrotherapy pool?
Can this be delivered by a single member of staff in a safe manner? If yes, then offer it as a choice, if not, then do not! Provide it as part of the group dynamic.
How do teaching staff prepare session plans when they do not know what the student will choose?
They don't! Not in the the way that session plans are produced for a typically structured curriculum. There will be a 'session plan' that covers such sessions but it will not change (makes for less paper work) although there will still be a need to address the specific objectives for individual learners. However, each meaningful activity will need to be covered by appropriate methodologies, aims and objectives for the guidance of staff members working with Learners making that selection.
What if three Learners make the same selection?
If resources will stretch to it then the system should continue as normal. If the resources will not then the Learners might come together as a sub-group and work on the activity together with the staff.
What if a Learner elects to use a resource that is already be occupied by another student or group such as the multi-sensory room?
As the Learner is supported by his/her own staff member perhaps it may be possible for them to join the group in the use of that resource without interfering with their activity. If this is not possible perhaps a mobile multi-sensory area might be created as a resource for anyone to use when necessary. Typically multi-sensory rooms cost thousands of pounds however, a mobile multi-Sensory area could be created for a much smaller figure especially as the establishment is already likely to have many of its components. Virtually everything available in standard multi-sensory rooms can be provided outside of that environment in a cost-effective manner.
I have a Learner who has visual problems and would not be able to see the objects.
Then assist the Learner to explore the objects through touch. Put the 'choices' in a bag and encourage the Learner to explore the bag's content. Which ever object is first to be taken from the bag, take that to be the Leaner's 'choice'. Start simple. If the scheme is considered as an Objects Of Reference approach it would be advisable to start with just one presented object as a 'choice' See the OOR page on this website for more information. Remember OOR were originally designed for the use of deaf blind individuals.
My Learner is registered blind and also could not put his hand into a bag because of physical limitations.
OK, if the Learner will not or can not go to the objects then the objects must go to the Learner. Could he work with objects close up just moving his hand a little? If not, then you might begin by allowing the Learner to experience a single object (tell him that you are going to gently stroke it on his skin before doing so). Different experiences equate to different activities. After a while of doing this you can move to providing two experiences: To which experience is there a more enthusiastic reaction? Treat this as the choice.
He'll never understand that.
How do you know? Have you tried it consistently over a period of time and monitored reactions? What have you got to lose by so doing? Furthermore, what has the Learner got to gain in so doing? Help him to understand. See the Objects Of Reference Page on this website for further ideas. Begin with single objects selected by staff and gradually build over time. Simply saying this will never work prevents any, even slight, possibility of progress. Is there some adaptation that you believe might work which you will trial?
I still think it is a completely crazy and unworkable idea.
Then don't implement it! There is no compulsion to adopt any of the ideas on this page; you are free to adopt, adapt or reject them as you see fit. Perhaps one suggestion will spark an idea with which you will be happy to work.
"Today our clients can influence what we do. We have in our weekly schedule a choice in the opportunities we can give. Obviously we cannot give limitless choice. But earlier, everyone painted today and made puzzles tomorrow. However, now [following OIVA training] individuals can have their say [in the daily routine]." (Koski, 2014, page 54)
SELF Control is a curriculum that puts the Learner at it's centre and allows the Learner to choose what s/he wants to do and when. SELF stands for Student Enabled Learning Focus and 'control' refers to the goal of the scheme (The goal is control) putting the Learner in control. In such a curriculum Learners would be free to select the activities they follow during a portion of the day (for example, the morning). Such learning would have an individual focus rather than a group dynamic with Learners coming together for group sessions during the afternoon (for example) for such things as TASCS (See Idea XXX).
SELF Control assumes at least a two year program of study:
Year 1: Promoting Awareness
Year 2: Controlled Experience
SELF Control is an enhanced Objects of Reference (OOR) System supported through Multi-Sensory Referencing (MSR) techniques. As these aspects are covered in depth elsewhere on this website they will not be detailed further here. Initially, in (at least) year one, the system is staff controlled in order to promote awareness in the students of the relationship between an object (alternatively sensory surface or symbol if appropriate) and its referent (the activity). This follows the typical OOR methodologies outlined on the Multi-Sensory Referencing Page (This website).
Once a basic awareness of a relationship between objects and activities (POLE - Person Object Location Event) has been established, the staff begin to relinquish control to the students themselves allowing the students to choose the activity to follow. It does not not follow that the students need now be fluent in the comprehension of all objects utilised in the scheme, nor does it follow that student learning is complete; indeed, phase two is predicated on raising further student awareness.
During Phase Two (which may or may not be year two) each staff member begins to offer the Learners a choice of (meaningful) activities. This is repeated several times during a set period of time (the morning for example). The Learner is presented with an array of objects from which to choose. Each object is representative of an activity (awareness of which has been developed in phase one). On Learner selection of an object from an array, the staff member facilitates study on the area associated with the object for a period of at least ten minutes. Should the Learner be actively engaged, the activity might continue for longer until either the Learner 'indicates' (shows signs of flagging interest, gets up and walks away, behaviour changes, etc) it is time for a change or a maximum threshold of time is reached (one hour?). Following the first learning session, a further range of options for learning (OOR) are then offered to the Learner with staff withholding the object for the session previously selected (although this could again be re-offered for the next session). If more than an hour had passed by, the options on offer could include a drink break, personal care, etc. This would mean that the Learner could elect to take a break at a time of his/her choosing (the Learner acting as agent) rather than conforming to rigorously externally prescribed patterns. While this might mean that Learners are taking breaks at different times, in reality, such options would tend to be provided after at least one hour of study and, thus, most students would be electing to take their break during a similar time period. The same system might hold for the lunch break although canteen systems tend to work to a fixed schedule and, thus, there would be external constraints on the flexibility of such an approach (unless the student was to select and control the preparation of his/her own meal?).
The goal of such a scheme is to empower the Learner such that the Learner gets to choose what activities are done, in what order and, for how long (for a significant portion of the day). By definition, IEPMLD require one to one support and so staffing such a scheme should not be problematic. However, there may be some areas that require a two to one ratio (personal care, in some instances, for example) and this might not allow for continuing one to one support for all members of the student body. Resolving such issues must be a part of the planning for the scheme.
The approach requires that a number of activities are available from which a Learner may choose. As such, each activity must be prepared in advance. With resource boxes ready to go, and each staff member familiar with their use, staff can quickly accommodate any student selection. Ideally, the session tutor is freed to move from Learner to Learner, supporting the staff, ensuring correct use of the resources, and noting any significant progression. The session tutor, being 'free' in this way, could also help to resolve the aforementioned issue of an occasional requirement for two to one support for small periods of the day, stepping in to provide temporary cover until the staff member is able to return and allow the tutor to move between all Learners once again.
That's crazy! My students cannot make such choices.
That's the point! Unless we provide options and teach choice, how is the Learner ever going to come to understand that s/he has control over their own learning? The scheme does not demand that all Learners have prerequisite cognitive and physical skills, rather it provides a methodology through which such skills might emerge. If two or three objects are placed in front of a Learner it is fairly likely that s/he will reach out and interact with one (or look at one). If this is taken to be a choice (see Jean Ware 2003), even though it may not be any such thing, the Learner may eventually come to associate the object with the activity that follows. The Learner makes a 'choice', an activity (the activity associated with the object) follows. If the Learner doesn't settle with this activity (which may indicate that the Learner has not yet associated the object with the activity and did not intend to select it to follow) staff should take this to mean 'I have finished with this now, let me choose again'. Staff can then re-present the same range of activity objects minus the one that has already been 'chosen'.
What if the Learner chooses the same activity over and over again?
The Learner has chosen: Isn't that a good thing? Doesn't it also tell us something about the Learner's ability to recognise a particular object even when it is presented in different positions (Note: some Learners will have a positional bias and may always select the rightmost object {for example} presented. Therefore it is good practice to vary the position of objects in any array each time they are presented)? However, the selection of the same activity over and over is made impossible if the object relating to that activity is withdrawn from the options following the activity.
That's stupid! My Learners would not associate an object with an activity. How would they know what the objects meant?
They have had phase one to begin to make this association. However, the scheme does not assume that they know! Rather, by consistently following the choice of a particular object with a particular activity, it is hoped the Learner will come to comprehend the relationship and be empowered to make meaningful choices at some future time.
One of my students would grab all of the items on display at the same time. How could that be a choice?
Then you might need to limit the choice to two items and space them far enough apart to prevent your student from easily getting at them at the same time. Alternatively, if s/he takes them all, does s/he 'play with'/'focus on' one of them more than the others?
That might take months or even years.
Yes, it might. It certainly will not happen over night. However, isn't it a meaningful thing to attempt to do? Isn't it empowering? Doesn't it fulfill the goal (control)? Furthermore, don't the Learners get one one to one support on meaningful activities regardless of whether they understand the choice that they have made from the onset? How does that differ from simply bringing them into a classroom and staff deciding what is delivered which is what is common practice presently? It is not that the system doesn't provide meaningful activities (you may elect to use some of the meaningful activities presented on this page). It's not that the system does not provide the necessary support. However, the system does permit the development of the Learner as 'agent', controlling his/her life.
The student might select items but continually miss out on one that would be important for him such as physiotherapy which s/he does not like.
If physio was a necessary part of the Learner's daily schedule then perhaps the choices during one option of the morning session could be between two or three different physiotherapy options for example: walking, stretching exercises on a floor mat, ball play, balancing ... Obviously, each of these activities would be designed and overseen by a qualified physiotherapist (and tailored to the specific requirement of the individual) but not necessarily delivered by him or her.
Wouldn't that mean the student would be stuck with the same staff member each and every day?
No, not really. Staff members could revolve around a small group of Learners changing each day. Furthermore, there are benefits to staff members getting to know a Learner extremely well and for Learners to be working with a small group of staff with whom they are familiar. Furthermore, the options are not for the whole day; a portion of the day would be set aside for group activities.
What happens if a staff member is absent and the establishment can no longer provide one to one support?
Such issues need contingency planning under any curriculum. It may be that the option process is temporarily suspended in favour of a group dynamic. It may be that one member of staff takes on two students and works on choices with both allowing each a turn at selecting. It may be that one student is capable of working on his/her own for a short period (watching TV, playing on a computer) providing there is covering support available in the same room.
Watching TV? Playing on a computer? They are not meaningful activities!
Yes they are! Providing the Learner has chosen to do this then they are meaningful. Is it likely that these activities will form any part of the future daily routine of the Learner in the future? Of course; they are an almost certain bet! Wouldn't it be great if the Learner could control the TV, change the channel, replay a video, select a YouTube item to watch, ... Isn't this empowering? Empowering the Learner in activities that are going to play an important part of the future life of any Learner should be a major part of the curriculum on offer.
I don't want to my student to spend all day watching TV.
Neither does Talksense and the system does not allow for that. However, even if it did, it would be the Learner's choice so to do.
What if the activity requires the need for transport to a place outside of the establishment?
If the activity requires a visit to a sensory garden or the local park and it is possible to move there without transport there is not an issue. Thus, not all external activities create problems. If the request is for something such as swimming where there would be a need for transport to a pool not within walking distance then this need cannot obviously easily be met. Thus, such options should not be available as part of the SELF control section of the timetable. However, it does not follow that swimming would not take place as a meaningful group activity within that section of the curriculum. The same would apply to bowling, horse-riding, etc. If any of these activities could be provided locally by a single member of staff in a safe manner then they could form part of the SELF control curriculum.
What if the request is to use the College hydrotherapy pool?
Can this be delivered by a single member of staff in a safe manner? If yes, then offer it as a choice, if not, then do not! Provide it as part of the group dynamic.
How do teaching staff prepare session plans when they do not know what the student will choose?
They don't! Not in the the way that session plans are produced for a typically structured curriculum. There will be a 'session plan' that covers such sessions but it will not change (makes for less paper work) although there will still be a need to address the specific objectives for individual learners. However, each meaningful activity will need to be covered by appropriate methodologies, aims and objectives for the guidance of staff members working with Learners making that selection.
What if three Learners make the same selection?
If resources will stretch to it then the system should continue as normal. If the resources will not then the Learners might come together as a sub-group and work on the activity together with the staff.
What if a Learner elects to use a resource that is already be occupied by another student or group such as the multi-sensory room?
As the Learner is supported by his/her own staff member perhaps it may be possible for them to join the group in the use of that resource without interfering with their activity. If this is not possible perhaps a mobile multi-sensory area might be created as a resource for anyone to use when necessary. Typically multi-sensory rooms cost thousands of pounds however, a mobile multi-Sensory area could be created for a much smaller figure especially as the establishment is already likely to have many of its components. Virtually everything available in standard multi-sensory rooms can be provided outside of that environment in a cost-effective manner.
I have a Learner who has visual problems and would not be able to see the objects.
Then assist the Learner to explore the objects through touch. Put the 'choices' in a bag and encourage the Learner to explore the bag's content. Which ever object is first to be taken from the bag, take that to be the Leaner's 'choice'. Start simple. If the scheme is considered as an Objects Of Reference approach it would be advisable to start with just one presented object as a 'choice' See the OOR page on this website for more information. Remember OOR were originally designed for the use of deaf blind individuals.
My Learner is registered blind and also could not put his hand into a bag because of physical limitations.
OK, if the Learner will not or can not go to the objects then the objects must go to the Learner. Could he work with objects close up just moving his hand a little? If not, then you might begin by allowing the Learner to experience a single object (tell him that you are going to gently stroke it on his skin before doing so). Different experiences equate to different activities. After a while of doing this you can move to providing two experiences: To which experience is there a more enthusiastic reaction? Treat this as the choice.
He'll never understand that.
How do you know? Have you tried it consistently over a period of time and monitored reactions? What have you got to lose by so doing? Furthermore, what has the Learner got to gain in so doing? Help him to understand. See the Objects Of Reference Page on this website for further ideas. Begin with single objects selected by staff and gradually build over time. Simply saying this will never work prevents any, even slight, possibility of progress. Is there some adaptation that you believe might work which you will trial?
I still think it is a completely crazy and unworkable idea.
Then don't implement it! There is no compulsion to adopt any of the ideas on this page; you are free to adopt, adapt or reject them as you see fit. Perhaps one suggestion will spark an idea with which you will be happy to work.
10. Remember, Remember, ...
" ... and this can help explain why people with PMLD seem to have huge difficulties in remembering even much repeated activities. Maybe some people with PMLD constantly experience, even much repeated, activities as if for the first time? Maybe even people they meet on a daily basis are strangers to them every time?" (Lacey, 2015)
The ability to form memories is the most important factor in learning for, without such a capacity, our efforts at addressing cognitive amelioration will be futile; although the Individual may show signs of comprehension s/he will simply not remember the experience later on that same day. Having some awareness of things as they happen is fantastic but, once gone, not retaining that knowledge, negates the possibility of real learning. Therefore, not only do we need to establish an awareness of history but we also need to be able to measure how far that awareness stretches (A minute? An hour? A day, A week? ...). If we can help a Learner establish the concept of the immediate past and measure for how long it stretches (and work to increase that period) then we can set the Learner free to build meaningful experiences of life which will be retained. Thus, establishing a 'history' can set an individual free: free to experience, free to grow and, most importantly, free to learn. We can check all the tick boxes on our session plans during a lesson but, without an individual's ability to lay down memories, it is a pointless exercise, not worth the paper (or computer power) utilised. Memory is one of the first few things addressed in the 'Routes To Learning' system (item 4, 2006) which emphasises a need to search for evidence of short term memory:
" 4. Increase the gaps, looking for evidence of short term memory (see Guidance booklet page 15 – Habituation). Use a variety of stimuli.
Show a new stimulus, rather than the same stimulus again. Look for a recovery of interest."
Memory is not the same as a concept of time; indeed, a comprehension of the concept of time may be something that is truly beyond the capabilities of IEPMLD:
"The concept of time as hours and minutes is not one that the PMLD student will ever grasp. What can be taught, however, is an awareness of daily routines and a limited sensory of history - what happened yesterday - and the future - what will happen tomorrow." (Cartwright & Wind-Cowie, 2005, page 67)
As Cartwright and Wind-Cowie (op.cit.) suggest, what is possible is building on awareness of things that were experienced previously to provide an anticipation of future events providing, that is, the memory system is functioning within the Individual's brain. One crucially important area of the brain with regard to memory is the hippocampus which lies with the temporal lobes. Damage to this area can result in significant impairment of memory:
"A striking finding in the literature on human memory is the profound but selective deficit seen after damage to the hippocampus and related structures in the temporal lobes of the human brain. This pattern of deficits was first seen in patient H.M. (Scoville and Milner, 1957), and has now been replicated in the data of a large number of other patients with similar lesions. These patients show a dramatic deficit in the
ability to acquire new explicit memories for the contents of specific episodes and events. For example, the ability to learn arbitrary word-pairs such as 'locomotive - dishtowel' is drastically impaired. Normal subjects will learn such lists after a few presentations, so that whenever the first word of a pair is presented they will be able to recall the second word of each pair. But H.M. and other similar amnesics may fail to learn even one pair after repeated presentations. There is also profound impairment in everyday memory abilities, such as the ability to learn names of new people. or the ability to remember important personal events and experiences." (McClelland, 1996, page 601)
As a result of such damage, Clive Wearing has one one the most significant impairments of memory ever recorded:
The ability to form memories is the most important factor in learning for, without such a capacity, our efforts at addressing cognitive amelioration will be futile; although the Individual may show signs of comprehension s/he will simply not remember the experience later on that same day. Having some awareness of things as they happen is fantastic but, once gone, not retaining that knowledge, negates the possibility of real learning. Therefore, not only do we need to establish an awareness of history but we also need to be able to measure how far that awareness stretches (A minute? An hour? A day, A week? ...). If we can help a Learner establish the concept of the immediate past and measure for how long it stretches (and work to increase that period) then we can set the Learner free to build meaningful experiences of life which will be retained. Thus, establishing a 'history' can set an individual free: free to experience, free to grow and, most importantly, free to learn. We can check all the tick boxes on our session plans during a lesson but, without an individual's ability to lay down memories, it is a pointless exercise, not worth the paper (or computer power) utilised. Memory is one of the first few things addressed in the 'Routes To Learning' system (item 4, 2006) which emphasises a need to search for evidence of short term memory:
" 4. Increase the gaps, looking for evidence of short term memory (see Guidance booklet page 15 – Habituation). Use a variety of stimuli.
Show a new stimulus, rather than the same stimulus again. Look for a recovery of interest."
Memory is not the same as a concept of time; indeed, a comprehension of the concept of time may be something that is truly beyond the capabilities of IEPMLD:
"The concept of time as hours and minutes is not one that the PMLD student will ever grasp. What can be taught, however, is an awareness of daily routines and a limited sensory of history - what happened yesterday - and the future - what will happen tomorrow." (Cartwright & Wind-Cowie, 2005, page 67)
As Cartwright and Wind-Cowie (op.cit.) suggest, what is possible is building on awareness of things that were experienced previously to provide an anticipation of future events providing, that is, the memory system is functioning within the Individual's brain. One crucially important area of the brain with regard to memory is the hippocampus which lies with the temporal lobes. Damage to this area can result in significant impairment of memory:
"A striking finding in the literature on human memory is the profound but selective deficit seen after damage to the hippocampus and related structures in the temporal lobes of the human brain. This pattern of deficits was first seen in patient H.M. (Scoville and Milner, 1957), and has now been replicated in the data of a large number of other patients with similar lesions. These patients show a dramatic deficit in the
ability to acquire new explicit memories for the contents of specific episodes and events. For example, the ability to learn arbitrary word-pairs such as 'locomotive - dishtowel' is drastically impaired. Normal subjects will learn such lists after a few presentations, so that whenever the first word of a pair is presented they will be able to recall the second word of each pair. But H.M. and other similar amnesics may fail to learn even one pair after repeated presentations. There is also profound impairment in everyday memory abilities, such as the ability to learn names of new people. or the ability to remember important personal events and experiences." (McClelland, 1996, page 601)
As a result of such damage, Clive Wearing has one one the most significant impairments of memory ever recorded:
While the severity hippocampal damage has been shown to be directly proportional to the level of learning difficulty (see, for example, Jambaqué et al, 2006), is damage to the hippocampus a necessary feature in the classification of IEPMLD? That is, do all Individuals Experiencing PMLD have damaged hippocampi? By no means! Indeed, Talksense was unable to find any research evidence of neuroimaging detailing the necessity for hippocampal:
As memory is an essential component in learning it is important that we show that Learners are able to lay down new memories as well as providing the experiences which will assist in memory development. What 'experiences' (activities, environmental encounters, etc) have be shown to assist the development of memory?
Movement:
"Movement is the language of the brain" (Baniel, 2016)
"Movement is life; without movement life is unthinkable." (Moshé Feldenkrais)
"Nothing happens until something moves" is a famous quote by Albert Einstein. It has been shown that movement (exercise) can double the production of new neurons in the hippocampus in the brain (Suzuki, 2015) and new neurons in the hippocampus equate to improved memory. The problem is that too often IEPMLD do not move enough! Some are confined to wheelchairs and some are even strapped into a fixed position. Indeed, the more profound the disability the less likely the person is to be moving. They need to be moving! Even those that are ambulant may be confined to a single classroom for most of the day and may not move much within that environment. Equally as problematic, is the fundamental lack of Learner control during the limited movement permitted: the Learner is passive and the staff are active when that situation really ought to be turned upon its head such that the staff take a more supportive role with Learners as active as their ability currently permits.
"People with intellectual disabilities tend to have low activity and fitness levels which decline over the years when compared with those without a disability. Like individuals with intellectual disabilities, persons with visual impairments also display poor performance in
locomotor skills and have low levels of habitual activity. Individuals who suffer from a combination of severe or profound intellectual and visual disabilities (severe or profound multiple disabilities, SIMD) are particularly at risk in terms of the potential development of deficits in both locomotor skills and daily functioning. Furthermore, the combination of these deficits suggests that persons having SIMD are likely to have lower levels of habitual activity, than persons with ID without visual impairment." (Waninge, 2011)
Repetition:
"Repeated occurrences of the same sequence of events, created by regular scheduling of the same activities at the same time. may help the development of anticipation, which is an important step in learning to communicate. It may also help the development of a sense of the passage of time. Additionally, one study found that children spend more time on task when consistency is maintained.. A timetable in which there is little consistency from day to day is therefore unlikely to be the most appropriate for pupils with PMLDs." (Ware, 1994, page 115)
"Constant repetition and a great deal of support will be needed to generalise learning into new situations." (MENCAP, 2008, Page 4)
" Essentially, I had to completely inhabit the level of ability that I could achieve before it was time to take the next step. In order to atain a new ability, I had to be able to repeat that effort with grace and control before taking the next step." (Bolte Taylor, 2008, page 90)
"I needed my caregivers to teach me with patience. Sometimes I needed them to show me something over and over again., until my body and brain could figure out what I was learning" (Bolte Taylor, 2008, page 119)
"Repetition provides rehearsal and consolidation of known games and activities, and a continuous secure base and reference points. Through repetition variations occur, leading to new games and activities." (Quest For Learning, 2009, page 41)
"In order to meet their specific learning needs, a curriculum designed for pupils with MSI must provide frequent repetition and redundancy of information" (Murdoch et al, 2009, page 12)
"Remember that short, daily repetition is more valuable than longer, weekly sessions" (Association of Teachers and Lecturers, 2013, page 4)
"Focused on repeating sequences of sensory storytelling with the same three stories told every week for six weeks and then another three stories. The would allow for,the development of a pattern of sensory experiences using voice and body, and words and multi sensory objects." (Dowling, 2011, page 29)
"The student that I had the most progress with, was the student that I had every day, was seeing the symbols every day, over and over and over again." (Bruce, Trief, and Cascella, 2011)
"The more you bring a memory back to mind, the stronger it becomes. Boring but true. At the neural level, with each repetition you are strengthening the synaptic connections underlying the memory, allowing it to resist interference from other memories or general degradation. Repetition engages the neural networks related to our attention system; in other words, we tend to remember what we pay attention to." (Suzuki, 2015, page 75)
"So if people with PMLD have such difficulties with memory, how can they learn? As was suggested earlier in this article, sheer repetition is likely to be the answer. If John can learn to open his mouth to anticipate food on the spoon, then he can learn to anticipate other things,
but not without a tremendous amount of repetition. In my experience we do not repeat activities sufficiently. We want to give learners with PMLD an interesting life with lots of different sensory experiences, where perhaps we should be concentrating on a few that are repeated
many times." (Lacey, 2015, page 44)
Ordered Routine (consistency):
"For learners with complex needs, life can be a fragmented series of experiences with little order. Without structure, learners may never develop anticipation and memory so it is essential to provide a simple, structured environment with ordered routines to which objects can refer. Once simple routines are established, the most appropriate object for a small number of activities can be chosen. Objects must be meaningful to each individual and will not therefore be standard for each child or in any one classroom." (Quest For Learning, 2006, page 44)
While agreeing with the majority of this quote, I call into question the latter part (will not therefore be standard for each child) as there is no real evidence to support this claim. Indeed, TalkSense argues that 'what is meaningful' can be anything providing it is experienced on a consistent and routine basis in association with a particular experience (POLE) (See Multi-Sensory Referencing page this website for further details). Indeed, work with completely abstract symbol sets (having no connection at all to the items to which they referred) with Kanzi (a Bonobo) by Sue Savage-Rumbaugh (See Savage-Rumbaugh in bibliography) and also with Koko (a Gorilla) by Francine Paterson (See Paterson in bibliography) demonstrates that it is not necessary for symbolic objects to be 'meaningful' in the sense utilised in the quote. What is necessary however is repetition, routine, and consistency which, themselves, establish meaningful relationships. However, TalkSense is not suggesting that we deliberately select unconnected and abstract objects for communication use, rather that objects do not necessarily always have immediately to be meaningful to the Learner. Furthermore, while individualised Objects Of Reference might theoretically be the 'ideal', the 'ideal' may neither be practical nor pragmatic for use in the real world in educational establishments.
- atrophy in PMLD;
- lesions in PMLD;
- trauma in PMLD;
As memory is an essential component in learning it is important that we show that Learners are able to lay down new memories as well as providing the experiences which will assist in memory development. What 'experiences' (activities, environmental encounters, etc) have be shown to assist the development of memory?
Movement:
"Movement is the language of the brain" (Baniel, 2016)
"Movement is life; without movement life is unthinkable." (Moshé Feldenkrais)
"Nothing happens until something moves" is a famous quote by Albert Einstein. It has been shown that movement (exercise) can double the production of new neurons in the hippocampus in the brain (Suzuki, 2015) and new neurons in the hippocampus equate to improved memory. The problem is that too often IEPMLD do not move enough! Some are confined to wheelchairs and some are even strapped into a fixed position. Indeed, the more profound the disability the less likely the person is to be moving. They need to be moving! Even those that are ambulant may be confined to a single classroom for most of the day and may not move much within that environment. Equally as problematic, is the fundamental lack of Learner control during the limited movement permitted: the Learner is passive and the staff are active when that situation really ought to be turned upon its head such that the staff take a more supportive role with Learners as active as their ability currently permits.
"People with intellectual disabilities tend to have low activity and fitness levels which decline over the years when compared with those without a disability. Like individuals with intellectual disabilities, persons with visual impairments also display poor performance in
locomotor skills and have low levels of habitual activity. Individuals who suffer from a combination of severe or profound intellectual and visual disabilities (severe or profound multiple disabilities, SIMD) are particularly at risk in terms of the potential development of deficits in both locomotor skills and daily functioning. Furthermore, the combination of these deficits suggests that persons having SIMD are likely to have lower levels of habitual activity, than persons with ID without visual impairment." (Waninge, 2011)
Repetition:
"Repeated occurrences of the same sequence of events, created by regular scheduling of the same activities at the same time. may help the development of anticipation, which is an important step in learning to communicate. It may also help the development of a sense of the passage of time. Additionally, one study found that children spend more time on task when consistency is maintained.. A timetable in which there is little consistency from day to day is therefore unlikely to be the most appropriate for pupils with PMLDs." (Ware, 1994, page 115)
"Constant repetition and a great deal of support will be needed to generalise learning into new situations." (MENCAP, 2008, Page 4)
" Essentially, I had to completely inhabit the level of ability that I could achieve before it was time to take the next step. In order to atain a new ability, I had to be able to repeat that effort with grace and control before taking the next step." (Bolte Taylor, 2008, page 90)
"I needed my caregivers to teach me with patience. Sometimes I needed them to show me something over and over again., until my body and brain could figure out what I was learning" (Bolte Taylor, 2008, page 119)
"Repetition provides rehearsal and consolidation of known games and activities, and a continuous secure base and reference points. Through repetition variations occur, leading to new games and activities." (Quest For Learning, 2009, page 41)
"In order to meet their specific learning needs, a curriculum designed for pupils with MSI must provide frequent repetition and redundancy of information" (Murdoch et al, 2009, page 12)
"Remember that short, daily repetition is more valuable than longer, weekly sessions" (Association of Teachers and Lecturers, 2013, page 4)
"Focused on repeating sequences of sensory storytelling with the same three stories told every week for six weeks and then another three stories. The would allow for,the development of a pattern of sensory experiences using voice and body, and words and multi sensory objects." (Dowling, 2011, page 29)
"The student that I had the most progress with, was the student that I had every day, was seeing the symbols every day, over and over and over again." (Bruce, Trief, and Cascella, 2011)
"The more you bring a memory back to mind, the stronger it becomes. Boring but true. At the neural level, with each repetition you are strengthening the synaptic connections underlying the memory, allowing it to resist interference from other memories or general degradation. Repetition engages the neural networks related to our attention system; in other words, we tend to remember what we pay attention to." (Suzuki, 2015, page 75)
"So if people with PMLD have such difficulties with memory, how can they learn? As was suggested earlier in this article, sheer repetition is likely to be the answer. If John can learn to open his mouth to anticipate food on the spoon, then he can learn to anticipate other things,
but not without a tremendous amount of repetition. In my experience we do not repeat activities sufficiently. We want to give learners with PMLD an interesting life with lots of different sensory experiences, where perhaps we should be concentrating on a few that are repeated
many times." (Lacey, 2015, page 44)
Ordered Routine (consistency):
"For learners with complex needs, life can be a fragmented series of experiences with little order. Without structure, learners may never develop anticipation and memory so it is essential to provide a simple, structured environment with ordered routines to which objects can refer. Once simple routines are established, the most appropriate object for a small number of activities can be chosen. Objects must be meaningful to each individual and will not therefore be standard for each child or in any one classroom." (Quest For Learning, 2006, page 44)
While agreeing with the majority of this quote, I call into question the latter part (will not therefore be standard for each child) as there is no real evidence to support this claim. Indeed, TalkSense argues that 'what is meaningful' can be anything providing it is experienced on a consistent and routine basis in association with a particular experience (POLE) (See Multi-Sensory Referencing page this website for further details). Indeed, work with completely abstract symbol sets (having no connection at all to the items to which they referred) with Kanzi (a Bonobo) by Sue Savage-Rumbaugh (See Savage-Rumbaugh in bibliography) and also with Koko (a Gorilla) by Francine Paterson (See Paterson in bibliography) demonstrates that it is not necessary for symbolic objects to be 'meaningful' in the sense utilised in the quote. What is necessary however is repetition, routine, and consistency which, themselves, establish meaningful relationships. However, TalkSense is not suggesting that we deliberately select unconnected and abstract objects for communication use, rather that objects do not necessarily always have immediately to be meaningful to the Learner. Furthermore, while individualised Objects Of Reference might theoretically be the 'ideal', the 'ideal' may neither be practical nor pragmatic for use in the real world in educational establishments.
Hypoperfusion:
It has been known for some time that cerebral hypoperfusion (inadequate blood flow) is involved in memory loss (see, for example, Tanabe et al, 1991). While a number of factors may contribute to hypoperfusion, some beyond the abilities of educational establishments to affect, a few are accessible, for example: exercise (see, for example, Suzuki, 2015) and diet (see, for example, Merino et al 2013; Cortright, 2015). As we have already covered the importance of movement earlier in this section, we will move directly to diet. The BAD (British Average Diet) and the SAD (Standard American Diet) diets are known to have a negative impact on arterial function and wholefood plant-based diets a positive impact (https://nutritionfacts.org/video/plant-based-diets-and-artery-function/). Anything we can do, however small, to improve the cognitive functioning of IEPMLD has to be worth consideration and, therefore, improving the standard of the food and drink consumed by Learners should be seen as important. As many further educational establishments have 24/7 control over dietary choices, this factor should at least be discussed at management level. Even further educational establishments which operate on a day basis (no control over what is consumed at home and out of college) may be able to contribute by not further compounding the problem by restricting the foods and drinks that are available.
Medication:
Virtually all medication is known to have side-effects (just look at the information on the container!) and some can interfere with memory function. These medications include (but are not limited to):
Nutrition:
Good nutrition is vital to the functioning of the brain. We have already noted that diet has an effect on blood flow and blood flow an effect on brain function. However, the effect of diet goes beyond blood flow, what we eat becomes the building blocks for the brain and if we have poor quality or sparse building materials then we cannot expect to erect a building that will withstand all that is demanded of it. As good nutrition is an important factor in assisting the development of cognitive skills (Stein & Susser, 1985; Simeon & Grantham-McGregor, 1990; Wachs et al, 1993; Morley & Lucas, 1997; Schmitt et al, 2005; Fuglestad et al, 2008; Gomez-Pinilla, 2008; Isaacs & Oates, 2008; Jockers, 2012; Zainuddin & Thuret, 2012; Cortright, 2015) educational establishments should do all they can to ensure that the meals they provide are nutritious and that all readily available sources of junk food are eliminated.
Note: It has been shown that the consumption of small amounts of specific herbs and spices can have a positive impact on memory function (see, for example, Nutritionfacts.org)
Note: Perhaps the reason we do not yet have adequate neuroimaging of IEPMLD brains lies in the inability of this group to cope with the physical and cognitive demands of the present day neuroimaging technologies (see National Geographic, My Brilliant Brain, Episode 2 Accidental Genius, 2007). However, as technology advances, there will come a time when we are able to peer inside the brains of IEPMLD and devise improved systems for cognitive amelioration. The scans that have been achieved thus far, appear to show a very different brain wiring network (see National Geographic 'My Brilliant Brain' episode 2, 2007) but, even if this were proven to be the case for all this group (and that is by no means certain), it does not in any way preclude the possibility of progress in learning.
Note: More ideas for the development and assessment of memory are given on the 'history' page on this website.
Memory is an important component of 'contingency awareness' (cause and effect skills) which is covered in the section below ...
It has been known for some time that cerebral hypoperfusion (inadequate blood flow) is involved in memory loss (see, for example, Tanabe et al, 1991). While a number of factors may contribute to hypoperfusion, some beyond the abilities of educational establishments to affect, a few are accessible, for example: exercise (see, for example, Suzuki, 2015) and diet (see, for example, Merino et al 2013; Cortright, 2015). As we have already covered the importance of movement earlier in this section, we will move directly to diet. The BAD (British Average Diet) and the SAD (Standard American Diet) diets are known to have a negative impact on arterial function and wholefood plant-based diets a positive impact (https://nutritionfacts.org/video/plant-based-diets-and-artery-function/). Anything we can do, however small, to improve the cognitive functioning of IEPMLD has to be worth consideration and, therefore, improving the standard of the food and drink consumed by Learners should be seen as important. As many further educational establishments have 24/7 control over dietary choices, this factor should at least be discussed at management level. Even further educational establishments which operate on a day basis (no control over what is consumed at home and out of college) may be able to contribute by not further compounding the problem by restricting the foods and drinks that are available.
Medication:
Virtually all medication is known to have side-effects (just look at the information on the container!) and some can interfere with memory function. These medications include (but are not limited to):
- anxiety medications (Xanax, Valium, and Ativan);
- tricyclic antidepressants;
- statins;
- beta-blockers;
- narcotic painkillers;
- incontinence drugs;
- sleep aids;
- antihistamines;
- seizure medications;
Nutrition:
Good nutrition is vital to the functioning of the brain. We have already noted that diet has an effect on blood flow and blood flow an effect on brain function. However, the effect of diet goes beyond blood flow, what we eat becomes the building blocks for the brain and if we have poor quality or sparse building materials then we cannot expect to erect a building that will withstand all that is demanded of it. As good nutrition is an important factor in assisting the development of cognitive skills (Stein & Susser, 1985; Simeon & Grantham-McGregor, 1990; Wachs et al, 1993; Morley & Lucas, 1997; Schmitt et al, 2005; Fuglestad et al, 2008; Gomez-Pinilla, 2008; Isaacs & Oates, 2008; Jockers, 2012; Zainuddin & Thuret, 2012; Cortright, 2015) educational establishments should do all they can to ensure that the meals they provide are nutritious and that all readily available sources of junk food are eliminated.
Note: It has been shown that the consumption of small amounts of specific herbs and spices can have a positive impact on memory function (see, for example, Nutritionfacts.org)
Note: Perhaps the reason we do not yet have adequate neuroimaging of IEPMLD brains lies in the inability of this group to cope with the physical and cognitive demands of the present day neuroimaging technologies (see National Geographic, My Brilliant Brain, Episode 2 Accidental Genius, 2007). However, as technology advances, there will come a time when we are able to peer inside the brains of IEPMLD and devise improved systems for cognitive amelioration. The scans that have been achieved thus far, appear to show a very different brain wiring network (see National Geographic 'My Brilliant Brain' episode 2, 2007) but, even if this were proven to be the case for all this group (and that is by no means certain), it does not in any way preclude the possibility of progress in learning.
Note: More ideas for the development and assessment of memory are given on the 'history' page on this website.
Memory is an important component of 'contingency awareness' (cause and effect skills) which is covered in the section below ...
11. Contingency Awareness
"If we have discovered the learner with PMLD is beginning to learn about 'contingency awareness' then that should become central to all their learning. School children may be working on a range of curriculum activities and adult learners are likely to be involved in a range of community activities but what is required for all at this stage is for teachers and supporters to provide as many opportunities as possible to practice contingency awareness. This should be done throughout the day, preferably with a range of different resources so the person can learn to generalise his/her understanding in many different situations." (Lacey, 2015, page 45)
"This suggests that response-contingent learning opportunities, and especially for children who demonstrate few instrumental behavior, is warranted as a form of early childhood intervention" (Raab, Dunst, Wilson, & Parkey 2009)
"The interventions and results show that rather simple and easily implemented contingency learning games can have rather dramatic effects on child learning, which included extended benefits to both the child and his or her caregivers. Interestingly, many of the interventions used with young children with profound developmental delays and multiple disabilities do not include the promotion of child behavior competence (Dunst, Raab, Wilson, & Parkey, 2007; Winefield, 1983). Rather, the interventions typically involve non-contingent stimulation to evoke child behavior or passive manipulation of child movements."(Raab, Dunst, Wilson, & Parkey 2009)
"Research has shown that people with PMD are aware of or can be made aware of such contingencies (Lancioni et al., 2003; Saunders et al., 2003). Learning contingencies enables the individual to have control over his/her environment." (Petry et al, 2007c, page 132)
Contingency Awareness (often referred to as understanding 'cause and effect') is a consciousness of a relationship between two different events; that is, an understanding of a relationship between actions and the outcomes those actions elicit in the environment. A baby in a cot kicks its legs in a certain way and accidentally makes the mobile, suspended above the cot, move. After some repetitions of the leg kicking, the child begins to form an association between his actions (kicking his leg in a certain way) and the movement of the mobile. At this stage, the child may not understand how the action of his leg is causing the mobile movement but nevertheless still recognises that s/he can exert control and has thus made a connection.
Contingency Awareness is an important milestone for Individuals Experiencing PMLD. However, the combination of cognitive, physical and sensory impairments experienced by many acts as a obstacle to block the typically developing pathway. Indeed, the (inadvertent) actions of Significant Others may have a detrimental contributory effect further increasing the size of the obstacle. As Significant Others routinely:
"Learned helplessness occurs when it is unclear to the learner that he or she is able to exert control over the environment... For many learners, their social history has offered few opportunities to self-select desired objects, people, or activities. At meal times plates are prepared and distributed. Additional serving are provided automatically. Coats are handed out and doors opened when it is time to go. Thus, throughout the day, the caregivers do virtually everything for the learners. Initially, some learners may have attempted to self-select items of interest, but were actively encouraged not to do so." (Reichle, J. 1991 p.141)
"The children's physical disabilities place considerable restrictions on their personal development. There are activities in which they will be unable to participate, and many fields where they will gain only limited experience Part of this limitation is caused primarily not by the motor handicap, however, but by the fact that, due to negative experiences, they believe they are unable to do anything. Later on they will no longer try to do things that they perhaps would have been capable of. They learn that they are dependent on others because others do things for them which they would be unable to manage alone. At the same time they will experience that they are an inconvenience, that they are a hindrance and that the adults are most content when they are passive. The adults' attitude to the children, which the children to a great extent assume themselves (cf. Madge and Fassam 1982), therefore plays a significant role in forming their life and opportunities for personal growth." (Von Tetzchner, S. & Martinsen, H. 1992)
"All children are dependent upon adult caretakers for fulfillment of their physical and emotional needs. In the process of becoming autonomous, children explore and test their world and begin signalling their growing independence to caretakers through physical actions and spoken messages. If provided with an adequate climate for growth, an increasingly solid foundation for independence in adult life will be formed. However, for children with severe communication and/or physical limitations this process of self growth may be overlooked or suppressed. Because many children experiencing the aforementioned challenges are not able to signal their readiness for exploration or independence in traditional ways, parents and other caretakers (e.g. professional service providers, educators, etc.) are inclined to continue to act as direct or indirect agents for fulfilling the child's needs. When later provided with adequate means to express, query, or explore, (e.g. assistive technology) the child may persist in a more passive state due to learned helplessness or learned dependency." (Sweeney, L. 1993)
Over 100 years ago, in a 1895 publication, James Baldwin outlined a relationship between a child's beginning to see actions as the cause of environmental effects and increases in responses of a social/emotional nature such as excitement, laughter, and smiling. Likewise, in studying his own children, similar observations were made by Jean Piaget (1952). In support of these claims, Haith (1972) and McCall (1972) pointed out that, because such cognition is pleasurable, the ability of a child to understand s/he is the cause of a particular environmental consequence produces social-emotional behaviour.
Almost all IEPMLD show at least some contingency awareness:
The fact that these actions are repeated seems to be indicative of a connection between an action (slapping, rocking, flapping, tapping...) and an (internal) event (favourable sensation). In a sense, these actions, often viewed by staff members pejoratively, have, at least, a positive aspect: if a Learner is behaving in this manner then s/he must have made a connection and, having made one connection, the Learner must be capable of making other connections given the opportunity to do so.
The words 'given the opportunity' begs the questions: 'how do we give?' and 'what opportunities?'. This webpage hopes to provide at least some answers to those questions. One avenue, worthy of further exploration, is the use of (switch activated) assistive technology as a means to this end. This has been recognised since the earlier days of electronic assistive technology:
Research has demonstrated that switch technology can be used successfully to facilitate the formation of contingency awareness in individuals with severe and/or multiple disabilities. (York, Nietupski, & Hamre-Nietupski, 1985)
"I have suggested that learning contingency awareness via microswitch control might be a valuable approach with multiply impaired students." (Goldbart, 1994, page 57)
It is extremely important that this area of development is addressed by providing frequent, structured opportunities to help Learners gain an understanding of contingency awareness and, thus, discover that they can exercise control over their surroundings and others in their surroundings. Included on this webpage are a number of suggestions for ways to assist with the development of contingency awareness. You are, of course, free to adopt, adapt or abrogate any of them. However, Talksense hopes that at least some of what follows will inspire your thinking.
"This suggests that response-contingent learning opportunities, and especially for children who demonstrate few instrumental behavior, is warranted as a form of early childhood intervention" (Raab, Dunst, Wilson, & Parkey 2009)
"The interventions and results show that rather simple and easily implemented contingency learning games can have rather dramatic effects on child learning, which included extended benefits to both the child and his or her caregivers. Interestingly, many of the interventions used with young children with profound developmental delays and multiple disabilities do not include the promotion of child behavior competence (Dunst, Raab, Wilson, & Parkey, 2007; Winefield, 1983). Rather, the interventions typically involve non-contingent stimulation to evoke child behavior or passive manipulation of child movements."(Raab, Dunst, Wilson, & Parkey 2009)
"Research has shown that people with PMD are aware of or can be made aware of such contingencies (Lancioni et al., 2003; Saunders et al., 2003). Learning contingencies enables the individual to have control over his/her environment." (Petry et al, 2007c, page 132)
Contingency Awareness (often referred to as understanding 'cause and effect') is a consciousness of a relationship between two different events; that is, an understanding of a relationship between actions and the outcomes those actions elicit in the environment. A baby in a cot kicks its legs in a certain way and accidentally makes the mobile, suspended above the cot, move. After some repetitions of the leg kicking, the child begins to form an association between his actions (kicking his leg in a certain way) and the movement of the mobile. At this stage, the child may not understand how the action of his leg is causing the mobile movement but nevertheless still recognises that s/he can exert control and has thus made a connection.
Contingency Awareness is an important milestone for Individuals Experiencing PMLD. However, the combination of cognitive, physical and sensory impairments experienced by many acts as a obstacle to block the typically developing pathway. Indeed, the (inadvertent) actions of Significant Others may have a detrimental contributory effect further increasing the size of the obstacle. As Significant Others routinely:
- anticipate and fulfill the needs of the IEPMLD (Individual Experiencing Profound and Multiple Learning Difficulties);
- block access to experimentation by the IEPMLD;
"Learned helplessness occurs when it is unclear to the learner that he or she is able to exert control over the environment... For many learners, their social history has offered few opportunities to self-select desired objects, people, or activities. At meal times plates are prepared and distributed. Additional serving are provided automatically. Coats are handed out and doors opened when it is time to go. Thus, throughout the day, the caregivers do virtually everything for the learners. Initially, some learners may have attempted to self-select items of interest, but were actively encouraged not to do so." (Reichle, J. 1991 p.141)
"The children's physical disabilities place considerable restrictions on their personal development. There are activities in which they will be unable to participate, and many fields where they will gain only limited experience Part of this limitation is caused primarily not by the motor handicap, however, but by the fact that, due to negative experiences, they believe they are unable to do anything. Later on they will no longer try to do things that they perhaps would have been capable of. They learn that they are dependent on others because others do things for them which they would be unable to manage alone. At the same time they will experience that they are an inconvenience, that they are a hindrance and that the adults are most content when they are passive. The adults' attitude to the children, which the children to a great extent assume themselves (cf. Madge and Fassam 1982), therefore plays a significant role in forming their life and opportunities for personal growth." (Von Tetzchner, S. & Martinsen, H. 1992)
"All children are dependent upon adult caretakers for fulfillment of their physical and emotional needs. In the process of becoming autonomous, children explore and test their world and begin signalling their growing independence to caretakers through physical actions and spoken messages. If provided with an adequate climate for growth, an increasingly solid foundation for independence in adult life will be formed. However, for children with severe communication and/or physical limitations this process of self growth may be overlooked or suppressed. Because many children experiencing the aforementioned challenges are not able to signal their readiness for exploration or independence in traditional ways, parents and other caretakers (e.g. professional service providers, educators, etc.) are inclined to continue to act as direct or indirect agents for fulfilling the child's needs. When later provided with adequate means to express, query, or explore, (e.g. assistive technology) the child may persist in a more passive state due to learned helplessness or learned dependency." (Sweeney, L. 1993)
Over 100 years ago, in a 1895 publication, James Baldwin outlined a relationship between a child's beginning to see actions as the cause of environmental effects and increases in responses of a social/emotional nature such as excitement, laughter, and smiling. Likewise, in studying his own children, similar observations were made by Jean Piaget (1952). In support of these claims, Haith (1972) and McCall (1972) pointed out that, because such cognition is pleasurable, the ability of a child to understand s/he is the cause of a particular environmental consequence produces social-emotional behaviour.
Almost all IEPMLD show at least some contingency awareness:
- Those that hit themselves or poke themselves in the eyes must be 'aware' that doing so brings sensory stimulation: they have made the link between the action (self harm) and response (sensory stimulation);
- Those that rock back and forth must be doing this for some reason. It is generally assumed that this is stimulatory behaviour which brings some reward. At some point the individual must have made this connection and continued the behaviour;
- Those that twirl or flap objects by their eyes or their face at every available moment must have, at some prior point, made a connection between the action and a favourable sensation.
- Those that will reach out and repeatedly tap a switch surface must be doing it continually (until they grow tired of it or until the switch is removed) for some reason. It must be providing the person with some sensory feedback which is fulfilling / motivating in some way.
The fact that these actions are repeated seems to be indicative of a connection between an action (slapping, rocking, flapping, tapping...) and an (internal) event (favourable sensation). In a sense, these actions, often viewed by staff members pejoratively, have, at least, a positive aspect: if a Learner is behaving in this manner then s/he must have made a connection and, having made one connection, the Learner must be capable of making other connections given the opportunity to do so.
The words 'given the opportunity' begs the questions: 'how do we give?' and 'what opportunities?'. This webpage hopes to provide at least some answers to those questions. One avenue, worthy of further exploration, is the use of (switch activated) assistive technology as a means to this end. This has been recognised since the earlier days of electronic assistive technology:
Research has demonstrated that switch technology can be used successfully to facilitate the formation of contingency awareness in individuals with severe and/or multiple disabilities. (York, Nietupski, & Hamre-Nietupski, 1985)
"I have suggested that learning contingency awareness via microswitch control might be a valuable approach with multiply impaired students." (Goldbart, 1994, page 57)
It is extremely important that this area of development is addressed by providing frequent, structured opportunities to help Learners gain an understanding of contingency awareness and, thus, discover that they can exercise control over their surroundings and others in their surroundings. Included on this webpage are a number of suggestions for ways to assist with the development of contingency awareness. You are, of course, free to adopt, adapt or abrogate any of them. However, Talksense hopes that at least some of what follows will inspire your thinking.
12. Reduction of Passivity and Learned Helplessness

All things come to those who wait (French Proverb)
"The risks of professional domination are significant: encouraging 'learned helplessness' (Seligman M. 1984); increasing a learner's passivity (Hooker C. 1976); and creating problems associated with learner compliance and satisfaction." (Smith-Lewis M. & Ford A. 1987)
"These learners either showed no interest in their environments or were able to participate in the environment without engaging in communicative behaviour. This condition has been referred to as learned helplessness." (Reichle J. 1991)
"The dependence associated with language learning is related to the degree of passivity and dependence on others found in all groups in need of augmentative communication. People who belong to the expressive language group share the characteristic that, in the majority of situations and especially with regard to self expression, they have been dependent on other people helping them. This antecedent creates habits and ways of adapting to communication that may be difficult to alter when one attempts to give them new means of expressing themselves." (Von Tetzchner S. & Martinsen H. 1992)
"The counselor's task in the former situation of learned helplessness is an extremely difficult one. I have to confess that unless such people have a reason to be dissatisfied with a life-long dependent position I have not yet found ways of reducing the threat of a real change on this dimension. Sometimes, however, the dependency is less widespread and areas may be found where they are willing and able to stand on their own two feet. Someone who concedes all conversations to a partner when in company may speak up at work or when responsible for children." (Dalton P. 1994 page 58)
Passivity is commonplace among people with a severe communication impairment. In a study by Sweeney (1991) 42 out of 50 users of alternative forms of communication showed some level of learned helplessness when interacting with one or more significant others. The more severe the communication impairment the greater the degree of helplessness. It would appear that, the development of an individual's ability to communicate is somehow related to an individual's ability to act independently. The factors that are involved in creating an atmosphere that is supportive of communication are also the factors that tend to demand more interactive skills of an individual. The relationship is reciprocal: greater communicative ability may lead to greater independence and greater independence may lead to greater communicative ability. Likewise, if we turn the previous statement on its head, less communicative ability may foster an atmosphere that makes others act in ways which lead, directly or indirectly, to increasing Learner passivity.
Prevention is better than cure: the role of building communication skills in the avoidance of personal passivity should be stressed:
"Without an effective means of communication during childhood development of autonomy, exploratory/experiential opportunity, and relative strength of self-image/esteem will be compromised." (Sweeney L. 1993)
However well written, structured, or sound a program of work and study may be, without the right attitude of the people who have to implement the strategies developed, it will be doomed to failure. It is therefore incumbent on the management team to ensure that all staff interact with Learners in a manner that fosters the growth of communication skills. It is the attitudes, knowledge, understanding, and abilities of significant others that will contribute most to the success (or failure) of the development of communication skills in the Learner. Candappa and Burgess (1989) have shown how the perceptions and attitudes of Significant Others play a primary role in the normalisation of people with a cognitive impairment. They argue:
"Our own study, ...... strongly suggests that addressing the values and perceptions of carers is one of the primary tasks of normalisation." (Candappa & Burgess 1989)
This is supported by Sweeney (1993):
"All children are dependent upon adult caretakers for fulfillment of their physical and emotional needs. In the process of becoming autonomous, children explore and test their world and begin signalling their growing independence to caretakers through physical actions and spoken messages. If provided with an adequate climate for growth, an increasingly solid foundation for independence in adult life will be formed. However, for children with severe communication and/or physical limitations this process of self growth may be overlooked or suppressed. Because many children experiencing the aforementioned challenges are not able to signal their readiness for exploration or independence in traditional ways, parents and other caretakers (e.g. professional service providers, educators, etc.) are inclined to continue to act as direct or indirect agents for fulfilling the child's needs. When later provided with adequate means to express, query, or explore, (e.g. assistive technology) the child may persist in a more passive state due to learned helplessness or learned dependency." (Sweeney, 1993)
"For children who grow up with motor disorders, the difficulties they experience in moving and speaking and the influence from their environment both contribute to the development of a passive style. These children often place great demands on their parents. Training, feeding and washing take up a lot of time, and there are few activities that the children and their parents can take part in together. Even when the children are small, their parents consider them to be happiest when they are passive. ‘She's as quiet as an angel', and, ‘She is so good', are typical remarks made by mothers about their small children with cerebral palsy." (Von Tetzchner & Martinsen,1992) (See also Shere & Kastenbaum,1966)
For Learners to be successful in learning about and acquiring control skills, they have to have an understanding that they can affect their world. The very institutionalisation of some settings may, however, reinforce user passivity. Only when there is a change in institutional practices, reflected through the attitudes of the staff, will any progress be made. A person for whom all needs are provided (according to a timetable) may not have any motivation to take control.
"Learned helplessness occurs when it is unclear to the learner that he or she is able to exert control over the environment... For many learners, their social history has offered few opportunities to self-select desired objects, people, or activities. At meal times plates are prepared and distributed. Additional serving are provided automatically. Coats are handed out and doors opened when it is time to go. Thus, throughout the day, the caregivers do virtually everything for the learners. Initially, some learners may have attempted to self-select items of interest, but were actively encouraged not to do so." (Reichle, 1991 p.141)
It may only be through the creation of anomaly, of discord in the daily routine, that such motivation is created. A routine that has been developed to ease the load on both staff and student can discourage the development of active self-development skills. If life is presented to a person ‘on a plate’ such that the person learns ‘all will come to he who waits’, and ‘there is a time and place for everything’, there is little need nor opportunity to be active. The individual learns that the desired event will happen regardless and to demand it at any other time would be met by an ‘It’s not time yet’ type of response. There needs to be some deviation from the routine to create both the desire and the opportunity to be active.
There is a difference between environments that promote active Learners and environments that promote passive Learners. This difference is nothing to do with the level of caring or the the qualifications of the staff or even the cleanliness of the environment. Indeed, an active environment may,by its very nature, be more untidy than its passive equivalent. It is 'Active Environments' that promote 'Active Learners' and 'Passive Environments' that promote passivity. The latter is very rarely intentional: more often than not, it it an unwanted side-effect of establishments policy, procedure and practice.
In an Active Environment there is evidence of staff encouragement of cognitive engagement of Learners. The list below details some of the attributes of both active and passive environments. If you think of think of things that are missing please contact TalkSense and let us know and we will add to the lists below. The more items that can be ticked from any one list the more it is likely that the establishment is either 'active' or 'passive'.
"The risks of professional domination are significant: encouraging 'learned helplessness' (Seligman M. 1984); increasing a learner's passivity (Hooker C. 1976); and creating problems associated with learner compliance and satisfaction." (Smith-Lewis M. & Ford A. 1987)
"These learners either showed no interest in their environments or were able to participate in the environment without engaging in communicative behaviour. This condition has been referred to as learned helplessness." (Reichle J. 1991)
"The dependence associated with language learning is related to the degree of passivity and dependence on others found in all groups in need of augmentative communication. People who belong to the expressive language group share the characteristic that, in the majority of situations and especially with regard to self expression, they have been dependent on other people helping them. This antecedent creates habits and ways of adapting to communication that may be difficult to alter when one attempts to give them new means of expressing themselves." (Von Tetzchner S. & Martinsen H. 1992)
"The counselor's task in the former situation of learned helplessness is an extremely difficult one. I have to confess that unless such people have a reason to be dissatisfied with a life-long dependent position I have not yet found ways of reducing the threat of a real change on this dimension. Sometimes, however, the dependency is less widespread and areas may be found where they are willing and able to stand on their own two feet. Someone who concedes all conversations to a partner when in company may speak up at work or when responsible for children." (Dalton P. 1994 page 58)
Passivity is commonplace among people with a severe communication impairment. In a study by Sweeney (1991) 42 out of 50 users of alternative forms of communication showed some level of learned helplessness when interacting with one or more significant others. The more severe the communication impairment the greater the degree of helplessness. It would appear that, the development of an individual's ability to communicate is somehow related to an individual's ability to act independently. The factors that are involved in creating an atmosphere that is supportive of communication are also the factors that tend to demand more interactive skills of an individual. The relationship is reciprocal: greater communicative ability may lead to greater independence and greater independence may lead to greater communicative ability. Likewise, if we turn the previous statement on its head, less communicative ability may foster an atmosphere that makes others act in ways which lead, directly or indirectly, to increasing Learner passivity.
Prevention is better than cure: the role of building communication skills in the avoidance of personal passivity should be stressed:
"Without an effective means of communication during childhood development of autonomy, exploratory/experiential opportunity, and relative strength of self-image/esteem will be compromised." (Sweeney L. 1993)
However well written, structured, or sound a program of work and study may be, without the right attitude of the people who have to implement the strategies developed, it will be doomed to failure. It is therefore incumbent on the management team to ensure that all staff interact with Learners in a manner that fosters the growth of communication skills. It is the attitudes, knowledge, understanding, and abilities of significant others that will contribute most to the success (or failure) of the development of communication skills in the Learner. Candappa and Burgess (1989) have shown how the perceptions and attitudes of Significant Others play a primary role in the normalisation of people with a cognitive impairment. They argue:
"Our own study, ...... strongly suggests that addressing the values and perceptions of carers is one of the primary tasks of normalisation." (Candappa & Burgess 1989)
This is supported by Sweeney (1993):
"All children are dependent upon adult caretakers for fulfillment of their physical and emotional needs. In the process of becoming autonomous, children explore and test their world and begin signalling their growing independence to caretakers through physical actions and spoken messages. If provided with an adequate climate for growth, an increasingly solid foundation for independence in adult life will be formed. However, for children with severe communication and/or physical limitations this process of self growth may be overlooked or suppressed. Because many children experiencing the aforementioned challenges are not able to signal their readiness for exploration or independence in traditional ways, parents and other caretakers (e.g. professional service providers, educators, etc.) are inclined to continue to act as direct or indirect agents for fulfilling the child's needs. When later provided with adequate means to express, query, or explore, (e.g. assistive technology) the child may persist in a more passive state due to learned helplessness or learned dependency." (Sweeney, 1993)
"For children who grow up with motor disorders, the difficulties they experience in moving and speaking and the influence from their environment both contribute to the development of a passive style. These children often place great demands on their parents. Training, feeding and washing take up a lot of time, and there are few activities that the children and their parents can take part in together. Even when the children are small, their parents consider them to be happiest when they are passive. ‘She's as quiet as an angel', and, ‘She is so good', are typical remarks made by mothers about their small children with cerebral palsy." (Von Tetzchner & Martinsen,1992) (See also Shere & Kastenbaum,1966)
For Learners to be successful in learning about and acquiring control skills, they have to have an understanding that they can affect their world. The very institutionalisation of some settings may, however, reinforce user passivity. Only when there is a change in institutional practices, reflected through the attitudes of the staff, will any progress be made. A person for whom all needs are provided (according to a timetable) may not have any motivation to take control.
"Learned helplessness occurs when it is unclear to the learner that he or she is able to exert control over the environment... For many learners, their social history has offered few opportunities to self-select desired objects, people, or activities. At meal times plates are prepared and distributed. Additional serving are provided automatically. Coats are handed out and doors opened when it is time to go. Thus, throughout the day, the caregivers do virtually everything for the learners. Initially, some learners may have attempted to self-select items of interest, but were actively encouraged not to do so." (Reichle, 1991 p.141)
It may only be through the creation of anomaly, of discord in the daily routine, that such motivation is created. A routine that has been developed to ease the load on both staff and student can discourage the development of active self-development skills. If life is presented to a person ‘on a plate’ such that the person learns ‘all will come to he who waits’, and ‘there is a time and place for everything’, there is little need nor opportunity to be active. The individual learns that the desired event will happen regardless and to demand it at any other time would be met by an ‘It’s not time yet’ type of response. There needs to be some deviation from the routine to create both the desire and the opportunity to be active.
There is a difference between environments that promote active Learners and environments that promote passive Learners. This difference is nothing to do with the level of caring or the the qualifications of the staff or even the cleanliness of the environment. Indeed, an active environment may,by its very nature, be more untidy than its passive equivalent. It is 'Active Environments' that promote 'Active Learners' and 'Passive Environments' that promote passivity. The latter is very rarely intentional: more often than not, it it an unwanted side-effect of establishments policy, procedure and practice.
In an Active Environment there is evidence of staff encouragement of cognitive engagement of Learners. The list below details some of the attributes of both active and passive environments. If you think of think of things that are missing please contact TalkSense and let us know and we will add to the lists below. The more items that can be ticked from any one list the more it is likely that the establishment is either 'active' or 'passive'.
|
ACTIVE
Cognitively Engagement; Communicative Learners; Language and communication is a focus; Learner Choices; Learners take decisions and staff respond; Learners encouraged to D-I-Y; Learners are given responsibilities; Fly-swatting is avoided; Symbols on Switches; Hold on Help... hang back; Inclusion, involvement, ideas, ... independence and integration; Most Learner time on-task; Learners are motivated (intrinsically amd extrinsically); All Learners working in sessions; Learners know when they are successful; Environment is engineered for learning; Environment is 'Responsive'; Self Stimulatory behaviour is reduced (or eliminated); Staff use open questions; Critical thinking and exploration; Pause on Prompting; Questions (from Learners); Staff use descriptive question types; Timetabling flexibility; Staff expectations are high; Staff expect participation by all; Multi-disciplinary approach; Verifcation of Learner Understanding; Open to change and to challenge; Higher demands on staff |
PASSIVE
Lack of cognitive engagement; Learners are mostly silent; Silence is golden; Functional communication seen as sufficient; Hobson's choice; Staff take decisions and Learners follow; Learners discouraged to try things for themselves; Learners do not have responsibilities for tasks and chores; Evidence of fly-swatting; Switches and BIGmacks have no symbols or sensory surfaces. Staff are too helpful; they do not allow time for Learners to DIY; Little evidence of a movement towards the three I's; Learners allowed to spend lot of time off task; Learner Queuing Lack of Learner motivation; Learners watching videos or Television during teaching sessions; Little Learner feedback; Environment is supportive of learning; Environment is not 'Responsive'; Self Stimulatory Behaviour is evident and problematic; Staff use closed questions; Rote learning and copying; Lots of intrusive prompting; Lack of Learner questioning; Staff use referential question types; Strict adherence to a timetable; Staff expectations are low; Staff do not ensure participation by all; Staff tend to plan and work in isolation; Unverified assumptions of understanding by Significant Others; Unwillingness to embrace change; Lower demands on staff |
While not all of the above are applicable to classes for IEPMLD, the lists provide a means of assessing an establishment's overall active/passive rating. If you believe that your situation promotes passivity and does not action activity then you need to commit to change.
13. Intensive Interaction
Intensive interaction is a system for working with and teaching the fundamentals of communication to individuals who have profound learning difficulties. Developed during the eighties by the team of staff working at Harperbury Hospital School Herfordshire (notably Dave Hewett and Melanie Nind), this approach has been widely researched and has numerous articles, research papers and books written on its use and its efficacy (See for example:Hewett & Nind, 1993; Nind, 1993; Hewett, 1996; Watson & Fisher, 1997; Jones & Williams, 1998; Lovell, Jones & Ephraim, 1998; Kellett, 2000; Cameron & Bell, 2001; Elgie & Maguire, 2001; Kennedy, 2001; Samuel, 2003; Culham, 2004; Firth, 2006; Barber, 2007; Crabbe, 2007; Firth, 2008).
As there is so much information on this approach available on line, rather than attempt to cover it here as a meaningful approach, I will simply provide a set of links to other sites to follow. Simply click on any link to open a new webpage:
As there is so much information on this approach available on line, rather than attempt to cover it here as a meaningful approach, I will simply provide a set of links to other sites to follow. Simply click on any link to open a new webpage:
- http://www.intensiveinteraction.co.uk/
- http://www.bild.org.uk/information/factsheets/ (download the factsheet on Intensive Interaction)
- http://davehewett.com/about-intensive-interaction/
- https://en.wikipedia.org/wiki/Intensive_interaction
- http://www.allsortsglos.org.uk/Documents/intensive%20interaction.pdf
- So what is Intensive interaction: YouTube
14. Co-Active Interaction
Co-Active Interaction is a development of Intensive Interaction. It does not seek to replace Intensive Interaction nor suggest it to be unnecessary. Like Intensive Interaction, Co-active Interaction (CI) takes place between a staff member and a Learner. However, instead of mirroring a Learner's lead CI allows for staff to assist the Learner to make appropriate responses to develop 'contingency awareness'.
CI can take many forms, only one of which will be detailed here as an example. The idea is for staff and Learner to have fun while, at the same time, assisting the Learner to understand cause and effect relationships and to take control of the situation.
In this example, staff and student are sitting face to face on the floor. It is known that the student enjoys rocking back and forth to music. In this instance the music is supplied by a BIGmack (a simple technology communication device from AbleNet) for an eight second (eight is great) burst. On the surface of the BIGmack has been mounted a tactile top (available from Ability-World) representing the concept 'more'. The staff member assists the student to activate the BIGmack using 'hand-under-hand' techniques. The music begins to play and staff and student work together 'co-actively' rocking back and forth to the music. When the music stops, the staff member once again assists the Learner to activate the BIGmack such that the fun may continue. This may be repeated several times as necessary. However, after a few repetitions, the staff member waits for a few seconds before assisting in the hope that the Learner will take control and active the BIGmack him/herself without assistance. The staff member may prompt the Learner by gaining eye contact and then looking at the BIGmack using exaggerated head movements or even moving his/her hand towards the device in an attempt to model what action is necessary. However, if the learner does not respond, the staff member, once again, assists the Learner to activate the switch. Each time the music stops, the staff member ceases the Co-active Interaction and sits still and waits, allowing time for the Learner to initiate the music and restart the activity. Each time the staff member should wait a little while longer (only a second or two) than previously before assisting the Learner in the activation.
Co-active Interaction:
In the example, the student is communicating a preference for 'more' of the activity and is, in so doing, taking control of the situation. The tactile top representing 'more' may also be utilised with the same student in other areas of the curriculum to assist with the transference of skills: For example, asking for 'more' while being assisted with eating and drinking during a meal break.
It may be that the activity in question does not require music or music would not be appropriate; in this instance the BIGmack might simply say the word 'Go' which would be the prompt to the staff member involved to begin working with the student. However, there is not a musical timing factor present and so the staff member him/herself would be required to 'freeze' (stop assisting) after a certain period of time until 'unfrozen' by a Learner's repeated request using the BIGmack to 'go'. Note: the word 'go' is not sacrosanct; it could be 'start', 'now', 'more', 'again' ...
CI can take many forms, only one of which will be detailed here as an example. The idea is for staff and Learner to have fun while, at the same time, assisting the Learner to understand cause and effect relationships and to take control of the situation.
In this example, staff and student are sitting face to face on the floor. It is known that the student enjoys rocking back and forth to music. In this instance the music is supplied by a BIGmack (a simple technology communication device from AbleNet) for an eight second (eight is great) burst. On the surface of the BIGmack has been mounted a tactile top (available from Ability-World) representing the concept 'more'. The staff member assists the student to activate the BIGmack using 'hand-under-hand' techniques. The music begins to play and staff and student work together 'co-actively' rocking back and forth to the music. When the music stops, the staff member once again assists the Learner to activate the BIGmack such that the fun may continue. This may be repeated several times as necessary. However, after a few repetitions, the staff member waits for a few seconds before assisting in the hope that the Learner will take control and active the BIGmack him/herself without assistance. The staff member may prompt the Learner by gaining eye contact and then looking at the BIGmack using exaggerated head movements or even moving his/her hand towards the device in an attempt to model what action is necessary. However, if the learner does not respond, the staff member, once again, assists the Learner to activate the switch. Each time the music stops, the staff member ceases the Co-active Interaction and sits still and waits, allowing time for the Learner to initiate the music and restart the activity. Each time the staff member should wait a little while longer (only a second or two) than previously before assisting the Learner in the activation.
Co-active Interaction:
- is a fun activity for the student;
- is, initially, staff controlled but aims to pass control as early as possible to the student;
- requires an external 'controlling mechanism' that is easily accessible by the student;
- can continue for as long as the student finds it motivating;
- can 'ADE' (Assess, Develop [Awareness and Skills], Evidence [ student learning and abilities]) students.
In the example, the student is communicating a preference for 'more' of the activity and is, in so doing, taking control of the situation. The tactile top representing 'more' may also be utilised with the same student in other areas of the curriculum to assist with the transference of skills: For example, asking for 'more' while being assisted with eating and drinking during a meal break.
It may be that the activity in question does not require music or music would not be appropriate; in this instance the BIGmack might simply say the word 'Go' which would be the prompt to the staff member involved to begin working with the student. However, there is not a musical timing factor present and so the staff member him/herself would be required to 'freeze' (stop assisting) after a certain period of time until 'unfrozen' by a Learner's repeated request using the BIGmack to 'go'. Note: the word 'go' is not sacrosanct; it could be 'start', 'now', 'more', 'again' ...
15. More Please Sir

"Child as he was, he was desperate with hunger, and reckless with misery. He rose from the table; and advancing to the master, basin and spoon in hand, said: somewhat alarmed at his own temerity:
'Please, sir, I want some more'."
(Dickens, Oliver Twist, first published as a serial 1837–39)
Oliver here is trying to take control of the situation in which he has no control. The concept of 'more' is an important one for IEPMLD to begin to understand and to use appropriately. Over many years, some Learners will have 'learned helplessness' (see section this page) and become passive waiting for others to provide for their needs. Other Learners may have turned to behaviours that staff may find challenging to communicate a desire for staff attention (see section on behaviour this webpage)
'Please, sir, I want some more'."
(Dickens, Oliver Twist, first published as a serial 1837–39)
Oliver here is trying to take control of the situation in which he has no control. The concept of 'more' is an important one for IEPMLD to begin to understand and to use appropriately. Over many years, some Learners will have 'learned helplessness' (see section this page) and become passive waiting for others to provide for their needs. Other Learners may have turned to behaviours that staff may find challenging to communicate a desire for staff attention (see section on behaviour this webpage)
16. Objects Of Reference
An Object Of Reference (OOR) is typically a tangible, thee-dimensional object that is utilised by a Significant Other to represent a POLE (Person, Object, Location or Event) for purposes of communication at a very basic level. By presenting a specific OOR to a Learner and ensuring it is always immediately followed by the same POLE each time, it is hoped that the Learner will eventually come to understand that the OOR represents the POLE.
For example, if a Learner liked to go to the local park and take a turn on the swings, then an object could be chosen to indicate that this location/event was to follow. What object could be used for going to the park? That depends on why the Learner likes going there: is it the flowers (we could use a plastic flower), feeding the ducks (we could use a rubber duck), the playground (we could use a toy swing or roundabout), or something else? For an object to represent a POLE, it has to become associated with it in the mind of the Learner. Using what is considered by staff to be a representative object in this way does not mean that the Learner will comprehend its meaning. Simply because it's obvious to staff that a 'riding cap' stands for horse riding (for example), it does not follow that this is obvious to the Learner. Thus, staff should not simply assume but rather teach the connection.
Objects Of Reference are covered in great depth on the Objects Of Reference page of this website. Thus, they will not be addressed further here. Click on the image (above left) to open the OOR page.
For example, if a Learner liked to go to the local park and take a turn on the swings, then an object could be chosen to indicate that this location/event was to follow. What object could be used for going to the park? That depends on why the Learner likes going there: is it the flowers (we could use a plastic flower), feeding the ducks (we could use a rubber duck), the playground (we could use a toy swing or roundabout), or something else? For an object to represent a POLE, it has to become associated with it in the mind of the Learner. Using what is considered by staff to be a representative object in this way does not mean that the Learner will comprehend its meaning. Simply because it's obvious to staff that a 'riding cap' stands for horse riding (for example), it does not follow that this is obvious to the Learner. Thus, staff should not simply assume but rather teach the connection.
Objects Of Reference are covered in great depth on the Objects Of Reference page of this website. Thus, they will not be addressed further here. Click on the image (above left) to open the OOR page.
17. Doorways: D-OOR-Ways

D-oor-ways, as it's name suggests, may form a part of an OOR system. The system comprises a set of drop-in slots mounted on on proximal to the entrance to rooms or areas of the college in which activities are to take place. The slot is formed by a three sided U-shaped frame into which a piece of plastic or hardboard can easily be dropped and removed. These drop-ins are typically neutral in colour and are there to provide a surface on to which an OOR may be permanently mounted (using glue for example). If an area serves one purpose only the 'slider' need never be changed. For example, the toilets, the physiotherapy room, the nurse's office, the staff room, etc may all have permanent sliders in position. However, most working areas in colleges do not only have one function and change subjects throughout the working day. Here the sliding plate comes into its own; as subjects change so the staff member with responsibility for that session swaps the plate for the appropriate d-oor-way. To facilitate this, a box of slider plates should be available within the room. Each of the slider plates in the box housing an OOR for one of the subjects taking place in that area during the week such that it takes only a matter of seconds for a staff member to locate and display the correct three dimensional representation of the subject at the entrance to the area.
An IEPMLD arriving at the room will be carrying an OOR. The Learner should be encouraged to match the OOR to the d-oor-way and shown (told and signed) that they are the same before entering the working area. The d-oor-way does not replace symbol labels for there can also be an additional symbolic marker also displayed at the entrance for those students who so require it. The same applies to a text label, indeed, to any other form of communicative system of representation in use in the college.
While d-oor-ways are specifically intended to support the learning requirements of IEPMLD they may also benefit other Learners within the college and, indeed, staff too. They are easily seen and recognised and, for those that have issues of visual acuity, provide a tactile point of reference.
D-oor-way sliders may be made by anyone with sufficient craft skills or, alternatively may be purchased ready-made from Ability-World.
What if the Learners pull the objects off the slider plates?
That does happen from time to time but it's typically infrequent. In that instance, you have no recourse other than to reattach the object to the plate using glue or some other suitable method of fixing.
We are NOT allowed to attach items to doors or walls in our establishment not even with Velcro.
I have come across this problem before and I find it problematic that a place of education is thus handicapped. However, if this is the case, and there is room, you might consider creating some free standing posts onto which such a system might be mounted. If there is a rail (or some other such suitable appendage) the d-oor-way can be affixed using Velcro straps or some form of hooking such that the system can be hooked over the rail.
An IEPMLD arriving at the room will be carrying an OOR. The Learner should be encouraged to match the OOR to the d-oor-way and shown (told and signed) that they are the same before entering the working area. The d-oor-way does not replace symbol labels for there can also be an additional symbolic marker also displayed at the entrance for those students who so require it. The same applies to a text label, indeed, to any other form of communicative system of representation in use in the college.
While d-oor-ways are specifically intended to support the learning requirements of IEPMLD they may also benefit other Learners within the college and, indeed, staff too. They are easily seen and recognised and, for those that have issues of visual acuity, provide a tactile point of reference.
D-oor-way sliders may be made by anyone with sufficient craft skills or, alternatively may be purchased ready-made from Ability-World.
What if the Learners pull the objects off the slider plates?
That does happen from time to time but it's typically infrequent. In that instance, you have no recourse other than to reattach the object to the plate using glue or some other suitable method of fixing.
We are NOT allowed to attach items to doors or walls in our establishment not even with Velcro.
I have come across this problem before and I find it problematic that a place of education is thus handicapped. However, if this is the case, and there is room, you might consider creating some free standing posts onto which such a system might be mounted. If there is a rail (or some other such suitable appendage) the d-oor-way can be affixed using Velcro straps or some form of hooking such that the system can be hooked over the rail.
18. Sensory Cues
Back in 1991, Sally Clark (page 17) wrote:
"If any interaction with the environment and adults is to be meaningful it is necessary to ensure that the school is kept as stimulating as possible. Each room, or part of a room, should retain its own atmosphere and smells. It is also important that certain activities always take place in certain areas so that the child may come to a sense of anticipation when moved to that area... A visually impaired child may also receive his cues from smells and different textures."
What Clark is outlining here is the basis for Sensory Cueing. Sensory Cueing is a technique that assists an IEPMLD to reference a particular POLE (Person Object Location or Event/Experience) through Environmental Engineering (See section 15 below). Under the Sensory Cueing technique, a particular sensation (sight, sound smell, taste, feeling, etc.) is managed consistently such that it begins to be associated with a specific occurrence, for example:
Sensory Cueing is covered in greater depth on the Multi-Sensory Referencing page of this website.
"If any interaction with the environment and adults is to be meaningful it is necessary to ensure that the school is kept as stimulating as possible. Each room, or part of a room, should retain its own atmosphere and smells. It is also important that certain activities always take place in certain areas so that the child may come to a sense of anticipation when moved to that area... A visually impaired child may also receive his cues from smells and different textures."
What Clark is outlining here is the basis for Sensory Cueing. Sensory Cueing is a technique that assists an IEPMLD to reference a particular POLE (Person Object Location or Event/Experience) through Environmental Engineering (See section 15 below). Under the Sensory Cueing technique, a particular sensation (sight, sound smell, taste, feeling, etc.) is managed consistently such that it begins to be associated with a specific occurrence, for example:
- Personal care areas may be given a particular (pleasant) smell. The specific smell may then become associated with the events and experiences that an individual encounters in that particular environment allowing the Learner to anticipate the procedures that will occur.
- Visiting a supermarket may be accompanied by assisting a Learner to feel the bars of the shopping trolley before entering the store. Continuing (consistent) exposure to such a technique may assist the Learner to anticipate and prepare for the forthcoming experience.
- Entering the physiotherapy area might be accompanied by a particular piece of music. As the Learner hears this piece of music every time physiotherapy is about to commence it begins to be associated with the activity and assists the Learner to prepare for the experience.
- A particular person can be immediately referenced if they present in the same unique way each time. This means it is better if staff stick to the same colour clothing, the same perfume or aftershave, the same hairstyle, or wear the same bracelet or badge... Of course, typically people do not do that; some people do not want to wear the same thing every day. However, it would be a better sensory cue if they did!
Sensory Cueing is covered in greater depth on the Multi-Sensory Referencing page of this website.
19. Tactile Tops and Tactile Symbols

It is one of TalkSense's switch rules (see page this website) that, where possible, all switches should be labelled with a symbol denoting the POLE (Person, Object, Location, or Event/Experience) controlled by its activation. However, not all learners will benefit from a visual symbol. IEPMLD may require the use of tactile tops rather than standard visual symbols to reference the POLE. While a wide range of such tactile symbols (as far as we are aware at the time of writing) is yet to be available from any commercial outlet, it is possible to produce your own fairly simply. Many popular commercially-produced switches come with a clear plastic 'symbol' cover sometimes called a 'snap cap'. In some instances the 'snap caps' require ordering separately. By spraying a film of adhesive through a template (simply made in best 'Blue Peter' fashion from a piece of card) onto the snap caps surface and then dropping, spreading, or otherwise attaching a sensory surface to the cap a 'Tactile Top' is produced. For example, in the image left a tactile top has been create by gluing a sandy surface to an AbleNet snap cap.
Tactile Tops are used in preference for individuals who for whatever reason do benefit from standard printed symbols. They must be used consistently for switch work to control any POLE. While there is no available list of tactile surfaces or tactile symbols to use with any particular POLE a number of suggestions are made on several other pages on this website. For example, when working with greetings in special education environments TalkSense uses a faux fur top made from the left hand of a pair of fur gloves. This was attached to the snap cap using Velcro rather than glue to allow for easy removal for washing. The right hand glove was worn by the staff member during the interchange with each Learner:
- Good Morning John (spoken and signed to Learner)
- Hand shaken with Learner while wearing the fur glove.
- BIGmack system with fur snap cap presented.
- Good morning spoken by Learner using BIGMack.
In this interchange the use of the fur glove provides a specific tactile feedback which is then directly and immediately associated with the fur on the BIGmack used to provide a audible response from the Learner.
Other examples might be:
While tactile tops may be used for switches and low tech single message communication aids, tactile symbols have wider communicative and cognitive applications. MORE HERE
*****************************************************************************
Tactile Tops are used in preference for individuals who for whatever reason do benefit from standard printed symbols. They must be used consistently for switch work to control any POLE. While there is no available list of tactile surfaces or tactile symbols to use with any particular POLE a number of suggestions are made on several other pages on this website. For example, when working with greetings in special education environments TalkSense uses a faux fur top made from the left hand of a pair of fur gloves. This was attached to the snap cap using Velcro rather than glue to allow for easy removal for washing. The right hand glove was worn by the staff member during the interchange with each Learner:
- Good Morning John (spoken and signed to Learner)
- Hand shaken with Learner while wearing the fur glove.
- BIGmack system with fur snap cap presented.
- Good morning spoken by Learner using BIGMack.
In this interchange the use of the fur glove provides a specific tactile feedback which is then directly and immediately associated with the fur on the BIGmack used to provide a audible response from the Learner.
Other examples might be:
- sponge for water based activities;
- sand for play;
- guitar strings for music.
- the tops are used consistently in all areas;
- the staff can readily access the necessary tops (ten second rule) to support consistency;
- their are tops available for the varying sizes of switches in use which may mean a regular and large version of each tactile top is made available;
- the tops are labelled on the underside stating their function and where they reside (if they go missing!).
While tactile tops may be used for switches and low tech single message communication aids, tactile symbols have wider communicative and cognitive applications. MORE HERE
*****************************************************************************
20. Environmental Engineering
 Just going to engineer the environment Sally. Sorry but your bedroom has to go.
Just going to engineer the environment Sally. Sorry but your bedroom has to go.
Environmental Engineering does not simply mean the knocking down of walls and widening of doorways to accommodate wheelchairs but rather a whole raft of wider techniques. More importantly than physical access (although physical access is undoubtedly important), the techniques are used to accommodate learning and understanding. Engineering the environment can be as simple as moving a desired object out of reach (or out of sight) such that a Learner has to communicate the need for it (other than by simply getting it him or herself or by pointing). It is not that pointing isn't a good communication technique but rather that, when pointing is well established, it is time to challenge the Learner a little more.
Thus, Environmental Engineering refers to range of techniques used by Significant Others to alter some part of the Learner's world (even in subtle or small ways) to motivate the learner to act in ways that s/he might not otherwise. For example:
In the video below, Mum is working with her daughter who is controlling the situation giving Mum commands by using a simple communication device. Mum deliberately messes up on one of her daughter's commands. The daughter then repeats the command proving that she simply isn't moving from one button to another blindly. Of course, this might have been just a chance happening; the one time Mum made a deliberate mistake, the daughter just happened to active the same button again except that, every time Mum made a 'mistake' on any task, her daughter 'corrected' her. Mum is 'engineering' the situation to promote learning and assess understanding.
Thus, Environmental Engineering refers to range of techniques used by Significant Others to alter some part of the Learner's world (even in subtle or small ways) to motivate the learner to act in ways that s/he might not otherwise. For example:
- Placing a small but desired piece of dark chocolate inside a plastic jar (no lid) to see if the Learner can obtain it without assistance. If that proves successful then doing it again with the lid in place. Each time there is success stepping it up just a little and making the task slightly more challenging.
- Wearing something very strange to see how the Learner reacts.
- Putting an object out of reach such that the Learner has to indicate his/her desire for it.
- Forgetting to put the straw in a drink such that a Learner (who needs a straw to drink) has to 'show' you the problem.
In the video below, Mum is working with her daughter who is controlling the situation giving Mum commands by using a simple communication device. Mum deliberately messes up on one of her daughter's commands. The daughter then repeats the command proving that she simply isn't moving from one button to another blindly. Of course, this might have been just a chance happening; the one time Mum made a deliberate mistake, the daughter just happened to active the same button again except that, every time Mum made a 'mistake' on any task, her daughter 'corrected' her. Mum is 'engineering' the situation to promote learning and assess understanding.
21. Sensory Stories
"A sensory Story is any set of experiences tailored to the specific needs of an individual (or individuals) that are N.I.C.E. and, when taken as a whole, relay some message, moral, myth, monologue, monograph, or matter." (Bullivant and Jones 2016)
In the quote above NICE stands for:
- Normal;
- Inclusive and Interactive;
- Comprehensible and Consistent;
- Enjoyable and Educational.
The design, Development and Delivery of Sensory Stories are covered in depth on another page of this website and therefore will not be detailed here. Please click on the image above left in order to open the Sensory Stories page in another window for further information on this area.
In the quote above NICE stands for:
- Normal;
- Inclusive and Interactive;
- Comprehensible and Consistent;
- Enjoyable and Educational.
The design, Development and Delivery of Sensory Stories are covered in depth on another page of this website and therefore will not be detailed here. Please click on the image above left in order to open the Sensory Stories page in another window for further information on this area.
22. Ten Second Rule

TalkSense cannot claim this idea as its own for it is based on an idea from Professor Caroline Musselwhite who often spoke about a thirty second rule in her lectures. The rule states that the extra things we ask staff to do to support the process of teaching and learning in the classroom should not take more than ten seconds (or in Prof. Musselwhite's case, thirty seconds). Why? The answer is simple; staff will already have their hands full and adding additional requirements will likely be too much. If we expect staff to drop everything and perform some additional task that takes minutes to do they will tend not to do it. However, if we make the additional requirement as simple and as easy to do they might just take it on board especially if it takes less than ten seconds.
How is this a meaningful activity for IEPMLD when it relates specifically to staff? Any practice that assists staff to carry out processes consistently assists in the classroom for IEPMLD because consistency is vitally important. This has long been recognised:
"Consistency and continuity both at home and school are important." (Clark 1991 page 14)
Staff are unlikely to perform new practices consistently if they are too demanding, too complex, too confusing, or take too much time. However, this only applies in the process of the teaching period and does not apply to prior preparation for sessions such as the preparation of support materials. Indeed, it might be the adequate preparation of supporting materials for the session over a couple of hours on the previous evening that permits the staff in the session to undertake a new practice within ten (or fewer seconds).
How is this a meaningful activity for IEPMLD when it relates specifically to staff? Any practice that assists staff to carry out processes consistently assists in the classroom for IEPMLD because consistency is vitally important. This has long been recognised:
"Consistency and continuity both at home and school are important." (Clark 1991 page 14)
Staff are unlikely to perform new practices consistently if they are too demanding, too complex, too confusing, or take too much time. However, this only applies in the process of the teaching period and does not apply to prior preparation for sessions such as the preparation of support materials. Indeed, it might be the adequate preparation of supporting materials for the session over a couple of hours on the previous evening that permits the staff in the session to undertake a new practice within ten (or fewer seconds).
23. TASCS: Talksense's Applied Sensory Control System

TASCS (pronounced 'tasks') is a Learner controlled sensory developmental program which has been designed to increase Learners' awareness of and active engagement with their environment through sensory stimulation. TASCS can be undertaken with a single student or with a group of students.
Requirements
Methodology
Assume a group of eight students supported by eight staff (That is a perfect scenario although we realise that life is rarely perfect and thus we will discuss a two student to one staff ratio later). During a TASC one hour session there will be (at least) eight tasks with each task's duration lasting approximately seven minutes.
Aims
Requirements
- choice of music in varying genres;
- means of student selection of music for task;
- area in which the lighting can be controlled via a switch or switches accessible to the students;
- range of sensory stimulation activities;
- equipment necessary to provide sensory stimulation activities;
- two BIGmacks (one red cap and one green cap) per student recorded with the words 'stop' and 'go';
Methodology
Assume a group of eight students supported by eight staff (That is a perfect scenario although we realise that life is rarely perfect and thus we will discuss a two student to one staff ratio later). During a TASC one hour session there will be (at least) eight tasks with each task's duration lasting approximately seven minutes.
Aims
24. Address a behaviour that society might find challenging

Challenging Behaviour has a social aspect; deping on the norms of the particular society, and a particular time and place, a behaviour can be seen either as acceptable or as 'challenging'. For example:
I was told recently of a situation in London in which an Individual Experiencing PMLD was asked to leave a performance at a theatre because her enjoyment manifested in a manner that was disruptive to others in the audience. Her support worker tried to explain her condition to the staff member concerned but to no avail, they were forced to leave the performance. However, had the performance been a matinee attended by boisterous youngsters, her cries of delight might have gone completely without comment. A young man of 19 became agitated while riding on public transport and started to rock and scream each time the bus came to a halt. This upset several of the pasengers and a child sat nearby started to cry frightened at the 'strange behaviour'. However, the very same behaviour when travelling to college on a college minibus caused no upset, rather resulted in 'calming' actions from supporting staff.
Behaviours that Staff may find Challenging (BSC) can take many forms. Included among these are:
Individuals Experiencing Profound and Multiple Learning Difficulties are more likely to exhibit behaviours that others might find challenging than other forms of learning disabilty (see for example: (Jacobson 1982; Oliver et al 1987; Johnson & Day 1992; Oliver 1993; Kiernan & Qureshi 1993; Borthwick-duffy, 1994; Kiernan & Kiernan 1994; Qureshi 1994; Rojahn 1994; Hillery & Mulcahy 1997; Bosch and Ringdahl 2001; McClintock et al., 2003; Lowe et al. 2007; Poppes et al. 2010; Emerson & Einfeld, 2011). Furthermore, the prevalence of challenging behaviour increases as people get older peaking between 15 - 25 years of age, only declining after the individual reaches mid-life (Oliver et al 1987; Kiernan & Qureshi 1993; Borthwick-Duffy 1994; Kiernan & Kiernan 1994; Rojahn 1994, Emerson et al 2001). In addition, IEPMLD are more likely to demonstrate such behaviours more frequently than other learners (Poppes et al. 2010). This may result, in part, because challenging behaviors are more likely to be seen in individuals who have:
"Indeed, since studies of deinstitutionalization have failed to identify any consistent effects on challenging behaviour reported by key informants, it would appear that such behaviours lead to institutionalization, and not that institutional environments lead to challenging behaviour." (Emerson, 2001, page 26)
Thus, it would appear that post-school educational provision for IEPMLD is likely to experience more behaviours that staff may find challenging, more frequently, than at other periods in a Learner's life time.
Addressing the BSC (Behaviours that Staff/Society may find Challenging) in IEPMLD is important because BSC are likely to:
"However, the consequences of challenging behaviour go far beyond their immediate physical impact. Indeed, the combined responses of the community, carers, care staff and service agencies to people who show challenging behaviours may prove significantly more detrimental to their quality of life than the immediate physical consequences of the challenging behaviours themseves. These social responses may include, inapproriate treatment, exclusion, deprivation, and systematic neglect." (Emerson, 2001)
Thus, addressing the behaviours that society may find challenging is an important area of concern for provision at post-school level. Indeed, as it has been recognised that such behaviours develop in childhood (from around five years of age)(see, for example: Emerson et al, 1988; Guess & Carr 1991; Murphy et al, 1993; Schneider et al, 1995; Murphy et al, 1999) and then increase with age (Jacobson 1982; Kiernan & Kiernan 1994; Hall et al., 2001). As such, challenging behaviours should be addressed at all stages of development. It has been known since the 1960s that addressing such behaviours can have positive outcomes (Lovaas et al, 1965; Ullman & Krasner, 1965; Tate & Baroff, 1966; Bailey & Meyersen, 1969; Azrin & Foxx, 1971).
One of the methodologies used to address these issues is 'behaviourist'. Under an operant behaviourist model (Skinner 1938), the factors that serve to increase behaviours are known as 'reinforcers' and those that serve to decrease behaviours as 'punishers' (reinforcement and punishment). There are two types of each (positive and negative):
- Self harm might not be seen as unacceptable by some if it was part of some religious ritual rite (people scourge themselves);
- Loud, offensive, and aggressive behaviour might be deemed more tolerable coming from a crowded football terrace in the UK than from a single individual wandering around a shopping mall;
- supporting a young adult to have a beer in a public house might be seen as acceptable by most but unacceptable by the young man's family if they happen to be muslim.
I was told recently of a situation in London in which an Individual Experiencing PMLD was asked to leave a performance at a theatre because her enjoyment manifested in a manner that was disruptive to others in the audience. Her support worker tried to explain her condition to the staff member concerned but to no avail, they were forced to leave the performance. However, had the performance been a matinee attended by boisterous youngsters, her cries of delight might have gone completely without comment. A young man of 19 became agitated while riding on public transport and started to rock and scream each time the bus came to a halt. This upset several of the pasengers and a child sat nearby started to cry frightened at the 'strange behaviour'. However, the very same behaviour when travelling to college on a college minibus caused no upset, rather resulted in 'calming' actions from supporting staff.
Behaviours that Staff may find Challenging (BSC) can take many forms. Included among these are:
- stimming (self stimulatory behaviour)(Included would be violent rocking enough to tip a chair);
- stibbing (self-injurous behaviour)(Included are such things as eye poking, face slapping, self punching, skin picking and scratching, biting/chewing own body parts, hair pulling, head bangiing, body banging, excessive teeth grinding, holding breath, burning, cutting with any object used as a tool, pulling out finger or toe nails, deliberate coughing to excess...);
- aggressive behaviour(s) towards others (hair pulling, kicking, punching, biting, choking, spittting ...);
- dopping (destruction of property [own and others]) Included here would also be furniture tipping);
- throwing or pulling (on any item given or in reach);
- screaming (especially continual screaming);
- pica (eating substances not generally consumed including own feaces [coprophagia], soil (geophagia), ... );
- refusal of food and or drink;
- inappropriate masturbation;
- inappropriate removal of clothing;
- temper tantrums;
- wandering / running off;
- ritual behaviour (Recently, I met a young man who would not go anywhere without holding an object (cushion, books, etc) in front of his face completely obscuring any view of his features);
- copropraxia: rectal digging, fecal smearing;
- regurgitation and emesis (Rogers et al 1992);
- rumination: repeated vomiting, chewing and re-ingesting;
- drinking to excess (any liquid);
- forcing / inserting (dangerous) objects (including own fingers/hands) into body orifices;
- fixation (generally on one object or person to the exclusion of all other stimuli);
- aerophagia (air swallowing);
- bruxism (excessive teeth grinding);
- persistent echolalia;
- inappropriate repetitive vocalisations (including vocabulary that others might find offensive);
- non-compliance (deliberate or otherwise).
Individuals Experiencing Profound and Multiple Learning Difficulties are more likely to exhibit behaviours that others might find challenging than other forms of learning disabilty (see for example: (Jacobson 1982; Oliver et al 1987; Johnson & Day 1992; Oliver 1993; Kiernan & Qureshi 1993; Borthwick-duffy, 1994; Kiernan & Kiernan 1994; Qureshi 1994; Rojahn 1994; Hillery & Mulcahy 1997; Bosch and Ringdahl 2001; McClintock et al., 2003; Lowe et al. 2007; Poppes et al. 2010; Emerson & Einfeld, 2011). Furthermore, the prevalence of challenging behaviour increases as people get older peaking between 15 - 25 years of age, only declining after the individual reaches mid-life (Oliver et al 1987; Kiernan & Qureshi 1993; Borthwick-Duffy 1994; Kiernan & Kiernan 1994; Rojahn 1994, Emerson et al 2001). In addition, IEPMLD are more likely to demonstrate such behaviours more frequently than other learners (Poppes et al. 2010). This may result, in part, because challenging behaviors are more likely to be seen in individuals who have:
- additional impairements of hearing or vision (Maisto, Baumeister, & Maisto, 1978; Schroeder et al, 1978; Kiernan & Kiernan 1994);
- great difficulty with receptive and expressive communication (Schroeder et al 1978; Borthwick-Duffy, 1994; Kiernan & Kiernan 1994; Bott, Farmer, & Rhode, 1997; Carr et al 1997; Emerson et al, 2001);
- poor social skills (Duncan et al, 1999);
- sleep deprivation (Kiernan & Kiernan, 1994);
- isues with mental health (Borthwick- Duffy, 1994);
- significant impairments of mobility (Kiernan & Qureshi, 1993; Kiernan & Kiernan, 1994);
- a more restrictive lifestyle (day placement, residential facility) (Emerson, 1992; Johnson & Day, 1992; Harris, 1993; Borthwick-Duffy, 1994; Bruininks et al, 1994). However, as there is a direct relationship between the level of challenging behaviour witnessed and the accompanying restrictiveness of the environment, it is likely that a restricted lifestyle is not a contributory cause of such behaviour but more likely its result:
"Indeed, since studies of deinstitutionalization have failed to identify any consistent effects on challenging behaviour reported by key informants, it would appear that such behaviours lead to institutionalization, and not that institutional environments lead to challenging behaviour." (Emerson, 2001, page 26)
Thus, it would appear that post-school educational provision for IEPMLD is likely to experience more behaviours that staff may find challenging, more frequently, than at other periods in a Learner's life time.
Addressing the BSC (Behaviours that Staff/Society may find Challenging) in IEPMLD is important because BSC are likely to:
- impact on an individual's future Quality of Life (QoL);
- impact on a student's learning (Carpenter et al., 2015);
- cause health and welfare issues for the Learner, as well as for those who provide care and support (Emerson 2001);
- result in serious and irreverseable harm to their body and even death (Borthwick-Duffy 1994; Nissen and Haveman 1997);
- cause injury to others (Spreat, Lipinski, Hill & Halpin, 1986; Konarski, Sutton, & Huffman, 1997);
- increase abuse from supporting staff (Maurice & Trudel 1982; Rusch, Hall & Griffin 1986);
- reduce the amount of time the Individual spends out in the community (Eyman & Call, 1977; Schalock, Harper, & Genung, 1981; Intagliata & Willer, 1982; Lakin et al, 1983; Hill & Bruininks, 1984; Borthwick-Duffy, Eyman & White, 1987; Jackson 2014);
- serve to remove the individual from family life;
- require an increased level of support from other individuals;
- increase stress levels of supporting carers and staff (Bersani & Heifetz, 1985; Quine & Pahl, 1985; Quine & Pahl 1991; Sloper et al, 1991; Qureshi, 1992; Saxby & Morgan, 1993; Hatton et al, 1995; Jenkins, Rose, & Lovell, 1997; Stores et al, 1998; Rojahn et al. 2011);
- result in the prescriptions of medication that have additional side-effects (such as drowsiness) (Oliver, Murphy , & Corbet, 1987; Meador & Osborn, 1992; Davidson et al, 1994, Kiernan, Reeves, & Alborz, 1995, Emerson et al, 2001, King 2007);
- result in inappropriate solutions by staff to 'remedy' the problem (for example, the use of splints to prevent self harm such as eye poking. (Griffin, Ricketts, & Williams 1986; Richmond,Schroder, & Bickel 1986; Spreat et al 1986; Luiselli 1992)
"However, the consequences of challenging behaviour go far beyond their immediate physical impact. Indeed, the combined responses of the community, carers, care staff and service agencies to people who show challenging behaviours may prove significantly more detrimental to their quality of life than the immediate physical consequences of the challenging behaviours themseves. These social responses may include, inapproriate treatment, exclusion, deprivation, and systematic neglect." (Emerson, 2001)
Thus, addressing the behaviours that society may find challenging is an important area of concern for provision at post-school level. Indeed, as it has been recognised that such behaviours develop in childhood (from around five years of age)(see, for example: Emerson et al, 1988; Guess & Carr 1991; Murphy et al, 1993; Schneider et al, 1995; Murphy et al, 1999) and then increase with age (Jacobson 1982; Kiernan & Kiernan 1994; Hall et al., 2001). As such, challenging behaviours should be addressed at all stages of development. It has been known since the 1960s that addressing such behaviours can have positive outcomes (Lovaas et al, 1965; Ullman & Krasner, 1965; Tate & Baroff, 1966; Bailey & Meyersen, 1969; Azrin & Foxx, 1971).
One of the methodologies used to address these issues is 'behaviourist'. Under an operant behaviourist model (Skinner 1938), the factors that serve to increase behaviours are known as 'reinforcers' and those that serve to decrease behaviours as 'punishers' (reinforcement and punishment). There are two types of each (positive and negative):
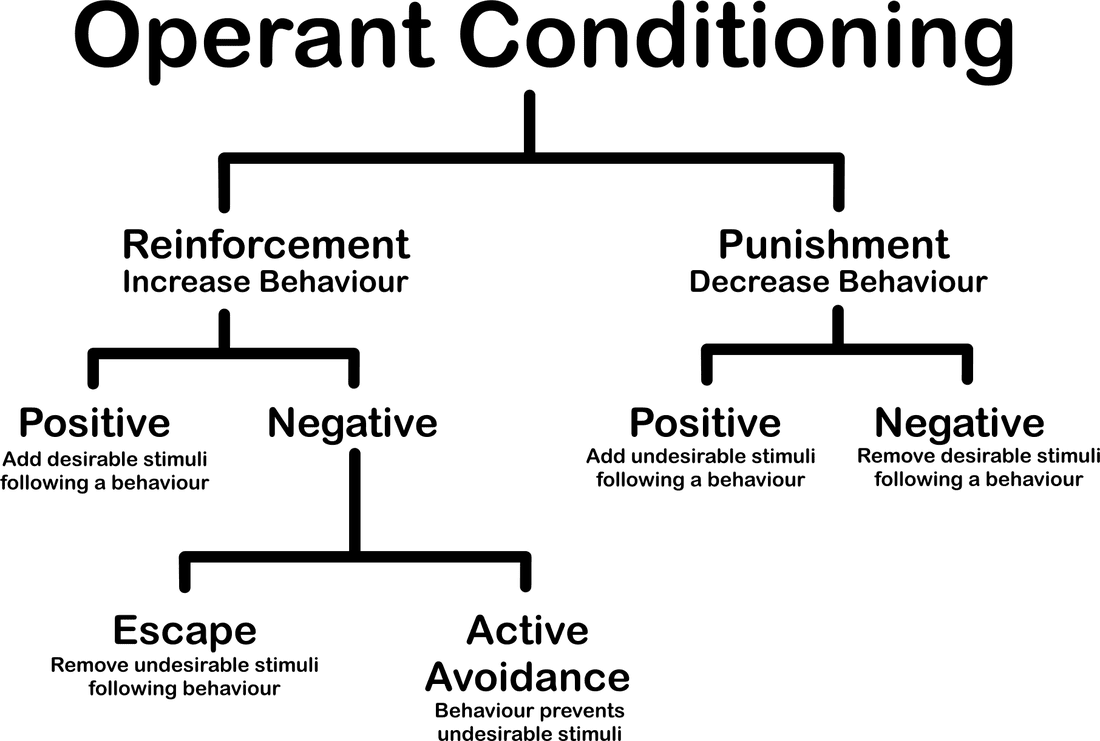
- Positive reinforcement: Positive reinforcement concerns adding a reinforcing action or event (stimulus) to a behaviour (good or bad behaviour) which makes the behaviour more likely to occur again. Thus, in practice, if a Learner receives a 'reward' (a BEST: Best Ever Stimulating Thing) after any behaviour, it is more likely that the behaviour will reoccur (the response is strengthened). For example, if you were to give your son a sum of money ($10 / £10) every time he put his dirty clothes in the laundry basket, he might begin doing it more often. If you were to reward a Learner after concentrating on a task for five minutes with praise and a walk in the sensory garden (a positive stimulus which she is known to love), it might result in the Learner concentrating (desired behaviour) more frequently. However, positive reinforcment does not always lead to a desired outcome: For example, if a Learner starts to scream every time you try to get him to go into a particular session of the curriculum and, as a result, he is taken to the multi-sensory room (which he is known to love) then this (going to the MSR) is positively reinforcing (increasing the future likelihood an undesirable behaviour (screaming). Thus, a positive reinforcer is any stimulus event for which a Learner might repeat a behaviour (either desirable or undesirable) in order to obtain it.

- Negative reinforcement: In negative reinforcement, something (not desired) is removed or avoided as a result of a particular behaviour. For example, if loud music was playing on a radio in your bedroom and you couldn't sleep, getting out of bed and turning the radio off (removing the undesirable event) allows you to go back to bed and get to sleep. Thus, turning off loud music before you get into bed is more likely to occur in the future. The noise that is preventing sleeping, is terminated following the behaviour of turning off the radio leading to negative reinforcement of the behaviour. Alternatively, it may be that you do something to avoid an undesirable outcome such as studying hard to avoid failing an exam. Negative Reinforcement can also lead to undesirable outcomes from the perspective of staff: For example, if a Learner starts to scream when staff attempt to put on his coat and, as a result staff don't put on his coat, the screaming might be more likely to occur the next time this action is attempted. Screaming takes away the staff putting on of coat leading to a reinforcement of the (in this case, from the staff's perspective, undesirable) behaviour (see, for example, Carr, Newsom & Binkoff,1980; Steege et al, 1990).
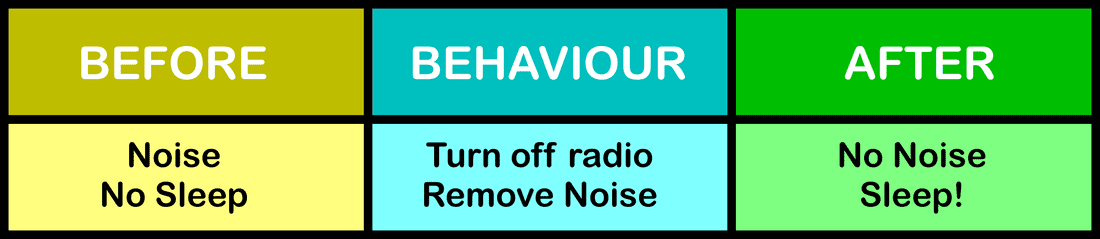
It can be seen that both Positive and Negative Reinforcement have reinforcing outcomes (both desirable and not so desirable depending on your perspective) and, as a result there is an increase in the behaviour. In Positive Reinforcement something is added while, in Negative Reinforcement, something is taken away. While both Positive and Negative Reinforcement provide a positive outcome for a Learner, the outcome (an increase in the behavior) may not always be positive for staff.
Positive Reinforcement - Add - Increase behaviour (Desirable or undesirable)
Negative Reinforcement - Subtract - Increase behaviour (Desirable or undesirable)
It should be seen that staff may, as a result of their actions following a particular behaviour, increase the likelihood of the behaviour's reoccurrence whether desirable or undesirable. It is therefore necessary for staff to consider their response to a particular behaviout they might find challenging so as not unwittingly to promote the likelihood of its future occurrence. It is also important to note that, simply because a staff member might consider a particular response on their part to be undesirable, it may however not be interpreted in that way by a Learner: A Learner might enjoy the attention received as result of a particular behaviour even though staff are shouting at him.
Similarly punishment has two operant conditioning forms; positive and negative: In the positive branch of punishment something (an undesirable stimulus) is added following a behaviour. The intention of the undesirable stimulus is to reduce the behaviour. For example, while a spanking would be considered to be a negative thing to do, it is, in fact, a positive punishment (in that it is added following the behaviour) if it serves to reduce the future likelihood of the behaviour occurring again. In the negative branch of punishment something (a desirable stimulus) is removed. For example; if a Learner repeatedly hits out at staff and each time s/he does so, the staff member moves away and leaves the Learner isolated (but not in any danger) for a short period of time then this action might result in the frequency of the undesirable behaviour (hitting) being reduced providing that the Learner perceives being isolated as undesirable. Thus removing the attention of staff might act as a negative punishment for a particular Learner. However, if the Learner likes (or does not care about) being left alone to his or her own devices, such a staff response might act as a positive reinforcer! What might be seen as a punishment for one individual may be a reward for another and, thus, consideration must be given to all staff responses on an individual Learner level and behaviour management plans developed accordingly.
Behaviour is an expression of a problem but it is not the problem: address the problem not the behaviour
*******INCOMPLETE***************************
What can be done to reduce BSC? An A - Z of options:
Actualise Acceptable Alternatives (Favell, McGimsey, & Schell, 1982; Durand & Crimmins,1991);
Banish Boredom; Build active sessions (Horner et al, 1980; Jackson 2014)
"self-engagement behaviours are due to a lack of stimulation. For people who have been under stimulated for many years these bahaviours may now have become part of their usual routine: however, if they are provided with object or activities that capture their attention they may still reduce their self-engagement bahaviours." (Fowler , page 18, 1997)
Champion Choice (Brown, Appel, Corsi, & Wenig, 1993)
"We strongly believe ‘voice’ does not simply mean ‘speaking’ (‘linguistic competence’). Instead, voice can mean children’s preferences, opinions, and agency expressed over time and across contexts." (Simmons & Watson, page 26, 2014)
"Through exploration and a variety of sensory experiences, people are able to debelop likes and dislikes. This development is a prerequisite to making informed choices. Offering people the opportunity to make choices enables them to move from having a passive role to taking active control over the things happening to them and their enviroment." (Fowler, page 35, 1997)
Don't Deliver a school-based approach ...
Enable Expressive communication (Carr & Durand, 1985a; Carr, Levin, McConnachie, Carlson, Kemp, & Smith,1997);
Find the Fun
"Although such activities are structured, they are still set upin a way that allows people to have fun and enjoy the sessions.They are more likely to participate and learn if they are having fun." Fowler, page 38, 1997)
G
Healthy Habits - Eating & Drinking (Podboy & Mallory, 1977; Hughes,1996)
Additives and ingredients of specific foods and drinks (For example: caffeine, sugar, E numbers) that are known to cause anxiety, constipation, painful reactions, sleepless nights may have a direct or indirect impact on the strength and frequency of BSC.
Caffeine - Podboy and Mallory 1977; Hughes,1996
Increase purposeful activity (Mansell, Felce, de Kock, & Jenkins,1982; Mansell, Jenkins, Felce, & de Kock,1984).
Jean Ayres: Sensory Integration (Ayres, 1970; Trott, 1993; Kranowitz, 1998; Aquilla, Sutton, & Yack, 2003; Smith & Gouze, 2004)
Sensory Integration is a theory developed by Jean Ayres detailing the neurological mechanism involved in processing and integrating sensory information from the body and the environment and how this contributes to learning, behavior and emotion. Individuals Experiencing PMLD are not only likely to have additional sensory impairments but also considerable issues with the integration of remaining sensory input into meaninful and useful information resulting in confusion about the nature of their world. Such confusion may lead them to behave in ways with which others find difficult to cope and to undertsand. Thus, for the individual who is experiencing dysfunctional sensory processing, traditional behavioural therapy approaches involving reinforcements and punishments may prove to be ineffective as they are not addressing the underlying cause. Sensory Integration will therefore be addressed in a separate section of this web page.
Knowing me, Knowing you (Halle & Spradlin, 1993; Touchette, MacDonald, & Langer, 1985)
The presence and or absence of specific staff members can have a direct impact on the behaviour of specific students. While it may not be possible to prevent the absence of speciifc members of staff from time to time, it is not good practice to position staff apart from students who are agitated by their non-presence. That is not to say such staff have to work one-on-one with a specific Learner each and every day, all day, rather to acknowledge the present need for a student to be weaned off this reliance over time. This may be addressed by ensuring that the staff member is a part of the group that works with the student (in the same room though not always providing direct support) and gradually increasing periods when the staff member is 'absent' whilst engaging the student in meaningful activity. It becomes more difficult if the staff member in question is a teacher and cannot be in the same room as the Learner except for allocated times on the curriculum.
Listen to challenging behaviour (Lacey, 2011; Gardner & Rikberg Smyly,1997; Bullivant, 2015);
Make use of technology (Gardner, 1985; Jones, 2016);
N
Overcrowding and BSC (Boe, 1977; McAfee 1987)
Classroom density may have a significant effect on the frequncy of BSC in IEPMLD. Studies (op.cit.) demonstrate that individuals experiencing learning difficulties exhibit challenging behaviour more frequently under crowded conditions. While other factors (such as classroom management, location of staff, etc.) may play a role, there appears to be evidence for a direct relationship between overcrowding in a learning environment and a higher rate of aggressive behaviour in Learners who are severely cognitively impaired. As such, overcrowding is to be avoided.
Promote reinforcement that serves to reduce challenging behaviour;
Q
Reduce/Remove Reinforcement that serves to increase challenging behaviour:
Slash Staff Stress levels (Emerson 2001)
"Similarly, fluctuations in the levels of experience, competence, stress, stability, and fatigue among members of a staff team are likely to determine their capacity to cope with the disruption caused by some who shows severe self -injury." (Emerson, 2001, page 8)
It can be seen that high levels of staff stress reduces their ability to cope with the inevitable disruptions in a post-sixteen special education environment. Thus, anything that managment can do to increase competence, decrease fatigue, and reduce stress is likely to result in a more positive educational experience for all.
Task length and BSC
Use sensory extinction (Rincover 1978; Aiken & Salzberg, 1984; Maag et al.,1986; Dalrymple,1989);
In this approach, stereotypy is regarded as operant behaviour that is maintained by its consequences. For example, the individual that continually waves his hand in front of his face might be maintained by the proprioceptive feedback it generates. Sensory Extinction involves changing, masking, or removing specific sensory consequences of any behaviour; the theory being, if the consequences are removed, the behaviour will stop. For example, if a Learner continually taps at a switch (instead of just a single activation) removing the sensory consequences (the sound of the switch clicking perhaps) might terminate the behaviour as the Learner is no longer receiving sensory feedback/reward. For a further example, see the section entitled 'String Switch Sessions' (below on this webpage) which covers accidental and purposeful triggering of sensory extinction.
Videotape analysis (Carr, Yarbrough, & Langdon, 1997; Caldwell, 2006; Kennedy, 2011; Rees, 2014)
"Given the large number of specific antecedents that have been demonstrated to influence problem behavior, it is plausible that one might occasionally overlook relevant antecedent stimuli during the course of conducting a functional analysis, with the result that the analysis produces misleading results." (Carr, Yarbrough, & Langdon 1997)
Walk, run, dance, exercise! (Kern, Koegel, Dyer, Blew, & Fenton 1982; Baumeister & MacLean, 1984; McGimsey & Favell, 1988)
X
Y
Zzzzz! The importance of a good night's sleep (Kennedy & Meyer, 1996; Piazza, Fisher & Kahng, 1996; Wiggs & Stores, 1996; Brylewski & Wiggs, 1999; Symons et al., 2000; Didden et al, 2002)
Healthy uninterrupted sleep is an important factor. .
25. Develop Shared Attention through Interactive 'Games'
When working with IEMPLD we must consider varying supporting strategies that will work to meet individual needs.One such strategy is the use of interactive games. Such an approach may provide a motivating opportunity for young adults to begin to enjoy working, interacting, and cooperating with others (see, for example, Kingsley 2009). Individuals Experiencing PMLD (IEPMLD) are likely to have problems in attending to a specific POLE (Person Object Location or Event) introduced by any staff member for more than a few seconds of novel interest. Even more problematic is an expectation of joint focus (The IEPMLD and a Significant Other (in this example, a staff member)) on any specific POLE for any length of time. Shared attention ( "a process in which a child and another person both attend to the same object or event" (Kuder, 2003, page 146)) is not only vital for better outcomes for teaching but also is a vital component of the development of communication skills.
An IEPMLD may have significant difficulty in working with others in sharing focus on a specific task. S/he may:
Working towards increasing periods of shared attention is vital in the development of collaboration between student and staff and a platform on which future learning may take place. Early learning about social interactions often takes place through imitation (deliberately copying another's movement and or sounds). Imitation can be a productive and interactive way of developing shared attention because it can get the attention of the individual (Hewett & Nind, 1993) and, occasionally, begin a communication interchange of random vocalizations. The introduction of interactive games, in which imitation is utilised, is a relatively easy method to introduce a framework for the establishment of a shared focus. The notion of a 'game' here is, of course, much wider than playing 'snakes and ladders' as the image above left might suggest. Indeed, the introduction of such a game is likely to lead to one of the 'problematic' outcomes mentioned earlier! Thus, the term 'game' here refers to any form of reciprocal interplay between student and staff with or without the use of an object (such as ball). This might involve the use of 'co-active interaction' as outlined earlier on this page.
An IEPMLD may have significant difficulty in working with others in sharing focus on a specific task. S/he may:
- show no interest at all;
- lose interest almost immediately;
- interact with the newly introduced POLE in a manner that staff find problematic;
- show no interest in cooperating with the significant other in interactions with the POLE;
- reject the POLE altogether.
Working towards increasing periods of shared attention is vital in the development of collaboration between student and staff and a platform on which future learning may take place. Early learning about social interactions often takes place through imitation (deliberately copying another's movement and or sounds). Imitation can be a productive and interactive way of developing shared attention because it can get the attention of the individual (Hewett & Nind, 1993) and, occasionally, begin a communication interchange of random vocalizations. The introduction of interactive games, in which imitation is utilised, is a relatively easy method to introduce a framework for the establishment of a shared focus. The notion of a 'game' here is, of course, much wider than playing 'snakes and ladders' as the image above left might suggest. Indeed, the introduction of such a game is likely to lead to one of the 'problematic' outcomes mentioned earlier! Thus, the term 'game' here refers to any form of reciprocal interplay between student and staff with or without the use of an object (such as ball). This might involve the use of 'co-active interaction' as outlined earlier on this page.
26. Difference Awareness Development (DAD)
DAD stands for Difference Awareness Development ... Anat Baniel ...
27. Create A Responsive Environment

"The transition to intentional communication may be supported by consistently over-interpreting the client’s behaviour as if it were intentional." (Petry & Maes, 2006)
28. Control The Environment

One thing that an IEPMLD can easily do is to control her/his environment via one or more switches through an interface. There are at least three possibilities here:
Adapting battery powered and mains powered items for switch use are covered in separate sections on this page (please see below). This section will focus on infra-red controlled systems such as TVs, CD players, etc. These days there are so many commercial items that can be operated easily via an infrared control device that it a relatively simple and cost effective matter to equip at least one session area for this purpose. While searching for such items ensure that they come with their own infra-red remote control (most living rooms these days have at least one infra red remote control device laying around): For example, it is possible to purchase electronically operated curtains with their own armchair controller. It is this control box that can be emulated to provide switch access to the same functions. Thus, in this example, a Learner would be able to open and close the curtains via a switch.
What sorts of everyday electronically operated things can come with an infra red remote control? Here are just a few items that are readily available from the high street or on line:
Yes, there are companies that will provide a customised environmental control space but this tends to come with a hefty price tag. DIY solutions are not that difficult, really cost effective and, if you do-it-yourself, you tend to have a better idea how to fix it if there is a problem.
- mains powered electrical items switch controlled through a PowerLink or Equivalent
- Battery Powered Items adapted and switch controlled through a Battery Device Adapter;
- Infra-red controlled items switch controlled through an infra-red emulator.
Adapting battery powered and mains powered items for switch use are covered in separate sections on this page (please see below). This section will focus on infra-red controlled systems such as TVs, CD players, etc. These days there are so many commercial items that can be operated easily via an infrared control device that it a relatively simple and cost effective matter to equip at least one session area for this purpose. While searching for such items ensure that they come with their own infra-red remote control (most living rooms these days have at least one infra red remote control device laying around): For example, it is possible to purchase electronically operated curtains with their own armchair controller. It is this control box that can be emulated to provide switch access to the same functions. Thus, in this example, a Learner would be able to open and close the curtains via a switch.
What sorts of everyday electronically operated things can come with an infra red remote control? Here are just a few items that are readily available from the high street or on line:
- Boombox (CD, radio, etc all in one);
- Cameras and camcorders;
- Curtains;
- DVD players;
- Lamps, Lights, torches;
- Plug sockets (these simply plug into standard mains wall outlets and then can turn on the power to any device that is plug into them.);
- Television;
- Toys (for example, helicopters).
Yes, there are companies that will provide a customised environmental control space but this tends to come with a hefty price tag. DIY solutions are not that difficult, really cost effective and, if you do-it-yourself, you tend to have a better idea how to fix it if there is a problem.
In order to emulate infra-red remote control devices and make them switch accessible you will need an interface that permits control directly via a switch. While there are environmental control systems on the market that can offer such control it may not be in a one-to-one correspondence between switch action and device function but rather through a scanning option in which the Learner has to activate the switch when the scanning device reaches a specific option. Although such systems are wonderfully empowering, almost by definition, the ability to use them is beyond the cognition of the vast majority of IEPMLD (although, it is by no means impossible that, an individual could be taught to use such a system). Therefore, it is better to acquire a system that does not simply rely on an understanding of scanning technology but offers a direct link from switch activation to device action; in other words, the Learner presses a switch and the CD begins to play (for example). There are several such devices on the market but they tend to come and go (thus, the following links may or may not work depending on when you are reading this page).

This section will recommend two such systems (currently available at the time of development of this section.)
Note: These systems may be available though other suppliers in different countries. Search the net to locate your nearest source.
While the Big Jack is the simpler of the two with which to work, the Advocate is currently on offer and represents remarkable value for money especially as it may be necessary (depending on how many devices are being controlled) to purchase several. Each device can 'learn' the remote infra-red signals from any system's existing infra-red controller and then emulate them via a single switch activation. In so doing, an entire area in a College or Day Centre (or other establishment) could be set up to provide control experiences for an Individual Experiencing PMLD who is able to operate a switch by any means.
The provision of control experiences for an IEPMLD may assist in:
- The 'Advocate' (image above left) available from Inclusive Technology;
- The Gewa Big Jack (image left) available (in UK) from Possum.
Note: These systems may be available though other suppliers in different countries. Search the net to locate your nearest source.
While the Big Jack is the simpler of the two with which to work, the Advocate is currently on offer and represents remarkable value for money especially as it may be necessary (depending on how many devices are being controlled) to purchase several. Each device can 'learn' the remote infra-red signals from any system's existing infra-red controller and then emulate them via a single switch activation. In so doing, an entire area in a College or Day Centre (or other establishment) could be set up to provide control experiences for an Individual Experiencing PMLD who is able to operate a switch by any means.
The provision of control experiences for an IEPMLD may assist in:
- improving future Quality of Life (QoL);
- developing contingency awareness (Cause and effect recognition);
- a reduction in behaviours that staff may find challenging.
29. Modify Battery Powered Technology

As modern technology is typically powered by electricity, and there are three forms of supply (mains, battery and USB), there are at least three forms of equipment 'modification' (Don't panic the modification is simple!) for everyday items. While ready switch-adapted technology is available it can be more expensive and hard to locate just what is needed. If you switch adapt the technology yourself, you can not only save a lot of money but also enlarge the range of everyday sensory items available for use in any session.
In the image (left) the young man is enjoying experiencing a vibrating pillow. However, had he been able to control the pillow through a single switch activation consider the educational possibilities! Modifying most devices powered by batteries is relatively simple and takes only minutes to do. Only the following equipment is required:
In the image (left) the young man is enjoying experiencing a vibrating pillow. However, had he been able to control the pillow through a single switch activation consider the educational possibilities! Modifying most devices powered by batteries is relatively simple and takes only minutes to do. Only the following equipment is required:
- the item to be modified;
- a Battery Device Adapter (BDA) suited to the size of the batteries used by the device being modified;
- a small triangular file;
- a switch (preferably one that the Learner knows).
- have a simple on-off switch only (not an on/off switch together with a further a press button to start the action);
- work from either AA, AAA, C, or D batteries. Do not select devices that run from watch batteries or other alternative battery forms
A Battery Device Adapter looks like a small circle of copper with a trailing wire that ends in a socket into which any standard 3.5 mm switch may be plugged. In actuality it is not one circle of copper but two identical circles sandwiching an insulating layer of plastic through which electricity cannot pass (see image left). Typically there are two sizes of BDA available; one for small batteries such as AA and AAA and a larger one for C and D size battery powered systems. If you are unsure purchase the smaller one because the smaller one will work for the bigger batteries but the larger one may not fit into the compartment housing the smaller batteries. Most special needs suppliers will stock Battery Device Adapters for example go to the Ability-World Website and search for them by name.
In order to adapt your device:
In order to adapt your device:
- remove the battery compartment cover;
- remove one of the batteries;
- place the copper disc next to the exposed positive terminal inside the battery compartment;
- replace the battery such that the copper disc is now trapped between the positive terminal of the battery and the positive terminal in the battery compartment;
- file a small notch in the battery compartment cover to allow the lead safe exit. Typically covers are made of plastic and can be 'notched' easily using a small triangular file;
- replace the battery cover ensuring the lead passes through via the notch.
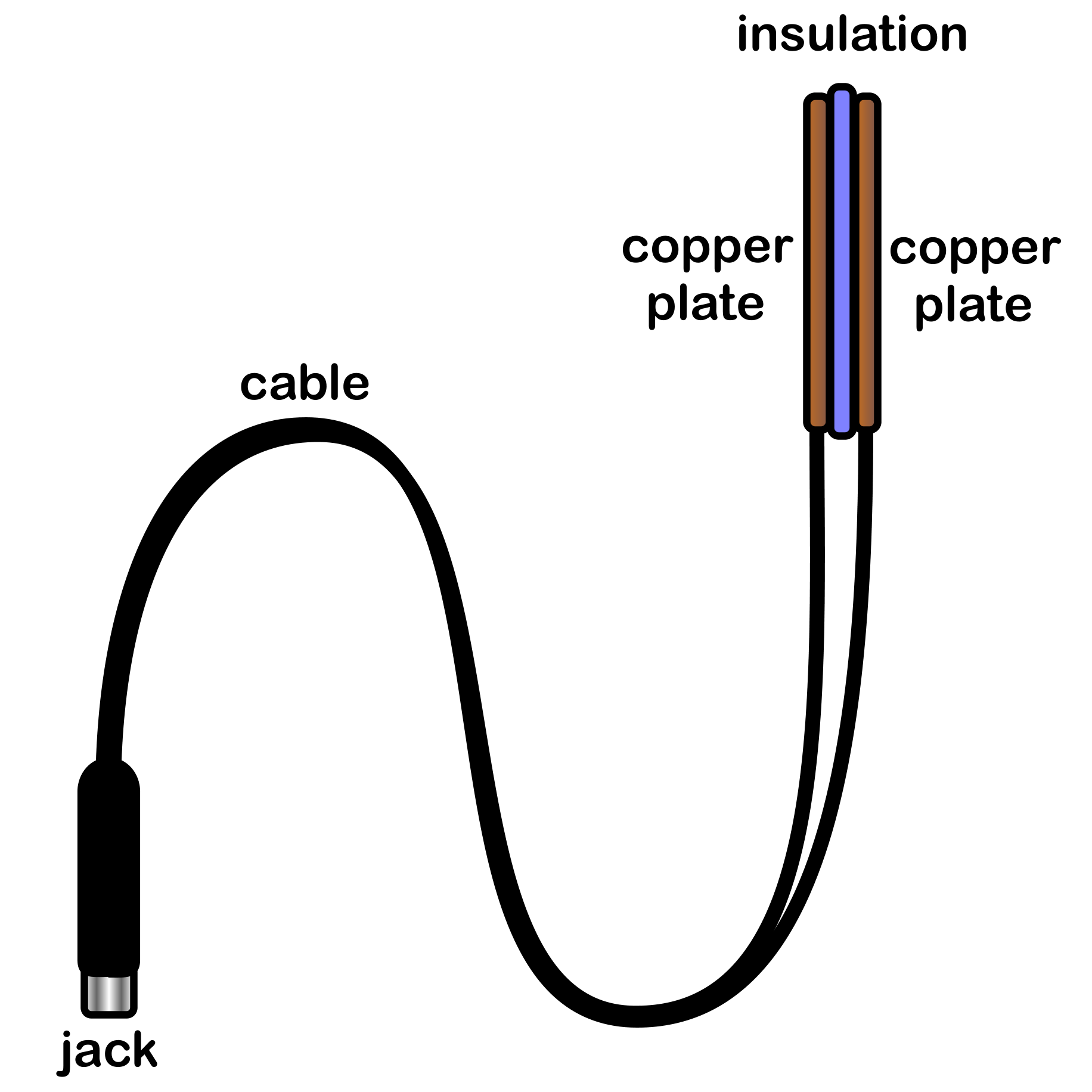
|
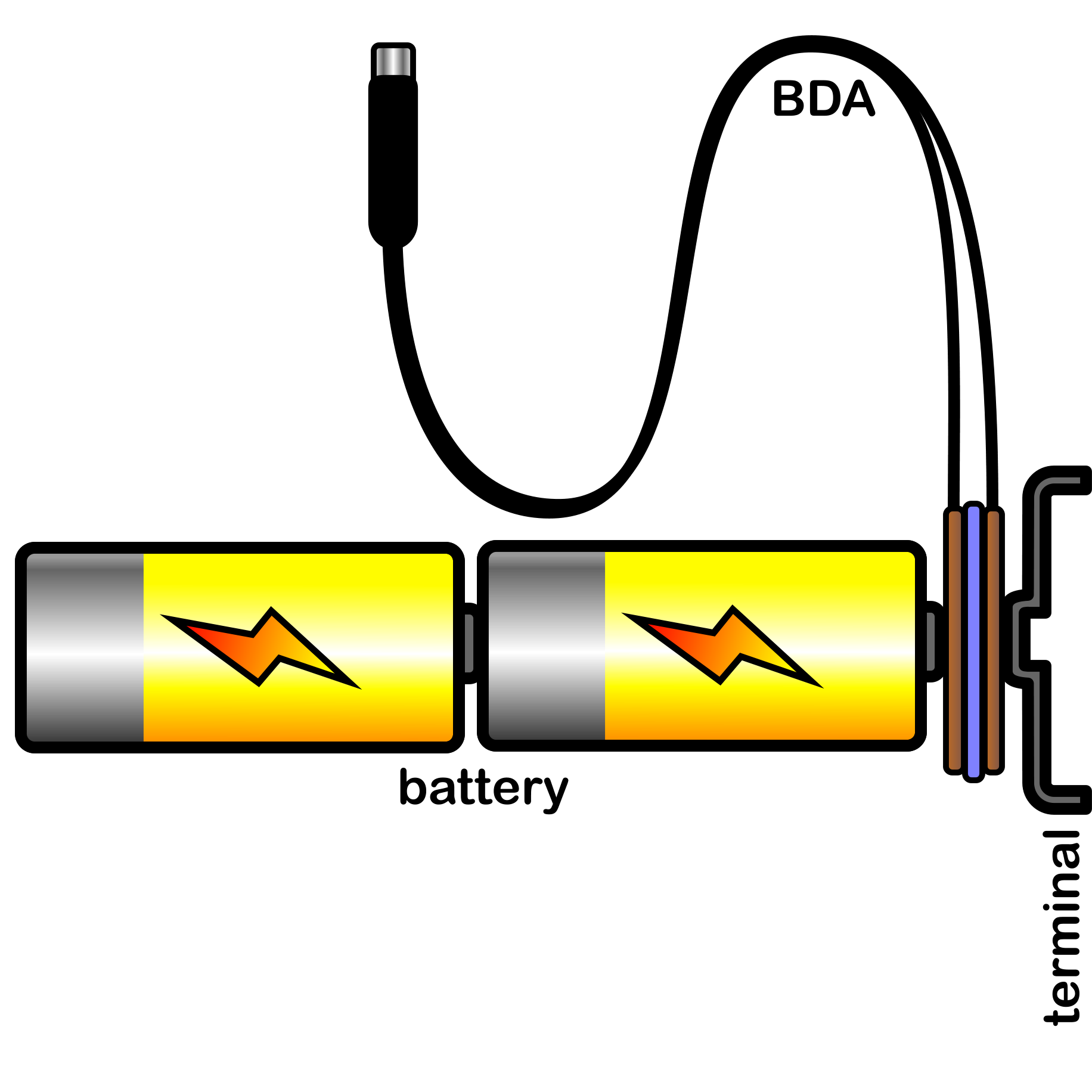
|
If You are still unsure what to do, watch the following easy-to-understand YouTube video (https://www.youtube.com/watch?v=DaivAvvvKy0)
Plug your switch into the cable and turn on the device. If you have followed the instructions correctly the device will only work while the switch is activated. Once the switch is released the device will stop.
Some Learners may find it difficult at first to activate a switch for long enough to get sufficient feedback from the device (radio, cassette, vibration device, etc.). It s possible for the learner to activate the switch briefly and yet for the device to continue running for a set period of time. The easy way to do this is via a BIGmack. A BIGmack is a simple-technology, single-message, communication device available from your AbleNet dealer. By plugging the BIGmack into the adapted appliance (The BIGmack comes ready supplied with a lead to do this. The lead has a 3.5 mm jack plug at each end) and plugging your switch into the BIGmack (The sockets are clearly labelled on the BIGmack), the BIGmack can then act as a timer for a period of up to two minutes! To do this, record either a sound effect, or a message, or 'silence' on to the BIGmack (he system comes with simple instructions on how to do this). the recording should be the exact length of time that you want your adapted device to remain on after the Learner's switch is activated. TalkSense would recommend this should be around 8 seconds (Eight is Great). If you make it too long, the Learner does not have to work to get a reward and not come to understand the cause and effect relationship between the switch and the device. If you make it too short, the Learner may not have time to comprehend what is happening.
Some Learners may find it difficult at first to activate a switch for long enough to get sufficient feedback from the device (radio, cassette, vibration device, etc.). It s possible for the learner to activate the switch briefly and yet for the device to continue running for a set period of time. The easy way to do this is via a BIGmack. A BIGmack is a simple-technology, single-message, communication device available from your AbleNet dealer. By plugging the BIGmack into the adapted appliance (The BIGmack comes ready supplied with a lead to do this. The lead has a 3.5 mm jack plug at each end) and plugging your switch into the BIGmack (The sockets are clearly labelled on the BIGmack), the BIGmack can then act as a timer for a period of up to two minutes! To do this, record either a sound effect, or a message, or 'silence' on to the BIGmack (he system comes with simple instructions on how to do this). the recording should be the exact length of time that you want your adapted device to remain on after the Learner's switch is activated. TalkSense would recommend this should be around 8 seconds (Eight is Great). If you make it too long, the Learner does not have to work to get a reward and not come to understand the cause and effect relationship between the switch and the device. If you make it too short, the Learner may not have time to comprehend what is happening.
30. Modify mains powered items for use via a switch
It is possible to adapt virtually any simple, standard mains powered device for use with a switch. However, some devices (such as modern TV sets), even when powered up, will not automatically operate without an additional remote control. Such items are not suitable for the adaption methodology detailed here. If the device has an off/on button and, when activated, starts to operate immediately, the following method of adaptation is likely to be suitable.
You will need:
The PowerLink4 from AbleNet (available in most countries from your local AbleNet supplier) is a device that permits a single switch (or two switches) to operate a mains powered device safely. The PowerLink comes with two plug sockets such that two devices can be controlled by two Learners independently if required. The device can be easily configured to operate in varying 'modes' (such as timed in seconds or timed in minutes). By plugging a switch into one of the switch ports and connecting your mains device, it becomes possible to turn the power to the device on or off via the switch. Thus, if the device is on and the switch is activated, the device will immediately begin to operate.
It is also possible to configure a Jelly Beamer to operate the PowerLink remotely such that there are no wires connecting the Learner to the PowerLink and to the device which the learner can pull. TalkSense recommends such an approach.
Note: There alternatives to the PowerLink available, from different companies, in most countries, with different variations in control methodologies. However, all will operate mains powered items via a switch.
You will need:
- the device to be switch adapted (for example, a hairdryer);
- A PowerLink4 or some alternative system;
- A switch.
The PowerLink4 from AbleNet (available in most countries from your local AbleNet supplier) is a device that permits a single switch (or two switches) to operate a mains powered device safely. The PowerLink comes with two plug sockets such that two devices can be controlled by two Learners independently if required. The device can be easily configured to operate in varying 'modes' (such as timed in seconds or timed in minutes). By plugging a switch into one of the switch ports and connecting your mains device, it becomes possible to turn the power to the device on or off via the switch. Thus, if the device is on and the switch is activated, the device will immediately begin to operate.
It is also possible to configure a Jelly Beamer to operate the PowerLink remotely such that there are no wires connecting the Learner to the PowerLink and to the device which the learner can pull. TalkSense recommends such an approach.
Note: There alternatives to the PowerLink available, from different companies, in most countries, with different variations in control methodologies. However, all will operate mains powered items via a switch.
31. Modify USB powered items for use via a switch

There are an increasing number of USB powered items available. These tend to be things that draw their power via computer USB sockets. However, it is possible to operate them via a single switch by using a USB plug as illustrated in the image (left). A USB plug looks like the standard plug (for your country) but it has no wires rather a USB socket to which your USB powered device can be attached. Such plug adapters are now commonplace in most countries: Indeed, you probably already have one in you own an iPad. They can be purchased for little outlay in many stores.
To convert a USB powered device to switch control you will need:
NOTE: some USB powered devices will not work directly when plugged into a computer's USB socket. For example, there is a hamster that runs around a wheel available as a USB desk top executive toy. However, when this is plugged into the computer's USB socket, the hamster does not move! This is because the device was designed to operate in response to keystrokes from the keyboard: The faster you type, the faster the hamster will run. Such systems will not work directly from a single switch. Thus, when purchasing USB powered devices, ensure that, when they are plugged into a power source such as a computer, they operate immediately (there may be an on/off switch which should remain at the ON position).
To convert a USB powered device to switch control you will need:
- A USB powered device (for example, fairy lights);
- A USB plug (illustrated);
- A PowerLink (or alternative)(See previous section);
- A switch.
NOTE: some USB powered devices will not work directly when plugged into a computer's USB socket. For example, there is a hamster that runs around a wheel available as a USB desk top executive toy. However, when this is plugged into the computer's USB socket, the hamster does not move! This is because the device was designed to operate in response to keystrokes from the keyboard: The faster you type, the faster the hamster will run. Such systems will not work directly from a single switch. Thus, when purchasing USB powered devices, ensure that, when they are plugged into a power source such as a computer, they operate immediately (there may be an on/off switch which should remain at the ON position).
32. Sensory Self Stimulation Sessions
What is a Sensory Self Stimulation Session (SSSS)? An SSSS is a period of time provided for a young person to experience sensory stimulation of different types and on different areas of the body via switch technology under the individual's control. If the Learner does not like the sensation, because it is under the learner's control, s/he can stop it easily. Switches can control powered items directly (when the switch is activated the device operates, when the switch is released the device stops), latched (like a light switch; with one activation it is on and with a second activation it is off); or in timed mode (one activation of the switch will operate for a preset amount of time usually measured in seconds)
How do we adapt differently electrically powered items for control by an individual? See the previous three sections above.
The idea is to have a range of powered items (that can supply sensory feedback to a Learner) available for exploration by a Learner such that we might observe the Learner's:
Which everyday items provide sensory feedback and can be adapted to work through a switch? Below is a list of ideas. However, please note, this list is not intended to be comprehensive; there will be other things that may also be useful in such a session. As you walk around stores while out shopping keep your eyes open for any item that might be utilised in this way.
Safety is an important factor:
If the item is:
the Learner can be shown how to access the switch and permitted to explore the sensation caused. The switch may be mounted to a tray or to a wheelchair arm or to any handy surface easily accessed by the Learner.
If the device is small enough such that it can be handled with ease, the Learner can be given the device and, again, shown how to access the switch to explore the sensations.
Over time the Learner may come to have particular preferences. The Learner can now be given a choice. If two or three devices are arranged in clear view of the Learner, which does s/he reach for, or look at, or otherwise indicate? This should be taken to be a choice even if you believe it to be otherwise. The Learner should be given the 'chosen' item for a set period of time, typically this will be for as long as the Learner is actively engaged with it and controlling it via the switch. This time may be short as the Learner may have a short attention span. In which case try presenting more items and see if there is a further reaction and another choice made.
How do we adapt differently electrically powered items for control by an individual? See the previous three sections above.
The idea is to have a range of powered items (that can supply sensory feedback to a Learner) available for exploration by a Learner such that we might observe the Learner's:
- reaction to each item as it is presented;
- preference for one form of sensory stimulation over another;
- attention span with different stimuli;
- ability to control the item via a switch;
- ability to manipulate the item (if appropriate);
- coordination of varying parts of the body;
- comprehension of cause and effect (contingency awareness).
Which everyday items provide sensory feedback and can be adapted to work through a switch? Below is a list of ideas. However, please note, this list is not intended to be comprehensive; there will be other things that may also be useful in such a session. As you walk around stores while out shopping keep your eyes open for any item that might be utilised in this way.
- fans (small fans and big powerful fans);
- vibrators (there are many that are commercially available)(vibrating cushions, mats, massagers, even sex toys!);
- back massagers (I was bought one as a present for use in the car - it's very good);
- lights (Disco lighting, fairy lighting, torches (but NOT laser pens), led lights, desk lamps, etc.);
- battery powered electrical toothbrush (ensure it is one with removal standard batteries);
- old electric razors (ensure it is safe for use);
- hair dryers (not on a high heat setting);
- vacuum cleaners (especially ones that can be set to blow as well as suck);
- radios (battery operated preferably);
Safety is an important factor:
- Do not select items with moving parts that could cut or trap body parts.
- Battery powered devices are going to be generally safer than mains items but ensure that the battery compartment is fixed firmly as batteries themselves can be hazardous if swallowed.
- Switches imply switch wires. While such wires can be chewed safely, they still present a strangulation hazard. Therefore no Learner should be left unsupervised at any time.
- If you are using mains powered items always take extra care over safety. Such items should be firmly mounted such that the Learner cannot pull the item on top of them but in a position to provide the maximum sensory stimulation.
- Of all the switch modes, direct is the safest. In direct mode; the device will only operate while the switch is activated. if the switch is released the device will stop. However, some Learners may have difficulty in maintaining the switch activation. If this is the case, use a timed mode with a setting of around eight seconds (eight is great so wait for eight).
If the item is:
- mounted (a hair dryer can be mounted on a stand);
- free-standing (such as an electric fan);
- positional (like a back massager that sits between seat back and the Learner, or a vibrating cushion),
the Learner can be shown how to access the switch and permitted to explore the sensation caused. The switch may be mounted to a tray or to a wheelchair arm or to any handy surface easily accessed by the Learner.
If the device is small enough such that it can be handled with ease, the Learner can be given the device and, again, shown how to access the switch to explore the sensations.
Over time the Learner may come to have particular preferences. The Learner can now be given a choice. If two or three devices are arranged in clear view of the Learner, which does s/he reach for, or look at, or otherwise indicate? This should be taken to be a choice even if you believe it to be otherwise. The Learner should be given the 'chosen' item for a set period of time, typically this will be for as long as the Learner is actively engaged with it and controlling it via the switch. This time may be short as the Learner may have a short attention span. In which case try presenting more items and see if there is a further reaction and another choice made.
33. String Switch Sessions

What is a string switch? Its a switch that is activated by pulling on a string that comes out of the side of the box housing the technology. It is small and easily mounted to a wheelchair or a chair/table leg (I use just an elastic band!). It is an AbleNet product and thus will be available from you local AbleNet dealer.
There are many Learners who don't really comprehend switches, simply ignore them, or push them away. the string switch may be ideal for such a Learner.
Using a string switch is a means to effect sensory extinction through accidental or purposeful triggering of alternate sensory input. The string switch is activated by less than one ounce of force pulling on the string. The Learner is not going to pull on the string? Yes s/he is! Here is how you set it up. You will need a couple of strong elastic bands, a wrist band (a really cool one) or a head band and a deice for the switch to operate: I typically start with a good floor mounted fan. The elastic bands are looped through the string of the switch and attached to the sweat band (loop them through no need for knots!) the switch is attached to the fan (in this example) via a PowerLink (see earlier section on Powerlinks). The string switch box may be attached to the wheelchair or a table or chair leg (just use an elastic band). The wrist band is placed either on the Learner's wrist or on the Learner's ankle (head band goes on the head obviously).
There are many Learners who don't really comprehend switches, simply ignore them, or push them away. the string switch may be ideal for such a Learner.
Using a string switch is a means to effect sensory extinction through accidental or purposeful triggering of alternate sensory input. The string switch is activated by less than one ounce of force pulling on the string. The Learner is not going to pull on the string? Yes s/he is! Here is how you set it up. You will need a couple of strong elastic bands, a wrist band (a really cool one) or a head band and a deice for the switch to operate: I typically start with a good floor mounted fan. The elastic bands are looped through the string of the switch and attached to the sweat band (loop them through no need for knots!) the switch is attached to the fan (in this example) via a PowerLink (see earlier section on Powerlinks). The string switch box may be attached to the wheelchair or a table or chair leg (just use an elastic band). The wrist band is placed either on the Learner's wrist or on the Learner's ankle (head band goes on the head obviously).
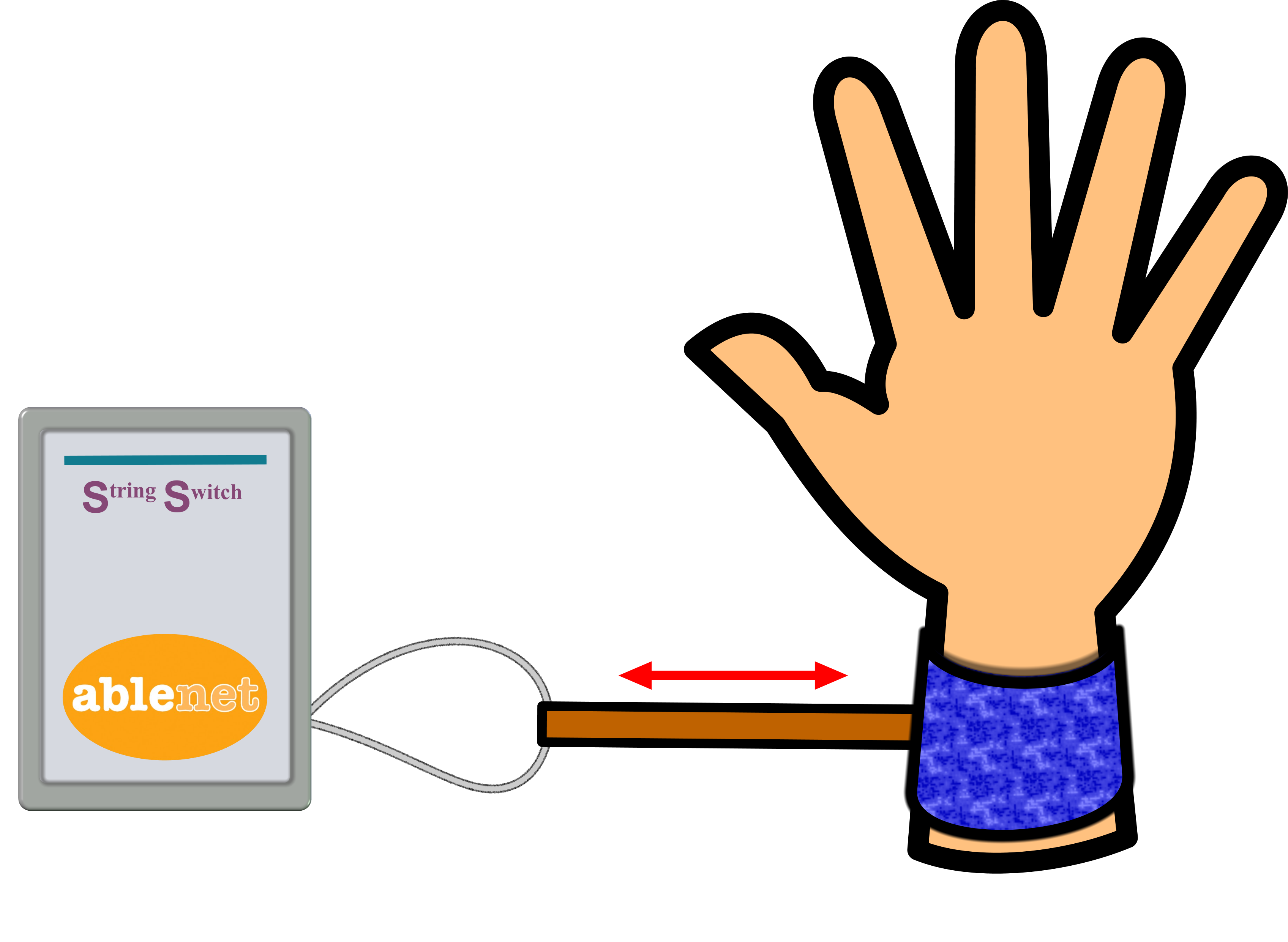
It is possible to adjust the distance the Learner's hand has to travel (in any direction) before the string switch is activated simply by adding an extra elastic band between the string and the wrist band. As the Learner moves his/her arm about there will come a time when it is moved a sufficient distance (accidental triggering) to cause the switch to be activated and the fan to blow (on to the Learner). The Learner will not make the connection between an arm movement (or leg movement or head movement) and operating the fan at first. Indeed, it may take some time. However, it is hoped, after a period of time the Learner may come to realise the connection. The PowerLink should be set to 'count' and a record should be kept of how many switch activations take place in a specific period of time (ten minutes?) each time this methodology is introduced for the Learner. If the number of activations from a baseline session:
The idea is a methodology to give Learners a way to control peripheral items easily through simple body movements which, unlike standard switches, are non-directional (The string switch does not care about the direction of the arm only the distance traveled which you can easily and simply adjust).
Learners who self harm by slapping their face or poking their eyes (for example) may be distracted by this methodology. As they move their hand to poke their eye, the string switch is activated before this can happen (purposeful triggering; purposeful triggering involves the use of the Individual's own body movement to self stimulate. As the Individual moves the body part, so it triggers the switch which, in turn, provides an alternate, nmore acceptable, form of sensory stimulation). The fan then blows into the Learner's face providing them with a safer and more acceptable alternative to eye poking. Eventually, it may be possible to fade the strength of the sensory stimulation and yet still motivate the Learner to continue to control the system thereby reducing the challenging behaviour.
- stays approximately the same it is likely that the Learner has not made any connection;
- increases over time this may imply that the Learner is starting to make a connection;
- decreases over time, it may be that the Learner is tired, bored with the sensation, does not like the sensation, or the switch is not working!
The idea is a methodology to give Learners a way to control peripheral items easily through simple body movements which, unlike standard switches, are non-directional (The string switch does not care about the direction of the arm only the distance traveled which you can easily and simply adjust).
Learners who self harm by slapping their face or poking their eyes (for example) may be distracted by this methodology. As they move their hand to poke their eye, the string switch is activated before this can happen (purposeful triggering; purposeful triggering involves the use of the Individual's own body movement to self stimulate. As the Individual moves the body part, so it triggers the switch which, in turn, provides an alternate, nmore acceptable, form of sensory stimulation). The fan then blows into the Learner's face providing them with a safer and more acceptable alternative to eye poking. Eventually, it may be possible to fade the strength of the sensory stimulation and yet still motivate the Learner to continue to control the system thereby reducing the challenging behaviour.
34. Get On The Right Track: Computer Access via a Switch

IEPMLD are unlikely to be able to access the world of computing through the standard methodology of keyboard and mouse; they will require alternative access. There are a number of ways to provide such access to a computer each of which is detailed in this section below.
1. Probably the simplest method is to use a BIGtrack (see figure left). This AbleNet Device simply plugs into a spare computer USB port. The BIGtrack is a mouse alternative comprising a large yellow track ball and two blue left and right mouse click buttons. However, it is unlikely that an IEPMLD will be able to control a computer even through this expanded and simplified system. The beauty of the BIGtrack lies in the fact that on each side of the device there is a 3.5 mm switch port to which a switch may be attached to provide either left or right mouse clicks respectively. As many programs, designed for use by IEPMLD, can be operated by a single mouse click, there is typically only a requirement for one switch for the left mouse click to be utilised.
It is possible to plug a single switch into the left socket of the BIGtrack and be ready to go. However a variation on this approach is to use a Jelly Beamer (from AbleNet) and receiver to provide wireless switch accessibility. The receiver section of the Jelly Beamer plugs into the left mouse socket of the Big Track and the Learner either uses the transmitter section of the Jelly Beamer as his/her switch OR the Learner's personal switch is plugged into this to provide wireless control.
1. Probably the simplest method is to use a BIGtrack (see figure left). This AbleNet Device simply plugs into a spare computer USB port. The BIGtrack is a mouse alternative comprising a large yellow track ball and two blue left and right mouse click buttons. However, it is unlikely that an IEPMLD will be able to control a computer even through this expanded and simplified system. The beauty of the BIGtrack lies in the fact that on each side of the device there is a 3.5 mm switch port to which a switch may be attached to provide either left or right mouse clicks respectively. As many programs, designed for use by IEPMLD, can be operated by a single mouse click, there is typically only a requirement for one switch for the left mouse click to be utilised.
It is possible to plug a single switch into the left socket of the BIGtrack and be ready to go. However a variation on this approach is to use a Jelly Beamer (from AbleNet) and receiver to provide wireless switch accessibility. The receiver section of the Jelly Beamer plugs into the left mouse socket of the Big Track and the Learner either uses the transmitter section of the Jelly Beamer as his/her switch OR the Learner's personal switch is plugged into this to provide wireless control.
It is possible to plug a single switch into the left socket of the BIGtrack and be ready to go. However, a variation on this approach is to use a Jelly Beamer (from AbleNet) and receiver to provide wireless switch accessibility. The receiver section of the Jelly Beamer plugs into the left mouse socket of the BIGTrack and the Learner either uses (the transmitter section of) the Jelly Beamer as his/her switch, OR the Learner's personal switch is plugged into this to provide wireless control. Wireless control is far safer for those Learners who tend to pull on wires.
Method one, detailed above, simply provides a left mouse click from a switch. While a lot can be done using this simple methodology, if the computer program requires more than a simple mouse click then alternative forms of access are required. However, an IEPMLD typically may not be able to cope with more than a single switch access and, therefore, method one may be all that is required.

2. Method two requires the purchase of a switch interface. A switch interfaces is typically a small rectangular box that plugs into a spare computer USB port. The interface can be configured to work in one of a choice (usually 4 or five) of 'modes' with each mode providing a set of available computer keys via switch access. There are several of these interfaces on the market but, here, I will only detail one of them; the Hitch. The Hitch is such an interface designed by AbleNet and available from your local AbleNet distributor/supplier.
While the Hitch might look a little complicated it is, in fact, very simple to use. It will work with a PC or Macintosh computer and simply plugs into an available USB port. Select one of six set-up choices from the options on the top of the Hitch, plug in a switch and you are ready to go! each choice provides switch access to five different keyboard keys: For example, the sixth set-up choice provides left mouse click, right mouse click, double click, space bar key, and enter key each from a separate switch. If the program required 'space' and 'enter' two switches would have to be attached into the switch jacks aligned with each option, one switch would then act as the 'space bar' and the other would act as the 'enter' key. The video below explains this very clearly if you are confused.
While the Hitch might look a little complicated it is, in fact, very simple to use. It will work with a PC or Macintosh computer and simply plugs into an available USB port. Select one of six set-up choices from the options on the top of the Hitch, plug in a switch and you are ready to go! each choice provides switch access to five different keyboard keys: For example, the sixth set-up choice provides left mouse click, right mouse click, double click, space bar key, and enter key each from a separate switch. If the program required 'space' and 'enter' two switches would have to be attached into the switch jacks aligned with each option, one switch would then act as the 'space bar' and the other would act as the 'enter' key. The video below explains this very clearly if you are confused.
Method Two actually costs less than method one and has the advantage of providing a larger range of computer key options. However, method one provides an enlarged trackball which may be a useful feature for other students in your establishment. All methods detailed here will provide a single switch access to a computer for specific software (typically special educational needs software).

Method 3. A third method of gaining switch access to a computer is via another type of switch box. However, unlike method two in which the options available are prescribed, method three allows you to decide exactly what each attached switch does (which key stroke it performs). Thus, if it was necessary to have one switch working as the 's' key from a computer keyboard and another working as the 'F1' key and yet another working as the '$' key, method three would permit this. In other words, each switch is definable. This is achieved via on screen software which is packaged with the product; the software allows each attached switch (typically, there can be several switches attached) to be designated as any computer keyboard key. There are several 'method three' interfaces available on the market, the one detailed here is called 'The JoyBox' and is available from Sensory Software or any Sensory Software supplier. The JoyBox allows eight switches to be connected for any use and four more switches can be connected for directional control. It can be used with almost all switch software, including switch games and communication programs. The JoyBox can be used as a mouse mover. Four switches (which are not included) control the movement of the pointer, with additional switches for click, double click, or other functions. The JoyBox comes complete with its own software to designate any switch that is attached. A cut down version of the JoyBox called the JoyCable, that permits a maximum of up to two attached switches is also available.
While method three is the most versatile of all the methods detailed here, with versatility comes increased complexity and some staff may not find it as easy as methods one and two. However, in a College or School setting in which there are a diverse range of abilities, method three comes into its own. It is extremely unlikely however that you would require method three for an IEPMLD's use.
While method three is the most versatile of all the methods detailed here, with versatility comes increased complexity and some staff may not find it as easy as methods one and two. However, in a College or School setting in which there are a diverse range of abilities, method three comes into its own. It is extremely unlikely however that you would require method three for an IEPMLD's use.
Now that the Learner can access a computer via a switch what programs are accessible and IEPMLD friendly? The problem here is that the vast majority of software that is available for IEPMLD was written for children and may not be appropriate for young adults. However, there is good news; it is fairly easy to create your own resources for this purpose. To this end, one section of this webpage (available below) is devoted to the creation of such resources using the Microsoft PowerPoint Program
35. PowerPoint for PMLD
Why PowerPoint for PMLD? There are a number of reasons:
- It is likely that your establishment already has this program and therefore it is available for immediate use;
- If your establishment already has it there is no further financial outlay;
- It can easily be made age-appropriate;
- it can be switch driven or accessed via a touch screen;
- it can work with multi-media formats (music and videos) which might prove highly motivating;
- it is non-judgmental;
- it does not tire and never gives up;
- it is always consistent.
- All Learners have BESTs (Best Ever Stimulating Thing) which are highly motivating. Admittedly, in some cases, a Learner's BEST may be difficult to discover. However, there will be, at least, one thing that will captivate a Learner's attention even for a brief period of time. PowerPoint can be used to supply a Learner's BESTs simply and consistently without ever stopping (The Learner will tire of the program before the program tires of the Learner). Let us assume that a Learner likes lorries, tractors and other such vehicles of this ilk. It is a simple mater to put a picture of one such vehicle on each slide of a PowerPoint accompanied by suitable sound effects and or music and have it be controlled by a single switch activation. Billions of images are available on Google and YouTube can provide videos and sound effects: It is not necessary to stray from an on-line computer to develop a PowerPoint program tailored to the needs of an individual. I once worked with a young man who was crazy about motorbikes. I developed this PowerPoint for him. ************* MOTORBIKE POWERPOINT HERE **********
- Animations (a): An animation that may capture a Learner's attention, and only animates when a switch is activated, can easily be created with PowerPoint. There are so many possibilities here and it would take a lot of space to detail them all so I will illustrate the concept with just three such ideas (see items 2, 3, and 4). The first is a pop-out (up, down, or from either side) controlled by a switch. On activating the switch, something happens for a brief period of time, after which the PowerPoint ceases all activity until the switch is activated again. If the switch is activated too many times then the program jumps between pop outs and the Learner does not get the full pop out. However, as the PowerPoint loops back on itself, it is only a matter of time before the Learner begins to comprehend the relationship between the switch and the activity. Of course, for IEPMLD this may take some time but PowerPoint is patient! Attached, is such a pop-out designed on a transport theme. If you don't have a switch attached, the PowerPoint will also work from a mouse click anywhere on the screen. Click here to download the 'Transport' PowerPoint.
- Animations (b): An animation may be something really simple such as a shape spinning or moving around the screen, Such animations can be accompanied by silly (or not so silly sound effects). Animations can be created within PowerPoint itself (there are a range of options available) or it is possible to use already animated images (typically refered to as animated gifs) that can be found all over the web. It is possible to look for an animated gif on any topic via a web search engine and save it for use within PowerPoint. The better animated gifs have a transparent background which makes them easier to use. Such animated gifs can be made to appear on the PowerPoint screen at the activation of a switch and then disappear on a further activation only to be replaced by some other interesting animation. Adding sounds effects and music can bring the whole thing to life.
- Animations (c): An animation may tell a simple story; a story that a Learner may understand. Such animations involve both sight and sound but typically do not require the repeated activation of a switch (although a switch may be used to start a story or move between it's component parts). Such animations are often used to illustrate Sensory Stories which are covered in a different section of this page.
- Scanning: Typically scanning is beyond the cognitive capabilities of IEPMLD to comprehend and, thus, it is with some hesitation that I include it at all in this section. However, it is one way of offering a choice via a single switch and it can be made very simple (although, as stated, it still may be beyond the abillities of some Learners). In a simple one switch scan, two options are presented (there can be as many options as is desired) one at a time with the ability to select either one by activating the switch. This is fairly easy to do using PowerPoint. Rather than attempting to explain the process further, it may be better understood by looking at an actual example. The example is a choice of two drinks (orange or apple) on a three second scan. Remember, you need to press CTRL A when the PowerPoint starts. Activating the switch selects a drink. When a drink has been selected, activating the switch again, restarts the scan. If you have not got a switch attached, you can also use your left mouse button and click anywhere on the screen. To download the 'Drinks' PowerPoint click here.
36. If music be the food ...

"If Music be the food of love, play on". The famous quote from Shakespeare's Twelfth Night is used here to make a tenuous link between music and dining. It is not uncommon for young people to want to listen to music while eating and it is no different simply because the young adult in question happens to have a disability.
I remember as a child listening to the radio whilst having Sunday lunch (Two way family favourites) and I always thought it a very special time. How can we make music available under the control of IEPMLD during lunch break in the dining hall?
Earlier on this webpage a methodology for controlling PowerPoint remotely (see appropriate section above) was detailed. If, instead of using a Jelly Beamer to provide remote access, the technology is switched to the use of a Big Beamer (also from AbleNet) which is then mounted flat against a suitable wall, at wheelchair height, almost any Learner would be able to activate its surface to cause PowerPoint to perform some action. The PowerPoint action in question would be to play a particular piece of music through a speaker system attached to the computer. The computer need not be new or fancy so long as it capable of running a version of PowerPoint it can be an old laptop stripped down to perform just this one function. It may be that the PowerPoint presentation is projected onto a suitable wall such that the music is accompanied by video. However, this is not essential. The 'computer' itself can be tucked out of harms way anywhere in the room; the Big Beamer's radio signal will easily reach it and thus play a particular track while the Learners are eating. Each slide of the PowerPoint (The PowerPoint can have as many slides as desirable, although it might be better to start with just a few slides providing seven or eight different songs) should carry one music video or just one piece of music such that, each time the wall switch is activated, the PowerPoint moves on a slide and plays a different piece of music. The presentation should be looped such that, if the final slide has been reached, and the switch is activated once again, it simply returns to the first track and begins over. In this way, a particularly determined individual could play the same track over and over! It would be good practice to vary the music considerably to see if the Learners have a particular preference. Learners may also come to realise that they can stop a disliked track simply by activating the wall switch once again. The music need not be loud, indeed some Learners may not like loud sounds and some may prefer a peaceful lunch break. However, peaceful lunch-breaks and special education are not typically comfortable bedfellows; there is usually a lot of noise and, thus, some soothing music might actually make the situation calmer (although many Learners may prefer music that is a little more energetic!).
Once set up (on a dedicated (inexpensive computer) with the activating BIGbeamer attached to an easily accessible wall), the staff really don't have much else to do: The BIG Beamer will require switching on during the time it is required as will the computer, and the PowerPoint program can be run by clicking on an icon on the desk top (save the PowerPoint as a PowerPoint show). The rest is in the hands (legs, feet, etc) of the Learners.
There are other ways of providing the same Learner controlled music via a single switch. It does not matter which is used so long as it is functional on a daily basis.
I remember as a child listening to the radio whilst having Sunday lunch (Two way family favourites) and I always thought it a very special time. How can we make music available under the control of IEPMLD during lunch break in the dining hall?
Earlier on this webpage a methodology for controlling PowerPoint remotely (see appropriate section above) was detailed. If, instead of using a Jelly Beamer to provide remote access, the technology is switched to the use of a Big Beamer (also from AbleNet) which is then mounted flat against a suitable wall, at wheelchair height, almost any Learner would be able to activate its surface to cause PowerPoint to perform some action. The PowerPoint action in question would be to play a particular piece of music through a speaker system attached to the computer. The computer need not be new or fancy so long as it capable of running a version of PowerPoint it can be an old laptop stripped down to perform just this one function. It may be that the PowerPoint presentation is projected onto a suitable wall such that the music is accompanied by video. However, this is not essential. The 'computer' itself can be tucked out of harms way anywhere in the room; the Big Beamer's radio signal will easily reach it and thus play a particular track while the Learners are eating. Each slide of the PowerPoint (The PowerPoint can have as many slides as desirable, although it might be better to start with just a few slides providing seven or eight different songs) should carry one music video or just one piece of music such that, each time the wall switch is activated, the PowerPoint moves on a slide and plays a different piece of music. The presentation should be looped such that, if the final slide has been reached, and the switch is activated once again, it simply returns to the first track and begins over. In this way, a particularly determined individual could play the same track over and over! It would be good practice to vary the music considerably to see if the Learners have a particular preference. Learners may also come to realise that they can stop a disliked track simply by activating the wall switch once again. The music need not be loud, indeed some Learners may not like loud sounds and some may prefer a peaceful lunch break. However, peaceful lunch-breaks and special education are not typically comfortable bedfellows; there is usually a lot of noise and, thus, some soothing music might actually make the situation calmer (although many Learners may prefer music that is a little more energetic!).
Once set up (on a dedicated (inexpensive computer) with the activating BIGbeamer attached to an easily accessible wall), the staff really don't have much else to do: The BIG Beamer will require switching on during the time it is required as will the computer, and the PowerPoint program can be run by clicking on an icon on the desk top (save the PowerPoint as a PowerPoint show). The rest is in the hands (legs, feet, etc) of the Learners.
There are other ways of providing the same Learner controlled music via a single switch. It does not matter which is used so long as it is functional on a daily basis.

|

|
|
Wall mounted Big Beamer signals to PowerPoint on laptop
What equipment will you need?
What equipment will you need?
- wall mounted BigBeamer with suitable symbol;
- receiver for BigBeamer which is plugged into ...;
- Hitch interface (or other alternative) which is plugged into ...;
- computer (laptop or otherwise) which is running ...;
- PowerPoint which is running ...;
- one music track per PowerPoint slide looped continuously.
37. Choice Food

Choice has to be a fundamental part of any educational system that puts the development of Learner empowerment through control at its heart. There should not be any part of the day that isn't an educational experience, that is not an opportunity for learning. All establishments, post 16 years of age, should not always be seeking to compartmentalise learning and put it into a room, at a specific time, in a specific curriculum; this tends to be a school model (although schools do not have to think this way). Rather, post sixteen education might seek to make the whole day an educational experience that is not limited to a classroom, a single building, a specifically ordered curriculum, or group based activities (see the section on self control above). Radical approach or not, or a mixture of approaches, there should not be any part of the day in which staff are not thinking about ways of providing choice for Learners. One such area is lunch. Often, this is not the case:
"However, individuals with severe handicaps often have little control over the foods and drinks that constitute their meals because of a lack of choice-making skills or opportunities to choose." (Parsons & Reid, 1990, page 184)
Staff should not be choosing foods for individual Learners in order to speed the process and increase efficiency but rather empowering Learners to make choices for themselves. It has been demonstrated that staff can not judge the preferences of Learner's in such matters accurately (Green et al., 1988; Parsons & Reid, 1990; Green, Reid, Canipe & Gardner, 1991; Fisher, Piazza Bowman, & Amari, 1996; Green, Gardner & Reid, 1997) and, furthermore, it has long been known that choosing for oneself is linked to increased happiness and greater quality of life outcomes (see, for example: Shevin & Klein, 1984; Guess, Benson, & Siegel Causey, 1985; Houghton, Bronicki, & Guess, 1987; Bannerman, Sheldon, Sherman, & Harchik, 1990) although at least one study questions this connection (see Schwartzman et al, 2004)
While, most canteen systems offer a choice of menu, too much choice can be as problematic as Hobson's choice (that is, no choice at all):
"When people have no choice, life is almost unbearable. As the number of available choices increases, as it has in our consumer culture, the
autonomy, control, and liberation this variety brings are powerful and positive. But as the number of choices keeps growing, negative
aspects of having a multitude of options begin to appear. As the number of choices grows further, the negatives escalate until we become overloaded. At this point, choice no longer liberates, but debilitates." (Schwartz, 2005, page 2)
Thus, best practice dictates that staff should limit presentation of meal choices for IEPMLD to a selection between two at any one time with the option of proving further choice if the Individual has no preference for the first items proffered (Pace, Ivancic, Edwards, Iwata & Page, 1985; Parsons & Reid, 1990; Fisher et al., 1992; DeLeon & Iwata, 1996; Fisher, Thompson, Piazza, Crosland & Gotjen, 1997).
Presentation of choice should always utilise tangible objects (real items rather than pictures, signs, or verbal descriptors) unless the Individual has been assessed and has been proven to be able to match tangible items to pictures, signs, or verbal descriptors (See Yu and Martin 2003). Thus, symbolic menu systems may not provide a reliable means of providing a choice of options at mealtimes for IEPMLD unless the individual has previously demonstrated an ability to match symbols to actual objects (in this instance, items of food and or drink). Of course, the use of symbols, signs, and language accompanying real objects is an acceptable means of teaching the association between them (symbol, sign, word) and the referent (real object) in real life situations.
"However, individuals with severe handicaps often have little control over the foods and drinks that constitute their meals because of a lack of choice-making skills or opportunities to choose." (Parsons & Reid, 1990, page 184)
Staff should not be choosing foods for individual Learners in order to speed the process and increase efficiency but rather empowering Learners to make choices for themselves. It has been demonstrated that staff can not judge the preferences of Learner's in such matters accurately (Green et al., 1988; Parsons & Reid, 1990; Green, Reid, Canipe & Gardner, 1991; Fisher, Piazza Bowman, & Amari, 1996; Green, Gardner & Reid, 1997) and, furthermore, it has long been known that choosing for oneself is linked to increased happiness and greater quality of life outcomes (see, for example: Shevin & Klein, 1984; Guess, Benson, & Siegel Causey, 1985; Houghton, Bronicki, & Guess, 1987; Bannerman, Sheldon, Sherman, & Harchik, 1990) although at least one study questions this connection (see Schwartzman et al, 2004)
While, most canteen systems offer a choice of menu, too much choice can be as problematic as Hobson's choice (that is, no choice at all):
"When people have no choice, life is almost unbearable. As the number of available choices increases, as it has in our consumer culture, the
autonomy, control, and liberation this variety brings are powerful and positive. But as the number of choices keeps growing, negative
aspects of having a multitude of options begin to appear. As the number of choices grows further, the negatives escalate until we become overloaded. At this point, choice no longer liberates, but debilitates." (Schwartz, 2005, page 2)
Thus, best practice dictates that staff should limit presentation of meal choices for IEPMLD to a selection between two at any one time with the option of proving further choice if the Individual has no preference for the first items proffered (Pace, Ivancic, Edwards, Iwata & Page, 1985; Parsons & Reid, 1990; Fisher et al., 1992; DeLeon & Iwata, 1996; Fisher, Thompson, Piazza, Crosland & Gotjen, 1997).
Presentation of choice should always utilise tangible objects (real items rather than pictures, signs, or verbal descriptors) unless the Individual has been assessed and has been proven to be able to match tangible items to pictures, signs, or verbal descriptors (See Yu and Martin 2003). Thus, symbolic menu systems may not provide a reliable means of providing a choice of options at mealtimes for IEPMLD unless the individual has previously demonstrated an ability to match symbols to actual objects (in this instance, items of food and or drink). Of course, the use of symbols, signs, and language accompanying real objects is an acceptable means of teaching the association between them (symbol, sign, word) and the referent (real object) in real life situations.
38. Sensory Integration
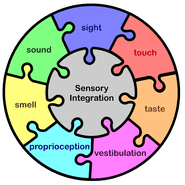
Sensory Integration is "the organization of sensory input for use. the use may be a perception of the body or the world, or an adaptive response, or a learning process, or the development of some neural function. Through sensory integration, the many parts of the nervous system work togetherso that a person can interact with the environment effectively and experience appropriate satisfaction." (Jean Ayres, 1979, page 184)
Our brains are processing information all through our waking moments. Information is flooding in from our eyes, ears, nose, skin, and tongue as well as from the sense that copes with the awareness of the position of our body in space (proprioception) and the sense that keeps us balanced such that we don't fall over when we stand (for example) vestibulation). In order to comprehend the world around us, understand our place within it, and be able to interact with what we 'sense', our brains must peform a huge number of calculations every second. All this normally goes on in the background below the level of our conscious minds. It is only when some task is a knew experience, particularly difficult, or something is impeding our thought process that we might become aware of some of the 'backroom processes' in play as we consciously attempt to bring them to the fore to aid in the achievement of our goal. Think for example of learning to ride a bike. Did you simply climb on and effortlessly ride off into the sunset? If you did you are a remarkably gifted person; most of us required assistance, stabilisers, and wobbled our way through short hesitant steps to something that we seemingly do without conscious thought today.
Our brains have to organise sensory input and put it to good use in achieving a specific goal. If something goes wrong then the goal becomes that much harder to achieve. Consider trying to read a book when a member of your family comes in and turns on the television and watches a music video. Some people might cope with blockig out the additional input; I would not. I would find myself reading the same line over and over until I had to turn off the TV or move to another room. Consider trying to follow a complex lecture while experiencing a migraine or an ear ache. We have all had experiences in which a goal has been twarted temporarily because of some sensory over stimulation or deficit (reading in poor light for example). If all these issues are possible for an average person on the street, consider how much more problematic it will be for the Individual experiencing Learning Difficulties; then, take it several stages further by prefixing 'learning difficulties' with the word 'profound'.
We know that definitions of 'Individuals Experiencing Profound & Multiple Learning Difficulties' (see earlier this web page) include reference to a likelihood one or more impairments of sensory input (visual impairment, hearing loss, tactile defensiveness, ...):
"An estimated 90% of people with PMD have profound, mostly cerebral, visual disorders and 25% have auditory limitations (Evenhuis
& Nagtzaam, 1999; Evenhuis, Theunissen, Denkers, Verschuure, & Kemme, 2001; van den Broek, Janssen, van Ramhorst, & Deen,
2004). Moreover, other senses, such as taste, smell and touch, are often damaged. It is obvious that these limitations affect the way people
with PMD process the stimuli that are offered to them. Therefore, it is essential that sensory abilities and limitations are charted and taken into account when offering activities, making the environment recognizable and looking for adequate forms of communication." (Petry et al, 2007c, page 135)
If such sensory impairments are additionally compounded by dysfunctional sensory integration processes:
Our brains are processing information all through our waking moments. Information is flooding in from our eyes, ears, nose, skin, and tongue as well as from the sense that copes with the awareness of the position of our body in space (proprioception) and the sense that keeps us balanced such that we don't fall over when we stand (for example) vestibulation). In order to comprehend the world around us, understand our place within it, and be able to interact with what we 'sense', our brains must peform a huge number of calculations every second. All this normally goes on in the background below the level of our conscious minds. It is only when some task is a knew experience, particularly difficult, or something is impeding our thought process that we might become aware of some of the 'backroom processes' in play as we consciously attempt to bring them to the fore to aid in the achievement of our goal. Think for example of learning to ride a bike. Did you simply climb on and effortlessly ride off into the sunset? If you did you are a remarkably gifted person; most of us required assistance, stabilisers, and wobbled our way through short hesitant steps to something that we seemingly do without conscious thought today.
Our brains have to organise sensory input and put it to good use in achieving a specific goal. If something goes wrong then the goal becomes that much harder to achieve. Consider trying to read a book when a member of your family comes in and turns on the television and watches a music video. Some people might cope with blockig out the additional input; I would not. I would find myself reading the same line over and over until I had to turn off the TV or move to another room. Consider trying to follow a complex lecture while experiencing a migraine or an ear ache. We have all had experiences in which a goal has been twarted temporarily because of some sensory over stimulation or deficit (reading in poor light for example). If all these issues are possible for an average person on the street, consider how much more problematic it will be for the Individual experiencing Learning Difficulties; then, take it several stages further by prefixing 'learning difficulties' with the word 'profound'.
We know that definitions of 'Individuals Experiencing Profound & Multiple Learning Difficulties' (see earlier this web page) include reference to a likelihood one or more impairments of sensory input (visual impairment, hearing loss, tactile defensiveness, ...):
"An estimated 90% of people with PMD have profound, mostly cerebral, visual disorders and 25% have auditory limitations (Evenhuis
& Nagtzaam, 1999; Evenhuis, Theunissen, Denkers, Verschuure, & Kemme, 2001; van den Broek, Janssen, van Ramhorst, & Deen,
2004). Moreover, other senses, such as taste, smell and touch, are often damaged. It is obvious that these limitations affect the way people
with PMD process the stimuli that are offered to them. Therefore, it is essential that sensory abilities and limitations are charted and taken into account when offering activities, making the environment recognizable and looking for adequate forms of communication." (Petry et al, 2007c, page 135)
If such sensory impairments are additionally compounded by dysfunctional sensory integration processes:
- intermittent input;
- non-sense in;
- not related (one sense to the other);
- over stimulated (hyper);
- under stimulated (hypo);
|
Sensory Integration can be seen as comprising three broad areas of interest as the diagram (right) depicts: Sensory Modulation and Sensory Discrimination which in turn influence Motor Planning. Problems can occur at any point within or between any of these areas. Indeed, there can be combined problems from more than one area conjoining to form one, often puzzling to outsiders, behavioural outcome.
Sensory Modulation is the way in which the brain adjusts the perception of sensory experiences as they arrive (or don't arrive) from the varying sense organs of the body. Some signals the brain 'chooses' to screen out: for example, people living near to a busy road may no longer be aware of the traffic flowing by whereas a person from a quiet country lane who comes to stay cannot initially get to sleep because of the sound. Habituation (to one or more particular sensory input) is a part of Sensory Modulation, one input gets turned down by the brain as it is unimportant to the particular focus at a specific time. Likewise it may be necessary to turn another sensory input up; if you were straining trying to hear what people were saying in another room for example. In order to do that you may choose to inhibit other sensory input such as shutting your eyes to turn off unwanted and distracting visual input. |
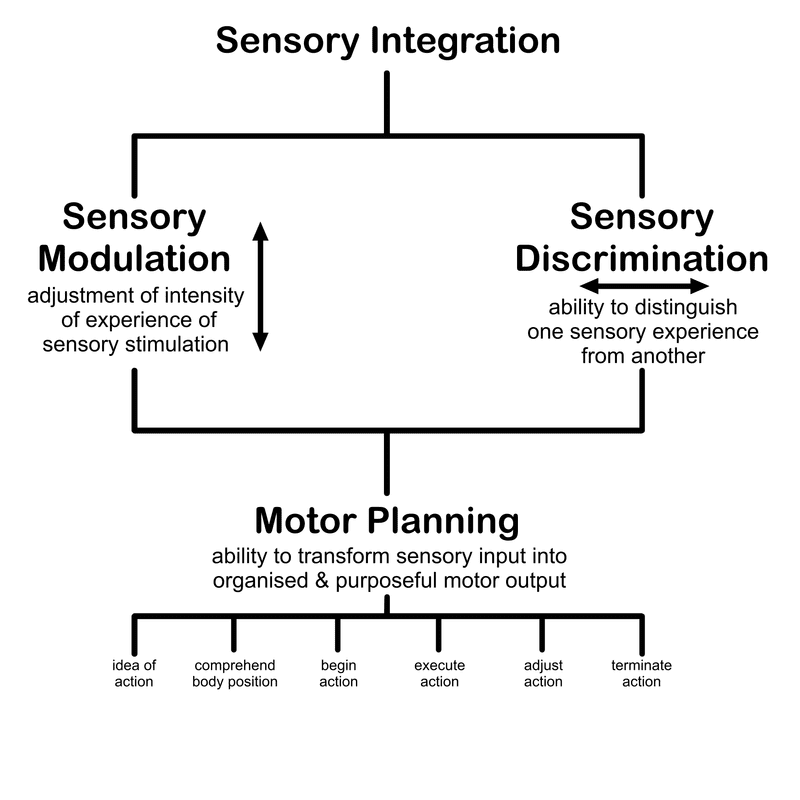
|
Now imagine that you cannot turn one or more sensory inputs up, down, off, or that there is no input from that particular sense at all. You would become hypersensitive (too much) or hyposensitive (too little) or experience some form of sensory deprivation (no input from that particular sense). How might such a sensory dysfunction affect understanding, your ability, and your behaviour? Learner energy and effort put into coping with one sensory input may displace/interfere with ability in another such that the 'other' may not be at its optimum level. For example, attention may suffer if a Learner is overloaded by auditory input with which s/he cannot cope. In order to optimise sensory awareness in one area it may be necessary to reduce sensory input/stimulation in another. Keeping extraneous input to a minimum (even eliminating it altogether) may be essential to promote learning in IEPMLD. Noisy, crowded and frequently interrupted sessions are thus not the best environment to foster learning.
Sensory Discrimination refers to a person's ability to distinguish between sensory inputs to the brain. If, for example, you could not tell if a sensation was coming from a specific part of your hand and believed it to be emanating from a different position how might that that affect your co-ordination. Have you ever had a toothache but been uncertain as to which tooth was causing the pain? Imagine extracting the wrong tooth!
If we combine issues with Sensory Modulation with issues with Sensory Discrimination it is not difficult to imagine the kinds of problems that might cause. Add to that a further complication in taking that dysfunction sensory input and translating it into some form of meaningful motor output/response and it can be seen that IEPMLD may have all manner of problems with sensory integration.
Sensory Integration practices are not seen by all as beneficial for IEPMLD. While the technique has its advocates (see, for example: Price, 1977; Reisman, 1993; Stonefelt & Stein,1998; Linderman & Stewart, 1999; Uyanik, Bumin, & Kayihan, 2003), it also has those who state that its claims are not justified:
"there is no valid, convincing proof in the limited studies conducted thus far on sensory integrative therapy to indicate that this treatment has
directly remediated or helped anyone with a learning disorder of any kind." (Lerer, 1981, page 4)
"until the therapeutic effectiveness of sensory integration therapy with mentally retarded persons is demonstrated, there exists no convincing empirical or theoretical support for the continued use of this therapy with that population outside of a research context" (Arendt et al.,1988. page 409)
"Our only addendum is that the current fund of research findings may well be sufficient to declare SI therapy not merely an unproven, but a demonstrably ineffective, primary or adjunctive remedial treatment for learning disabilities and other disorders." (Hoehn & Baumeister, 1994. Page 348)
However, perhaps the last words should go to Smith Roley et al (2007) who said:
"Part of the controversy stems from the many publications and intervention programs that do not truly reflect the principles of Ayres’s work but that have nonetheless been mistakenly associated with sensory integration."
and to Parham et al (2007) who said:
"Validity of sensory integration outcomes studies is threatened by weak fidelity in regard to therapeutic process. Inferences regarding sensory integration effectiveness cannot be drawn with confidence until fidelity is adequately addressed in outcomes research."
Meaning that the jury is still out on sensory integration as a tool for the amelioration of the cognitive and physical condition of Learners. We should not dismiss this practice out of hand, rather look to see what is useful in assisting those who we are charged to help.
Sensory Discrimination refers to a person's ability to distinguish between sensory inputs to the brain. If, for example, you could not tell if a sensation was coming from a specific part of your hand and believed it to be emanating from a different position how might that that affect your co-ordination. Have you ever had a toothache but been uncertain as to which tooth was causing the pain? Imagine extracting the wrong tooth!
If we combine issues with Sensory Modulation with issues with Sensory Discrimination it is not difficult to imagine the kinds of problems that might cause. Add to that a further complication in taking that dysfunction sensory input and translating it into some form of meaningful motor output/response and it can be seen that IEPMLD may have all manner of problems with sensory integration.
Sensory Integration practices are not seen by all as beneficial for IEPMLD. While the technique has its advocates (see, for example: Price, 1977; Reisman, 1993; Stonefelt & Stein,1998; Linderman & Stewart, 1999; Uyanik, Bumin, & Kayihan, 2003), it also has those who state that its claims are not justified:
"there is no valid, convincing proof in the limited studies conducted thus far on sensory integrative therapy to indicate that this treatment has
directly remediated or helped anyone with a learning disorder of any kind." (Lerer, 1981, page 4)
"until the therapeutic effectiveness of sensory integration therapy with mentally retarded persons is demonstrated, there exists no convincing empirical or theoretical support for the continued use of this therapy with that population outside of a research context" (Arendt et al.,1988. page 409)
"Our only addendum is that the current fund of research findings may well be sufficient to declare SI therapy not merely an unproven, but a demonstrably ineffective, primary or adjunctive remedial treatment for learning disabilities and other disorders." (Hoehn & Baumeister, 1994. Page 348)
However, perhaps the last words should go to Smith Roley et al (2007) who said:
"Part of the controversy stems from the many publications and intervention programs that do not truly reflect the principles of Ayres’s work but that have nonetheless been mistakenly associated with sensory integration."
and to Parham et al (2007) who said:
"Validity of sensory integration outcomes studies is threatened by weak fidelity in regard to therapeutic process. Inferences regarding sensory integration effectiveness cannot be drawn with confidence until fidelity is adequately addressed in outcomes research."
Meaning that the jury is still out on sensory integration as a tool for the amelioration of the cognitive and physical condition of Learners. We should not dismiss this practice out of hand, rather look to see what is useful in assisting those who we are charged to help.
39. Process not Product: Sensory Art

"Remember, it is the process of being involved in an activity that is important, not just the end product." (Fowler, page 37, 1997)
While Fowler (op.cit.) is undoubtedly correct in her assertion, I would argue that, within sensory art, it is the process that matters and the end product is relatively unimportant. However, the end product should be valued in its own right for what it is; the outcome of an individual Learner's experience and interaction with a set of materials at a given point in time. The experience and interaction of the Learner is what is important: It should not be the experience and interaction of staff performed on the 'Learner's behalf':
"When I took it home and showed Alex's mum, she said straight away, "Alex didn't do that. She couldn't make something as good as that. It is someone else's work."
The above quote came from a staff member (who also worked with Alex at home) during a meeting at a special education establishment. She was making the point that perfect products are the result of staff efforts and do not fool parents or carers into believing that they have been produced by their child. Indeed, is anyone fooled by claims that perfect results (paintings, baking, Christmas decorations, etc) are the product of IEPMLD especially if the Learner has additional physical and sensory impairments?
I am always concerned when I witness staff icing cakes or carefully placing papier-mâché on a balloon (or, indeed, any such thing) while a Learner sits and 'watches' (the Learner may not even be watching) and then exaggerated claims are made about Learner participation and understanding. Perfect products are problematic. Staff should not focus on the product but, rather, on the process.
MORE HERE ************************
While Fowler (op.cit.) is undoubtedly correct in her assertion, I would argue that, within sensory art, it is the process that matters and the end product is relatively unimportant. However, the end product should be valued in its own right for what it is; the outcome of an individual Learner's experience and interaction with a set of materials at a given point in time. The experience and interaction of the Learner is what is important: It should not be the experience and interaction of staff performed on the 'Learner's behalf':
"When I took it home and showed Alex's mum, she said straight away, "Alex didn't do that. She couldn't make something as good as that. It is someone else's work."
The above quote came from a staff member (who also worked with Alex at home) during a meeting at a special education establishment. She was making the point that perfect products are the result of staff efforts and do not fool parents or carers into believing that they have been produced by their child. Indeed, is anyone fooled by claims that perfect results (paintings, baking, Christmas decorations, etc) are the product of IEPMLD especially if the Learner has additional physical and sensory impairments?
I am always concerned when I witness staff icing cakes or carefully placing papier-mâché on a balloon (or, indeed, any such thing) while a Learner sits and 'watches' (the Learner may not even be watching) and then exaggerated claims are made about Learner participation and understanding. Perfect products are problematic. Staff should not focus on the product but, rather, on the process.
MORE HERE ************************
40. FACTS: Focus, Attend, Concentrate Training Scheme
In order to learn an individual needs to attend; it's a fact:
"Learners' ability to attend and learn may also differ with the time of day due to biorhythms. Levels of hormones, such as cortisol and adrenalin, vary throughout the day and affect learners' states of alertness. Blood sugar levels may also have an effect." (Quest for Learning Guidance Booklet 2007)
"Learners' ability to attend and learn may also differ with the time of day due to biorhythms. Levels of hormones, such as cortisol and adrenalin, vary throughout the day and affect learners' states of alertness. Blood sugar levels may also have an effect." (Quest for Learning Guidance Booklet 2007)
41. LOADS: Learning Object Awareness Differentiation Scheme
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
LOADS
42. Dressing Skills
James arrives at College each day in a minibus. He is met by the same staff member Debbie every time unless Debbie is absent. After saying hello, the first thing they do together is move into the College. Once inside, Debbie presents James with an Object Of Reference for moving to the lockers and removing clothing; in this instance his coat. They move together to the lockers and Debbie helps James to open his locker door. Debbie attempts to get James to refocus on the Object Of Reference which is a green, plastic coat hanger. She tells him that he needs to take his coat off and makes appropriate movements and signs. James smiles but does nothing. Debbie tries once again to get James to take off his coat independently. Once again, James does nothing. Debbie holds up the coat hanger and, with her free hand, unzips James' coat. Something stirs inside James and he starts to pull his coat open but goes no further. Debbie hangs the OOR on the locker door and assists James to remove his coat but always allowing him to do as much for himself as possible and prompts when and where necessary. Some days James will take his coat off by himself almost entirely, some days he needs a lot of help. Once James has removed his coat, Debbie assists him to put it on the hanger. James has never done this himself but Debbie always goes through the motions nevertheless. The routine continues with hanging the coat in the locker on its hanger and then closing the locker door. Debbie expects James to do as much of the process for himself and only assists as necessary when James is struggling or there is no response.
The clothes hanger has become the Object Of Reference for movement to the locker and for taking off clothing (if clothing is on) and for putting on clothing (if clothing is off). An empty clothes hanger means movement to the lockers. A second presentation of the empty hanger together with appropriate signs and simple language, means removal of specific items of clothing. However, if at the locker, the coat hanger plus coat is presented, the meaning is reversed; the coat needs to be put on. As clothes hangers are cheap and plentiful, some are kept in the classrooms for use at the end of the day to indicate the need to move to the locker area. Once presented, Learners are expected to carry the hanger to the locker area as independently as possible; they are not simply 'taken' (led hand in hand) to that specific place but rather 'assisted' with navigation through the College. Staff do not lead, they follow, and they assist as necessary. The coat hanger always means a movement to the locker area and, depending on its state (already with coat or without coat) on second presentation at the locker and the context (the student has his coat on or the coat is on the hanger), the student is expected to understand what is required.
The same routine is consistently and continually applied day after day. Indeed, James' parents have been informed about the practice and are now using a similar process at home also using a green plastic coat hanger. It is envisaged that one day James will only need to be presented with the coat hanger for him to take control and go through the process almost completely independently.
Samantha is a residential student. Each morning two staff members arrive at the same time to wake her. Each morning they have the same routine. Part of that routine is for Samantha to dress herself. In order to keep things a simple as possible, a staff member presents a choice of a single item of clothing one at a time in the order of dressing. For example, two tops are held up from which Sam may select. Sam's physical condition prevents her from being able to dress herself. However, she can choose what she wants to wear that day if the choices are simple (either of two tops for example). Sam typically eye points to the one she wants. On some days she will move an arm on the appropriate side to make a selection. Staff always go with the one that Sam appears to have chosen even if they believe the other option would be the better choice. 'What Sam looks at, is what Sam gets' is the rule. When the staff are assisting Sam in dressing, the staff encourage Sam to help as much as possible within her known abilities to make the process easier. Staff note and record any of Sam's anticipatory actions (body movements) in the dressing process. Sometimes Sam will move her arms to assist with dressing especially if she is a good mood. Staff do not have a special OOR for dressing, the clothes themselves are the OOR. Where practical, the clothes are presented in pairs such that Sam may make a choice. Typically Sam looks at one item more than the other but some days she refuses to cooperate and staff have taken this to mean that she does not want to wear either of the items presented and quickly present a further two selections.
At the end of the day, staff assist Sam to get undressed and into her night clothes. As the majority of what she is wearing needs to go into the laundry, they use a laundry basket as an OOR to indicate the need to get undressed.
Can students experiencing PMLD learn to dress and undress themselves independently for at least some items of clothing? Yes, they can providing they have the physical ability! (see, for example, Azrin, Schaeffer, & Wesolowski, 1976; Diorio & Konarski, 1984; Sisson, Kilwein & Van Hasselt, 1988; Reese and Snell, 1991; Hughes, Schuster, & Nelson, 1993; Lancioni et al, 2006; Lancioni et al, 2007). Reese and Snell (1991) made use of oversize clothes to facilitate the ease of dressing and undressing for individuals in their study and, as success was achieved, gradually reduced the size of the clothing until the individuals were dressing and undressing with appropriately sized garments.
In the classroom, sometimes (especially during Sensory Story activities), Learners get to dress up in scarves and hats, etc. The clothes themselves are the OOR in use. For example, Learners may be given a choice of hats to wear. While some may reach and take a hat, others may look at one hat more than the other; each will have their own unique way of indicating (what is taken to be) a 'choice'. Once a choice has been made staff assist each Learner with dressing up as necessary. Learners can indicate a great deal of understanding if, for example, they take a hat and put it on their head without prompting or assistance (see self-awareness section this web page). Large (safe) mirrors should always be available such that students can see the results of their choices.
While each Learner is different, each should be expected to do as much as they can independently of staff to get dressed or undressed. "Jeder nach seinen Fähigkeiten, jedem nach seinen Bedürfnissen" (from each according to ability, to each according to need) (Karl Marx 1875). Dressing and undressing involves communication, choice, cooperation, and control. It is an important aspect of the Learner's life and should not be rushed or seen as something that is external to the curriculum and of limited importance (we do it for her/him).
The clothes hanger has become the Object Of Reference for movement to the locker and for taking off clothing (if clothing is on) and for putting on clothing (if clothing is off). An empty clothes hanger means movement to the lockers. A second presentation of the empty hanger together with appropriate signs and simple language, means removal of specific items of clothing. However, if at the locker, the coat hanger plus coat is presented, the meaning is reversed; the coat needs to be put on. As clothes hangers are cheap and plentiful, some are kept in the classrooms for use at the end of the day to indicate the need to move to the locker area. Once presented, Learners are expected to carry the hanger to the locker area as independently as possible; they are not simply 'taken' (led hand in hand) to that specific place but rather 'assisted' with navigation through the College. Staff do not lead, they follow, and they assist as necessary. The coat hanger always means a movement to the locker area and, depending on its state (already with coat or without coat) on second presentation at the locker and the context (the student has his coat on or the coat is on the hanger), the student is expected to understand what is required.
The same routine is consistently and continually applied day after day. Indeed, James' parents have been informed about the practice and are now using a similar process at home also using a green plastic coat hanger. It is envisaged that one day James will only need to be presented with the coat hanger for him to take control and go through the process almost completely independently.
Samantha is a residential student. Each morning two staff members arrive at the same time to wake her. Each morning they have the same routine. Part of that routine is for Samantha to dress herself. In order to keep things a simple as possible, a staff member presents a choice of a single item of clothing one at a time in the order of dressing. For example, two tops are held up from which Sam may select. Sam's physical condition prevents her from being able to dress herself. However, she can choose what she wants to wear that day if the choices are simple (either of two tops for example). Sam typically eye points to the one she wants. On some days she will move an arm on the appropriate side to make a selection. Staff always go with the one that Sam appears to have chosen even if they believe the other option would be the better choice. 'What Sam looks at, is what Sam gets' is the rule. When the staff are assisting Sam in dressing, the staff encourage Sam to help as much as possible within her known abilities to make the process easier. Staff note and record any of Sam's anticipatory actions (body movements) in the dressing process. Sometimes Sam will move her arms to assist with dressing especially if she is a good mood. Staff do not have a special OOR for dressing, the clothes themselves are the OOR. Where practical, the clothes are presented in pairs such that Sam may make a choice. Typically Sam looks at one item more than the other but some days she refuses to cooperate and staff have taken this to mean that she does not want to wear either of the items presented and quickly present a further two selections.
At the end of the day, staff assist Sam to get undressed and into her night clothes. As the majority of what she is wearing needs to go into the laundry, they use a laundry basket as an OOR to indicate the need to get undressed.
Can students experiencing PMLD learn to dress and undress themselves independently for at least some items of clothing? Yes, they can providing they have the physical ability! (see, for example, Azrin, Schaeffer, & Wesolowski, 1976; Diorio & Konarski, 1984; Sisson, Kilwein & Van Hasselt, 1988; Reese and Snell, 1991; Hughes, Schuster, & Nelson, 1993; Lancioni et al, 2006; Lancioni et al, 2007). Reese and Snell (1991) made use of oversize clothes to facilitate the ease of dressing and undressing for individuals in their study and, as success was achieved, gradually reduced the size of the clothing until the individuals were dressing and undressing with appropriately sized garments.
In the classroom, sometimes (especially during Sensory Story activities), Learners get to dress up in scarves and hats, etc. The clothes themselves are the OOR in use. For example, Learners may be given a choice of hats to wear. While some may reach and take a hat, others may look at one hat more than the other; each will have their own unique way of indicating (what is taken to be) a 'choice'. Once a choice has been made staff assist each Learner with dressing up as necessary. Learners can indicate a great deal of understanding if, for example, they take a hat and put it on their head without prompting or assistance (see self-awareness section this web page). Large (safe) mirrors should always be available such that students can see the results of their choices.
While each Learner is different, each should be expected to do as much as they can independently of staff to get dressed or undressed. "Jeder nach seinen Fähigkeiten, jedem nach seinen Bedürfnissen" (from each according to ability, to each according to need) (Karl Marx 1875). Dressing and undressing involves communication, choice, cooperation, and control. It is an important aspect of the Learner's life and should not be rushed or seen as something that is external to the curriculum and of limited importance (we do it for her/him).
43. Practical Puzzles
I watched a young woman, whom I had observed spending most of her morning doing little more than simply rocking back and forth, open a drinks bottle and take a drink during her lunch break. She picked up thje plastic bottle, unscrewed the cap, put the cap on the table top, then lifted the bottle to her mouth and began to drink. I was somewhat taken aback after having spent the greater part of two hours observing her and others in her group during the morning. This young woman had abilities that were not evident at all in the classroom and yet, when she was motivated to achieve a particular goal, she evidently had no problems at all, either cognitively or physically, in obtaining a drink from a sealed container. Ignoring, for the moment, the obvious question concerning the appropriateness of the classroom activities during the morning sessions, her ability to cope with a somewhat challenging puzzle (obtaining the drink) highlighted the importance of motivation in learning. The drink was motivating for this young adult experiencing Profound and Multiple Learning Difficulties. She had somehow learned to:
I began to wonder if she would be able to discriminate between bottles. I thought about the inherent danger in leaving her in any situation where there might be a nearby bottle containing other than a drink. I shuddered at the thought. I also began to think about ways in which staff might build upon this already established behaviour in ways to promote learning and understanding.
Practical Puzzles are means to promote learning and understanding through challenging uses of BESTs (Best Ever Stimulating Thing[s] - motivational POLEs {People, Objects, Locations, events and experiences}). For example, if we were to cover the young woman's bottle of juice with a tea towel would she uncovered it in order to obtain her drink; in other words, does she display an understanding of object permanence (Object permanence refers to the understanding that out of sight does not equate to out of mind; the item is still there, it has not gone)? What if we covered the bottle with a box? What if we ... it is possible to envisage all sorts of small increases in the challenge posed by a task that might exercise individual cognition: Practical puzzles are means to doing just that.
For some Learners, a task which we might find unproblematic, might pose a significant challenge either cognitively or physically or both. To obtain a BEST, will a Learner solve a simple challenge (one that has been tailored to his/her specific needs)? If we were to put a piece of chocolate in a clear plastic container (without a lid) could the Learner retrieve it? If yes, what would happen if we placed a piece of cardboard over the top of the container containing the reward? Each success suggests yet another challenge, another puzzle for the Individual to solve. Failure? There is no such thing as failure here! There was previously success, what possible explanations could account for our Learner's current inability to solve the puzzle? Can we address any of them? Can we step back to a previous level and move forward in a different way? Is there a smaller increment that we can attempt?
My Learner's BEST is a walk in the sensory garden. I can't put that in a bottle!
OK. Can we make the key to the doorway to the sensory garden (or some other relevant object) the object that the Learner must provide to obtain this treat? If we were to get the Learner to hold the key over several trips to the garden such that the key itself becomes the Object Of Reference for this particular BEST (be wary of using any key because then any Learner encounter with a key must result in a trip to the garden - see Object Of Reference page this website) then the key might become the focus for our Practical Puzzles. For example; is the Learner able to:
My Learner hasn't the physical skills to do what you are suggesting.
The word 'practical' in 'practical puzzles' suggests that each puzzle has to be 'practical' for (relevant and tailored to the requirements of) each Learner. Thus, limited physical abilities require puzzles that require limited physical dexterity. However, if there is an absence of any physical ability then this particular activity might not be meaningful for this particular Individual. Not everything on this page will apply to every Learner.
- recognise bottles as containing drinks;
- recognise and locate the bottle top;
- remove the top by unscrewing;
- handle bottles in such a way as to place the correct part to her mouth;
- tilt the bottle to obtain the drink;
- not spill the drink;
- put the bottle down right way up after drinking.
I began to wonder if she would be able to discriminate between bottles. I thought about the inherent danger in leaving her in any situation where there might be a nearby bottle containing other than a drink. I shuddered at the thought. I also began to think about ways in which staff might build upon this already established behaviour in ways to promote learning and understanding.
Practical Puzzles are means to promote learning and understanding through challenging uses of BESTs (Best Ever Stimulating Thing[s] - motivational POLEs {People, Objects, Locations, events and experiences}). For example, if we were to cover the young woman's bottle of juice with a tea towel would she uncovered it in order to obtain her drink; in other words, does she display an understanding of object permanence (Object permanence refers to the understanding that out of sight does not equate to out of mind; the item is still there, it has not gone)? What if we covered the bottle with a box? What if we ... it is possible to envisage all sorts of small increases in the challenge posed by a task that might exercise individual cognition: Practical puzzles are means to doing just that.
For some Learners, a task which we might find unproblematic, might pose a significant challenge either cognitively or physically or both. To obtain a BEST, will a Learner solve a simple challenge (one that has been tailored to his/her specific needs)? If we were to put a piece of chocolate in a clear plastic container (without a lid) could the Learner retrieve it? If yes, what would happen if we placed a piece of cardboard over the top of the container containing the reward? Each success suggests yet another challenge, another puzzle for the Individual to solve. Failure? There is no such thing as failure here! There was previously success, what possible explanations could account for our Learner's current inability to solve the puzzle? Can we address any of them? Can we step back to a previous level and move forward in a different way? Is there a smaller increment that we can attempt?
My Learner's BEST is a walk in the sensory garden. I can't put that in a bottle!
OK. Can we make the key to the doorway to the sensory garden (or some other relevant object) the object that the Learner must provide to obtain this treat? If we were to get the Learner to hold the key over several trips to the garden such that the key itself becomes the Object Of Reference for this particular BEST (be wary of using any key because then any Learner encounter with a key must result in a trip to the garden - see Object Of Reference page this website) then the key might become the focus for our Practical Puzzles. For example; is the Learner able to:
- get the key out of a box?
- locate the key from within one of several boxes?
- take the key from a bent wire by moving it along?
- select the key from a box of other objects?
- select the correct key from of other keys (let's begin with just two very dissimilar keys)?
My Learner hasn't the physical skills to do what you are suggesting.
The word 'practical' in 'practical puzzles' suggests that each puzzle has to be 'practical' for (relevant and tailored to the requirements of) each Learner. Thus, limited physical abilities require puzzles that require limited physical dexterity. However, if there is an absence of any physical ability then this particular activity might not be meaningful for this particular Individual. Not everything on this page will apply to every Learner.
44. Leisurely Development

"A second problem pertains to the limited number and lack of variation in developmental and leisure activities, resulting in boredom and repetitive routines (De Waele & Van Hove, 2005; Seifert, 2002; Seys et al., 1998; Zijlstra & Vlaskamp, 2005). People with PIMD have only limited opportunities to participate in everyday activities, and only a small proportion of their leisure time is spent away from the living unit (Campo, Sharpton, Thompson, & Sexton, 1997; Seifert, 2002; Zijlstra & Vlaskamp, 2005). In addition, their preferences, interests and capacities are not sufficiently taken into account when designing programs and selecting activities (Seifert, 2002; Zijlstra & Vlaskamp, 2005)."
(Maes et al, 2007, page 164)
"In studies on the quality of life of individuals with intellectual disability in general, it has become obvious that people with PIMD are a vulnerable group... They also have fewer opportunities to live in a typical community environment, less variety in their day-today and leisure activities, less choice, fewer opportunities for social participation, a less active life-style, and a lower level of engagement in meaningful daily
activities (Emerson et al., 2000; Felce, Lowe, Beecham, & Hallam, 2000; Felce, Lowe, & Jones, 2002; Hatton, Emerson, Robertson, Henderson, & Cooper, 1996; Mansell, Beadle-Brown, Macdonald, & Ashman, 2003; Stancliffe & Lakin, 1998)." (Maes et al, 2007, page 164)
(Maes et al, 2007, page 164)
"In studies on the quality of life of individuals with intellectual disability in general, it has become obvious that people with PIMD are a vulnerable group... They also have fewer opportunities to live in a typical community environment, less variety in their day-today and leisure activities, less choice, fewer opportunities for social participation, a less active life-style, and a lower level of engagement in meaningful daily
activities (Emerson et al., 2000; Felce, Lowe, Beecham, & Hallam, 2000; Felce, Lowe, & Jones, 2002; Hatton, Emerson, Robertson, Henderson, & Cooper, 1996; Mansell, Beadle-Brown, Macdonald, & Ashman, 2003; Stancliffe & Lakin, 1998)." (Maes et al, 2007, page 164)
45. Increase Toleration

Many Learners Experiencing Profound and Multiple Learning Difficulties (IEPMLD) will likely display intolerance to specific objects designed to be of help. For example, some individuals may not appear to tolerate the wearing of glasses to correct their vision although seemingly the glasses are designed to help. Other individuals may remove headphones designed to focus their hearing on specific outcomes of their actions (for example, activating a switch to a computer to play some auditory reward).
While some may claim such 'intolerance' is a personal choice not to allow a specific item to be used or worn and therefore it should be respected, unless it can be shown that the individual is capable of understanding and making such a choice and the individual has chosen not to work with the item, it is counterproductive to simply stop all further use of such items: Such a course of action neither aids progress nor assists the individual. Rather, a more professional course of action would be to work on increasing the Learner's tolerance of a specific experience:
"It may be that the learner constantly pulls them off his face. In such cases it may be possible to set up, and keep to, a rigid timetable of gradually building up having them worn. Try starting with a few seconds and, if necessary, offer some sort of reward so that wearing glasses equals 'good stuff'!" (Aitken and Buultjens 1992, page 66).
There will be those Learners who are 'tactile defensive'. Tactile defensiveness (first identified by Dr. Jean Ayres in the 1960s) is defined as forms of observable behavioural and emotional responses, which are aversively disproportionate to specific forms of tactile stimuli that the majority of people would find to be non-painful and non-threatening (see Royeen & Lane, 1991). It is a type of Sensory Integrative Dysfunction (see Jean Ayres, 1970) which may be described as the brain’s inability to process, coordinate, and utilise information from the senses. Those with tactile defensive may react to haptic experiences with 'fight, flight or fright' (see Trott 1993)(fight - behaviour that staff might consider challenging; flight - moving (body part) away from the sensory source, withdrawing cooperation; fright - showing signs of anxiety, distress). While tactile defensiveness itself may not directly interfere with learning, the inability to tolerate sensory stimuli and refusal to work with specific experiences may indirectly impede progress. It should also be noted that Individuals experiencing tactile defensiveness are more likely to have additional hypersensitivity to other forms of sensory stimulation (such as lights, sound, and movements). Such 'Sensory Defensiveness' can impact significantly on an individual's ability to cope in a learning environment particularly one which is crowded and noisy. Typically, the tactile defensive individual is likely to be characterised by one or more of the following attributes (Ayres 1964, 1972, 1979). The Individual may:
"the tactilely defensive child has too much protective activity and not enough discriminative processing. Instead of finding out what sensations mean, he tends to react to them in a fight or-flight way" (Ayres, 1979, page 110).
What can be done to assist those who are tactile defensive? The following techniques may be of help (see Sears, 1981; Mailloux, 1992, Nackley, 2001):
While some may claim such 'intolerance' is a personal choice not to allow a specific item to be used or worn and therefore it should be respected, unless it can be shown that the individual is capable of understanding and making such a choice and the individual has chosen not to work with the item, it is counterproductive to simply stop all further use of such items: Such a course of action neither aids progress nor assists the individual. Rather, a more professional course of action would be to work on increasing the Learner's tolerance of a specific experience:
"It may be that the learner constantly pulls them off his face. In such cases it may be possible to set up, and keep to, a rigid timetable of gradually building up having them worn. Try starting with a few seconds and, if necessary, offer some sort of reward so that wearing glasses equals 'good stuff'!" (Aitken and Buultjens 1992, page 66).
There will be those Learners who are 'tactile defensive'. Tactile defensiveness (first identified by Dr. Jean Ayres in the 1960s) is defined as forms of observable behavioural and emotional responses, which are aversively disproportionate to specific forms of tactile stimuli that the majority of people would find to be non-painful and non-threatening (see Royeen & Lane, 1991). It is a type of Sensory Integrative Dysfunction (see Jean Ayres, 1970) which may be described as the brain’s inability to process, coordinate, and utilise information from the senses. Those with tactile defensive may react to haptic experiences with 'fight, flight or fright' (see Trott 1993)(fight - behaviour that staff might consider challenging; flight - moving (body part) away from the sensory source, withdrawing cooperation; fright - showing signs of anxiety, distress). While tactile defensiveness itself may not directly interfere with learning, the inability to tolerate sensory stimuli and refusal to work with specific experiences may indirectly impede progress. It should also be noted that Individuals experiencing tactile defensiveness are more likely to have additional hypersensitivity to other forms of sensory stimulation (such as lights, sound, and movements). Such 'Sensory Defensiveness' can impact significantly on an individual's ability to cope in a learning environment particularly one which is crowded and noisy. Typically, the tactile defensive individual is likely to be characterised by one or more of the following attributes (Ayres 1964, 1972, 1979). The Individual may:
- tolerate her/his own self-initiated touch but react negatively to touch from another individual, especially if the touch is unexpected, from behind, or out of the individual's field of vision.
- demonstrate increased motor activities and affective responses (often negative) when tactile stimulation is continuous because of the cumulative effects of the tactile stimuli.
- becomes distressed and uncomfortable when situated within a group of people due to her/his anticipation and fear of being touched.
- initiate a behaviour that staff may find challenging in order to withdraw from a situation perceived as tactilely threatening or demonstrate more overt responses to touch which reflect his anxiety, hostility, emotional lability, and/or aggression.
- avoid touching certain surfaces and textures because of sensations ranging from discomfort to pain which result from the contact.
- prefer to keep her/his body well covered with clothing regardless of the temperature.
- dislike getting hands into such materials as finger paint, glue, paste, or papier mache and avoids walking barefoot in sand or wading in water.
- demonstrate extreme defensiveness about the head and face, especially around the mouth.
"the tactilely defensive child has too much protective activity and not enough discriminative processing. Instead of finding out what sensations mean, he tends to react to them in a fight or-flight way" (Ayres, 1979, page 110).
What can be done to assist those who are tactile defensive? The following techniques may be of help (see Sears, 1981; Mailloux, 1992, Nackley, 2001):
- The use of firm pressure when touching the individual. Avoid the use of light touch.
- Firm, straight, downward pushes on both shoulders may be calming.
- No surprises: Ensure the Individual is expecting the touch.
- Approach the individual from the front. Avoid working from behind the Individual.
- Position yourself at the Learner's eye level so that all your movements can be observed.
- Try to communicate what is going to occur before touching the Learner. Attempt to direct the Learner through any activity little by little such that Learner-initiated touch is used.
- Demonstrate on your own body rather than the Learner's.
- Encourage but never force participation.
- Let the Learner control the situation. Give time and space for the Learner to experience the sensations without stress or fear.
- Minimise the likelihood of others touching the Individual by accident. Do not work in crowded conditions for example in which the Learner may display anxiety.
- Establish a consistent work space for the Learner in the classroom; one that s/he come to learn to trust and within which s/he feels safe. The space should be outside of typical pathways used by others to move around, enter, or leave the room. Allow the Learner to work in this 'personal space' for task demands. In some instances, you can move desks and other furniture around to create barriers to prevent others from entering the personal space.
- Avoid overcrowded spaces. Don't position the Individual near to others especially those who are likely to move around a lot.
- Establish a consistent staff support such that Learner comes to trust specific members of the team.
- Establish a means of Escape. That is, create a method by which the Learner can communicate anxiety and be removed from the threat. Thus providing an acceptable alternative to possible challenging behaviour.
- Create Consistent Communication: use the same signs (and other modes of communication) to represent attributes of objects. Don't swap between big, large, chunky, sizable, etc to describe an object - select a simple form and use it consistently such that the Learner has a chance to come to know what to expect.
- Minimize possible overwhelming environmental stimuli (use natural lighting; shut the classroom door; use rubber bottoms on the chair and desk legs; provide curtains, blinds, and room dividers).
- Try to eliminate non-pertinent classroom aromas;
- Heavier items are generally better than lighter ones for use in activities.
- Talk to the therapy team (particularly the OT) for strategies to address this issue.
46. Self Awareness
Self-awareness refers to the capacity of becoming the object of one’s own attention (Duval & Wicklund, 1972).
"Self-awareness entails bodily awareness (Kyselo 2014) as measured by self-face recognition (Gallup 1985), thinking about any possible private (internal) and public (visible) self-aspects (Ben-Artzi et al. 1995), as well as about one's past (autobiography; Markowitsch & Staniloiu 2011) and future (prospection; Szpunar 2010). Self-awareness is also associated with a host of various self-related operations, among which are self-description (Marsh 1994), self-knowledge (Wilson 2009), self-concept formation (L'Ecuyer 1978) self-evaluation (Higgins, 1987), self-esteem (Rosenberg 1965), sense of agency (a minimal form of self-awareness; Farrer & Frith 2002), self-regulation (Baumeister & Vohs 2007), self-efficacy (Bandura 1977), and Theory-of-Mind (ToM) (Dimaggio et al. 2008)." (Morin, 2017)
In typically developing humans, self-awareness can be demonstrated as occurring at 18 - 24 months of age.
"Prior to the age of eighteen months, infants do not seem to know that what they are seeing in a mirror is their own reflection. After eighteen months, they do. This can be shown by surreptitiously marking infants’ faces with rouge, so that they are unaware that the mark has been placed. When younger infants see their reflections, they point to the mirror and not to themselves. After the age of eighteen months or so, they touch the rouge on their own faces instead of just pointing to the mirror." (Stern, 1985, p. 165)
In interviews with 100 individuals with ages ranging from 10 through 24 years who were experiencing varying levels of learning difficulties, Narayan et al (1993) showed that the level of cognition was directly related to the concept of self-awareness with individuals at the lowest levels demonstrating none.
Several experimental methodologies have been designed to explore aspects of self-awareness and self-consciousness in animals. Perhaps the best known among them, the mirror mark test, developed by Gallup (1970), seeks to determine whether an animal recognizes itself in the mirror by placing a coloured dot on the animal’s body. The mark is positioned in an out-of-view body part so that it can be detected only with assistance of a mirror. This is done without the subject noticing or with a procedure of sham marking used as a control. The mark test determines if the animal can use its reflection to locate the mark on its body, as measured by its inspection, touching, or rubbing of the spot. Very few species pass the mark test of mirror self-recognition. In research using similar methodologies with Individuals Experiencing Profound and Multiple Learning difficulties there was little or no self awareness demonstrated (Shentoub, SouIairac, & Rustin, 1955; Pechacek et al., 1973; Harris 1977; Hill & Tomlin,1981). However, there is an alternate explanation to these results; in order to demonstrate self awareness through the Gallup (1970) methodology a person (animal in Gallup case) must be cognisant of the fact that a mirror reflects an image of themselves. Failing to understand the concept of a mirror is not the same as a failure to have self-awareness; it may be that there is self-awareness but no understanding that the image in the mirror is in fact a reflection of themselves. However, while the mirror methodology may not be able to disprove a lack of self awareness (absence of evidence is not evidence of absence), should the Individual respond to the mirror test positively and investigate a mark on her/his face then this action would be seen as evidence of self awareness.
Gallup (1970) and Amsterdam (1972) based on work with primarily primates and infants, identified three responses to encounters with mirrors:
"Self-awareness entails bodily awareness (Kyselo 2014) as measured by self-face recognition (Gallup 1985), thinking about any possible private (internal) and public (visible) self-aspects (Ben-Artzi et al. 1995), as well as about one's past (autobiography; Markowitsch & Staniloiu 2011) and future (prospection; Szpunar 2010). Self-awareness is also associated with a host of various self-related operations, among which are self-description (Marsh 1994), self-knowledge (Wilson 2009), self-concept formation (L'Ecuyer 1978) self-evaluation (Higgins, 1987), self-esteem (Rosenberg 1965), sense of agency (a minimal form of self-awareness; Farrer & Frith 2002), self-regulation (Baumeister & Vohs 2007), self-efficacy (Bandura 1977), and Theory-of-Mind (ToM) (Dimaggio et al. 2008)." (Morin, 2017)
In typically developing humans, self-awareness can be demonstrated as occurring at 18 - 24 months of age.
"Prior to the age of eighteen months, infants do not seem to know that what they are seeing in a mirror is their own reflection. After eighteen months, they do. This can be shown by surreptitiously marking infants’ faces with rouge, so that they are unaware that the mark has been placed. When younger infants see their reflections, they point to the mirror and not to themselves. After the age of eighteen months or so, they touch the rouge on their own faces instead of just pointing to the mirror." (Stern, 1985, p. 165)
In interviews with 100 individuals with ages ranging from 10 through 24 years who were experiencing varying levels of learning difficulties, Narayan et al (1993) showed that the level of cognition was directly related to the concept of self-awareness with individuals at the lowest levels demonstrating none.
Several experimental methodologies have been designed to explore aspects of self-awareness and self-consciousness in animals. Perhaps the best known among them, the mirror mark test, developed by Gallup (1970), seeks to determine whether an animal recognizes itself in the mirror by placing a coloured dot on the animal’s body. The mark is positioned in an out-of-view body part so that it can be detected only with assistance of a mirror. This is done without the subject noticing or with a procedure of sham marking used as a control. The mark test determines if the animal can use its reflection to locate the mark on its body, as measured by its inspection, touching, or rubbing of the spot. Very few species pass the mark test of mirror self-recognition. In research using similar methodologies with Individuals Experiencing Profound and Multiple Learning difficulties there was little or no self awareness demonstrated (Shentoub, SouIairac, & Rustin, 1955; Pechacek et al., 1973; Harris 1977; Hill & Tomlin,1981). However, there is an alternate explanation to these results; in order to demonstrate self awareness through the Gallup (1970) methodology a person (animal in Gallup case) must be cognisant of the fact that a mirror reflects an image of themselves. Failing to understand the concept of a mirror is not the same as a failure to have self-awareness; it may be that there is self-awareness but no understanding that the image in the mirror is in fact a reflection of themselves. However, while the mirror methodology may not be able to disprove a lack of self awareness (absence of evidence is not evidence of absence), should the Individual respond to the mirror test positively and investigate a mark on her/his face then this action would be seen as evidence of self awareness.
Gallup (1970) and Amsterdam (1972) based on work with primarily primates and infants, identified three responses to encounters with mirrors:
- Exploratory and social behaviour as if the individual were observing another member of the same species;
- Contingency behaviour whereby the individual performs a number of repetitive acts as a way of testing its actions against the visual stimulus;
- Self-directed behaviour whereby the individual uses the mirror to investigate a particular part of its body, often because an 'alien' out-of-place object has been position on it (typically this is a mark test).
However, a study by Broesch et al (2011) casts a little doubt on at least some aspects of all of this: When she tried the mark mirror test with children outside the U.S. (and developed Western world), she obtained results that were different. For example, in Kenya, only two out of 82 children succeeded with the mirror mark test and some of those were over five years of age! Those who did not pass did not have learning difficulties. The majority reacted to the mirror by 'freezing'; they stood still and appeared to be uncomfortable with the reflected image. Broesch and her team (op. cit.) took their test to Fiji, Saint Lucia, Grenada, Peru, Canada and the USA, where they tested 133 children aged between 36 and 55 months. The performance of the children from North America was in line with past research, with 88 per cent of the American children and 77 per cent of the Canadians 'succeeding' with the test. However, the success rate in Saint Lucia was lower (58 per cent), Peru (52%) and Grenada (51%) and, in Fiji, not one of the children passed the test. Thus, simply failing the mirror test may not, in itself, be a total indication of a lack of self awareness skills. Many animals may be unconcerned about a mark on their faces! It might be argued that pigs, for example, spend a lot of their time with marks on their faces and would simply ignore them; it does not follow that they are not self aware. Nevertheless, let's not throw the baby out with the bathwater! In the instance of the non-Western children, the researchers themselves postulated that the children did understand that it was themselves in the mirror (some were nearly six years old), and the mark was not a part of their normal body image, but they were unsure of an acceptable response and were scared to touch or to try to remove it. Whether this is correct or not, it has been repeatedly shown that (Western) children at around 15 months do not react to the mark test and yet, a few months later, the very same children, at around 18 months (some may take up to 24 months to pass the test), use the mirror to locate and touch the mark. While this does not conclusively prove that before 18 - 24 months of age children aren't self aware, it does suggest, at least, after this time, the vast majority of them are.
Research conducted with children experiencing learning difficulties indicated that, when mental age was used as the criterion, they also
exhibited self-recognition behaviors at about 18 to 24 months (Hill & Tomlin, 1981; Mans et al., 1978). If IEPMLD is defined by having a mental age of lower than two years then it provides a possible explanation of a lack of self awareness in this population (they have not yet developed to the mental level at which self awareness arises). Neuman and Hill (1978) found that above the chronological age of 5 years, Individuals with autism displayed self-recognition suggesting a developmental lag of around three years beyond that of typically developing peers.
"Self-awareness is the first step in becoming a self-advocate and is positively related to life success. Students must know and understand themselves before they can tell others what they want or need." (Reader, 2011).
Does it therefore follow if an individual demonstrates self-awareness they cannot be classified as experiencing PMLD? That, suddenly, they have progressed into the higher level 'experiencing SLD' category? It certainly is suggestive of such a level of ability. However, as self recognition can occur from 18 months, it may be simply that the Individual is demonstrating abilities at the higher end of a 'PMLD continuum', that is, there will be a proportion of Learners who will show such awareness. It also suggests that progression through this 'continuum' can be evidenced by developing and demonstrating self-awareness in Learners. Personally, I have never been comfortable with a definition of IEPMLD that includes a mental age equivalent of up to two years; I have always limited it to up to one year of mental age equivalence. Typically, children between one and two years of age demonstrate greater abilities than many of the Learners with whom I have worked.
"Many learners with PMLD do not progress very far along the developmental route set out by the biologist, Jean Piaget. Piaget describes the first stage of development in young infants as 'the sensory‐motor stage' (0‐ 2 years) within which typical babies learn to use their senses and
connect those with moving their bodies to start the journey of understanding the world around them (Goswami, 2008). Most people with PMLD remain within this stage throughout their lives, depending highly on personal sensory‐motor experiences which they find hard to generalise." (Lacey, 2015, page 43)
Thus, I would not expect IEPMLD to pass the mirror test and, if they did, I would not only be extremely pleased but also begin to believe that they could no longer be classified as 'profound' any longer.
What are the component factors in self awareness in Individuals Experiencing Learning Difficulty? In identifying, working with, and developing these abilities, we may move the Learner towards a state of self-awareness. A definitive list of such components is hard to find but we may speculate on at least some of the constituents (see, for example, Morin 2017). For example, one component must surely be the ability to recognise 'other': environmental awareness, at least in respect of items in the immediate environment:
"The important distinction here is as follows: One can perceive and process stimuli from the environment (e.g., a color, food) without explicitly knowing that one is doing so (consciousness).One becomes self-aware when one reflects on the experience of perceiving and processing stimuli (e.g., I see a blue object; I am eating food and it tastes good)." (Morin, 2011)
exhibited self-recognition behaviors at about 18 to 24 months (Hill & Tomlin, 1981; Mans et al., 1978). If IEPMLD is defined by having a mental age of lower than two years then it provides a possible explanation of a lack of self awareness in this population (they have not yet developed to the mental level at which self awareness arises). Neuman and Hill (1978) found that above the chronological age of 5 years, Individuals with autism displayed self-recognition suggesting a developmental lag of around three years beyond that of typically developing peers.
"Self-awareness is the first step in becoming a self-advocate and is positively related to life success. Students must know and understand themselves before they can tell others what they want or need." (Reader, 2011).
Does it therefore follow if an individual demonstrates self-awareness they cannot be classified as experiencing PMLD? That, suddenly, they have progressed into the higher level 'experiencing SLD' category? It certainly is suggestive of such a level of ability. However, as self recognition can occur from 18 months, it may be simply that the Individual is demonstrating abilities at the higher end of a 'PMLD continuum', that is, there will be a proportion of Learners who will show such awareness. It also suggests that progression through this 'continuum' can be evidenced by developing and demonstrating self-awareness in Learners. Personally, I have never been comfortable with a definition of IEPMLD that includes a mental age equivalent of up to two years; I have always limited it to up to one year of mental age equivalence. Typically, children between one and two years of age demonstrate greater abilities than many of the Learners with whom I have worked.
"Many learners with PMLD do not progress very far along the developmental route set out by the biologist, Jean Piaget. Piaget describes the first stage of development in young infants as 'the sensory‐motor stage' (0‐ 2 years) within which typical babies learn to use their senses and
connect those with moving their bodies to start the journey of understanding the world around them (Goswami, 2008). Most people with PMLD remain within this stage throughout their lives, depending highly on personal sensory‐motor experiences which they find hard to generalise." (Lacey, 2015, page 43)
Thus, I would not expect IEPMLD to pass the mirror test and, if they did, I would not only be extremely pleased but also begin to believe that they could no longer be classified as 'profound' any longer.
What are the component factors in self awareness in Individuals Experiencing Learning Difficulty? In identifying, working with, and developing these abilities, we may move the Learner towards a state of self-awareness. A definitive list of such components is hard to find but we may speculate on at least some of the constituents (see, for example, Morin 2017). For example, one component must surely be the ability to recognise 'other': environmental awareness, at least in respect of items in the immediate environment:
"The important distinction here is as follows: One can perceive and process stimuli from the environment (e.g., a color, food) without explicitly knowing that one is doing so (consciousness).One becomes self-aware when one reflects on the experience of perceiving and processing stimuli (e.g., I see a blue object; I am eating food and it tastes good)." (Morin, 2011)
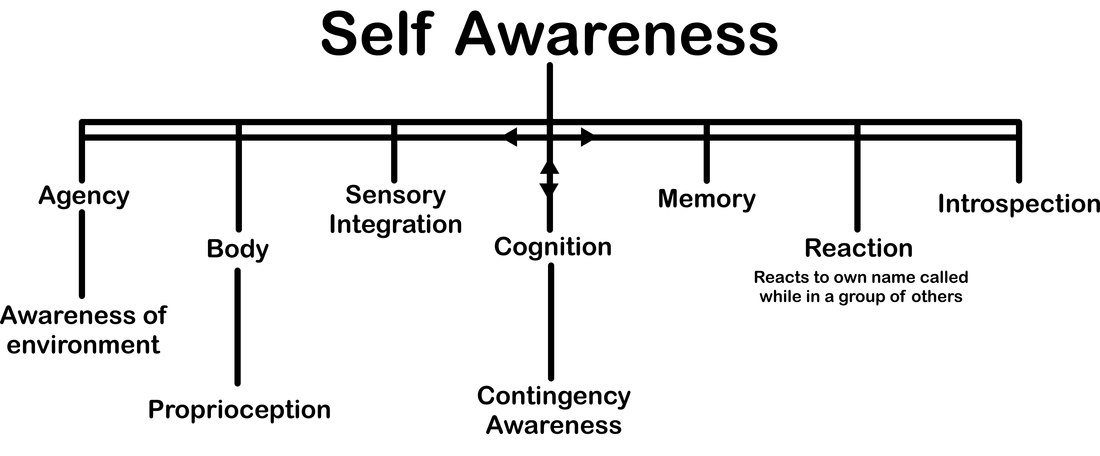
The above chart, detailing the components whose inter-relationship somehow combines to form self-awareness, is both speculative and non-definitive: It is open to acceptance or adjustments, amendments, and abrogations as the reader may see fit. It perhaps is a useful starting point from which we may begin to create tools to develop self awareness skills in Learners. If you believe something is missing or that some part is misleading then please contact Talksense with your suggestions ([email protected]). The chart aims to respond to the statement, "I knew I was becoming self-aware when ..." and goes on to supply several suggested subsidiary components, each of which is detailed further in the section below. I knew I was becoming self aware when ...
... I achieved agency:
Agency refers to a Learner's ability to act as an 'agent' within the world around her/him; to interact with objects in the immediate environment. If such agency is self-fulfilling (that is, it serves a purpose useful to the agent) the it would seem like that this forms a basis for some aspect of the concept of self-awareness.
"Another important aspect of consciousness concerns awareness of our own actions and our sense of being in control of them (the sense of agency." (Farrer & Frith, 2002)
"In our everyday life we often perform goal-directed actions which we normally do not reflect upon such as grasping a glass of water when we are thirsty. Actions or certain movements may happen because an intention-to-act generated a corresponding motor program in order to reach the intentional goal. But how do we know that we ourselves are the ones grasping the glass of water? An executed movement is associated with certain expected consequences, for example, feeling the arm move in a certain way or perceiving the glass in our hand. Such proprioceptive or visual re-afferences as well as corresponding motor signals may not only help to adjust a given motor program but may also contribute to the feeling that we are the agents, that is, initiators and executors of our grasping the glass of water. This experience of oneself as the agent of one’s own actions—and not of others’ actions—has been described as ‘‘the sense of agency” (Gallagher, 2000) and is a central feature of the different phenomenal experiences constituting self-consciousness." (David, Newen, & Vogeley 2008)(see also
Synofzik, Vosgerau, & Newen, 2008)
... I became aware of my immediate environment and objects within it:
It would seem logical to assume that if a person has no awareness of an external world that their knowledge of themselves as an agent within that world is severely curtailed if not nonexistent.
"Finally, probably the less ambiguous demonstration of Level 2 self-awareness is when infants start systematically to reach for objects they see, deliberately bringing their hands in contact with objects." (Rochat, 2003)
... I started to be aware of the parts of my body:
It would seem reasonable to expect that before one can become aware of oneself as a whole one must become aware of different parts of your body from head to toe and what you are able to do with them (abilities and limitations). This is the most basic form of self-knowledge (Wilson 2009). If a Learner can respond to a command to move a particular body part, or copy a body part movement illustrated by another, of correctly place an item of clothing onto a part of her/his own body, or pick up and correctly utilise an implement to interact with an external event then it would appear logical to assume some awareness of the corresponding body part(s).
“Everywhere in the world, self starts with body” (Baumeister, 1999, page 2)
"The components of physical self-concept have included physical ability and physical appearance." (Hong & Perkins, 1997)
... I became aware of my body in space; I was proprioceptive:
Proprioception is the awareness of a person of position in space of any part of their body, this also encompasses awareness of movement. To have such an awareness must, by definition, be a component of self-awareness. Proprioception must exist if the Learner can move and adjust any limb (or other body part) in time and space to manipulate an external object, for example, picking up a beaker and taking a drink or turning body/head to look at a particularly interesting stimulus.
"To sum up, as has been shown here, proprioceptive sense plays a crucial role in education and formation, and is a basis of individual differences and personality construct." (Liutsko, 2013)
... all my senses were telling me I was; I had Sensory Integration:
As sensory integration is covered elsewhere on this webpage it will not be detailed further here other than to state that information coming in from all the sense available to the Learner must play a part in the concept of self. If such information does not form a coherent whole then it is difficult to see how an individual can make sense of the world both without and within.
"Many children experience some level of challenge coping with sensory input from their everyday environments and activities. Some
children may experience difficulty in processing stimuli for one or more of the five ‘external senses’ – touch, sight, sound, taste and smell. Sensory processing issues may also affect a child’s sense of movement and/or sense of body awareness which are the ‘internal senses’"
(NCAC, 2011)
"Multisensory integration can update the mental representation of one’s body, such as the sense of ownership of body parts (Longo et al.,
2008) or whole body (Ehrsson, 2007; Lenggenhager et al., 2007; Petkova & Ehrsson, 2008), the physical appearance of one’s body (Longo et al., 2009), and the more abstract narrative representations of one’s self (Bergouignan, Nyberg, & Ehrsson, 2014)." (Tsakiris, 2017, page 599)
... my cognition showed it; I was able to think about myself:
The notion of cognition has already been covered in this section. It is central to the whole concept and interrelates with each aspect listed. As cognition develops with age typically developing children develop self awareness between 18 and 24 months which may impair self awareness for IEMPLD who may be operating at mental age levels below that. One thing we know about PMLD is, a defining characteristic, reduced cognition:
"Learners with PMLD by definition have enormous difficulties in the area of cognition (thinking and learning). They struggle with even the most rudimentary logical thinking, understanding cause and effect, solving simple problems and using what they have learned in one context in another. Even those who have acquired basic understanding of cause and effect, appear to be very limited in how they can apply this understanding." (Lacey, 2015, page 43)
... I developed cause and effect skills, I had contingency awareness:
Contingency awareness (cause and effect skills) is covered elsewhere on this webpage and will therefore not be covered in depth here. However, the knowledge that one can have an effect on the environment, objects and beings within it must relate to the concept of self-awareness (see agency above).
"Infants also learn to detect the contingency between their actions and consequent environmental events. For example, one study found that 2-month old infants increase their rate of leg-kicking when it moves a mobile, but not when it does not (Watson, 1972). Moreover, infants smile and coo more when viewing a mobile they control, suggesting not only that they are able to detect contingencies, but also that they enjoy the ability to control objects in their environment. In consideration of these and other findings, Gergely and Watson (1999; see also,
Gergely, 2001) have proposed that humans are born with a 'contingency detection module' that analyzes the contingency between their actions and environmental events. Initially, the module is geared toward identifying self-initiated actions that produce perfectly contingent outcomes. Presumably, this preference helps the infant develop a representation of the self as distinct from the physical environment." (Brown, J.D., 2009)
Perhaps, it would be best to leave the final word, in this section, to Penny Lacey:
"If we have discovered the learner with PMLD is beginning to learn about 'contingency awareness' then that should become central to all their learning. School children may be working on a range of curriculum activities and adult learners are likely to be involved in a range of community activities but what is required for all at this stage is for teachers and supporters to provide as many opportunities as possible to practice contingency awareness. This should be done throughout the day, preferably with a range of different resources so the person can learn to generalise his/her understanding in many different situations." (Lacey, 2015, page 45)
... I could remember what I looked like not just when looking in the mirror but also photographs of myself from years before. My memory helped to show me that I knew me:
There is an old myth that goldfish have but a three second memory and, thus, it is not cruel to keep them in a small bowl as the fish see everywhere they look as a new image:
"A lot of people have this stereotype image of a goldfish with a three second memory and that's not the case at all. It is probably accurate to say that many fishes such as minnows, sticklebacks and guppies are capable of the same intellectual feats as rats or mice." (Webster, 2008)(see also Balcombe, 2016)
Even with such a level of cognition is it likely that goldfish are self aware? Are rats self aware? There are some that appear to suggest that they are (see for example, Foote & Crystal, 2007). However, it would seem logical to assume that, if memory is severely curtailed it is going to be more difficult to recognise a self-image as recognition, by definition implies a prior memory:
"After formulizing the representation of each face, the last step is to recognize the identities of these faces. In order to achieve automatic recognition, a face database is required to build. For each person, several images are taken and their features are extracted and stored in the database. Then when an input face image comes in, we perform face detection and feature extraction, and compare its feature to each face class stored in the database." (Chao, 2007)
As the quote states, digital face recognition requires a comparison to a database of stored images. Likewise, self-awareness must require active recall: a memory of things past. It is thought that IEPMLD have poor memory skills:
"The work of Hulme and Mckenzie (1992) suggests that difficulties with memory are experienced, not just by people with Down syndrome
but by others with severe learning difficulties and this can help explain why people with PMLD seem to have huge difficulties in remembering even much repeated activities. Maybe some people with PMLD constantly experience, even much repeated, activities as if for the first time? Maybe even people they meet on a daily basis are strangers to them every time?" (Lacey, 2015, page 44)
This, if the case, might exclude such Learners from self-awareness but what if we work to improve cognition and memory. Can memory be improved? There is a wealth of research material supporting the notion that it can (See, for example, Suzuki, 2015 & 2016). Furthermore, if we turn the concept on its head, and we can demonstrate self-awareness in any Learner then, the Individual's memory must, by definition, be sufficient to support the ability.
I have argued that, for IEPMLD, memory is history and history is memory; that history sessions in educational establishments should not be on events from hundreds of year in the past but, rather, from moments in an individual's experience of the present which, as you read this statement, has just become your past and your history. Thus, let your history sessions become memory sessions ... you are still providing 'history' but history that has relevance to the Individual. For more on this concept and ideas for teaching history to IEPMLD go to the history page on this website.
... I was aware of external stimuli and reacted and I responded to interactions; for example, I reacted appropriately when someone called out my name when I was in a group:
In 2006 Alain Morin wrote:
"It is assumed that to direct attention outward or inward an organism first needs to be awake; if not, the term 'unconsciousness' is used to designate the state in which there is no processing of information, either from the environment or the self. Examples of unconscious
conditions are coma and sleep. When awake and 'conscious', one will process information in the environment and intelligently respond to stimuli. In that state an organism will directly experience perceptions, sensations, thoughts, etc. without being aware that such perceptual
and mental events are taking place. The organism will be totally immersed in experience - an unreflective actor in one’s environment. In this perspective, most - if not all - animals possess 'consciousness'. Humans too arguably spend a large amount of time in a state of
consciousness, interacting with objects and persons, talking, walking, or coherently thinking, without monitoring these activities. I would argue here that Block’s notion of 'phenomenal consciousness' (1995), that is, what it is like to experience mental events such as seeing,
smelling, tasting, or having pains, represents consciousness as defined above. Note that although this definition emphasizes an awareness of external stimuli, and not the self, a minimal consciousness of self is required for the organism to move in, and interact with, the
environment. This has been termed 'first-person perspective' or 'subjective perspectivalness' (Vogeley & Fink, 2003); it involves a diffuse, implicit body awareness allowing articulate spatial self-navigation." (Morin, 2006, page 359)
Morin states that he believes a "minimal consciousness of self is required for the organism to move in, and interact with, the environment" and, thus, in interacting with the environment IEPMLD are demonstrating a 'consciousness of self' although, albeit, a minimal awareness. However, in demonstrating an ability to interact with external objects and events in a purposeful manner the Individual is also demonstrating self-awareness.
There are instances in which an individual can demonstrate self-awareness through reactions to external stimuli:
... when I was capable of Introspection:
In patients who have experienced some form of severe brain trauma, it has been noted that, for those who go on to make a good recovery, conscious experience typically returns at the same time as inner speech (Ojemann,1986; Morin, 2009). Furthermore, many individuals (without any trauma) state the they experience a loss of inner speech at the point when they are falling asleep and losing wakeful consciousness (Rusalova, 2005). It is unsurprising therefore that a loss of inner speech (as a result of brain trauma) adversely impacts self-awareness:
"I had lost the ability to converse with others, I had also lost the ability to engage in self-talk. In other words, I did not have the ability to think about the future - to worry, to anticipate or perceive it - at least not with words. Thus for the first 4 or 5 weeks after hospitalization I simply existed." (Moss, 1972, page 10)
"This indicates that the more one engages in introspection to acquire self-information and develop a self-concept, the more one talks to oneself (about oneself), and vice-versa" (Morin, 2009) See also (Briscoe, 2002; Leary, 2004; Morin, 2004; Nelson, 2005)
As, by definition, IEPMLD do not possess speech, can it be also assumed that such Learners do not have inner-speech either? In other words, is self-reflection possible without speech and, therefore, is self-awareness possible without self-reflection?
"So inner speech, and thus language, would play an important role in self-referential activities. Said differently: inner speech would represent an important cognitive process underlying self-awareness. Note that this view does not implicate that there is no self-awareness without language. We can be aware of a pain without having to talk to ourselves about it... as I stated before, self-awareness may be possible without language." (Morin, No date, Language and Self Awareness, Science and Consciousness Review)
However, Helen Keller noted that:
"before my teacher came to me, I did not know that I am. I lived in a world that was a no world... When I learned the meaning of ‘I’ and ‘me’ and found that I was something, I began to think. Then consciousness first existed for me." (cited in Salzen, 1998, page 307)
In addition, Ojemann states:
"As recovery occurs, conscious experience returns as well. It seems to return in parallel with the phenomenon of inner speech. Inner speech may be limited, restricted, concrete, foggy, not normal after these kinds of lesions, but at least conscious experience has come back." (Ojemann,1986, page 161)
If some animals can demonstrate self-awareness and animals do not have inner speech (at least in the sense of an inner form of verbalised output) then it must be theoretical possible for some IEPMLD to be self-aware also (or to develop self-awareness). As Morin states (op.cit.) 'self-awareness may be possible without language'. If an ant can be said to be self-aware (Cammaerts & Cammaerts, 2015) then surely all IEPMLD can be helped to achieve this goal. The Development and demonstration of Learner self-awareness should be a part of any curriculum that purports to benefit IEPMLD. It has been shown that even after extensive damage to the brain an individual can still be self- aware (Philippi et al, 2012).
"The findings in this study confirm that Roger's Self-Awareness is largely preserved. In keeping with previous work ..., the findings show that Roger is a conscious, self-aware, and sentient human being despite the widespread destruction of cortical regions purported to play a critical role in Self-Awareness, namely the insula, anterior cingulate cortex, and medial prefrontal cortex." (Philippi et al, 2012)
MOE ON BRAIN DAMAGE HERE
The following are some strategies that may prove useful in such a scheme (there is no pretence that the list is comprehensive);
... I achieved agency:
Agency refers to a Learner's ability to act as an 'agent' within the world around her/him; to interact with objects in the immediate environment. If such agency is self-fulfilling (that is, it serves a purpose useful to the agent) the it would seem like that this forms a basis for some aspect of the concept of self-awareness.
"Another important aspect of consciousness concerns awareness of our own actions and our sense of being in control of them (the sense of agency." (Farrer & Frith, 2002)
"In our everyday life we often perform goal-directed actions which we normally do not reflect upon such as grasping a glass of water when we are thirsty. Actions or certain movements may happen because an intention-to-act generated a corresponding motor program in order to reach the intentional goal. But how do we know that we ourselves are the ones grasping the glass of water? An executed movement is associated with certain expected consequences, for example, feeling the arm move in a certain way or perceiving the glass in our hand. Such proprioceptive or visual re-afferences as well as corresponding motor signals may not only help to adjust a given motor program but may also contribute to the feeling that we are the agents, that is, initiators and executors of our grasping the glass of water. This experience of oneself as the agent of one’s own actions—and not of others’ actions—has been described as ‘‘the sense of agency” (Gallagher, 2000) and is a central feature of the different phenomenal experiences constituting self-consciousness." (David, Newen, & Vogeley 2008)(see also
Synofzik, Vosgerau, & Newen, 2008)
... I became aware of my immediate environment and objects within it:
It would seem logical to assume that if a person has no awareness of an external world that their knowledge of themselves as an agent within that world is severely curtailed if not nonexistent.
"Finally, probably the less ambiguous demonstration of Level 2 self-awareness is when infants start systematically to reach for objects they see, deliberately bringing their hands in contact with objects." (Rochat, 2003)
... I started to be aware of the parts of my body:
It would seem reasonable to expect that before one can become aware of oneself as a whole one must become aware of different parts of your body from head to toe and what you are able to do with them (abilities and limitations). This is the most basic form of self-knowledge (Wilson 2009). If a Learner can respond to a command to move a particular body part, or copy a body part movement illustrated by another, of correctly place an item of clothing onto a part of her/his own body, or pick up and correctly utilise an implement to interact with an external event then it would appear logical to assume some awareness of the corresponding body part(s).
“Everywhere in the world, self starts with body” (Baumeister, 1999, page 2)
"The components of physical self-concept have included physical ability and physical appearance." (Hong & Perkins, 1997)
... I became aware of my body in space; I was proprioceptive:
Proprioception is the awareness of a person of position in space of any part of their body, this also encompasses awareness of movement. To have such an awareness must, by definition, be a component of self-awareness. Proprioception must exist if the Learner can move and adjust any limb (or other body part) in time and space to manipulate an external object, for example, picking up a beaker and taking a drink or turning body/head to look at a particularly interesting stimulus.
"To sum up, as has been shown here, proprioceptive sense plays a crucial role in education and formation, and is a basis of individual differences and personality construct." (Liutsko, 2013)
... all my senses were telling me I was; I had Sensory Integration:
As sensory integration is covered elsewhere on this webpage it will not be detailed further here other than to state that information coming in from all the sense available to the Learner must play a part in the concept of self. If such information does not form a coherent whole then it is difficult to see how an individual can make sense of the world both without and within.
"Many children experience some level of challenge coping with sensory input from their everyday environments and activities. Some
children may experience difficulty in processing stimuli for one or more of the five ‘external senses’ – touch, sight, sound, taste and smell. Sensory processing issues may also affect a child’s sense of movement and/or sense of body awareness which are the ‘internal senses’"
(NCAC, 2011)
"Multisensory integration can update the mental representation of one’s body, such as the sense of ownership of body parts (Longo et al.,
2008) or whole body (Ehrsson, 2007; Lenggenhager et al., 2007; Petkova & Ehrsson, 2008), the physical appearance of one’s body (Longo et al., 2009), and the more abstract narrative representations of one’s self (Bergouignan, Nyberg, & Ehrsson, 2014)." (Tsakiris, 2017, page 599)
... my cognition showed it; I was able to think about myself:
The notion of cognition has already been covered in this section. It is central to the whole concept and interrelates with each aspect listed. As cognition develops with age typically developing children develop self awareness between 18 and 24 months which may impair self awareness for IEMPLD who may be operating at mental age levels below that. One thing we know about PMLD is, a defining characteristic, reduced cognition:
"Learners with PMLD by definition have enormous difficulties in the area of cognition (thinking and learning). They struggle with even the most rudimentary logical thinking, understanding cause and effect, solving simple problems and using what they have learned in one context in another. Even those who have acquired basic understanding of cause and effect, appear to be very limited in how they can apply this understanding." (Lacey, 2015, page 43)
... I developed cause and effect skills, I had contingency awareness:
Contingency awareness (cause and effect skills) is covered elsewhere on this webpage and will therefore not be covered in depth here. However, the knowledge that one can have an effect on the environment, objects and beings within it must relate to the concept of self-awareness (see agency above).
"Infants also learn to detect the contingency between their actions and consequent environmental events. For example, one study found that 2-month old infants increase their rate of leg-kicking when it moves a mobile, but not when it does not (Watson, 1972). Moreover, infants smile and coo more when viewing a mobile they control, suggesting not only that they are able to detect contingencies, but also that they enjoy the ability to control objects in their environment. In consideration of these and other findings, Gergely and Watson (1999; see also,
Gergely, 2001) have proposed that humans are born with a 'contingency detection module' that analyzes the contingency between their actions and environmental events. Initially, the module is geared toward identifying self-initiated actions that produce perfectly contingent outcomes. Presumably, this preference helps the infant develop a representation of the self as distinct from the physical environment." (Brown, J.D., 2009)
Perhaps, it would be best to leave the final word, in this section, to Penny Lacey:
"If we have discovered the learner with PMLD is beginning to learn about 'contingency awareness' then that should become central to all their learning. School children may be working on a range of curriculum activities and adult learners are likely to be involved in a range of community activities but what is required for all at this stage is for teachers and supporters to provide as many opportunities as possible to practice contingency awareness. This should be done throughout the day, preferably with a range of different resources so the person can learn to generalise his/her understanding in many different situations." (Lacey, 2015, page 45)
... I could remember what I looked like not just when looking in the mirror but also photographs of myself from years before. My memory helped to show me that I knew me:
There is an old myth that goldfish have but a three second memory and, thus, it is not cruel to keep them in a small bowl as the fish see everywhere they look as a new image:
"A lot of people have this stereotype image of a goldfish with a three second memory and that's not the case at all. It is probably accurate to say that many fishes such as minnows, sticklebacks and guppies are capable of the same intellectual feats as rats or mice." (Webster, 2008)(see also Balcombe, 2016)
Even with such a level of cognition is it likely that goldfish are self aware? Are rats self aware? There are some that appear to suggest that they are (see for example, Foote & Crystal, 2007). However, it would seem logical to assume that, if memory is severely curtailed it is going to be more difficult to recognise a self-image as recognition, by definition implies a prior memory:
"After formulizing the representation of each face, the last step is to recognize the identities of these faces. In order to achieve automatic recognition, a face database is required to build. For each person, several images are taken and their features are extracted and stored in the database. Then when an input face image comes in, we perform face detection and feature extraction, and compare its feature to each face class stored in the database." (Chao, 2007)
As the quote states, digital face recognition requires a comparison to a database of stored images. Likewise, self-awareness must require active recall: a memory of things past. It is thought that IEPMLD have poor memory skills:
"The work of Hulme and Mckenzie (1992) suggests that difficulties with memory are experienced, not just by people with Down syndrome
but by others with severe learning difficulties and this can help explain why people with PMLD seem to have huge difficulties in remembering even much repeated activities. Maybe some people with PMLD constantly experience, even much repeated, activities as if for the first time? Maybe even people they meet on a daily basis are strangers to them every time?" (Lacey, 2015, page 44)
This, if the case, might exclude such Learners from self-awareness but what if we work to improve cognition and memory. Can memory be improved? There is a wealth of research material supporting the notion that it can (See, for example, Suzuki, 2015 & 2016). Furthermore, if we turn the concept on its head, and we can demonstrate self-awareness in any Learner then, the Individual's memory must, by definition, be sufficient to support the ability.
I have argued that, for IEPMLD, memory is history and history is memory; that history sessions in educational establishments should not be on events from hundreds of year in the past but, rather, from moments in an individual's experience of the present which, as you read this statement, has just become your past and your history. Thus, let your history sessions become memory sessions ... you are still providing 'history' but history that has relevance to the Individual. For more on this concept and ideas for teaching history to IEPMLD go to the history page on this website.
... I was aware of external stimuli and reacted and I responded to interactions; for example, I reacted appropriately when someone called out my name when I was in a group:
In 2006 Alain Morin wrote:
"It is assumed that to direct attention outward or inward an organism first needs to be awake; if not, the term 'unconsciousness' is used to designate the state in which there is no processing of information, either from the environment or the self. Examples of unconscious
conditions are coma and sleep. When awake and 'conscious', one will process information in the environment and intelligently respond to stimuli. In that state an organism will directly experience perceptions, sensations, thoughts, etc. without being aware that such perceptual
and mental events are taking place. The organism will be totally immersed in experience - an unreflective actor in one’s environment. In this perspective, most - if not all - animals possess 'consciousness'. Humans too arguably spend a large amount of time in a state of
consciousness, interacting with objects and persons, talking, walking, or coherently thinking, without monitoring these activities. I would argue here that Block’s notion of 'phenomenal consciousness' (1995), that is, what it is like to experience mental events such as seeing,
smelling, tasting, or having pains, represents consciousness as defined above. Note that although this definition emphasizes an awareness of external stimuli, and not the self, a minimal consciousness of self is required for the organism to move in, and interact with, the
environment. This has been termed 'first-person perspective' or 'subjective perspectivalness' (Vogeley & Fink, 2003); it involves a diffuse, implicit body awareness allowing articulate spatial self-navigation." (Morin, 2006, page 359)
Morin states that he believes a "minimal consciousness of self is required for the organism to move in, and interact with, the environment" and, thus, in interacting with the environment IEPMLD are demonstrating a 'consciousness of self' although, albeit, a minimal awareness. However, in demonstrating an ability to interact with external objects and events in a purposeful manner the Individual is also demonstrating self-awareness.
There are instances in which an individual can demonstrate self-awareness through reactions to external stimuli:
- While in a group of Learners, the Individual reacts appropriately to hearing her/his own name called out and yet does not respond to the names of others;
- The Individual moves away from unpleasant stimuli (a simple automatic response to pain would NOT count);
- The Individual moves toward pleasurable stimuli (actively seeks more pleasurable experiences unaided and unprompted): See, for example, the section entitled Co-Active Interaction above);
- The individual utilises a piece of equipment in a direct relationship with an appropriate part of the body (For example: Picks up a hat and places it on own head correctly);
- The individual will copy/mirror the movement of others, examples of others, interactions of others with equipment (they are doing this and so I will do this) without assistance and or prompting;
- The individual shows more interest in own image than in images of others;
- Other?
... when I was capable of Introspection:
In patients who have experienced some form of severe brain trauma, it has been noted that, for those who go on to make a good recovery, conscious experience typically returns at the same time as inner speech (Ojemann,1986; Morin, 2009). Furthermore, many individuals (without any trauma) state the they experience a loss of inner speech at the point when they are falling asleep and losing wakeful consciousness (Rusalova, 2005). It is unsurprising therefore that a loss of inner speech (as a result of brain trauma) adversely impacts self-awareness:
"I had lost the ability to converse with others, I had also lost the ability to engage in self-talk. In other words, I did not have the ability to think about the future - to worry, to anticipate or perceive it - at least not with words. Thus for the first 4 or 5 weeks after hospitalization I simply existed." (Moss, 1972, page 10)
"This indicates that the more one engages in introspection to acquire self-information and develop a self-concept, the more one talks to oneself (about oneself), and vice-versa" (Morin, 2009) See also (Briscoe, 2002; Leary, 2004; Morin, 2004; Nelson, 2005)
As, by definition, IEPMLD do not possess speech, can it be also assumed that such Learners do not have inner-speech either? In other words, is self-reflection possible without speech and, therefore, is self-awareness possible without self-reflection?
"So inner speech, and thus language, would play an important role in self-referential activities. Said differently: inner speech would represent an important cognitive process underlying self-awareness. Note that this view does not implicate that there is no self-awareness without language. We can be aware of a pain without having to talk to ourselves about it... as I stated before, self-awareness may be possible without language." (Morin, No date, Language and Self Awareness, Science and Consciousness Review)
However, Helen Keller noted that:
"before my teacher came to me, I did not know that I am. I lived in a world that was a no world... When I learned the meaning of ‘I’ and ‘me’ and found that I was something, I began to think. Then consciousness first existed for me." (cited in Salzen, 1998, page 307)
In addition, Ojemann states:
"As recovery occurs, conscious experience returns as well. It seems to return in parallel with the phenomenon of inner speech. Inner speech may be limited, restricted, concrete, foggy, not normal after these kinds of lesions, but at least conscious experience has come back." (Ojemann,1986, page 161)
If some animals can demonstrate self-awareness and animals do not have inner speech (at least in the sense of an inner form of verbalised output) then it must be theoretical possible for some IEPMLD to be self-aware also (or to develop self-awareness). As Morin states (op.cit.) 'self-awareness may be possible without language'. If an ant can be said to be self-aware (Cammaerts & Cammaerts, 2015) then surely all IEPMLD can be helped to achieve this goal. The Development and demonstration of Learner self-awareness should be a part of any curriculum that purports to benefit IEPMLD. It has been shown that even after extensive damage to the brain an individual can still be self- aware (Philippi et al, 2012).
"The findings in this study confirm that Roger's Self-Awareness is largely preserved. In keeping with previous work ..., the findings show that Roger is a conscious, self-aware, and sentient human being despite the widespread destruction of cortical regions purported to play a critical role in Self-Awareness, namely the insula, anterior cingulate cortex, and medial prefrontal cortex." (Philippi et al, 2012)
MOE ON BRAIN DAMAGE HERE
The following are some strategies that may prove useful in such a scheme (there is no pretence that the list is comprehensive);
- Dressing and undressing;
- Make up, face paints, etc.;
- Washing body parts;
- Drying body parts with towels and with electric driers;
- Brushing and combing hair;
- Cleaning teeth;
- Hand painting and prints;
- Foot, mouth (or other) painting;
- Water Play;
- Masks;
- Music and movement;
- Sensory Stimulation: Provide sessions and experiences (such as sensory massages) that help the Learner concentrate on sensations on their body. Foot-spa. Vibrating cushions. Fans blowing on body...
- Sensory Stories that involve the above;
- Image capture: Cameras, Videos, Webcams;
- Communication development;
- Cognitive development;
- Mirror work (see next section).
47. Mirror Mirror Off the Wall: Magic and Illusion in Special Education
 Mirror Box
Mirror Box
The image (left) is a diagram of a mirror box; a system devised in the 1990s by neuroscientist Vilayanur S. Ramachandran, director of the San Diego Center for Brain and Cognition at the University of California, to provide patients with phantom limb problems with a visual illusion to assist them to overcome pain and other issues. It comprises a sturdy rectangular box which is divided down its centre by a double sided mirror (or a single sided mirror that can be removed and reversed). The box has a removal top or lid which can be placed on either side of the mirror to cover either the left or the rightmost section of the box. In the front panel of the box are two circular access holes into which a patient can place his/her arms and hands. Some individuals who have lost a limb or had a limb amputated nevertheless are still 'aware' of the limb's continuing presence and this may prove to be extremely troubling if this 'phantom limb' (Silas Weir Mitchell, 1871) is 'frozen' in one position and causing them a lot of pain. By placing the remaining hand into the box, covering the other side, and looking down into the box, the patient is fooled into seeing two hands by the mirror. As the patient moves her/his remaining hand, s/he has the illusion of seeing the phantom hand moving. Even though individuals are aware that it is an illusion, their brains are nevertheless fooled by the strength of the visual input that their missing hand is once again moving and, in many cases, their pain is relieved (for further information see Ramachandran & Blakeslee,1998; Guenther, 2016).
Self-Awareness and Self Image
Learners observe themselves using mirrors.
Help with praxis
Learners use mirrors when dressing or undressing; washing, brushing teeth, toileting ...
Rubber Hand
Self-Awareness and Self Image
Learners observe themselves using mirrors.
Help with praxis
Learners use mirrors when dressing or undressing; washing, brushing teeth, toileting ...
- Personal, social and emotional development: managing feelings and behaviour: Learners see how their facial expressions correlate with emotions.
- Expressive arts and design: exploring and using media and materials: Learners can select the materials that they would like to use to create their own self portraits and explore their use.
- Everyone identifies themselves in a mirror during a greeting period
Rubber Hand
48. Sensory Navigation

Sensory Navigation (SN) is a practical tool utilised to promote spatial awareness of location and direction of travel at an almost subconscious level. It can be used in conjunction with Sensory Integration (Ayres, 1970), Sensory Substitution (see, for example, Bubic, Striem-Amit, & Amedi, 2010), and Sensory Augmentation (see, for example, Kerdegari, Kim, & Prescott, 2016) schemes as well as to assist in the practical aspects of any Objects Of Reference venture. As in the cartoon (left), one might consider the white stick employed by many people with issues of visual acuity as a sensory navigation aid which in conjunction with sensory substitution assists an individual to move through an unfamiliar environment with a greater degree of awareness and, thus, safety.
While there are a plethora of high-tech sensory augmentation system in development to aid individuals with disabilities in all aspects of their lives, Sensory Navigation does not have to involve sophisticated electronic equipment. Indeed, the scheme detailed below uses everyday low or no tech items to promote spatial awareness of location and direction of travel. While it necessitates some 'environmental engineering' (see section on Environmental Engineering this page), it does not necessarily involve a significant financial outlay (although when planning for structural changes to premises or new builds it would be a positive step to take sensory navigation into account).
Have you ever walked through a forest and noticed coloured posts regularly spaced along the pathway? By electing to follow one one set of coloured posts, you are guided along one particular walk through the trees, typically back to your starting point. Such coloured posts are a simple example of a sensory navigation system; they assist people to navigate safely through unfamiliar territory without getting lost.
Have you ever driven to an unfamiliar destination for a repeat visit? While, these days, we all make use of satellite navigation to ease the process, it is still likely that you will note any landmarks that you pass on the way: You passed a large Tesco store, you noted the Green Dragon pub on your last visit, and there was a somewhat unusual but rather beautiful gate that you passed.
On stopping and asking for directions (again that is rather rare these days because of satellite navigation) you are likely to be given instructions that include sensory experiences: Take the third right, it's the road just after the Green Dragon Pub; Keep going until you pass the Tesco store on your left and then take the next left at the lights; When you get to the fire station you are almost there ...
Unfortunately, perhaps due to the expense of doing otherwise, buildings tends to be constructed with a uniform design; they tend to be one colour throughout, have similar style doors and windows, have the same flooring from one end to the other. It can prove to be something of a challenge to navigate a building on encountering it for the first time, because of its uniformity, even if you have been given directions to cope with its maze of corridors.
In an article entitled 'Journeys towards Communication' in PMLD Link (2005), Elizabeth Henderson details 'Sensory Journeys' which are virtual sensory story worlds created by staff. However, sensory navigation involves real life 'sensory journeys' along 'sensory pathways' which are environmentally engineered to provide optimum perceptual input for Learners travelling the route:
"The environment can be arranged in ways that optimize the probability that the learner will make requests spontaneously. The learner's propensity to make requests spontaneously may depend on the interaction between conditions imposed by the environment and the learner's state at any particular point in time." (Reichle & Sigafoos, 1991, page 160)
While IEPMLD are unlikely to 'make requests spontaneously' in the manner suggested by Reichle and Sigafoos (1991), nevertheless sensory modification of the environment may help to build Learner awareness of the path taken in moving from point A to point B. Staff play a crucial role in empowering Learners in this process:
"This feeling of safety is also enhanced by making the environment surveyable, recognizable and predictable. People with PMD can better follow and understand what is happening in the environment when support staff adapt to their pace, announce what is going to happen, avoid sudden transitions and give them time to get used to (new) situations. Regularly recurring behavior patterns and routines, familiar support staff, permanent structures and a recognizable organization are things they can hold onto and which make their environment comprehensible and predictable." (Petry et al., 2007c, page 137)
Ellen Trief et al (2013) have show that mobility is very important factor in the mastery of an Objects Of Reference system; those who were ambulant in this study made significantly more gains than those who were not.
"The only variable that yielded a statistically significant difference was mobility. The participants who ambulated independently acquired more knowledge and use of symbols than did those who were nonambulatory or ambulatory with assistance. Children who ambulate have a greater opportunity to explore their environment purposefully than do those who are nonambulatory. Purposeful exposure to environmental stimuli may help this group to understand the symbols more readily than the nonambulatory group."
(Trief, Cascella, & Bruce, 2013, page 189)
Talksense postulated (see OOR page this website) that this might be because staff tend to take control of movement of non-ambulant Learners when it comes to movement between classes; simply pushing them from A to B without any active involvement of the individual in the process.
"Moving from one place to another without changing body position (defined as relocation in this study) was seen more frequently; on average, a person with PIMD relocates nearly eight times a day from a position in or outside their environment. However, most of the participants were wheelchair-bound and had little active input." (van der Putten et al, 2017, page 5)
"How can he gain some sense of his larger environment if he is led everywhere?" (Wyman, 2000, page 130)
Perhaps it would aid understanding if the non-ambulant Learner were an active participant in the journey and the staff took a more supportive role with the expectation that the Learner would eventually direct them: Sensory Navigation systems are a means to support this end.
"Movement is the language of the brain" (Baniel, 2016)
"Movement is life; without movement life is unthinkable." (Moshé Feldenkrais)
"Results showed that the children receiving functionally focused activities achieved the greatest improvements in independence when performing movement activities. For children with PIMD, even a slight improvement in this independence can have enormous impact on participation and control over their own existence." (van der Putten, 2005)
"The objective of this study was to examine the effects of a functionally focused curriculum (MOVE) on the independence when performing movement skills of children with PIMD. The assumption that independence increases significantly in a group of children with PIMD supported
by a functionally focused curriculum is confirmed." (Van der Putten, 2005)
"In both the general population as well as in people with intellectual disability, it is generally acknowledged that being physically active on a regular basis is important because of the positive effects on physical and mental health." (Van der Putten et al, 2017)
"Nothing happens until something moves" is a famous quote by Albert Einstein. The problem is that too often IEPMLD do not move enough! Some are confined to wheelchairs and some are even strapped into a fixed position. Even those that are ambulant may be confined to a single classroom for most of the day and may not move much within that environment. Movement is likely to involve the vestibulatory system and it has been shown that this may lead to increased alertness especially in combination with visual and auditory input:
"The descriptive results revealed high percentages of active-alert behaviour in situations when visual/auditory and vestibular stimulation were combined." (Munde & Vlaskamp, 2015b).
Long periods, strapped into a fixed position is problematic. Equally problematic, is the fundamental lack of Learner control during the limited movement permitted: the Learner is passive and the staff are active when that situation really ought to be turned upon its head such that the staff take a more supportive role with Learners being as active as their ability currently permits. Indeed, in working with communication techniques such as Objects Of Reference, it is not enough to simply present an object and then whisk the Individual off to the location passively and expect OOR to be productive:
"Being whisked everywhere ... often without even being told where he is going, does not help students like Joseph to gain an understanding of his environment." (Wyman, 2000, page 130)
Passive receipt of staff action, practices that presume and promote powerlessness, and assumptions of either Learner inability to comprehend or, conversely, assumptions of Learner understanding ('S/he understands everything I say') should be eliminated from the curriculum:
"For years we just showed him a [picture of a] clock and said that it meant to take a break but to him it meant that it is a clock." (Koski, 2014)
Thus, IEPMLD may be put at greater risk of situational developmental delay as a result of the practices of the establishment. Low expectations and 'doing for' (even 'doing with') can result in a continuation of the 'status quo' in which the Individual Learner makes no progress and may even regress. Just showing a picture of a clock (as in the quote above) is not sufficient, the individual needs to participate actively in the whole process and not simply be a passive recipient of staff care. Yes, IEPMLD tend to have poor mobility and locomotor skills:
"People with intellectual disabilities tend to have low activity and fitness levels which decline over the years when compared with those without a disability. Like individuals with intellectual disabilities, persons with visual impairments also display poor performance in
locomotor skills and have low levels of habitual activity. Individuals who suffer from a combination of severe or profound intellectual and visual disabilities (severe or profound multiple disabilities, SIMD) are particularly at risk in terms of the potential development of deficits in both locomotor skills and daily functioning. Furthermore, the combination of these deficits suggests that persons having SIMD are likely to have lower levels of habitual activity, than persons with ID without visual impairment." (Waninge, 2011)
but that should not mean staff need to take control leaving the Individual to play a passive role. It is therefore important that daily mobility and movement are a part of staff expectations for IEPMLD. Mobility and movement have been associated with a range of positive outcomes for IEPMLD. These include improvements in:
While movement is beneficial for individuals experiencing an intellectual disability, it would appear that there is an inverse relationship between the level of intellectual disability a person experiences and the amount of their physical activity and movement in general (see, for example: Heath & Fenton, 1997; Messent et al, 1998; Robertson et al., 2000; Draheim et al, 2002; Temple & Walkley, 2003; Emerson, 2005; Frey et al, 2005; Temple et al, 2006; Lahtinen et al, 2007; McGuire et al, 2007; Frey et al, 2008; Peterson et al, 2008; Bodde & Dong-Chul, 2009; Hilgenkamp et al, 2012).
"The results showed a low frequency of transfers (in which the body position of the person with PIMD changes), and a low number of motor activities that facilitate the movement of the whole body or parts of the body. During the observation period, a total of 52% of the participants engaged in on average less than one motor activity per weekday. A total of 7% of the participants did not engage in any of those activities
at all during the observation period on weekdays, and nearly half of the participants did not engage in these activities during weekend days observed." (van der Putten et al, 2017, page 5)
Perhaps mobility is a factor in the quicker mastery of an OOR scheme (Trief etal, 2013) because movement equates to exercise and it has been shown that exercise equates to improvements in cognitive functioning in the general population (Tzu-Wei, Lin & Yu-Min, Kuo, 2013; Voss, Nagamatsu, Liu-Ambrose, & Kramer, 2011; Suzuki, 2016; Gourgouvelis, Yielder, & Murphy, 2017). Indeed, it has been shown (Ghaem et al, 1997; Maguire et al 1997, 1998, 2000, 2003, 2006; Gron et al, 2000; Woollett & Macguire, 2011) that the process of learning to navigate can lead directly to improvements in the hippocampus which is involved in memory. However, inter-session movement is typically restricted in all special educational establishments both in terms of time allowed and the physical activity incurred by Learners (staff ensuring rapid transfer between sessions often with minimal Learner participation and cognition). Perhaps movement between sessions should become an educational experience in its own right?
If:
"Traditionally, students considered to have physical disabilities or delayed motor development have received physical therapy, occupational therapy, and/or adapted physical education services to remediate motor skill deficits. Often, students were removed from the natural environments where they needed to use motor skills, and were taught motor skills in isolated therapy rooms or the "special" gym. They learned to climb steps to nowhere, but not the school-bus steps; they learned to put pegs in a board, but not straws in their milk cartons. More recently, we have started to realize that the most important motor skills to teach are those that occur in students' natural environments and routines. Furthermore, natural environments and routines provide ample opportunities to teach a variety of new and meaningful motor skills." (Rainforth, Giangreco, & Dennis, 1989, page 224)
To make such a system easier to envisage it might be helpful to outline an imaginary situation in some detail. Let's start by assuming an individual is leaving an art area after a lesson and is moving to attend a physiotherapy session. The staff have:
While there are a plethora of high-tech sensory augmentation system in development to aid individuals with disabilities in all aspects of their lives, Sensory Navigation does not have to involve sophisticated electronic equipment. Indeed, the scheme detailed below uses everyday low or no tech items to promote spatial awareness of location and direction of travel. While it necessitates some 'environmental engineering' (see section on Environmental Engineering this page), it does not necessarily involve a significant financial outlay (although when planning for structural changes to premises or new builds it would be a positive step to take sensory navigation into account).
Have you ever walked through a forest and noticed coloured posts regularly spaced along the pathway? By electing to follow one one set of coloured posts, you are guided along one particular walk through the trees, typically back to your starting point. Such coloured posts are a simple example of a sensory navigation system; they assist people to navigate safely through unfamiliar territory without getting lost.
Have you ever driven to an unfamiliar destination for a repeat visit? While, these days, we all make use of satellite navigation to ease the process, it is still likely that you will note any landmarks that you pass on the way: You passed a large Tesco store, you noted the Green Dragon pub on your last visit, and there was a somewhat unusual but rather beautiful gate that you passed.
On stopping and asking for directions (again that is rather rare these days because of satellite navigation) you are likely to be given instructions that include sensory experiences: Take the third right, it's the road just after the Green Dragon Pub; Keep going until you pass the Tesco store on your left and then take the next left at the lights; When you get to the fire station you are almost there ...
Unfortunately, perhaps due to the expense of doing otherwise, buildings tends to be constructed with a uniform design; they tend to be one colour throughout, have similar style doors and windows, have the same flooring from one end to the other. It can prove to be something of a challenge to navigate a building on encountering it for the first time, because of its uniformity, even if you have been given directions to cope with its maze of corridors.
In an article entitled 'Journeys towards Communication' in PMLD Link (2005), Elizabeth Henderson details 'Sensory Journeys' which are virtual sensory story worlds created by staff. However, sensory navigation involves real life 'sensory journeys' along 'sensory pathways' which are environmentally engineered to provide optimum perceptual input for Learners travelling the route:
"The environment can be arranged in ways that optimize the probability that the learner will make requests spontaneously. The learner's propensity to make requests spontaneously may depend on the interaction between conditions imposed by the environment and the learner's state at any particular point in time." (Reichle & Sigafoos, 1991, page 160)
While IEPMLD are unlikely to 'make requests spontaneously' in the manner suggested by Reichle and Sigafoos (1991), nevertheless sensory modification of the environment may help to build Learner awareness of the path taken in moving from point A to point B. Staff play a crucial role in empowering Learners in this process:
"This feeling of safety is also enhanced by making the environment surveyable, recognizable and predictable. People with PMD can better follow and understand what is happening in the environment when support staff adapt to their pace, announce what is going to happen, avoid sudden transitions and give them time to get used to (new) situations. Regularly recurring behavior patterns and routines, familiar support staff, permanent structures and a recognizable organization are things they can hold onto and which make their environment comprehensible and predictable." (Petry et al., 2007c, page 137)
Ellen Trief et al (2013) have show that mobility is very important factor in the mastery of an Objects Of Reference system; those who were ambulant in this study made significantly more gains than those who were not.
"The only variable that yielded a statistically significant difference was mobility. The participants who ambulated independently acquired more knowledge and use of symbols than did those who were nonambulatory or ambulatory with assistance. Children who ambulate have a greater opportunity to explore their environment purposefully than do those who are nonambulatory. Purposeful exposure to environmental stimuli may help this group to understand the symbols more readily than the nonambulatory group."
(Trief, Cascella, & Bruce, 2013, page 189)
Talksense postulated (see OOR page this website) that this might be because staff tend to take control of movement of non-ambulant Learners when it comes to movement between classes; simply pushing them from A to B without any active involvement of the individual in the process.
"Moving from one place to another without changing body position (defined as relocation in this study) was seen more frequently; on average, a person with PIMD relocates nearly eight times a day from a position in or outside their environment. However, most of the participants were wheelchair-bound and had little active input." (van der Putten et al, 2017, page 5)
"How can he gain some sense of his larger environment if he is led everywhere?" (Wyman, 2000, page 130)
Perhaps it would aid understanding if the non-ambulant Learner were an active participant in the journey and the staff took a more supportive role with the expectation that the Learner would eventually direct them: Sensory Navigation systems are a means to support this end.
"Movement is the language of the brain" (Baniel, 2016)
"Movement is life; without movement life is unthinkable." (Moshé Feldenkrais)
"Results showed that the children receiving functionally focused activities achieved the greatest improvements in independence when performing movement activities. For children with PIMD, even a slight improvement in this independence can have enormous impact on participation and control over their own existence." (van der Putten, 2005)
"The objective of this study was to examine the effects of a functionally focused curriculum (MOVE) on the independence when performing movement skills of children with PIMD. The assumption that independence increases significantly in a group of children with PIMD supported
by a functionally focused curriculum is confirmed." (Van der Putten, 2005)
"In both the general population as well as in people with intellectual disability, it is generally acknowledged that being physically active on a regular basis is important because of the positive effects on physical and mental health." (Van der Putten et al, 2017)
"Nothing happens until something moves" is a famous quote by Albert Einstein. The problem is that too often IEPMLD do not move enough! Some are confined to wheelchairs and some are even strapped into a fixed position. Even those that are ambulant may be confined to a single classroom for most of the day and may not move much within that environment. Movement is likely to involve the vestibulatory system and it has been shown that this may lead to increased alertness especially in combination with visual and auditory input:
"The descriptive results revealed high percentages of active-alert behaviour in situations when visual/auditory and vestibular stimulation were combined." (Munde & Vlaskamp, 2015b).
Long periods, strapped into a fixed position is problematic. Equally problematic, is the fundamental lack of Learner control during the limited movement permitted: the Learner is passive and the staff are active when that situation really ought to be turned upon its head such that the staff take a more supportive role with Learners being as active as their ability currently permits. Indeed, in working with communication techniques such as Objects Of Reference, it is not enough to simply present an object and then whisk the Individual off to the location passively and expect OOR to be productive:
"Being whisked everywhere ... often without even being told where he is going, does not help students like Joseph to gain an understanding of his environment." (Wyman, 2000, page 130)
Passive receipt of staff action, practices that presume and promote powerlessness, and assumptions of either Learner inability to comprehend or, conversely, assumptions of Learner understanding ('S/he understands everything I say') should be eliminated from the curriculum:
"For years we just showed him a [picture of a] clock and said that it meant to take a break but to him it meant that it is a clock." (Koski, 2014)
Thus, IEPMLD may be put at greater risk of situational developmental delay as a result of the practices of the establishment. Low expectations and 'doing for' (even 'doing with') can result in a continuation of the 'status quo' in which the Individual Learner makes no progress and may even regress. Just showing a picture of a clock (as in the quote above) is not sufficient, the individual needs to participate actively in the whole process and not simply be a passive recipient of staff care. Yes, IEPMLD tend to have poor mobility and locomotor skills:
"People with intellectual disabilities tend to have low activity and fitness levels which decline over the years when compared with those without a disability. Like individuals with intellectual disabilities, persons with visual impairments also display poor performance in
locomotor skills and have low levels of habitual activity. Individuals who suffer from a combination of severe or profound intellectual and visual disabilities (severe or profound multiple disabilities, SIMD) are particularly at risk in terms of the potential development of deficits in both locomotor skills and daily functioning. Furthermore, the combination of these deficits suggests that persons having SIMD are likely to have lower levels of habitual activity, than persons with ID without visual impairment." (Waninge, 2011)
but that should not mean staff need to take control leaving the Individual to play a passive role. It is therefore important that daily mobility and movement are a part of staff expectations for IEPMLD. Mobility and movement have been associated with a range of positive outcomes for IEPMLD. These include improvements in:
- autonomy (Schellingerhout, Smitsman, & Cox, 2005; Reimer & Siemonsma-Boom, 2013);
- behaviour (Jones et al, 2007);
- cognition (Trief et al, 2013);
- health (CDC, 2003; Hamiliton et al. 2007; Dowling et al, 2012);
- independence (Van der Putten et al., 2005);
- participation (Van der Putten et al., 2005);
- self control (Schellingerhout, Smitsman, & Cox, 2005; Reimer & Siemonsma-Boom, 2013);
- understanding of their environment (Schellingerhout, Smitsman, & Cox, 2005; Reimer & Siemonsma-Boom, 2013).
While movement is beneficial for individuals experiencing an intellectual disability, it would appear that there is an inverse relationship between the level of intellectual disability a person experiences and the amount of their physical activity and movement in general (see, for example: Heath & Fenton, 1997; Messent et al, 1998; Robertson et al., 2000; Draheim et al, 2002; Temple & Walkley, 2003; Emerson, 2005; Frey et al, 2005; Temple et al, 2006; Lahtinen et al, 2007; McGuire et al, 2007; Frey et al, 2008; Peterson et al, 2008; Bodde & Dong-Chul, 2009; Hilgenkamp et al, 2012).
"The results showed a low frequency of transfers (in which the body position of the person with PIMD changes), and a low number of motor activities that facilitate the movement of the whole body or parts of the body. During the observation period, a total of 52% of the participants engaged in on average less than one motor activity per weekday. A total of 7% of the participants did not engage in any of those activities
at all during the observation period on weekdays, and nearly half of the participants did not engage in these activities during weekend days observed." (van der Putten et al, 2017, page 5)
Perhaps mobility is a factor in the quicker mastery of an OOR scheme (Trief etal, 2013) because movement equates to exercise and it has been shown that exercise equates to improvements in cognitive functioning in the general population (Tzu-Wei, Lin & Yu-Min, Kuo, 2013; Voss, Nagamatsu, Liu-Ambrose, & Kramer, 2011; Suzuki, 2016; Gourgouvelis, Yielder, & Murphy, 2017). Indeed, it has been shown (Ghaem et al, 1997; Maguire et al 1997, 1998, 2000, 2003, 2006; Gron et al, 2000; Woollett & Macguire, 2011) that the process of learning to navigate can lead directly to improvements in the hippocampus which is involved in memory. However, inter-session movement is typically restricted in all special educational establishments both in terms of time allowed and the physical activity incurred by Learners (staff ensuring rapid transfer between sessions often with minimal Learner participation and cognition). Perhaps movement between sessions should become an educational experience in its own right?
If:
- Learners were assisted to comprehend their destination because they were given multi-sensory input including an Object Of Reference before making the journey;
- the corridors each provided a unique sensory code which assisted directional awareness;
- the coding in the corridors changed in relation to position a person's location;
- there were unique sensory experiences (sensory stations) at different positions throughout the building;
- staff understood that for some Learners movement (with attention) between sessions was an educational experience with as much value as any in session instruction;
- staff assisted each Learner to experience the sights, sounds, smells, and sensations of every journey to and from sessions;
- staff enabled each Learner, were possible, to walk between sessions / move their body between sessions / be aware of their environment between sessions;
- extra time was allowed for all the above.
"Traditionally, students considered to have physical disabilities or delayed motor development have received physical therapy, occupational therapy, and/or adapted physical education services to remediate motor skill deficits. Often, students were removed from the natural environments where they needed to use motor skills, and were taught motor skills in isolated therapy rooms or the "special" gym. They learned to climb steps to nowhere, but not the school-bus steps; they learned to put pegs in a board, but not straws in their milk cartons. More recently, we have started to realize that the most important motor skills to teach are those that occur in students' natural environments and routines. Furthermore, natural environments and routines provide ample opportunities to teach a variety of new and meaningful motor skills." (Rainforth, Giangreco, & Dennis, 1989, page 224)
To make such a system easier to envisage it might be helpful to outline an imaginary situation in some detail. Let's start by assuming an individual is leaving an art area after a lesson and is moving to attend a physiotherapy session. The staff have:
- played a short piece of music which signifies that a session has terminated and movement to another area must begin;
- presented the Learner with the OOR for physiotherapy;
- signed, in a manner appropriate to the needs of the individual concerned, the word 'physiotherapy';
- spoken the word 'physiotherapy';
- if possible, encouraged the Learner to get out of his/her wheelchair and walk with them to the next session using whatever aid is necessary;
- encouraged and functionally supported Learner (upper body) movement (even from seated position in a wheelchair);
- encouraged active attention to and engaged exploration of the journey environment,
The art room is located on the blue corridor. The walls are bricks and so painting the entire corridor blue was not a reasonable option. Instead a number of hardboard circles appear at regular intervals all along the corridor. The circles are all mainly blue in colour but as a person moves left down the corridor towards the green corridor the blue increasingly merges with green. Alternatively, if the Learner were to turn right towards the yellow corridor, the blue increasing merges with yellow. Only the blue corridor uses circles; the yellow corridor utilizes triangles and the green has squares. While it is easy to tell where you are going if you can see the colours it is not if you happen to be colour blind or have problems of visual acuity. However, the system designer thought of this! Each colour has also a unique feel; blue happens to have wavy lines (applied with a glue gun at time of construction and then over-sprayed in blue) to represent waves in water. Yellow has a sandy surface (sand sprinkled onto glue and over-sprayed in yellow) and green utilizes hessian cloth. Only the white corridor is completely smooth in texture. The circles are positioned on the wall such that an individual using a wheelchair can easily interact with them; they can be explored if the person can reach out and touch but not removed.
On the journey, the learner passes a number of unique 'sensory stations'. A 'Sensory Station' is a sensory experience located in in a specific location within (or without) a building. This particular experience (or, more likely, combination of experiences) only occurs at this one position and is not replicated anywhere else. Sensory stations are environmentally engineered sensory experiences that provide afferent cues to location. They assist in:
On the journey, the learner passes a number of unique 'sensory stations'. A 'Sensory Station' is a sensory experience located in in a specific location within (or without) a building. This particular experience (or, more likely, combination of experiences) only occurs at this one position and is not replicated anywhere else. Sensory stations are environmentally engineered sensory experiences that provide afferent cues to location. They assist in:
- aiding understanding of location;
- easing stress by increasing familiarity;
- improving the experience of what might otherwise be a dull journey!
- a visual cue such as a large indoor potted plant. There is only one such a type of potted plant in the building and it never moves from this location;
- a olfactory cue perhaps provided by the plant itself or from some other 'engineered' source;
- an auditory cue. Wind chimes can be positioned outdoors at one exit for example. Wall sensors can detect passers-by and produce a particular sound effect ...
- A tactile sensation: perhaps the floor at this location has a rug over which all learners must pass. Note (in the UK) how a pavement's surface changes to blister paving adjacent to road crossing points;
- A taste cue: Perhaps a staff member can supply a very small amount of a favourite sweet (one 'Smartie' for example) from a concealed but colourful pot at the Sensory Station. Thus, every time the Individual passes by, s/he might take more interest in the location. The pot itself can actually be empty with staff really supplying the sweet from their pocket but pretending it comes from the pot.
- motion - some people may not notice an item unless it moves some of the time; motion makes it memorable, perhaps more motion makes it more memorable.

|
|
|
Thus, on leaving the art room the Learner hears the same pieces of music that ends every session. S/he has begun to associate it with movement to another place. The Learner has been presented with an Object Of Reference; the OOR is for physio. S/he only experiences this OOR when the journey is to the physiotherapy department. S/he has a walking frame and is encouraged to use it to travel to Physio as independently as possible. As s/he cannot manage to carry the OOR and utilise the walking frame, Staff transport the OOR and occasionally show it to the Learner to remind him/her of the destination. Staff point out the colour changes on the walls as they move towards the physiotherapy department. Staff also ensure that the Learner stops at every Sensory Station they pass on route and spends a little time with them experiencing it. On reaching the physiotherapy department, staff point out the door marker (d-oor-way) is the same as the OOR for physio that has accompanied the Learner throughout the journey; literally taking the door marker from its housing and matching the two side by side such that the Learner has a clear view and/or can reach out (if able) and explore the objects. On entering the physio department the same piece of music is playing every time; it is not loud and it does not last too long but it is noticeable.
It has been shown (Krech et al, 1960; Rosenzweig et al, 1962, 1972; Diamond et al, 1964, 1966, 1972; Francis et al, 2002) that 'enriched' environments have positive affects on brain plasticity and function. Furthermore, it has also been demonstrated that:
Thus, in enriching the environment with multi-sensory experiences in a manner such as the one outlined above, and in maximising moving between sessions, we are providing maximum scope for assisting the cognitive growth of IEPMLD. Why would we NOT want to provide an environment which gives the best chance of cognitive growth? Indeed, we would suggest it is essential. Navigation through such an environment is beneficial for IEPMLD and should happen at least twice a day. It can happen:
But the post 16 Learners in my school stay in the same classroom and do not swap rooms when changing subject.
You should consider changing this if at all possible. However, if it is not possible for whatever reason then build movement into your session plan! That is go somewhere else in the building consistently at some suitable point during the morning and or the afternoon. If the morning is already broken by a trip to a different location for break and for lunch then this may be sufficient. However, allow greater time for the process and ensure that the Learners are in control as 'the goal is control'! Furthermore, you may want to build Learner movement (exercise in whatever form) into your session plan for each learning session especially near to the start and make a change of position into the classroom routine common practice:
"Within this study, however, it was assumed that a change of position while remaining in the same place, even without active input, gives a person with PIMD an opportunity to experience the environment differently. A change of position may evoke a motor response in the person with PIMD. Furthermore, changing position such that an individual with PIMD sits next to another individual gives them the opportunity to make contact." (van der Putten et al, 2017, page 5)
But we stay in the same classroom for break.
Arrange to swap with another group in another classroom such that both groups are moving somewhere new.
The focus at my establishment is on the sessions themselves and not on the inter-session periods. Indeed,we have been told to ensure that the Learners get to the next session as quickly as possible. Is that wrong?
It might be the right thing to do if you see the Learners as passive during these times and treat them as such. However, research (see studies quoted above) suggests that exercise, active Learner involvement and control, and an enriched environment are positive factors aiding cognitive development. Thus, movement between sessions can be a fertile area for development and should not be overlooked and certainly not neglected for its potential; indeed, as discussed above, inter-session 'periods' can be structured to maximise this potential. Learning can take place anywhere, it is not confined to a teacher-led classroom. With this in mind, it may be worthwhile looking again at movement and allowing the time and making the provision to optimise the provision.
Oh come on! You are not really suggesting that John can direct staff as to where to go to get to his next session, are you? We have a real job to get him to respond to intense stimulation in the classroom!
Actually, that is what we are suggesting but not in as naive a manner as your question would imply! It is not expected that your John will suddenly become more alert during inter-session travel and suddenly acquire the power of speech and say, "My dear, do you know you are going in the wrong direction for physiotherapy?"! However, we are suggesting that staff make every effort to involve John in the process of moving between points A and B by:
Finally in this section:
"If the child cannot explore the environment for himself it is important that different tactile stimuli are brought to the child." (Clark, 1991)
While not wishing to disagree with Sally Clark on this matter, perhaps enabling the Individual to explore the environment for her/himself is just as important or, at the very least, ensuring that movement through the environment is as stimulating and as meaningful as possible and not just a passive journey from A to B.
"The necessity arises when a child cannot partake in the multisensory aspects of the environment in meaningful ways. For some children the natural environment seems chaotic and unpredictable. When such a child is left without appropriate environmental modifications, the child's ability to engage with the external environment may be seriously compromised. The child will require an individual environment which is individually tailored to meet his or her particular needs." (Pagliano, 2001, page 6)
'Tailoring the environment' equates to 'environmental engineering'. Sensory Navigation utilises environmental engineering to tailor the environment.
It has been shown (Krech et al, 1960; Rosenzweig et al, 1962, 1972; Diamond et al, 1964, 1966, 1972; Francis et al, 2002) that 'enriched' environments have positive affects on brain plasticity and function. Furthermore, it has also been demonstrated that:
- exercise can double the production of new neurons in the hippocampus in the brain (Suzuki, 2015);
- long-term potentiation (LTP) which is a long lasting change in the electrical response between groups of neurons can be enhanced;
- olfactory stimulation can also result in the production of new neurons (Rochefort at al, 2002);
Thus, in enriching the environment with multi-sensory experiences in a manner such as the one outlined above, and in maximising moving between sessions, we are providing maximum scope for assisting the cognitive growth of IEPMLD. Why would we NOT want to provide an environment which gives the best chance of cognitive growth? Indeed, we would suggest it is essential. Navigation through such an environment is beneficial for IEPMLD and should happen at least twice a day. It can happen:
- when Learners arrive at school/college such that staff don't just take over and whisk them off to their classroom but rather encourage and support them to make their own way there;
- when Learners leave school/college at the end of the day such that staff don't just take over and whisk them off to their waiting transport but rather encourage and support them to make their own way there;
- when Learners leave school/college to go out shopping or to the park: staff can encourage the Learner to find (or direct) his/her way to the exit;
- between sessions as described above;
- at break and lunch times. Don't take break in the same classroom: move!
But the post 16 Learners in my school stay in the same classroom and do not swap rooms when changing subject.
You should consider changing this if at all possible. However, if it is not possible for whatever reason then build movement into your session plan! That is go somewhere else in the building consistently at some suitable point during the morning and or the afternoon. If the morning is already broken by a trip to a different location for break and for lunch then this may be sufficient. However, allow greater time for the process and ensure that the Learners are in control as 'the goal is control'! Furthermore, you may want to build Learner movement (exercise in whatever form) into your session plan for each learning session especially near to the start and make a change of position into the classroom routine common practice:
"Within this study, however, it was assumed that a change of position while remaining in the same place, even without active input, gives a person with PIMD an opportunity to experience the environment differently. A change of position may evoke a motor response in the person with PIMD. Furthermore, changing position such that an individual with PIMD sits next to another individual gives them the opportunity to make contact." (van der Putten et al, 2017, page 5)
But we stay in the same classroom for break.
Arrange to swap with another group in another classroom such that both groups are moving somewhere new.
The focus at my establishment is on the sessions themselves and not on the inter-session periods. Indeed,we have been told to ensure that the Learners get to the next session as quickly as possible. Is that wrong?
It might be the right thing to do if you see the Learners as passive during these times and treat them as such. However, research (see studies quoted above) suggests that exercise, active Learner involvement and control, and an enriched environment are positive factors aiding cognitive development. Thus, movement between sessions can be a fertile area for development and should not be overlooked and certainly not neglected for its potential; indeed, as discussed above, inter-session 'periods' can be structured to maximise this potential. Learning can take place anywhere, it is not confined to a teacher-led classroom. With this in mind, it may be worthwhile looking again at movement and allowing the time and making the provision to optimise the provision.
Oh come on! You are not really suggesting that John can direct staff as to where to go to get to his next session, are you? We have a real job to get him to respond to intense stimulation in the classroom!
Actually, that is what we are suggesting but not in as naive a manner as your question would imply! It is not expected that your John will suddenly become more alert during inter-session travel and suddenly acquire the power of speech and say, "My dear, do you know you are going in the wrong direction for physiotherapy?"! However, we are suggesting that staff make every effort to involve John in the process of moving between points A and B by:
- use of an Object Of Reference;
- use of sensory cues;
- use of sensory pathways;
- use of sensory stations;
- taking time to involve John in the sensory 'experience' of all of the above and not just whizzing to the next session as quickly and as passively as possible;
- communicating with John throughout the journey (even making use of simple technology such as BIGmacks);
- making the journey a 'responsive environment' (Ware 2003);
- allowing John to take as much control of the process as is possible;
- not assuming that John isn't aware of his environment on the journey but aiming to assist John's awareness at every step;
- maintaining a really positive staff attitude to the process even though John may not appear to be responding.
Finally in this section:
"If the child cannot explore the environment for himself it is important that different tactile stimuli are brought to the child." (Clark, 1991)
While not wishing to disagree with Sally Clark on this matter, perhaps enabling the Individual to explore the environment for her/himself is just as important or, at the very least, ensuring that movement through the environment is as stimulating and as meaningful as possible and not just a passive journey from A to B.
"The necessity arises when a child cannot partake in the multisensory aspects of the environment in meaningful ways. For some children the natural environment seems chaotic and unpredictable. When such a child is left without appropriate environmental modifications, the child's ability to engage with the external environment may be seriously compromised. The child will require an individual environment which is individually tailored to meet his or her particular needs." (Pagliano, 2001, page 6)
'Tailoring the environment' equates to 'environmental engineering'. Sensory Navigation utilises environmental engineering to tailor the environment.
49. Sensory Selections

'Sensory Selection' is a methodology for enhancing the provision of a more meaningful choice at any point during the day when a decision has to be made. Typically, choices are presented visually with sensory feedback being provided via characteristics of the the items in the array that are perceived by the Learner. For example, a Learner may be shown the two drinks currently available as a late night drink (coffee or hot chocolate) as a choice in their different containers as in the illustration left. The Learner is then asked to indicate a single preferred option from the two items in the array by using a methodology specific to their abilities (for example, reaching out or eye pointing). While this is not poor practice, there are a number of concerns about such an approach that should be considered:
It is important therefore that Significant Others demonstrate Learner comprehension of the components of the array if it is to be claimed that a 'choice' has been made for, if there is no Learner connection (comprehension) there is no selection!
For those experiencing the most significant learning difficulties (and, indeed, perhaps for others too), teaching and assessing Learner comprehension is a vital step in this process. The following ideas can be used to assist with this:
Sensory support for the Learner (Sensory Selections) involves 'environmental engineering'. That is the container is 'engineered' (altered) by adding an additional sensory surface to provide extra feedback to the Learner to assist with the identification of its contents. While it is preferable the sensory surface relates in some way to the contents, it is not essential: over time the Learner will come to relate the sensory feedback to that particular event (drink) providing the process is consistent over time. For example, using a template and spray mount adhesive, a circle of glue can be applied to the surface of the container at one or more appropriate points. Some of the contents of the container can then be sprinkled over the glue (if the contents are solid particles). When dry, this can be sprayed with a clear lacquer to protect it. The container now provides extra sensory feedback to the Learner when s/he interacts with it. The shape of the sensory surface can be varied for other choices to provide further sensory feedback for the Learner. Another idea would be to write the contents of the container on the container in this manner so as to provide additional sensory surface support for sensory selections even though the Learner is not actually reading it.
"You will need to be imaginative when helping someone to explore alternative options. Use all of the person's senses, if appropriate."
(Jackson and Jackson, 1999, page 80)
Taking this idea one stage further, it may be appropriate to attach a Sensory Object to the front of the container by Velcro (or some other means) such that the object is presented as the sensory surface to be explored at the same time as the container. The object can be detached and given to the Learner to explore further after making the choice and prior to the presentation of a (in this instance) particular drink such that the object becomes associated with the drink in the Learner's mind.
- It should not be claimed that the Learner has chosen a specific drink nor that s/he understands (in this case) coffee and hot chocolate;
- The Learner may be selecting on the basis of some characteristic of the containers and not on the drinks they contain. If the Learner likes both coffee and hot chocolate there is no way of ascertaining this;
- Learners with issues of visual acuity (and, indeed, those without also) may be selecting the item that reflects the light more readily in the environment at that time;
- The Learner may be selecting on positional preference (always chooses item on right, for example);
- The containers must remain the same throughout the entire period of selection. As product brands tend to change their packaging over relatively short periods of time, it is important that staff keep the initial packaging used and only use it for presentations in choices (not to make the actual drink) and make the drink from another package. Thus, the presentation material remains consistent throughout;
- As both drinks are equally valid choices for the Learner (S/he gets a drink s/he likes every time) it does not matter which is selected. While it appears the Learner is making a choice, in reality s/he may be just fly-swatting (reacting to a stimuli with a conditioned response without any real cognitive engagement with the objects).
It is important therefore that Significant Others demonstrate Learner comprehension of the components of the array if it is to be claimed that a 'choice' has been made for, if there is no Learner connection (comprehension) there is no selection!
For those experiencing the most significant learning difficulties (and, indeed, perhaps for others too), teaching and assessing Learner comprehension is a vital step in this process. The following ideas can be used to assist with this:
- Supplement the sensory feedback from each option as necessary (Sensory Selections);
- Work on one (assumed preferred BEST) item in the array to establish a link between item and event (drink). The Learner should always be presented with the same package (it must NOT change). As the packaging should remain consistent through out all choices for the event (in this case, a specific drink) over time, a package should be obtained that is NOT used for real (to make the drink) but only used for show (to show the Learner as an item in the array). Another package can be purchased to use for making the drink (or for refilling the original container once empty);
- Involve the Learner in all aspects of making the drink from the container such that s/he has an opportunity to understand that the contents are a vital part of the drink (the drink comes from the container and therefore choosing the container is choosing the drink);
Sensory support for the Learner (Sensory Selections) involves 'environmental engineering'. That is the container is 'engineered' (altered) by adding an additional sensory surface to provide extra feedback to the Learner to assist with the identification of its contents. While it is preferable the sensory surface relates in some way to the contents, it is not essential: over time the Learner will come to relate the sensory feedback to that particular event (drink) providing the process is consistent over time. For example, using a template and spray mount adhesive, a circle of glue can be applied to the surface of the container at one or more appropriate points. Some of the contents of the container can then be sprinkled over the glue (if the contents are solid particles). When dry, this can be sprayed with a clear lacquer to protect it. The container now provides extra sensory feedback to the Learner when s/he interacts with it. The shape of the sensory surface can be varied for other choices to provide further sensory feedback for the Learner. Another idea would be to write the contents of the container on the container in this manner so as to provide additional sensory surface support for sensory selections even though the Learner is not actually reading it.
"You will need to be imaginative when helping someone to explore alternative options. Use all of the person's senses, if appropriate."
(Jackson and Jackson, 1999, page 80)
Taking this idea one stage further, it may be appropriate to attach a Sensory Object to the front of the container by Velcro (or some other means) such that the object is presented as the sensory surface to be explored at the same time as the container. The object can be detached and given to the Learner to explore further after making the choice and prior to the presentation of a (in this instance) particular drink such that the object becomes associated with the drink in the Learner's mind.

|

|
In the first image, the choice is provided using just the two drinks cartons; there is not a lot of difference. For some Learners, this might provide sufficient sensory discrimination available but, for others, the second option (the addition of a plastic fruit Sensory Object for each drink) may give a better means of obtaining (or, at least, teaching) an informed choice.
50. Neuroplasticity and Neurogenesis in the classroom
The three pound piece of soft and, surprisingly, quite vulnerable matter inside your head (the brain) is the most complex living thing known to man:
"But the brain is much more complicated than any of these devices, a fact scientists confirm almost daily with each new discovery. The extent of the brain’s capabilities is unknown, but it is the most complex living structure known in the universe." (The Society for Neuroscience, 2002)
It has been estimated that there are approximately 100 billion neurons in the human brain (Brownson, 2012)(although figures for this estimation vary somewhat: see Braitenberg, 2001; Bartheld et al. 2016) and each can make up to fifteen thousand connections with its neighbours (Brotherson, 2005) providing some some 100 quadrillion (10 to the power 15) interconnections (Tang et al., 2001). With such complexity is it any wonder that there is potential for things to go wrong?
The brains of IEPMLD are, by definition, functionally different to their more cognitively able peers. Examinations and scans of the brains of Individuals Experiencing PMLD have shown that there may be:
"Possibly the most obvious outcome of this study is the demonstration of the frequency of structural abnormality in the brains of patients with severe mental retardation, and this is in accord with previous experience." (Crome, 1960, page 903)
With such 'structural abnormality' resulting in profound learning difficulties perhaps we should throw in the towel and simply provide palliative care especially when we factor in the likelihood of additional sensory impairments. However, we already know that cerebral issues, typically confounded with problematic sensory factors, are attributes of the IEPMLD condition and, yet, educational establishments the world over are still able to show mental and physical progress. No person who is breathing and awake is incapable of making progress even if only small in comparison to an age equivalent peer: if you question that then this webpage is not for you.
For many years it was believed that, post the period of childhood, the human brain reached maturity and became hard-wired with no further development. Indeed, it was thought that when brain cells died for whatever reason they would not be replaced leading to cognitive decline as a person grew older and older. It was also believed that specific areas of the brain assumed rigid functions and if these areas were damaged in an accident or by a stroke then they were lost forever and recovery would be minimal.
"Up to the late 1990s neuroscience accepted as fact that the brain stops growing new brain cells by adulthood. It was believed that after this cessation, it was just one slow, unavoidable slide into decrepitude as brain cells die off, never to be replaced, gradually at first, but then faster and faster as you age." (Cortright, 2015, page 11)
"Just 50 years ago, the idea that the adult brain can change in any way was heretical. Researchers accepted that the immature brain is malleable but also believed that it gradually hardens, like clay poured into a mold, into a permanently fixed structure by the time childhood had ended. It was also believed that we are born with all the brain cells we will ever have, that the brain is incapable of regenerating itself, and, therefore, that any damage or injuries it sustains cannot be fixed" (Costandi, 2016, page 2)
It is now known a new experience, repeatedly encountered, can have a significant effect which is contrary to the previously held belief that brain structure does not alter except for deterioration with advancing age:
"Our results contradict the traditionally held view that the anatomical structure of the adult human brain does not alter, except for changes in morphology caused by ageing or pathological conditions. Our findings indicate that learning-induced cortical plasticity is also reflected at a structural level." (Draganski et al, 2004)
Furthermore, it has been demonstrated that, at least, some parts of the brain are capable of the generation of new neurons throughout their life:
"During neural development, the nervous system is created from cells that have the potential to proliferate, to reproduce themselves, and to differentiate into the appropriate neuronal and glial phenotypes. Although the adult brain has classically been thought of as a structure
with very limited regenerative capacity, these neural stem cells have recently been shown to exist in the adult central nervous system (CNS) as well. It is now evident that the adult brain is efficiently and continuously generating specific neuronal populations." (Kuhn et al, 2001)
"It was long thought that neuronal production ended soon after birth, fueling a view of the adult brain as a finalized structure (as far as new neurons are concerned), with further plasticity concentrated on synapses. It took some time to realize and demonstrate that neuronal incorporation can, to different degrees, continue during the entire life of an animal." (Cecchi et al, 2001)
"The brain keeps growing new brain cells your entire life. This process is how the brain upgrades itself and enhances your quality of life." (Cortright, 2015, page 11)
The brain is 'plastic':
"In the last few decades, this fixed idea of the brain has been discarded. Instead, we talk about the brain being 'plastic', meaning that the brain changes its own wiring, perhaps almost continuously. Like a piece of silly putty, the brain is molded and reshaped by the forces of life
acting on it. Our wiring grows and develops depending on what we experience - even before birth. As we interact with the world, the world becomes internalized, or mapped, in our brain. The extensive plasticity of the brain continues throughout life." (Zull, 2004, page 69)
"The adult brain, in short, retains much of the plasticity of the developing brain, including the power to repair damaged regions, to grow new neurons, to rezone regions that performed one task and have them assume a new task, to change the circuitry that weaves neurons into networks that allow us to remember, feel, suffer, think, imagine and dream." (Begley, 2009, page 7)
While plasticity is good news it is also, at one and the same time, bad news; if it is plastic it can also deteriorate:
"Connections among neurons that have a high probability of displaying temporally correlated activity tend to become consolidated while connections among neurons that have a lower probability of being activated in a correlated manner tend to become removed." (Singer, 2008, page 100)
"It may come as a surprise to learn that depression and neurodegeneration can be bedfellows – but we now know that severely depressed patients can lose brain cells" (Morris & Fillenz, 2003, page 50)
However, let's be positive and look on the bright side; plasticity suggests the possibility, at least, with the right approaches, Individuals Experiencing PMLD can be helped to progress perhaps to a point at which they could no longer be classified as 'profound' any longer. The question becomes 'what are the right approaches'? What are the recommended practices both within and without the classroom that will assist in brain development? This is too big an area to answer in a section on this webpage and therefore it has been addressed on its own page HERE (in development, not yet accessible). The promotion of neurogenesis and positive neuroplasticity is, thus, a constructive approach in all phases of education and should be addressed wherever and whenever possible.
There is a commonly held misconception, it is false premise that, generally, people only use ten percent of their brain function:
"The 10 percent of the brain myth is a widely perpetuated urban legend that most or all humans only use 10 percent (or some other small percentage) of their brains. It has been misattributed to many people, including Albert Einstein. By extrapolation, it is suggested that a person may harness this unused potential and increase intelligence." (Wikipedia, 2017)
Of course, this assumes that the original form of this statement referred to ten percent by area: in other words, that 90% of the brain is sitting idle while the remaining ten per cent is doing all the work. This would be akin to having a ten room building but only having access to one room with nine rooms remaining locked and inaccessible. This view of the brain is wrong; brain scans have long shown that all rooms in the building are being utilised when we are thinking although, depending upon what we are thinking about, some rooms may be called into action more than others. However, what if the originating statement referred to ten per cent by potential rather than then per cent by area? In our ten room buildings, all the rooms would be being utilised but being utilised rather poorly: that is, if the rooms were re-organised, there would be potential for a 90% efficiency gain over the present methodology. It is our contention that, the original source of the statement concerned 'brain potential' (as opposed to 'brain area') and, thus, claims of it being a 'brain myth' and 'urban legend' are not entirely true. Indeed, it may be that the ten per cent figure is too high; we might only currently be using 1% of our brain's potential! What evidence is there to support such an outrageous claim? We are capable of improvements in:
Evidence that the brain is capable of tremendous feats also comes from another source; that of the autistic savant (Hermelin et al., 1987; Treffert, 1988, 1989; Mottron et al.,1998; Hermelin & O’Connor, 1991; Miller,1999; Heaton, & Wallace, 2004; Tammat, 2007, 2009; Howlin et al., 2009). In the savant, the brain is capable of extraordinary feats in one or more areas of human endeavour (Drawing, mathematics, memory. music, ...) while, at one and the same time, being challenged in virtually all other areas, as depicted in the 1988 film Rain Man (Morrow and Bass, 1988) loosely based on the character of Kim Peek. It is hypothesised that we all possess such latent talent within our brain but that it is suppressed by the natural workings of all the other areas and, therefore, is not normally exhibited (Snyder & Mitchell, 1999; Snyder et al, 2003, 2004; Snyder, 2009). On occasions, following accidental trauma to the brain, such potential has been 'released' in people who, before the trauma, had typically average abilities (LaFay 1987; Treffert 1988; Flaherty, 2015).
"I argue that savant skills are latent in us all. My hypothesis is that savants have privileged access to lower level, less-processed information, before it is packaged into holistic concepts and meaningful labels. Owing to a failure in top-down inhibition, they can tap into information that exists in all of our brains, but is normally beyond conscious awareness. This suggests why savant skills might arise spontaneously in otherwise normal people" (Snyder, 2009, page 1399)
Given the potential of the human brain there must surely be at least some scope for the amelioration of cognitive condition in those experiencing profound learning difficulties.
OK, so what if we accept that improvements in the the potential of the brain are possible; it does not follow that Individuals with learning difficulties can make gains!
The majority of the evidence cited in the section above was for learning difficulties! Also, there are many reported cases individuals who, in spite of significant amounts of cerebral damage, nevertheless function very well (For example; see Christina Santhouse story {https://www.youtube.com/watch?v=sJuwjOCW6Dg}; or the Noah Wall story {https://www.youtube.com/watch?v=UhvCJnjjW9A}; or the Jaxon Buell story {https://www.youtube.com/watch?v=BuN7DCGkjVk})
"But the brain is much more complicated than any of these devices, a fact scientists confirm almost daily with each new discovery. The extent of the brain’s capabilities is unknown, but it is the most complex living structure known in the universe." (The Society for Neuroscience, 2002)
It has been estimated that there are approximately 100 billion neurons in the human brain (Brownson, 2012)(although figures for this estimation vary somewhat: see Braitenberg, 2001; Bartheld et al. 2016) and each can make up to fifteen thousand connections with its neighbours (Brotherson, 2005) providing some some 100 quadrillion (10 to the power 15) interconnections (Tang et al., 2001). With such complexity is it any wonder that there is potential for things to go wrong?
The brains of IEPMLD are, by definition, functionally different to their more cognitively able peers. Examinations and scans of the brains of Individuals Experiencing PMLD have shown that there may be:
- multiple lesions (Crome, 1960; Kjos et al. 1990);
- enlarged ventricles (Crome, 1960; Gabrielli et al.,1998; Soto-Ares et al., 2003);
- smaller brain size (Crome, 1960; Kjos et al. 1990; Kivitie-Kallio, et al.,1998);
- biochemical anomalies (Crome, 1960);
- delayed or deviant myelination (Kjos et al. 1990; Gabrielli et al.,1998; Filippi et al., 2002);
- hypoplastic white matter (Kjos et al. 1990; Gabrielli et al., 1998, 2002; Soto-Ares et al., 2003);
- neuronal migration anomalies (Kjos et al. 1990);
- dysfunctional neuronal connectivity (Courchesne & Pierce, 2005);
- cerebellar cortical dysplasia (Gabrielli et al.,1998; Soto-Ares et al., 2003);
- malformation of the corpus callosum (Gabrielli et al.,1993,1998; 2002; Kivitie-Kallio, et al.,1998; Soto-Ares et al., 2003);
- partially opened septum pellucidum and/or cavum vergae (Soto-Ares et al., 2003);
- cerebral atrophy (Kjos et al. 1990);
- disorganised folia (Soto-Ares et al., 2003);
- enlarged subarachnoid space (Soto-Ares et al., 2003);
- enlarged perivascular spaces (Hirabuki et al.,1994; Soto-Ares et al., 2003);
- partially opened septum pellucidum and or cavum vergae (Soto-Ares et al., 2003);
- cerebral hypoperfusion (George et al., 1992; Zilbovicius et al., 1992; Gupta & Ratnam, 2009);
- other anomaly (there is no claim that this list is comprehensive);
- combinations of the above.
"Possibly the most obvious outcome of this study is the demonstration of the frequency of structural abnormality in the brains of patients with severe mental retardation, and this is in accord with previous experience." (Crome, 1960, page 903)
With such 'structural abnormality' resulting in profound learning difficulties perhaps we should throw in the towel and simply provide palliative care especially when we factor in the likelihood of additional sensory impairments. However, we already know that cerebral issues, typically confounded with problematic sensory factors, are attributes of the IEPMLD condition and, yet, educational establishments the world over are still able to show mental and physical progress. No person who is breathing and awake is incapable of making progress even if only small in comparison to an age equivalent peer: if you question that then this webpage is not for you.
For many years it was believed that, post the period of childhood, the human brain reached maturity and became hard-wired with no further development. Indeed, it was thought that when brain cells died for whatever reason they would not be replaced leading to cognitive decline as a person grew older and older. It was also believed that specific areas of the brain assumed rigid functions and if these areas were damaged in an accident or by a stroke then they were lost forever and recovery would be minimal.
"Up to the late 1990s neuroscience accepted as fact that the brain stops growing new brain cells by adulthood. It was believed that after this cessation, it was just one slow, unavoidable slide into decrepitude as brain cells die off, never to be replaced, gradually at first, but then faster and faster as you age." (Cortright, 2015, page 11)
"Just 50 years ago, the idea that the adult brain can change in any way was heretical. Researchers accepted that the immature brain is malleable but also believed that it gradually hardens, like clay poured into a mold, into a permanently fixed structure by the time childhood had ended. It was also believed that we are born with all the brain cells we will ever have, that the brain is incapable of regenerating itself, and, therefore, that any damage or injuries it sustains cannot be fixed" (Costandi, 2016, page 2)
It is now known a new experience, repeatedly encountered, can have a significant effect which is contrary to the previously held belief that brain structure does not alter except for deterioration with advancing age:
"Our results contradict the traditionally held view that the anatomical structure of the adult human brain does not alter, except for changes in morphology caused by ageing or pathological conditions. Our findings indicate that learning-induced cortical plasticity is also reflected at a structural level." (Draganski et al, 2004)
Furthermore, it has been demonstrated that, at least, some parts of the brain are capable of the generation of new neurons throughout their life:
"During neural development, the nervous system is created from cells that have the potential to proliferate, to reproduce themselves, and to differentiate into the appropriate neuronal and glial phenotypes. Although the adult brain has classically been thought of as a structure
with very limited regenerative capacity, these neural stem cells have recently been shown to exist in the adult central nervous system (CNS) as well. It is now evident that the adult brain is efficiently and continuously generating specific neuronal populations." (Kuhn et al, 2001)
"It was long thought that neuronal production ended soon after birth, fueling a view of the adult brain as a finalized structure (as far as new neurons are concerned), with further plasticity concentrated on synapses. It took some time to realize and demonstrate that neuronal incorporation can, to different degrees, continue during the entire life of an animal." (Cecchi et al, 2001)
"The brain keeps growing new brain cells your entire life. This process is how the brain upgrades itself and enhances your quality of life." (Cortright, 2015, page 11)
The brain is 'plastic':
"In the last few decades, this fixed idea of the brain has been discarded. Instead, we talk about the brain being 'plastic', meaning that the brain changes its own wiring, perhaps almost continuously. Like a piece of silly putty, the brain is molded and reshaped by the forces of life
acting on it. Our wiring grows and develops depending on what we experience - even before birth. As we interact with the world, the world becomes internalized, or mapped, in our brain. The extensive plasticity of the brain continues throughout life." (Zull, 2004, page 69)
"The adult brain, in short, retains much of the plasticity of the developing brain, including the power to repair damaged regions, to grow new neurons, to rezone regions that performed one task and have them assume a new task, to change the circuitry that weaves neurons into networks that allow us to remember, feel, suffer, think, imagine and dream." (Begley, 2009, page 7)
While plasticity is good news it is also, at one and the same time, bad news; if it is plastic it can also deteriorate:
"Connections among neurons that have a high probability of displaying temporally correlated activity tend to become consolidated while connections among neurons that have a lower probability of being activated in a correlated manner tend to become removed." (Singer, 2008, page 100)
"It may come as a surprise to learn that depression and neurodegeneration can be bedfellows – but we now know that severely depressed patients can lose brain cells" (Morris & Fillenz, 2003, page 50)
However, let's be positive and look on the bright side; plasticity suggests the possibility, at least, with the right approaches, Individuals Experiencing PMLD can be helped to progress perhaps to a point at which they could no longer be classified as 'profound' any longer. The question becomes 'what are the right approaches'? What are the recommended practices both within and without the classroom that will assist in brain development? This is too big an area to answer in a section on this webpage and therefore it has been addressed on its own page HERE (in development, not yet accessible). The promotion of neurogenesis and positive neuroplasticity is, thus, a constructive approach in all phases of education and should be addressed wherever and whenever possible.
There is a commonly held misconception, it is false premise that, generally, people only use ten percent of their brain function:
"The 10 percent of the brain myth is a widely perpetuated urban legend that most or all humans only use 10 percent (or some other small percentage) of their brains. It has been misattributed to many people, including Albert Einstein. By extrapolation, it is suggested that a person may harness this unused potential and increase intelligence." (Wikipedia, 2017)
Of course, this assumes that the original form of this statement referred to ten percent by area: in other words, that 90% of the brain is sitting idle while the remaining ten per cent is doing all the work. This would be akin to having a ten room building but only having access to one room with nine rooms remaining locked and inaccessible. This view of the brain is wrong; brain scans have long shown that all rooms in the building are being utilised when we are thinking although, depending upon what we are thinking about, some rooms may be called into action more than others. However, what if the originating statement referred to ten per cent by potential rather than then per cent by area? In our ten room buildings, all the rooms would be being utilised but being utilised rather poorly: that is, if the rooms were re-organised, there would be potential for a 90% efficiency gain over the present methodology. It is our contention that, the original source of the statement concerned 'brain potential' (as opposed to 'brain area') and, thus, claims of it being a 'brain myth' and 'urban legend' are not entirely true. Indeed, it may be that the ten per cent figure is too high; we might only currently be using 1% of our brain's potential! What evidence is there to support such an outrageous claim? We are capable of improvements in:
- thinking skills (Feuerstein et al, 2006; Hoffman & Rand, 2014; Feuerstein et al, 2010);
- memory (Holmes et al., 2009; Perrig et al., 2009; Holmes & Gathercole, 2014; Wilkens, 2017);
- creativity (Birdi, 2005; Snyder, 2009, Flaherty 2015; Sun et al., 2016);
- spatial awareness (Stanton et al., 2000; Fragala et al., 2014 )
- other (there is no claim made the above list is comprehensive)
Evidence that the brain is capable of tremendous feats also comes from another source; that of the autistic savant (Hermelin et al., 1987; Treffert, 1988, 1989; Mottron et al.,1998; Hermelin & O’Connor, 1991; Miller,1999; Heaton, & Wallace, 2004; Tammat, 2007, 2009; Howlin et al., 2009). In the savant, the brain is capable of extraordinary feats in one or more areas of human endeavour (Drawing, mathematics, memory. music, ...) while, at one and the same time, being challenged in virtually all other areas, as depicted in the 1988 film Rain Man (Morrow and Bass, 1988) loosely based on the character of Kim Peek. It is hypothesised that we all possess such latent talent within our brain but that it is suppressed by the natural workings of all the other areas and, therefore, is not normally exhibited (Snyder & Mitchell, 1999; Snyder et al, 2003, 2004; Snyder, 2009). On occasions, following accidental trauma to the brain, such potential has been 'released' in people who, before the trauma, had typically average abilities (LaFay 1987; Treffert 1988; Flaherty, 2015).
"I argue that savant skills are latent in us all. My hypothesis is that savants have privileged access to lower level, less-processed information, before it is packaged into holistic concepts and meaningful labels. Owing to a failure in top-down inhibition, they can tap into information that exists in all of our brains, but is normally beyond conscious awareness. This suggests why savant skills might arise spontaneously in otherwise normal people" (Snyder, 2009, page 1399)
Given the potential of the human brain there must surely be at least some scope for the amelioration of cognitive condition in those experiencing profound learning difficulties.
OK, so what if we accept that improvements in the the potential of the brain are possible; it does not follow that Individuals with learning difficulties can make gains!
The majority of the evidence cited in the section above was for learning difficulties! Also, there are many reported cases individuals who, in spite of significant amounts of cerebral damage, nevertheless function very well (For example; see Christina Santhouse story {https://www.youtube.com/watch?v=sJuwjOCW6Dg}; or the Noah Wall story {https://www.youtube.com/watch?v=UhvCJnjjW9A}; or the Jaxon Buell story {https://www.youtube.com/watch?v=BuN7DCGkjVk})
Indeed, Feuillet et al (2007) reported in 'The Lancet' the case of a French man who was operating with 90% of his brain missing (see also De Oliveira et al, 2011). It would appear that plasticity is possible even under severe challenges.
OK, so what if we accept that improvements in the potential of the brain are possible even for Individuals experiencing learning difficulties. It does not follow that IEPMLD are the same.
Even if IEPMLD are capable of only a fraction of the potential gains of others (let's assume for the moment that this is a fact), they are still capable of gains. Isn't a small improvement worthy of pursuit? Doesn't each tiny improvement have the potential to build on other improvements? Doesn't each improvement increase the likelihood of further improvements?
Even if we grant that improvements in cognitive capacity are possible, doesn't that demand time? Time is one thing that is not in plentiful supply in Specialist Further Education.
You are right in your assertion that time is a factor. What are you doing to address cognitive capacity in the time you do have?
The brain receives input from (at least) eight sensory pathways; the five well known ones (sight, sound, smell, touch, and taste) and three lesser known (proprioception, interoception, & vestibular).
Even if IEPMLD are capable of only a fraction of the potential gains of others (let's assume for the moment that this is a fact), they are still capable of gains. Isn't a small improvement worthy of pursuit? Doesn't each tiny improvement have the potential to build on other improvements? Doesn't each improvement increase the likelihood of further improvements?
Even if we grant that improvements in cognitive capacity are possible, doesn't that demand time? Time is one thing that is not in plentiful supply in Specialist Further Education.
You are right in your assertion that time is a factor. What are you doing to address cognitive capacity in the time you do have?
The brain receives input from (at least) eight sensory pathways; the five well known ones (sight, sound, smell, touch, and taste) and three lesser known (proprioception, interoception, & vestibular).
51. Interaction

"Every time we interact with another person at work, we have a choice to make: do we try to claim as much value as we can, or contribute value without worrying about what we receive in return?" (Grant, 2013)
There is a wealth of research that shows a continuing high level of good, friendly, and supportive interactions (inside and outside of educational sessions) between staff and Learners results in positive outcomes for Individuals experiencing learning difficulties (Golden & Reese, 1996; Schepis & Reid, 1994; Dobson et al., 2002; Bloomberg et al., 2003; Singh et al, 2003)
However, past research often highlighted a deficit of positive interactions between staff and Individuals (see, for example, Veit, Allen, & Chinsky, 1976; Repp, Felce, & de Kock,1987; Chan & Yau, 2002). The research by Chan and Yau (2002), for example, found that there were low or no staff/individual interactions in 63% of the sessions they observed. Additionally, they noted, the staff-initiated interactions, tended to focus on care provision which was short and had very little positive outcome. While much of this research did not occur in Further Education establishments and may be reasonably argued to be 'a thing of the past', it nevertheless highlights a need for continuing good practice in staff student interactions.
"Although positive interactions often result in beneficial outcomes, researchers have found that direct care staff seldom initiate interactions with individuals with disabilities. Therefore, training staff to increase the quality and quantity of interactions is important." (Martell, 2012, page 21)
It has been shown that there is an inverse relationship between the volume of staff interaction and the level of physical and communicative ability. That is the greater the level of physical disability and or communication impairment the less time staff spend in interacting (Grant & Moores, 1977). As IEPMLD tend to have a greater level of physical impairment coupled with a lack of spoken language this is an area of concern. As such, effectively addressing communication between staff and Learners can improve both the volume and quality of interactions. For example, Schepis and Reid (1995) found that when a Learner was taught how to use a communication aid, the frequency of interactions
between staff and student increased.
"Furthermore, the results of this study demonstrated that individuals diagnosed with moderate to profound intellectual disabilities may acquire social skills appropriate to their developmental level by simple exposure to appropriate behavior modeled by direct care staff. This finding lends support to previous research, demonstrating improved outcomes for residents with developmental disabilities when regularly engaged in positive social interaction with staff. Given these results, DCS ... should frequently engage residents in positive interactions during both structured and unstructured activities." (Martell, 2012, page 54)
There is a wealth of research that shows a continuing high level of good, friendly, and supportive interactions (inside and outside of educational sessions) between staff and Learners results in positive outcomes for Individuals experiencing learning difficulties (Golden & Reese, 1996; Schepis & Reid, 1994; Dobson et al., 2002; Bloomberg et al., 2003; Singh et al, 2003)
However, past research often highlighted a deficit of positive interactions between staff and Individuals (see, for example, Veit, Allen, & Chinsky, 1976; Repp, Felce, & de Kock,1987; Chan & Yau, 2002). The research by Chan and Yau (2002), for example, found that there were low or no staff/individual interactions in 63% of the sessions they observed. Additionally, they noted, the staff-initiated interactions, tended to focus on care provision which was short and had very little positive outcome. While much of this research did not occur in Further Education establishments and may be reasonably argued to be 'a thing of the past', it nevertheless highlights a need for continuing good practice in staff student interactions.
"Although positive interactions often result in beneficial outcomes, researchers have found that direct care staff seldom initiate interactions with individuals with disabilities. Therefore, training staff to increase the quality and quantity of interactions is important." (Martell, 2012, page 21)
It has been shown that there is an inverse relationship between the volume of staff interaction and the level of physical and communicative ability. That is the greater the level of physical disability and or communication impairment the less time staff spend in interacting (Grant & Moores, 1977). As IEPMLD tend to have a greater level of physical impairment coupled with a lack of spoken language this is an area of concern. As such, effectively addressing communication between staff and Learners can improve both the volume and quality of interactions. For example, Schepis and Reid (1995) found that when a Learner was taught how to use a communication aid, the frequency of interactions
between staff and student increased.
"Furthermore, the results of this study demonstrated that individuals diagnosed with moderate to profound intellectual disabilities may acquire social skills appropriate to their developmental level by simple exposure to appropriate behavior modeled by direct care staff. This finding lends support to previous research, demonstrating improved outcomes for residents with developmental disabilities when regularly engaged in positive social interaction with staff. Given these results, DCS ... should frequently engage residents in positive interactions during both structured and unstructured activities." (Martell, 2012, page 54)
52. The Worry of Waiting

Rote Round Robin Routines R Really Ruinous
"Inattention or off-task behavior is a significant problem in educational settings as inattention reduces students’ opportunities to learn. Therefore, it is imperative that researchers isolate antecedents of off-task behavior in order to identify potential avenues for intervention." (Godwin et al, 2016)
"We often feel like we’ve got too much to do, so we have to plan how to fit it all in. People with learning disabilities often have too little to do. They spend time waiting, perhaps bored, for the next opportunity to do something and make a contribution. Planning for a full day can help people lead more fulfilling lives." (Jones et al, 2009, page 8)
"Listed from high to low in terms of percentage of other time spent, Ashley, Karen, and Abby spent 29% of their time waiting; 12% in transitions; 10% in knowledge content (i.e., listening to information about technique, rules of game, strategy, or background); 8% in management; and 2% off task." (Place and Hodge 2001 page 401)
While it might be argued that this issue is a problem that was related to the past, a more recent report (Bradshaw, J. Beadle-Brown, J., Beecham J., Mansell, J., Baumker, T., Leigh, J., Whelton, R., & Richardson, L. 2013) showed that (page 25) on average people with an Intellectual Disability:
All Learners spend some time in education 'off task' (Roberts, 2001; Godwin et al, 2016); some will talk to peers, others just daydream. However, the reasons that IEPMLD are likely to be off-task is likely to vary from any 'norm': for example:
adjusted and if possible cut down. For medication may cause a number of side effects such as reduced alertness
or habituation and resistance." (Petry et al., 2007c, page 136)
However, when they are on-task and attentive, it is important we do not adopt practices that might result in a loss of attention and a movement towards off-task behaviours. Individuals in special education spend a lot of time waiting (Place and Hodge, 2001), it is important we minimise this aspect and take a fresh look at anything that might impede such action.
One behaviour that might lead to additional Learner waiting time is 'inter-staff chatter'. As special education classrooms are highly staffed and as, also, IEPMLD are, by definition, unable to converse with staff using spoken language, there is a tendency for communication to be predominantly between staff member and staff member. Such conversations are not necessarily work related (see Hile and Walbran, 1991). This means that staff members can be conversing about non-work related matters during interactions with Learners. It follows that such practice may increase the time Learners spend waiting as well as to reinforce their passive position. In addition to this, Learners can spend a great deal of time waiting in special needs environments for many other reasons: these might include (but not limited to) waiting for ...
The graphic in this section depicts an all too typical classroom situation in which the teacher is moving around a group one by one in a 'round robin' style. The problem with this approach is that, by definition, if there are ten members in the group (quite large for a group with special needs) then each Learner is active for one tenth of the time. The other nine tenths of the time is spent waiting.
What is an Individual Experiencing Profound and Multiple Learning Difficulties likely to be doing while s/he is waiting? We would suggest that any one of the following may be a possibility:
In other words the Learner is likely to find some means to SELF stimulate: something to fill in the time spent being inactive or with lacking any semblance of control. Of course, the staff presumption is that each Learner, while waiting, is sitting there paying attention to what each active member of the group is doing but is that likely? Perhaps there is a small chance that this happens the very first time it is done but what if this is a routine event? What does the the Learner learn to do in a Learner queuing system?
In a Learner queuing system the group of Learners are typically arranged in a row, a semi-circle or in a circle and an 'activity' is passed around the group one Learner at a time. For example, each member of the group is encouraged to say 'good morning' or interact with an sensory object as a staff member moves along the line. The last member of the group has to wait until all the others have had their individual turn and the first group member (once the interaction with the activity is complete to the satisfaction of the controlling staff member) has to wait until all others have completed the task and the focus moves back to the group dynamic once again. All group members are on task for a short period of time but play the waiting game for a much longer period of time: the more group members the longer the period of waiting. In a Learner queuing approach only one Learner is active at any one time:
L1 L2 L3 L4 L5 L6 L7 L8
each Learner becomes active as the focus passes around the group. Even though:
'<Learner> will learn how to wait appropriately',
or
'<Learner> will learn how to take turns,>
and that is somewhat concerning for it is likely that <Learner> will already be spending a great deal of time waiting or waiting his/her turn!!
The purpose of this website is not just to point out poor practice but to suggest practical alternatives. There are, at least, five possible alternatives to Learner queuing. These are outlined below. The first is the preferred methodology by Talksense. You may know of others. If you are willing to share alternative methodologies, please get in touch so that we may add other approaches to this section of this page. You may also want to raise issues with the whole of this section. Again, please feel free to get in touch using the form provided at the bottom of this page.
Alternative 1: The LAG Approach
The first alternative to Learner queuing is what may be called the LAG approach where LAG stands for Learner And Group. In this classroom technique a staff member's interactions with a group of Learners (individually) is interspersed with a short whole group activity. Thus, instead of the L1, L2, L3, ... arrangement as seen above, what we now have is:
L1 G L2 G L3 G L4 G L5 G...
where G = Group
Here, as you can see, the focus passes from Learner to Learner as before but, in between, there is a short group-based dynamic which maintains cognitive engagement for all participants with the given task. For example, if the session in question was a morning greeting. Learner One would be enabled to say 'good morning' to the group. Following this, and before Learner Two was enabled to say 'good morning', the whole group would be enabled/required to say 'good morning' to Learner One. This may be by signing (Makaton, Signalong or other) or through the use of SGDs or some other methodology. The session dynamic changes: no longer are individual Learners sitting awaiting their turn and waiting after their turn but, rather, only inactive for the time it takes a single Learner to say 'Good Morning' to the group before they are called into action again to respond to each group member's greeting.
Alternative 2: One on One
In the second alternative, individual Learners have one-on-one staff support. The staff member's task is to maintain Learner cognitive engagement while the focus progresses. However, this is easier said than done: how is a staff member to cognitively engage a Learner during a good morning activity, for example, in a meaningful manner while awaiting the Learner's turn and, even if they can do it, how do they do it without disturbing/distracting any other member of the group?
If the Learners are getting on with individual work while the good morning greeting is progressing, this creates a third alternative ...
Alternative 3: Individual work
In this alternative, Learners are actually working on some activity as a group or as individuals. While they are working, they are interrupted to allow a staff member to present a new focus to them one by one. While the Learners are not waiting, interrupting one period of cognitive engagement with another, only to expect the Learner to return to the first cognitive activity is probably not the best of practices!
Alternative 4: Break Down
In this alternative, supporting staff (Learning Support Assistants) break down the group into smaller units of just two or three members and thus any utilisation of a round robin approach requires much less waiting time. Indeed, the teacher may not work with a specific group at all in this approach but may rotate around the groups supporting the support staff and or withdraw one Learner at a time for specific one on one work.
Alternative 5: The Cannon Approach
This alternative was suggested by Sean Cannon. At the time, Sean was the interim Principal of a special education college in which TalkSense was giving a talk. Sean's suggestions was G IIIIIII G. In other words, the Sensory Story starts with a group dynamic but then splits into a round robin (with each Learner receiving individual sensory input for a different section of the story) and then (after each Learner has moved around all the round robin story sections) ends once again with the group together. For this to work, the story's middle section must not follow a logical sequence of events; only the beginning and end need to be in that position (all other sections can be in any order). For example, in one of the example stories on this page (see section lower down this page) entitles 'going on a boat', the beginning and the ending of the story have to be the beginning and the ending respectively BUT all the other sections in between can be put in any order and the story would still make sense. Thus, during the middle section of the story, the Learners could move from a group to individual work with each staff member responsible for delivering a specific section. After each Learner has experienced a particular middle section with one member of staff, the Learner rotates around all the other staff to a further sensory section, one by one, until each Learner has experienced each section. The Learners can all come together as a group once again for the end of the story. There are benefits to this approach:
"Inattention or off-task behavior is a significant problem in educational settings as inattention reduces students’ opportunities to learn. Therefore, it is imperative that researchers isolate antecedents of off-task behavior in order to identify potential avenues for intervention." (Godwin et al, 2016)
"We often feel like we’ve got too much to do, so we have to plan how to fit it all in. People with learning disabilities often have too little to do. They spend time waiting, perhaps bored, for the next opportunity to do something and make a contribution. Planning for a full day can help people lead more fulfilling lives." (Jones et al, 2009, page 8)
"Listed from high to low in terms of percentage of other time spent, Ashley, Karen, and Abby spent 29% of their time waiting; 12% in transitions; 10% in knowledge content (i.e., listening to information about technique, rules of game, strategy, or background); 8% in management; and 2% off task." (Place and Hodge 2001 page 401)
While it might be argued that this issue is a problem that was related to the past, a more recent report (Bradshaw, J. Beadle-Brown, J., Beecham J., Mansell, J., Baumker, T., Leigh, J., Whelton, R., & Richardson, L. 2013) showed that (page 25) on average people with an Intellectual Disability:
- were engaged in activity for less than half the time (44%);
- had little contact from staff for around 75% of the time;
- received direct assistance to partake in activities for only 6% of the time;
- typically had little support for choice with 22% getting what they considered to be good support in this area.
All Learners spend some time in education 'off task' (Roberts, 2001; Godwin et al, 2016); some will talk to peers, others just daydream. However, the reasons that IEPMLD are likely to be off-task is likely to vary from any 'norm': for example:
- they may be on medication that makes them drowsy:
adjusted and if possible cut down. For medication may cause a number of side effects such as reduced alertness
or habituation and resistance." (Petry et al., 2007c, page 136)
- their condition may make it difficult for them to process the information being presented;
- they may have had an earlier seizure and be tired or they may have had a poor previous evening and just need to sleep;
- and they are more likely to be ill (Schrojenstein Lantman‐de Valk et al, 1997; Kapell et al, 1998; Zijlstra & Vlaskamp, 2005b; Van Timmeren et al., 2016)(see also Jansen et al., 2004 for a review):
However, when they are on-task and attentive, it is important we do not adopt practices that might result in a loss of attention and a movement towards off-task behaviours. Individuals in special education spend a lot of time waiting (Place and Hodge, 2001), it is important we minimise this aspect and take a fresh look at anything that might impede such action.
One behaviour that might lead to additional Learner waiting time is 'inter-staff chatter'. As special education classrooms are highly staffed and as, also, IEPMLD are, by definition, unable to converse with staff using spoken language, there is a tendency for communication to be predominantly between staff member and staff member. Such conversations are not necessarily work related (see Hile and Walbran, 1991). This means that staff members can be conversing about non-work related matters during interactions with Learners. It follows that such practice may increase the time Learners spend waiting as well as to reinforce their passive position. In addition to this, Learners can spend a great deal of time waiting in special needs environments for many other reasons: these might include (but not limited to) waiting for ...
- the session to begin (session not prepared, waiting for all Learners to arrive, waiting for transport);
- a round robin to reach them;
- the session to return to whole group after their turn in round robin;
- a staff member to attend to them (staff busy with other matters, staff not noticing Learner need, staff talking to other staff);
- staff set-up (or repair) of equipment;
- other
The graphic in this section depicts an all too typical classroom situation in which the teacher is moving around a group one by one in a 'round robin' style. The problem with this approach is that, by definition, if there are ten members in the group (quite large for a group with special needs) then each Learner is active for one tenth of the time. The other nine tenths of the time is spent waiting.
What is an Individual Experiencing Profound and Multiple Learning Difficulties likely to be doing while s/he is waiting? We would suggest that any one of the following may be a possibility:
- Stimming: self stimulatory behaviour; Sibbing: Self Injurious Behaviour;
- Engaging in behaviours that others may find challenging;
- Losing Focus (off-task behaviour);
- Falling asleep.
In other words the Learner is likely to find some means to SELF stimulate: something to fill in the time spent being inactive or with lacking any semblance of control. Of course, the staff presumption is that each Learner, while waiting, is sitting there paying attention to what each active member of the group is doing but is that likely? Perhaps there is a small chance that this happens the very first time it is done but what if this is a routine event? What does the the Learner learn to do in a Learner queuing system?
In a Learner queuing system the group of Learners are typically arranged in a row, a semi-circle or in a circle and an 'activity' is passed around the group one Learner at a time. For example, each member of the group is encouraged to say 'good morning' or interact with an sensory object as a staff member moves along the line. The last member of the group has to wait until all the others have had their individual turn and the first group member (once the interaction with the activity is complete to the satisfaction of the controlling staff member) has to wait until all others have completed the task and the focus moves back to the group dynamic once again. All group members are on task for a short period of time but play the waiting game for a much longer period of time: the more group members the longer the period of waiting. In a Learner queuing approach only one Learner is active at any one time:
L1 L2 L3 L4 L5 L6 L7 L8
each Learner becomes active as the focus passes around the group. Even though:
- staff may be very well intentioned;
- the the activity itself may be worthwhile and;
- is very well done...
'<Learner> will learn how to wait appropriately',
or
'<Learner> will learn how to take turns,>
and that is somewhat concerning for it is likely that <Learner> will already be spending a great deal of time waiting or waiting his/her turn!!
The purpose of this website is not just to point out poor practice but to suggest practical alternatives. There are, at least, five possible alternatives to Learner queuing. These are outlined below. The first is the preferred methodology by Talksense. You may know of others. If you are willing to share alternative methodologies, please get in touch so that we may add other approaches to this section of this page. You may also want to raise issues with the whole of this section. Again, please feel free to get in touch using the form provided at the bottom of this page.
Alternative 1: The LAG Approach
The first alternative to Learner queuing is what may be called the LAG approach where LAG stands for Learner And Group. In this classroom technique a staff member's interactions with a group of Learners (individually) is interspersed with a short whole group activity. Thus, instead of the L1, L2, L3, ... arrangement as seen above, what we now have is:
L1 G L2 G L3 G L4 G L5 G...
where G = Group
Here, as you can see, the focus passes from Learner to Learner as before but, in between, there is a short group-based dynamic which maintains cognitive engagement for all participants with the given task. For example, if the session in question was a morning greeting. Learner One would be enabled to say 'good morning' to the group. Following this, and before Learner Two was enabled to say 'good morning', the whole group would be enabled/required to say 'good morning' to Learner One. This may be by signing (Makaton, Signalong or other) or through the use of SGDs or some other methodology. The session dynamic changes: no longer are individual Learners sitting awaiting their turn and waiting after their turn but, rather, only inactive for the time it takes a single Learner to say 'Good Morning' to the group before they are called into action again to respond to each group member's greeting.
Alternative 2: One on One
In the second alternative, individual Learners have one-on-one staff support. The staff member's task is to maintain Learner cognitive engagement while the focus progresses. However, this is easier said than done: how is a staff member to cognitively engage a Learner during a good morning activity, for example, in a meaningful manner while awaiting the Learner's turn and, even if they can do it, how do they do it without disturbing/distracting any other member of the group?
If the Learners are getting on with individual work while the good morning greeting is progressing, this creates a third alternative ...
Alternative 3: Individual work
In this alternative, Learners are actually working on some activity as a group or as individuals. While they are working, they are interrupted to allow a staff member to present a new focus to them one by one. While the Learners are not waiting, interrupting one period of cognitive engagement with another, only to expect the Learner to return to the first cognitive activity is probably not the best of practices!
Alternative 4: Break Down
In this alternative, supporting staff (Learning Support Assistants) break down the group into smaller units of just two or three members and thus any utilisation of a round robin approach requires much less waiting time. Indeed, the teacher may not work with a specific group at all in this approach but may rotate around the groups supporting the support staff and or withdraw one Learner at a time for specific one on one work.
Alternative 5: The Cannon Approach
This alternative was suggested by Sean Cannon. At the time, Sean was the interim Principal of a special education college in which TalkSense was giving a talk. Sean's suggestions was G IIIIIII G. In other words, the Sensory Story starts with a group dynamic but then splits into a round robin (with each Learner receiving individual sensory input for a different section of the story) and then (after each Learner has moved around all the round robin story sections) ends once again with the group together. For this to work, the story's middle section must not follow a logical sequence of events; only the beginning and end need to be in that position (all other sections can be in any order). For example, in one of the example stories on this page (see section lower down this page) entitles 'going on a boat', the beginning and the ending of the story have to be the beginning and the ending respectively BUT all the other sections in between can be put in any order and the story would still make sense. Thus, during the middle section of the story, the Learners could move from a group to individual work with each staff member responsible for delivering a specific section. After each Learner has experienced a particular middle section with one member of staff, the Learner rotates around all the other staff to a further sensory section, one by one, until each Learner has experienced each section. The Learners can all come together as a group once again for the end of the story. There are benefits to this approach:
- Learners get one to one attention;
- Learners get to work with all staff;
- Staff get to work with all Learners;
- Staff get to know one section of the story very well and can improve the delivery of its sensory aspects;
- Staff come to understand that a particular section needs adapting for specific Learners but not for others (for example, a staff might adjust his/her delivery for a Learner with a hearing loss);
- Staff know what resources are necessary to deliver their section and can be responsible for them;
- As one member of staff is responsible for one section, the section is more likely to be delivered consistently.
- This approach only works with a non sequential story line;
- In a confined space one sensory session may interfere with another. For example, a sound effect being delivered in one staff Learner pairing might interfere with another sound effect being delivered by yet another pairing - it would be difficult to prevent sound effects being heard by other Learners working on another section of the story. This might lead to confusion.
- Do Learners revolve around the staff OR do staff revolve around the Learners?
- How do staff ensure that the timing of the change over from section to section coincides?
53. I would prefer not to ...

"In this very attitude did I sit when I called to him, rapidly stating what it was I wanted him to do - namely, to examine a small paper with me. Imagine my surprise, nay, my consternation, when without moving from his privacy, Bartleby in a singularly mild, firm voice, replied, 'I would prefer not to.' ” (Melville, 1853)
In a short story by Herman Melville, first published in Putnam's monthly magazine in two parts, Melville tells the tale of a man named Bartleby who responded to almost every request of him using the phrase 'I would prefer not to' ! Thusly, Bartleby exercised control through choice over his environment and the people within it, albeit in a somewhat negative manner. Bartleby's preferences were, therefore, not really known other, than he preferred not to do something. Of course, while absenting oneself should be viewed as a legitimate response:
"Absenting oneself, or refusing to comply with a request, should be recognised as legitimate responses and areas where further learning can take place" (Jackson and Jackson 1999 page 84)
Continuing the choice of 'absenting' (as in the case of Bartleby) presents something of a problem especially when an establishment is being given a lot of money to provide 'education'. However, IEPMLD are unlikely to choose to 'absent' themselves unless they refrain from participation because of:
It is important that we establish the preferences of IEPMLD for, in knowing individual preferences we able better able to:
BEST = Best Ever Stimulating Thing
What is it the the Learner loves? Is it sweets/candy? Is it a particular game, a TV programme, a particular person? In other words, what is the Best Ever Stimulating Thing for a particular individual? Let's start working with this BEST as the motivator.
POLE = Person Object Location Event
The BEST thing will be a POLE. POLE is an acronym for Person, Object, Location, or Event.
If we can place a tangible POLE at the end of a Learner action (For example: provide the Learner with a POLE as a result of a request using an Augmentative Communication system or activating a switch) then we have a way of moving forward. Not just any sort of POLE! What sort of POLE? Well, a BEST POLE of course.
Here are some ideas:
For those that can touch: Start with a single BIGmack (or equivalent device). Label it with an appropriate symbol or a Sensory Surface for the Learner's BEST POLE. By demonstrating, modelling, prompting, or even waiting for accidental access, allow the Learner to 'see' that the activation of the device leads to ( is always followed by) the provision of a BEST POLE. Hopefully, after a number of activations of the BIGmack the Learner will begin to understand that his /her action (activating the BIGmack) results in a particularly favoured and rewarding event. However, even though a Learner may activate such a device repeatedly, it is difficult to establish intentionality: the Learner may continue to activate a device accidentally (for example) or just be exploring (and thus repeatedly activating) anything that has been placed in the Learner's reach without making any cognitive connection between his or her action and the rewards that seem to be occurring. How could we be more certain of some form of Learner cognizance?
If a baseline is taken in which the BIGmack (or equivalent) is utilised in a different manner (with a different sensory surface or symbol) such that it just plays a short piece of relatively uninteresting music (for example) then, when it is placed within the reach of the Learner, the number of activations (accidental and or purposeful) in a specified time period can recorded. Perhaps such practice might result in 4 activations in the first minute but this tails off afterwards such that it averages at less than one activation a minute. This is our baseline. If we now introduce the BIGmack resulting in the BEST POLE and this results in an increase in activations over time it would seem a reasonable assumption that the difference in Learner behaviour is as a result of some level of cognisance of the situation. As it is always good practice for staff to look for alternative explanations for changes in Learner behaviour, this situation should be no different. Perhaps the Learner is attracted to the BIGmack because it is a different colour (ensure that the same BIGmack is used). Perhaps the Learner is stimulated by the sensory surface that has been used and it is this that is causing the increased response level. How could we eliminate this possibility from our findings? We could swap the sensory surfaces used in the first experience (baseline) with the second and see if this provides similar results. While it is not good practice to use sensory surfaces it such a manner normally, in this instance it is justified. If the repeated baseline with the new sensory surface yields similar results to the original baseline then it cannot be the sensory surface itself that is responsible for the change in Learner response.
"Eliminate all other factors, and the one which remains must be the truth." (Sherlock Holmes, The sign of Four, Chapter 1, p. 92)
Once basic contingency awareness has been established and we have a Learner activating a BIGmack (or equivalent) to obtain a reward, it becomes necessary to step up the level of difficulty of the task very slightly further to ascertain Learner cognisance. If we add a second BIGmack of a different colour (New BIGmacks come with four different colour interchangeable tops) which, when activated, says "Please remove the BIGmacks for five minutes" in a voice that is neutral in tone (such that the sound itself does not become a motivator) complete with a different symbolic label or sensory surface (or a lack of symbolic label or sensory surface) and both BIGmacks are placed within the reach of the Learner, we can now assess if the Learner activates the BIGmack which leads to a BEST reward more than the one which leads to their removal. Thus, as you can see, the activation of the original BIGmack leads to a reward while the activation of the other different BIGmack leads to their removal (and therefore no possibility of BEST) for a specified period of time. Initially, to assist the Learner in achieving success, the BEST BIGmack can be positioned on the preferred side of the Learner such that it is likely that this is the one that will be activated. However, before moving to the next stage, it is important to swap the BIGmacks about such that, in wherever order they are positioned, the Learner still demonstrates that s/he can achieve success.
On success with two BIGmacks, step it up once more to three! Two of the BIGmacks lead to the removal of the setup (for a specified short time period) and only the original BIGmack obtains the BEST POLE. If the Learner learns to activate the BEST BIGmack no matter what position it occupies relative to the other two then there are a number of things that we might justifiably claim:
No, s/he's not doing that at all! S/he is just attracted to red BIGmacks and is going for the red one each time - no recall is taking place.
OK, that is a good point. So what should we do about that possibility? If it is known in advance that the Learner is attracted to the colour red then we should not use red as the BEST BIGmack but rather for the distractors! Alternatively, we can make all the BIGmacks red and just vary the attached symbols or the sensory surfaces.
We haven't got three BIGmacks!
It is Talksense's advice that every classroom should have at least three BIGmacks (AbleNet are not sponsoring me to say that! ) available for use. However, it does not have to be a BIGmack system, it can be any SGD (Speech Generating Device) or a device that has at least three cells (the other cells can remain blank). Alternatively, it is possible to use the Microsoft PowerPoint program on a touch sensitive screen although difficult to provide sensory surfaces by this methodology.
It's working too well: the Learner is asking for BEST all the time and we cannot support this!
Then remove the BIGmacks once the task has been completed and work on another area. You may also need to consider the use of 'limiting factors' was detailed on the fundamentals page of this website.
The BIGmacks can either have symbols on their surfaces or be presented with sensory switch caps. Only one BIGmack leads to the reward of a BEST POLE, the others either do something innocuous such as saying 'This BIGmack does nothing' or request their removal as stated above. The BIGmacks are positioned in front of the Learner. Beginning with a single BIGmack, the Learner will eventually activate it by accident. On so doing, the Learner is rewarded with the BEST. It is important that the reward follows the rules for BEST as outlined on the fundamentals page (follow link to go there).
My Learner is not interacting with the BIGmack even by accident.
For Learners that do not interact with the BIGmack it may be necessary for another member of staff to model the required behaviour such that the Learner can experience the staff member obtaining the BEST through the activation of a particular BIGmack. Should even that approach yield no result, the Learner can then be assisted to activate the BIGmack through hand-under-hand physical prompting.
In a short story by Herman Melville, first published in Putnam's monthly magazine in two parts, Melville tells the tale of a man named Bartleby who responded to almost every request of him using the phrase 'I would prefer not to' ! Thusly, Bartleby exercised control through choice over his environment and the people within it, albeit in a somewhat negative manner. Bartleby's preferences were, therefore, not really known other, than he preferred not to do something. Of course, while absenting oneself should be viewed as a legitimate response:
"Absenting oneself, or refusing to comply with a request, should be recognised as legitimate responses and areas where further learning can take place" (Jackson and Jackson 1999 page 84)
Continuing the choice of 'absenting' (as in the case of Bartleby) presents something of a problem especially when an establishment is being given a lot of money to provide 'education'. However, IEPMLD are unlikely to choose to 'absent' themselves unless they refrain from participation because of:
- some aspect of sensory integration dysfunction (for example, tactile defensiveness);
- a fixation on some other aspect of the environment (it could be a person);
- ongoing experience of pain (Breau et al., 2003; Breau & Burkitt, 2009);
- anxiety or fear (Matson et al., 1997);
- a need to sleep (Quine, 1991; Wiggs & Stores, 1996, 1998; Quine, 2001);
- other (there is no pretence that this listing is comprehensive).
It is important that we establish the preferences of IEPMLD for, in knowing individual preferences we able better able to:
- motivate Learners;
- enable learning;
- provide opportunities to teach choice;
BEST = Best Ever Stimulating Thing
What is it the the Learner loves? Is it sweets/candy? Is it a particular game, a TV programme, a particular person? In other words, what is the Best Ever Stimulating Thing for a particular individual? Let's start working with this BEST as the motivator.
POLE = Person Object Location Event
The BEST thing will be a POLE. POLE is an acronym for Person, Object, Location, or Event.
If we can place a tangible POLE at the end of a Learner action (For example: provide the Learner with a POLE as a result of a request using an Augmentative Communication system or activating a switch) then we have a way of moving forward. Not just any sort of POLE! What sort of POLE? Well, a BEST POLE of course.
Here are some ideas:
For those that can touch: Start with a single BIGmack (or equivalent device). Label it with an appropriate symbol or a Sensory Surface for the Learner's BEST POLE. By demonstrating, modelling, prompting, or even waiting for accidental access, allow the Learner to 'see' that the activation of the device leads to ( is always followed by) the provision of a BEST POLE. Hopefully, after a number of activations of the BIGmack the Learner will begin to understand that his /her action (activating the BIGmack) results in a particularly favoured and rewarding event. However, even though a Learner may activate such a device repeatedly, it is difficult to establish intentionality: the Learner may continue to activate a device accidentally (for example) or just be exploring (and thus repeatedly activating) anything that has been placed in the Learner's reach without making any cognitive connection between his or her action and the rewards that seem to be occurring. How could we be more certain of some form of Learner cognizance?
If a baseline is taken in which the BIGmack (or equivalent) is utilised in a different manner (with a different sensory surface or symbol) such that it just plays a short piece of relatively uninteresting music (for example) then, when it is placed within the reach of the Learner, the number of activations (accidental and or purposeful) in a specified time period can recorded. Perhaps such practice might result in 4 activations in the first minute but this tails off afterwards such that it averages at less than one activation a minute. This is our baseline. If we now introduce the BIGmack resulting in the BEST POLE and this results in an increase in activations over time it would seem a reasonable assumption that the difference in Learner behaviour is as a result of some level of cognisance of the situation. As it is always good practice for staff to look for alternative explanations for changes in Learner behaviour, this situation should be no different. Perhaps the Learner is attracted to the BIGmack because it is a different colour (ensure that the same BIGmack is used). Perhaps the Learner is stimulated by the sensory surface that has been used and it is this that is causing the increased response level. How could we eliminate this possibility from our findings? We could swap the sensory surfaces used in the first experience (baseline) with the second and see if this provides similar results. While it is not good practice to use sensory surfaces it such a manner normally, in this instance it is justified. If the repeated baseline with the new sensory surface yields similar results to the original baseline then it cannot be the sensory surface itself that is responsible for the change in Learner response.
"Eliminate all other factors, and the one which remains must be the truth." (Sherlock Holmes, The sign of Four, Chapter 1, p. 92)
Once basic contingency awareness has been established and we have a Learner activating a BIGmack (or equivalent) to obtain a reward, it becomes necessary to step up the level of difficulty of the task very slightly further to ascertain Learner cognisance. If we add a second BIGmack of a different colour (New BIGmacks come with four different colour interchangeable tops) which, when activated, says "Please remove the BIGmacks for five minutes" in a voice that is neutral in tone (such that the sound itself does not become a motivator) complete with a different symbolic label or sensory surface (or a lack of symbolic label or sensory surface) and both BIGmacks are placed within the reach of the Learner, we can now assess if the Learner activates the BIGmack which leads to a BEST reward more than the one which leads to their removal. Thus, as you can see, the activation of the original BIGmack leads to a reward while the activation of the other different BIGmack leads to their removal (and therefore no possibility of BEST) for a specified period of time. Initially, to assist the Learner in achieving success, the BEST BIGmack can be positioned on the preferred side of the Learner such that it is likely that this is the one that will be activated. However, before moving to the next stage, it is important to swap the BIGmacks about such that, in wherever order they are positioned, the Learner still demonstrates that s/he can achieve success.
On success with two BIGmacks, step it up once more to three! Two of the BIGmacks lead to the removal of the setup (for a specified short time period) and only the original BIGmack obtains the BEST POLE. If the Learner learns to activate the BEST BIGmack no matter what position it occupies relative to the other two then there are a number of things that we might justifiably claim:
- the Learner is retaining and recalling the function of a specific BIGmack;
- the Learner is discriminating between the symbols or the sensory surfaces or the colours (if all the BIGmacks used were red then it must be either the sensory surface or the symbol used that is discriminated);
- the Learner is connecting a specific action (his/her activation of the device) with a particular environmental effect (his/her obtaining a BEST).
No, s/he's not doing that at all! S/he is just attracted to red BIGmacks and is going for the red one each time - no recall is taking place.
OK, that is a good point. So what should we do about that possibility? If it is known in advance that the Learner is attracted to the colour red then we should not use red as the BEST BIGmack but rather for the distractors! Alternatively, we can make all the BIGmacks red and just vary the attached symbols or the sensory surfaces.
We haven't got three BIGmacks!
It is Talksense's advice that every classroom should have at least three BIGmacks (AbleNet are not sponsoring me to say that! ) available for use. However, it does not have to be a BIGmack system, it can be any SGD (Speech Generating Device) or a device that has at least three cells (the other cells can remain blank). Alternatively, it is possible to use the Microsoft PowerPoint program on a touch sensitive screen although difficult to provide sensory surfaces by this methodology.
It's working too well: the Learner is asking for BEST all the time and we cannot support this!
Then remove the BIGmacks once the task has been completed and work on another area. You may also need to consider the use of 'limiting factors' was detailed on the fundamentals page of this website.
The BIGmacks can either have symbols on their surfaces or be presented with sensory switch caps. Only one BIGmack leads to the reward of a BEST POLE, the others either do something innocuous such as saying 'This BIGmack does nothing' or request their removal as stated above. The BIGmacks are positioned in front of the Learner. Beginning with a single BIGmack, the Learner will eventually activate it by accident. On so doing, the Learner is rewarded with the BEST. It is important that the reward follows the rules for BEST as outlined on the fundamentals page (follow link to go there).
My Learner is not interacting with the BIGmack even by accident.
For Learners that do not interact with the BIGmack it may be necessary for another member of staff to model the required behaviour such that the Learner can experience the staff member obtaining the BEST through the activation of a particular BIGmack. Should even that approach yield no result, the Learner can then be assisted to activate the BIGmack through hand-under-hand physical prompting.
You might provide an intermediate stage in which the BIGmacks are presented but only one has a symbol attached as depicted in the illustration right. We are not trying to trick the Learner or make it difficult for him or her: we want the Learner to succeed and therefore you can provide as may intermediate stages as you think fit that will assist Learners on their way. Initially, for example, you might put the 'correct' BIGmack in the Learner's favoured position and then move it one place from there. You may also start with the Learner's preferred colour but this must be changed before the final stage of the procedure.
If a Learner can activate (on more than one occasion) the correct BIGmack by selecting a colour (and or a symbol) from three choices of colour (and or symbol) then it is party time! This a momentous achievement. Suppose all three BIGmacks are the same colour and all have symbols and yet the Learner still selects the reward (on more than one occasion) and with the BIGmacks in different relative position on each occasion - what can we now assert? The Learner must be discriminating between symbols! If a Learner can discriminate between symbols then the sky is the limit. Ensure you reward both yourself and your team for a job well done!
For those that cannot touch (but can see): At least five cards may be prepared. Each of the cards depicts a different random shape which has no specific meaning. One of the cards is selected to represent the BEST. This is taught to the individual Learner through a combination of association and modelling (see below) until the Learner can select the card (without error) using a their own specific yes/no response in a 'blind' staff presentation.
If a Learner can activate (on more than one occasion) the correct BIGmack by selecting a colour (and or a symbol) from three choices of colour (and or symbol) then it is party time! This a momentous achievement. Suppose all three BIGmacks are the same colour and all have symbols and yet the Learner still selects the reward (on more than one occasion) and with the BIGmacks in different relative position on each occasion - what can we now assert? The Learner must be discriminating between symbols! If a Learner can discriminate between symbols then the sky is the limit. Ensure you reward both yourself and your team for a job well done!
For those that cannot touch (but can see): At least five cards may be prepared. Each of the cards depicts a different random shape which has no specific meaning. One of the cards is selected to represent the BEST. This is taught to the individual Learner through a combination of association and modelling (see below) until the Learner can select the card (without error) using a their own specific yes/no response in a 'blind' staff presentation.



In a blind presentation, the staff member concerned shuffles the cards and then presents them, one by one, face towards the Learner such that the Learner can see the card but the staff member cannot. In this way there cannot be any unintentional cueing of the Learner as to when to respond. The Staff member continues to present the cards one by one, returning rejected cards to the back of the pack, until the Learner provides his/her 'yes response' to indicate this is the card selected. Only at this point can the staff member look at the face of the card at the front of the pack. If it is the card that has been selected as BEST then the reward must be provided. If it is any other card, then the opportunity to obtain BEST is withdrawn for a specified time (at least five minutes) while something else is done.
You're joking! That's way too advanced. My Learner will simply ignore the cards altogether.
Of course it is! That is why you have to begin with the single BEST card and teach the Learner it's meaning. Once you believe that the
Learner has a grasp of the concept then you can add a second card into the mix and see if the Learner can select the one that
represents the BEST. Selection of the other card should always lead to the withdrawal of the possibility of obtaining BEST for a specified
time period.
You're joking! My Learner cannot associate a card with a BEST. She'll just sit and rock.
You may be correct but what are you doing in place of this? How do you know if you do not try? Each time you give the Learner the BEST
for a whole term ensure that the card is presented just before. You could make the card shape tactile by drawing around the shape with a
glue gun to raise its borders and then filling the shape with a sensory surface such as sand and glue and when set painting it the
appropriate colour. After a whole term you could try to ascertain if the Learner goes for that particular card when mixed in with a couple of
plain cards. If that works then add a small dot to one of the plain cards and see if the Learner can still do it. Gradually increasing the
distractors.
You're joking! My Learner cannot see.
In that case why not try it with five distinct sounds (or with tactile tops to BIGmacks to make sensory surfaces as outlined earlier)?
One of the sounds you have linked to the BEST.
Why does it have to be so abstract? Why can't I use real pictures of real things?
You can, at least for the BEST link. If you were to use pictures for the others then it might be claimed that the Learner was simply
confused and requesting the image on the card. If a Learner fails at the task as outlined it means nothing but if s/he repeatedly
succeeds then it has a great deal of meaning!
My Learner loves stars so she always goes for that one even though it is incorrect.
What you're saying is that 'stars' are a BEST! Therefore, you should not be using a star image as one of the cards but one of the cards
can lead to some starry reward!
You're joking! That's way too advanced. My Learner will simply ignore the cards altogether.
Of course it is! That is why you have to begin with the single BEST card and teach the Learner it's meaning. Once you believe that the
Learner has a grasp of the concept then you can add a second card into the mix and see if the Learner can select the one that
represents the BEST. Selection of the other card should always lead to the withdrawal of the possibility of obtaining BEST for a specified
time period.
You're joking! My Learner cannot associate a card with a BEST. She'll just sit and rock.
You may be correct but what are you doing in place of this? How do you know if you do not try? Each time you give the Learner the BEST
for a whole term ensure that the card is presented just before. You could make the card shape tactile by drawing around the shape with a
glue gun to raise its borders and then filling the shape with a sensory surface such as sand and glue and when set painting it the
appropriate colour. After a whole term you could try to ascertain if the Learner goes for that particular card when mixed in with a couple of
plain cards. If that works then add a small dot to one of the plain cards and see if the Learner can still do it. Gradually increasing the
distractors.
You're joking! My Learner cannot see.
In that case why not try it with five distinct sounds (or with tactile tops to BIGmacks to make sensory surfaces as outlined earlier)?
One of the sounds you have linked to the BEST.
Why does it have to be so abstract? Why can't I use real pictures of real things?
You can, at least for the BEST link. If you were to use pictures for the others then it might be claimed that the Learner was simply
confused and requesting the image on the card. If a Learner fails at the task as outlined it means nothing but if s/he repeatedly
succeeds then it has a great deal of meaning!
My Learner loves stars so she always goes for that one even though it is incorrect.
What you're saying is that 'stars' are a BEST! Therefore, you should not be using a star image as one of the cards but one of the cards
can lead to some starry reward!

Not all our pupils have favourites.
Please do not say that! Yes, they do. It is just that with some individuals the BEST may be very hard to discover. I remember a school that told me they had thought that a particular Learner was not motivated by anything until one day a group of musicians came to the school and this young man was sat near to the tuba player and every time he played the young man's face lit up. It was a certain frequency of sounds that was motivating. Talk to Significant Others first - they are likely to know things that may be motivating or, at least, they may suggest a possible avenue of investigation. I am always concerned when a Learner is self harming as a form of stimulation. Trying to discover something that is more motivating than poking your own eyes or slapping your own face or biting yourself (and other such behaviours) is difficult (this is covered in greater detail in a following section). Thus don't say, 'This Learner is motivated by nothing' rather state more positively, 'We haven't yet discovered what motivates this Learner but we are still trying'. There will be something it just may not be obvious!
Please do not say that! Yes, they do. It is just that with some individuals the BEST may be very hard to discover. I remember a school that told me they had thought that a particular Learner was not motivated by anything until one day a group of musicians came to the school and this young man was sat near to the tuba player and every time he played the young man's face lit up. It was a certain frequency of sounds that was motivating. Talk to Significant Others first - they are likely to know things that may be motivating or, at least, they may suggest a possible avenue of investigation. I am always concerned when a Learner is self harming as a form of stimulation. Trying to discover something that is more motivating than poking your own eyes or slapping your own face or biting yourself (and other such behaviours) is difficult (this is covered in greater detail in a following section). Thus don't say, 'This Learner is motivated by nothing' rather state more positively, 'We haven't yet discovered what motivates this Learner but we are still trying'. There will be something it just may not be obvious!
What if a Learner's BEST is not age appropriate?
So what if it isn't? If it is a favourite, it is a place to start and an entry into their world. It is not that everything in the school day will be age inappropriate or that you will be treating them in an age inappropriate way - it is possible to use age inappropriate items in an age appropriate manner. Furthermore, the goal is not to remain with this item, the goal is to use the item as a springboard for moving forward. For me, providing it's ethical and it's a platform for development then its an acceptable tool. Furthermore the guiding factor should be 'Preference Not Deference' (see section on this below for further information). However, when the inspectors are around - I wouldn't recommend the use of age inappropriate things; some inspectors tend not to like them!
My Learner has no reaction to card presentation whatsoever even when paired with his BEST.
Try making the card more tactile. Use a glue gun to outline the shape and then infill it with some appropriate sensory surface. Present the
card and assist the Learner to explore it before providing the BEST. Always provide the minimum amount of a BEST that will be still motivating to the Learner. Do this for an entire term! Try repeating the technique in the following term.
The staff are getting around the blind presentation by allowing the Learner to make multiple guesses until she gets it 'correct' and then rewarding this response. Is this wrong?
Yes! It may be OK for a short time in a teaching phase to help the Learner to see that only one specific card gets a reward but that should be a planned period of time. After this period, the staff must treat the selection of one of the other cards as a request (communicative act by the Learner) to stop the activity for (at least) five minutes and do something else instead.
My Learner's BEST is horse riding and we cannot provide that at any time.
In that instance, there are at least two things that you can do instead: select a second favourite (a second BEST) or see if access to a short video of the Learner horse riding (or some other available substitute) will act as a substitute.
The Learner gets it correct about 50% of the time but can have 'off periods'. What is the procedure in this eventuality?
The procedure is always consistent: if the Learner selects an incorrect card staff should treat it as though the Learner had said, "I'm fed up with this, let's stop for five minutes and do something else instead." If the Learner has had a seizure earlier or is known to be 'off' for whatever reason then perhaps you should not undertake the procedure, especially if it is likely that all choices at this time will not be correct. However, if you go ahead, an incorrect choice must always result in the termination of the procedure for a set period of time.
The Learner's BEST is chocolate. We can't keep feeding him chocolate all morning!
You need to review the Limiting Rules on the Fundamentals Page of this website. First, you need to establish what is the smallest amount of BEST that you can provide and yet still be motivating. Thus, it need not be a whole bar of chocolate as a reward but rather one square. Indeed, would a half of a square still suffice? What about a quarter? What about a quarter of a chocolate button? Also, once you have done this four times perhaps it's time to stop and do something else instead. If the Learner has managed to get it correct four times then 'whoopee', what a success! Party time! Furthermore, that would equate to one whole chocolate button! That's not going to make him sick or ruin his appetite. Of course, if he chooses incorrectly, the process is terminated for a period of time and no reward is given. As such, it may take a whole session to get even a fraction of a chocolate button!
Stepping Up
So the Learner succeeds at one of the above techniques after quite a long period of time. What does that prove? And what then? Well, it shows that the Learning is capable of recalling - remembering a previous event and applying that knowledge to obtain another reward. Isn't that a form of contingency awareness? Maybe at a very basic level but isn't that where we are at?
What then? Ah! Now we leave an increasing time period between presentations of the technique: first we may do it twice or more a day but then we limit it to once a day. Is the Learner still successful? OK. Now we present every two days, then three days, then once a week, once a month ... what does this tell us if the Learner is successful on each presentation? Suppose we left it an entire year and then we did it again with the Learner and s/he still got it correct?! Unlikely I know but not impossible. What we are assessing is the extent of a Learner's memory for a particular POLE.
You're crazy! My Learner will never manage any of this idea.
OK, I am crazy! If you do not believe that this has the slightest chance of succeeding no matter how it is modified for your circumstances then what about trying one of the other ideas on this page? Surely one of then has some merit for your Learner?
"As a result of methodological difficulties there is a lack of explicit knowledge about the way an individual with profound multiple disabilities expresses his feelings and preferences (Daelman, 2003; Roemer & Van Dam, 2004; Zijlstra, 2003)." (Petry & Maes, 2006, page 3)
"Several studies illustrate how to systematically examine the preferences of people with PMD (Hagopian, Long, & Rush, 2004; Hatton,
2004; Lancioni et al., 1996; Logan & Gast, 2001). These preferences can be investigated in an indirect manner (e.g., interviewing
proxies) as well as in a direct manner. In the latter, the person is given (one after the other or in pairs) several alternatives (e.g., food,
personal things, toys, sensory stimuli) and one observes if the person turns towards the stimuli or aside and how long the person focuses
on certain stimuli. It is also possible to put the person in different situations in order to determine preferences for certain postures, interactions or activities. The stimuli, objects or activities for which the person has expressed a certain preference, can subsequently be built
in into the curriculum or used as reinforcers in a learning process." (Petry et al, 2007c, page 135)
So what if it isn't? If it is a favourite, it is a place to start and an entry into their world. It is not that everything in the school day will be age inappropriate or that you will be treating them in an age inappropriate way - it is possible to use age inappropriate items in an age appropriate manner. Furthermore, the goal is not to remain with this item, the goal is to use the item as a springboard for moving forward. For me, providing it's ethical and it's a platform for development then its an acceptable tool. Furthermore the guiding factor should be 'Preference Not Deference' (see section on this below for further information). However, when the inspectors are around - I wouldn't recommend the use of age inappropriate things; some inspectors tend not to like them!
My Learner has no reaction to card presentation whatsoever even when paired with his BEST.
Try making the card more tactile. Use a glue gun to outline the shape and then infill it with some appropriate sensory surface. Present the
card and assist the Learner to explore it before providing the BEST. Always provide the minimum amount of a BEST that will be still motivating to the Learner. Do this for an entire term! Try repeating the technique in the following term.
The staff are getting around the blind presentation by allowing the Learner to make multiple guesses until she gets it 'correct' and then rewarding this response. Is this wrong?
Yes! It may be OK for a short time in a teaching phase to help the Learner to see that only one specific card gets a reward but that should be a planned period of time. After this period, the staff must treat the selection of one of the other cards as a request (communicative act by the Learner) to stop the activity for (at least) five minutes and do something else instead.
My Learner's BEST is horse riding and we cannot provide that at any time.
In that instance, there are at least two things that you can do instead: select a second favourite (a second BEST) or see if access to a short video of the Learner horse riding (or some other available substitute) will act as a substitute.
The Learner gets it correct about 50% of the time but can have 'off periods'. What is the procedure in this eventuality?
The procedure is always consistent: if the Learner selects an incorrect card staff should treat it as though the Learner had said, "I'm fed up with this, let's stop for five minutes and do something else instead." If the Learner has had a seizure earlier or is known to be 'off' for whatever reason then perhaps you should not undertake the procedure, especially if it is likely that all choices at this time will not be correct. However, if you go ahead, an incorrect choice must always result in the termination of the procedure for a set period of time.
The Learner's BEST is chocolate. We can't keep feeding him chocolate all morning!
You need to review the Limiting Rules on the Fundamentals Page of this website. First, you need to establish what is the smallest amount of BEST that you can provide and yet still be motivating. Thus, it need not be a whole bar of chocolate as a reward but rather one square. Indeed, would a half of a square still suffice? What about a quarter? What about a quarter of a chocolate button? Also, once you have done this four times perhaps it's time to stop and do something else instead. If the Learner has managed to get it correct four times then 'whoopee', what a success! Party time! Furthermore, that would equate to one whole chocolate button! That's not going to make him sick or ruin his appetite. Of course, if he chooses incorrectly, the process is terminated for a period of time and no reward is given. As such, it may take a whole session to get even a fraction of a chocolate button!
Stepping Up
So the Learner succeeds at one of the above techniques after quite a long period of time. What does that prove? And what then? Well, it shows that the Learning is capable of recalling - remembering a previous event and applying that knowledge to obtain another reward. Isn't that a form of contingency awareness? Maybe at a very basic level but isn't that where we are at?
What then? Ah! Now we leave an increasing time period between presentations of the technique: first we may do it twice or more a day but then we limit it to once a day. Is the Learner still successful? OK. Now we present every two days, then three days, then once a week, once a month ... what does this tell us if the Learner is successful on each presentation? Suppose we left it an entire year and then we did it again with the Learner and s/he still got it correct?! Unlikely I know but not impossible. What we are assessing is the extent of a Learner's memory for a particular POLE.
You're crazy! My Learner will never manage any of this idea.
OK, I am crazy! If you do not believe that this has the slightest chance of succeeding no matter how it is modified for your circumstances then what about trying one of the other ideas on this page? Surely one of then has some merit for your Learner?
"As a result of methodological difficulties there is a lack of explicit knowledge about the way an individual with profound multiple disabilities expresses his feelings and preferences (Daelman, 2003; Roemer & Van Dam, 2004; Zijlstra, 2003)." (Petry & Maes, 2006, page 3)
"Several studies illustrate how to systematically examine the preferences of people with PMD (Hagopian, Long, & Rush, 2004; Hatton,
2004; Lancioni et al., 1996; Logan & Gast, 2001). These preferences can be investigated in an indirect manner (e.g., interviewing
proxies) as well as in a direct manner. In the latter, the person is given (one after the other or in pairs) several alternatives (e.g., food,
personal things, toys, sensory stimuli) and one observes if the person turns towards the stimuli or aside and how long the person focuses
on certain stimuli. It is also possible to put the person in different situations in order to determine preferences for certain postures, interactions or activities. The stimuli, objects or activities for which the person has expressed a certain preference, can subsequently be built
in into the curriculum or used as reinforcers in a learning process." (Petry et al, 2007c, page 135)
54. Favour the Furtherance of Functional over Form-al Frameworks

"The results of this study provide insight into the effects of a functional movement curriculum when compared with a regular programme offered to children with PIMD who attend a CSE (Centre for Special Education). The general conclusion is that a functional movement curriculum such as MOVE may possibly have added value for children with PIMD in acquiring independence when performing movement skills and that a curriculum such as MOVE could form part of the total package of activities and interventions within a CSE. This has clear implications for practice with regard to both the content and organizational aspects of care for children with PIMD. In concrete terms, this means the possible integration of functional activities within the entire day programme, performed by all the child’s DSP (Direct Support Provider) and directed towards specific measurable goals set within a multidisciplinary framework. Despite the apparently limited possibilities of this group of children, the interventions offered should be directed towards increasing the independence of the child, although this may appear minimal. For example, by enabling a child to move small distances himself with only the support of a walking frame gives him a great deal of say over where, when and with whom he wants to be, and whether he wants to participate in a group activity. Thus a limited increase in independence, possibly achieved through a programme such as MOVE, has a great effect on a child when directed towards the acquisition of autonomy and control over his own life." (Van Putten, 2005)
55. Food for Thought: Diet and Nutrition

As we have seen in an earlier section, the brain has 'plasticity' throughout its lifetime. It can adapt its structure in a number of ways in response to environmental experiences under optimal conditions. There is no reason to doubt that this applies to all Individuals including those experiencing PMLD. To believe otherwise is to state that IEPMLD are incapable of learning anything at all which, if you are studying this webpage, is a belief that you are very unlikely to hold. Therefore, although, by definition, the learning of this group of people is profoundly impaired as a result of some previous trauma to the structure and function of the brain, it does not follow that, in providing optimal conditions for learning, some amelioration of the cognitive condition is not possible.
The adult brain weighs approximately three pounds which is around 2% of body weight and yet it uses around 25% of the calories a person consumes, 25% of the total blood flow in the body, and 20% of the oxygen breathed (Perretta, 2001; Amen, 2010).
"There are some foods that increase neurogenesis and support brain health and therefore helpful to include in your diet. There are other foods that it would be wise to avoid or minimize as they decrease neurogenesis." (Cortright, 2015, page 37)
Nutrition
The adult brain weighs approximately three pounds which is around 2% of body weight and yet it uses around 25% of the calories a person consumes, 25% of the total blood flow in the body, and 20% of the oxygen breathed (Perretta, 2001; Amen, 2010).
"There are some foods that increase neurogenesis and support brain health and therefore helpful to include in your diet. There are other foods that it would be wise to avoid or minimize as they decrease neurogenesis." (Cortright, 2015, page 37)
Nutrition
56. Cognitive Milestones

The Cognitive Development Chart (CDC) below is an attempt to map out cognitive milestones for IEPMLD assuming an operational level of 0 - 2 years of age. It is inclusive of social and emotional development although typically this is dealt with separately to cognition. While the chart implies a sequenced developmental pathway with one skills building on another there is no claim that this, in fact, is the case: indeed, while some skills are dependent on the development of other areas (skill building on skill) the different levels portrayed are more likely to run parallel than in series although the development of the senses necessarily precedes the other items listed.
It should further be noted that their is no claim that each branch of the chart is comprehensive and that nothing has been missed although Talksense has tried to be as thorough as possible.
The dotted lines represent some fundamental inter- and intra-level connections although there are many connections not shown; indeed, so many as to make it a tangle of lines were they to be depicted! Thus, it does not follow that simply because a connecting line does not appear there is no connection between any two (or more items).
The three dotted lines to the left of the CDC represent domains of skill that flow throughout all the areas. For example, physical (motor skills) development impacts all areas and its impairment may have significant consequences for each item. In addition to these three areas, the notion of awareness also pervades all areas. Awareness necessarily implies alertness, focus, and wakefulness for, without these, learning is seriously diminished if not eradicated. Environmental and social distractions are detrimental to attention to topic and therefore to comprehension and to learning. Thus, 'awareness' is a factor in all areas.
While IEPMLD in Further Education are likely to be 18 years or older, by definition they will not be operating at a cognitive level commensurate with their physical age. It is generally considered (see early this page for definition of IEPMLD) that they are operational in Piaget's 'sensory motor' stage (Piaget, 1952) which runs from birth through till 24 months (0 - 2 years). Indeed, Talksense would state that the majority of IEPMLD are operating up to an earlier level (0 -1 year) although still within the sensory motor stage. However, as they have had an additional 16 plus years of experiences there can be significant differences between individuals in both awareness and ability.
Each item will be outlined further in the section below the chart. Should you have any suggestions for modifications to the chart please use the form provided towards the bottom of this page.
It should further be noted that their is no claim that each branch of the chart is comprehensive and that nothing has been missed although Talksense has tried to be as thorough as possible.
The dotted lines represent some fundamental inter- and intra-level connections although there are many connections not shown; indeed, so many as to make it a tangle of lines were they to be depicted! Thus, it does not follow that simply because a connecting line does not appear there is no connection between any two (or more items).
The three dotted lines to the left of the CDC represent domains of skill that flow throughout all the areas. For example, physical (motor skills) development impacts all areas and its impairment may have significant consequences for each item. In addition to these three areas, the notion of awareness also pervades all areas. Awareness necessarily implies alertness, focus, and wakefulness for, without these, learning is seriously diminished if not eradicated. Environmental and social distractions are detrimental to attention to topic and therefore to comprehension and to learning. Thus, 'awareness' is a factor in all areas.
While IEPMLD in Further Education are likely to be 18 years or older, by definition they will not be operating at a cognitive level commensurate with their physical age. It is generally considered (see early this page for definition of IEPMLD) that they are operational in Piaget's 'sensory motor' stage (Piaget, 1952) which runs from birth through till 24 months (0 - 2 years). Indeed, Talksense would state that the majority of IEPMLD are operating up to an earlier level (0 -1 year) although still within the sensory motor stage. However, as they have had an additional 16 plus years of experiences there can be significant differences between individuals in both awareness and ability.
Each item will be outlined further in the section below the chart. Should you have any suggestions for modifications to the chart please use the form provided towards the bottom of this page.
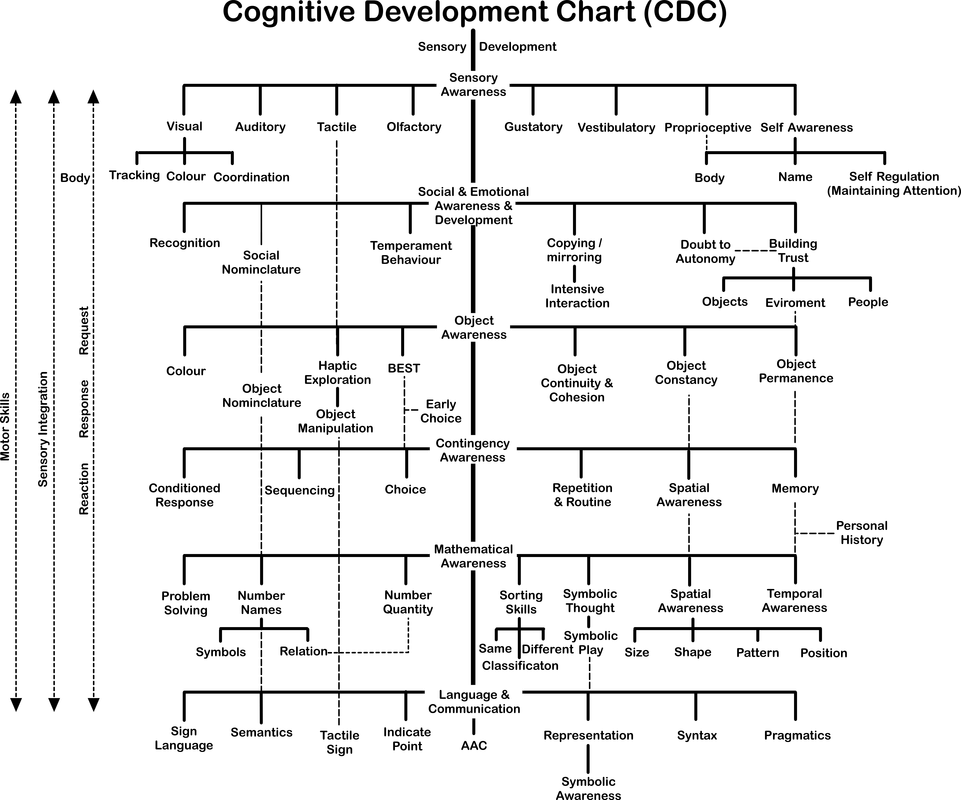
Although we typically state five senses when we think about them there are several more; the chart lists eight although there is no claim that this is all there is. It is common for IEPMLD to have impairment of one or more of the senses; for example, there may be a hearing loss or an issue with visual acuity. However, it is less common for there to be a total loss of a sense altogether, even people who are registered blind can usually detect light and many can see images albeit somewhat out of focus. It is therefore important to assess (or have assessed) each of the senses such that you are better able to produce teaching materials suited to the abilities and and needs of the individual Learner.
One of the first things that it is important to do is to assess a Learner's sensory awareness. The Reaction Response Request vertical dotted line reinforces this fact - we need a reaction to sensory stimuli first of all. For vision this might be as simple as increasing the intensity of a light source to see if the Learner's pupil react by getting smaller (For visual assessment see Aitken & Buultjens, 1992). Following a reaction we need a response. This necessarily involves the individual learner indicating an 'awareness'; for example, the individual can respond visually to light bouncing off the surface off an object by tracking it with her/his eyes as it moves through her/his visual field or by reaching out and grasping it demonstrating hand eye coordination. While no response does NOT necessarily equate to a lack of cognition (or, alternatively, in this case, vision)(absence of evidence is not evidence of absence) a positive response does begin to tell us something about the comprehension of the Learner.
In a similar fashion, we can gauge a reaction to sounds (auditory), tactile sensations, smells (Olfactory), and tastes (gustatory): does the Individual react in anyway (changes in body language, for example) to these sensory stimuli? How strong is the reaction? What happens if we change the intensity of the sensory stimuli? Or its duration? Or (for tactile reactions) its location on the body?
In addition to the five main senses there is also the proprioceptive sense, sometimes referred to as the sixth sense, which informs us of our body position in space. It is typically tested by external manipulation of a specific part of an individual's body by another while said individual
is blindfolded or otherwise unable to see what is happening. For example, the foot might be moved in a specific direction and the individual asked to report on the direction of movement without actually being able to see it moving just by the sensation alone. However, such a test would not be appropriate for IEPMLD, the Learner's inability to self-report being one among many reasons for this. Nevertheless, it may be possible to test basic proprioceptive awareness by utilisation of a BEST (Best Ever Stimulating Thing) in a shielded-from-vision experiment. For example, a Learner could be shown a BEST and it could be placed in reach. If:
As the assessment of reaction and response to sensory stimuli in IEPMLD is very likely to be confounded by other physical and sensory issues as well as by communication difficulties it will be difficult to state with 100% certainty a lack of ability in one specific area. However, if the Individual is able to perform positively on more than one occasion (eliminating the possibility of a mere accidental chance result) it is evidence for the contrary; awareness and ability in sensory discrimination of stimuli. Of course, mere observation of individual behaviour may also tell speak volumes in this respect too, providing that is, the behaviour which evidences the awareness and or ability cannot be explained by another rationale.
The vestibulatory sense is the sense of balance which is often compromised in IEPMLD (see Horak et al., 1988)(but, again, confounded by other physical and sensory issues). Individuals may not be able to maintain a stable position when seated, for example, without support. There is evidence that the vestibulatory sense (as well as other senses) can be 'replaced' (or rather 'substituted') by the utilisation of a neuroplasticity technique know as 'sensory substitution' (Strupp et al., 1998; Bagadia et al., 2001; Bach-y-Rita & Kercel, 2003). Cheryl Schiltz had been given an antibiotic drug during a hospital stay for a routine operation and lost almost her entire vestibulatory system. However, on working with Paul Bach-y-Rita using sensory substitution techniques she was able to function normally again (see Doidge 2007, Chapter One):
One of the first things that it is important to do is to assess a Learner's sensory awareness. The Reaction Response Request vertical dotted line reinforces this fact - we need a reaction to sensory stimuli first of all. For vision this might be as simple as increasing the intensity of a light source to see if the Learner's pupil react by getting smaller (For visual assessment see Aitken & Buultjens, 1992). Following a reaction we need a response. This necessarily involves the individual learner indicating an 'awareness'; for example, the individual can respond visually to light bouncing off the surface off an object by tracking it with her/his eyes as it moves through her/his visual field or by reaching out and grasping it demonstrating hand eye coordination. While no response does NOT necessarily equate to a lack of cognition (or, alternatively, in this case, vision)(absence of evidence is not evidence of absence) a positive response does begin to tell us something about the comprehension of the Learner.
In a similar fashion, we can gauge a reaction to sounds (auditory), tactile sensations, smells (Olfactory), and tastes (gustatory): does the Individual react in anyway (changes in body language, for example) to these sensory stimuli? How strong is the reaction? What happens if we change the intensity of the sensory stimuli? Or its duration? Or (for tactile reactions) its location on the body?
In addition to the five main senses there is also the proprioceptive sense, sometimes referred to as the sixth sense, which informs us of our body position in space. It is typically tested by external manipulation of a specific part of an individual's body by another while said individual
is blindfolded or otherwise unable to see what is happening. For example, the foot might be moved in a specific direction and the individual asked to report on the direction of movement without actually being able to see it moving just by the sensation alone. However, such a test would not be appropriate for IEPMLD, the Learner's inability to self-report being one among many reasons for this. Nevertheless, it may be possible to test basic proprioceptive awareness by utilisation of a BEST (Best Ever Stimulating Thing) in a shielded-from-vision experiment. For example, a Learner could be shown a BEST and it could be placed in reach. If:
- the Learner is able to move a hand and arm to obtain the item and;
- the arm could is deliberately deflected from its path by a staff member (left or right, up or down) and;
- the Learner's view of the correct adjustment is blocked at this point and;
- the Learner correctly moves his/her arm towards the item;
As the assessment of reaction and response to sensory stimuli in IEPMLD is very likely to be confounded by other physical and sensory issues as well as by communication difficulties it will be difficult to state with 100% certainty a lack of ability in one specific area. However, if the Individual is able to perform positively on more than one occasion (eliminating the possibility of a mere accidental chance result) it is evidence for the contrary; awareness and ability in sensory discrimination of stimuli. Of course, mere observation of individual behaviour may also tell speak volumes in this respect too, providing that is, the behaviour which evidences the awareness and or ability cannot be explained by another rationale.
The vestibulatory sense is the sense of balance which is often compromised in IEPMLD (see Horak et al., 1988)(but, again, confounded by other physical and sensory issues). Individuals may not be able to maintain a stable position when seated, for example, without support. There is evidence that the vestibulatory sense (as well as other senses) can be 'replaced' (or rather 'substituted') by the utilisation of a neuroplasticity technique know as 'sensory substitution' (Strupp et al., 1998; Bagadia et al., 2001; Bach-y-Rita & Kercel, 2003). Cheryl Schiltz had been given an antibiotic drug during a hospital stay for a routine operation and lost almost her entire vestibulatory system. However, on working with Paul Bach-y-Rita using sensory substitution techniques she was able to function normally again (see Doidge 2007, Chapter One):
Re-mapping sensory information within the brain using sensory substitution is something that has been utilised in special education for some time albeit in a somewhat limited fashion. For example, tactile sign language uses this technique to enhance communication. There is scope for much more use to be made of sensory substitution especially with the progression of technology making it more readily available at an affordable price.
Self-awareness concludes the set of sensory awareness detailed in the CDC. As this is covered in a separate section of this page it will not be expanded further here. However, emanating from the self awareness branch are at least three sub-sections: body, name, and self-regulation. 'Body' relates to awareness of the various parts of one's own body (head, and shoulders, knees, and toes ... as the song goes) and as such connects also to the proprioceptive section. 'Name' relates to the ability to the awareness of and the ability to respond to one's own name. Self-regulation refers to the ability to control your impulses and to maintain focus, attending to the subject in hand and not to be distracted every other moment by other extraneous stimuli. This is particularly difficult for many IEPMLD (Crosby & Blatt, 1968; Fox & Wade, 1998; Fernandez-Jaen, 2006).
In addition to impairment of one or more of the senses there might also be a problem of Sensory Integration (See the work of Jean Ayers) as denoted by the vertical dotted line to the left of the chart. As this is covered in a separate section of this webpage it will not be detailed further here.
The next section of the Cognitive Development Chart details some aspects of social and emotional awareness and development.
Ability to recognise/sense an occurrence/stimuli
Ability to respond to an occurrence/stimuli
Object Constancy: The knowledge that an object remains the same despite changes in how it is viewed (for example: changes in perspective or distance)
Object Continuity and Cohesion: The knowledge that objects are cohesive entities and
Object Permanence: The knowledge that an object continues to exist in both time and space even when it can no longer be 'sensed' (seen, heard, ...)
Contingency Awareness
Selection of items: Preference: Choice:
Sensory Awareness: ability to recognise a stimulus; ability to respond consistently to a stimulus
Object Representation: Object Constancy; Object Continuity and Cohesion; Object Permanence
Social Representation: Knowledge of People - feature recognition; emotional recognition;
Mathematical Representation: Awareness of number
Contingency Awareness:
Conceptual Awareness:
Spatial awareness:
Differentiation: tell objects apart, know that one is bigger, taller, heavier ...
Thinking is different at different stages of development Piaget Sensory Motor stage (0 - 2 years)
BEST under coloured translucent beakers find the lady. How do you put a BIG BEST or a abstract BEST under a beaker?
Contact Comfort (See the work of Harry Harlow)
Erik Erikson Trust vs Mistrust (Erikson, E.H. (1950). Childhood and society. WW Norton & Company.)
Autonomy Vs Doubt (Independence: do it yourself Vs I can't do that; wary of different; it's not safe; ...)
Self-awareness concludes the set of sensory awareness detailed in the CDC. As this is covered in a separate section of this page it will not be expanded further here. However, emanating from the self awareness branch are at least three sub-sections: body, name, and self-regulation. 'Body' relates to awareness of the various parts of one's own body (head, and shoulders, knees, and toes ... as the song goes) and as such connects also to the proprioceptive section. 'Name' relates to the ability to the awareness of and the ability to respond to one's own name. Self-regulation refers to the ability to control your impulses and to maintain focus, attending to the subject in hand and not to be distracted every other moment by other extraneous stimuli. This is particularly difficult for many IEPMLD (Crosby & Blatt, 1968; Fox & Wade, 1998; Fernandez-Jaen, 2006).
In addition to impairment of one or more of the senses there might also be a problem of Sensory Integration (See the work of Jean Ayers) as denoted by the vertical dotted line to the left of the chart. As this is covered in a separate section of this webpage it will not be detailed further here.
The next section of the Cognitive Development Chart details some aspects of social and emotional awareness and development.
Ability to recognise/sense an occurrence/stimuli
Ability to respond to an occurrence/stimuli
Object Constancy: The knowledge that an object remains the same despite changes in how it is viewed (for example: changes in perspective or distance)
Object Continuity and Cohesion: The knowledge that objects are cohesive entities and
Object Permanence: The knowledge that an object continues to exist in both time and space even when it can no longer be 'sensed' (seen, heard, ...)
Contingency Awareness
Selection of items: Preference: Choice:
Sensory Awareness: ability to recognise a stimulus; ability to respond consistently to a stimulus
Object Representation: Object Constancy; Object Continuity and Cohesion; Object Permanence
Social Representation: Knowledge of People - feature recognition; emotional recognition;
Mathematical Representation: Awareness of number
Contingency Awareness:
Conceptual Awareness:
Spatial awareness:
Differentiation: tell objects apart, know that one is bigger, taller, heavier ...
Thinking is different at different stages of development Piaget Sensory Motor stage (0 - 2 years)
BEST under coloured translucent beakers find the lady. How do you put a BIG BEST or a abstract BEST under a beaker?
Contact Comfort (See the work of Harry Harlow)
Erik Erikson Trust vs Mistrust (Erikson, E.H. (1950). Childhood and society. WW Norton & Company.)
Autonomy Vs Doubt (Independence: do it yourself Vs I can't do that; wary of different; it's not safe; ...)
57. I
58. J
59. K
60. L
61. M
62. N
63. O
64. P
65. Q
66. R
67. S
68. T
69. U
70. V
71. W
72. X
73. J
74. K
75. L
76. M
77. N
78. O
79. P
80. Q
81. R
82. Sensing, Specifying, and Stating (documenting) Signs of Significance

Last night I had a dream as we all do every night. I awoke during the dream and continued my thoughts into a semi-awoken state; again, as I suspect the majority of people experience. However, what was special about this dream was that it was set in a special education establishment and involved real people with whom I had experience in an interaction which I recognised was meaningful and, because I awoke during the dream, I remembered it and it wasn't lost in sleep as countless others are. Furthermore, the events in the dream were significant in that I realised it wasn't just a silly dream but that it had meaning in the context of this page. Thus, I find myself very early in the morning (4 am), sitting at my computer writing down the an idea that came to me in a dream! I was disappointed to realise, after waking fully, the events that took place were only a dream and didn't happen for real but then it occurred to me that it didn't matter; the notion was of importance and it should be recorded.
In the dream I am in a special educational establishment observing practice as I have often done. There was a female support assistant interacting with a young lady who was an Individual Experiencing PMLD (IEPMLD). The support assistant called the young lady Caroline. 'Caroline' was being particularly uncooperative in the transition from one session to another and the support assistant said something like, "Caroline, if you don't get going I am going to have to get another member of staff to work with me to take you to X" ('X' because I forget where she said they were going). At which point Caroline walked off (she was ambulant) and said quite distinctly, "Oh no, not two!". The support assistant continue to try to assist her and everything continued as previously. I shouted 'stop'! I asked the support assistant what had just happened and what was it's significance. I got a blank look. Had I not been present that moment would have been lost in among countless other moments during the working day and its significance never spotted and never recorded. Perhaps Caroline wold never demonstrate such abilities again and staff would never realise her potential.
OK it was just a dream. OK it is highly improbable that an IEPMLD would suddenly begin to talk. However, let's pretend that it was real scenario and something similar had just happened in the workplace, what is the significance? Write down the significant factors and them compare them with the list below ...
Your scenario is stupid. My Learners don't speak and they don't have mathematical abilities at the level you are stating.
I said it was a dream and that IEPMLD by definition don't operate at that level. With respect, you are missing the point. The point is that staff sometimes miss significant situations (memorable moments) and if they are missed they may be lost forever in the hurly-burly of the day.
Yes but how do you know what is significant?
If the behaviour is commonplace, in that the Learner does it all the time and is not unusual then it isn't likely to be significant. However, if it is a one off or out of the ordinary or in any way unusual then it should be recorded. Staff need not worry about a particular behaviour's significance; if they are unsure they should record it anyway. The class teacher (or the person with responsibility for monitoring Caroline's progress) has the ultimate say on an item's significance: staff should monitor, record, and pass the information through the establishment's channels. All staff should receive training in this area.
I haven't got time to be recording every nuance of learner behaviour. The job is demanding enough as it is. How can I just put a learner 'on hold' while I sit down and write out a report. That's crazy!
Admittedly, if you are responsible for a Learner and cannot leave that person's side for a minute or more you are not going to be able to record in real time; it is not a realistic expectation. However, you may be in an environment (such as an enclosed classroom) with other staff and be able to create some time to record significant behaviour while leaving a Learner for a short time with safety. Recording of significant situation should be made simple to ease this process for staff; for example the session plan (which should be available to all during a session) could be annotated. All staff should be aware of the system in place for recording such moments and encouraged to use it. Remember, the reason you are working in an educational establishment is to educate, to progress a Learner to be better able to cope with the events that they are likely to meet in their lives. A major part of that role is to record progress. So you should record situations you consider to be significant even if that means you have to do it during a break after the event.
What happens, as in your scenario, if a member of staff misses a significant occurrence?
Nothing happens; it is missed! If another person happens to witness it they can ask the staff member concerned to analyse what had just taken place but, if no one else witnessed it, it will be lost forever unless the Learner repeats the behaviour at another time when it is noticed and recorded.
In the dream I am in a special educational establishment observing practice as I have often done. There was a female support assistant interacting with a young lady who was an Individual Experiencing PMLD (IEPMLD). The support assistant called the young lady Caroline. 'Caroline' was being particularly uncooperative in the transition from one session to another and the support assistant said something like, "Caroline, if you don't get going I am going to have to get another member of staff to work with me to take you to X" ('X' because I forget where she said they were going). At which point Caroline walked off (she was ambulant) and said quite distinctly, "Oh no, not two!". The support assistant continue to try to assist her and everything continued as previously. I shouted 'stop'! I asked the support assistant what had just happened and what was it's significance. I got a blank look. Had I not been present that moment would have been lost in among countless other moments during the working day and its significance never spotted and never recorded. Perhaps Caroline wold never demonstrate such abilities again and staff would never realise her potential.
OK it was just a dream. OK it is highly improbable that an IEPMLD would suddenly begin to talk. However, let's pretend that it was real scenario and something similar had just happened in the workplace, what is the significance? Write down the significant factors and them compare them with the list below ...
- Caroline spoke! I know it's very unlikely to happen simply by definition for an IEPMLD but, in the context of this scenario and this exercise, it is of high significance.
- Caroline understood what the Support Assistant was saying.
- Caroline can hear or she can lip read.
- Caroline has basic number concept; she was able to calculate 'one more than one' and reach the correct answer.
- Caroline has opinions of her own on how she is treated.
- all staff should record significant events.
- in the scenario the member of staff did not spot the significance.
Your scenario is stupid. My Learners don't speak and they don't have mathematical abilities at the level you are stating.
I said it was a dream and that IEPMLD by definition don't operate at that level. With respect, you are missing the point. The point is that staff sometimes miss significant situations (memorable moments) and if they are missed they may be lost forever in the hurly-burly of the day.
Yes but how do you know what is significant?
If the behaviour is commonplace, in that the Learner does it all the time and is not unusual then it isn't likely to be significant. However, if it is a one off or out of the ordinary or in any way unusual then it should be recorded. Staff need not worry about a particular behaviour's significance; if they are unsure they should record it anyway. The class teacher (or the person with responsibility for monitoring Caroline's progress) has the ultimate say on an item's significance: staff should monitor, record, and pass the information through the establishment's channels. All staff should receive training in this area.
I haven't got time to be recording every nuance of learner behaviour. The job is demanding enough as it is. How can I just put a learner 'on hold' while I sit down and write out a report. That's crazy!
Admittedly, if you are responsible for a Learner and cannot leave that person's side for a minute or more you are not going to be able to record in real time; it is not a realistic expectation. However, you may be in an environment (such as an enclosed classroom) with other staff and be able to create some time to record significant behaviour while leaving a Learner for a short time with safety. Recording of significant situation should be made simple to ease this process for staff; for example the session plan (which should be available to all during a session) could be annotated. All staff should be aware of the system in place for recording such moments and encouraged to use it. Remember, the reason you are working in an educational establishment is to educate, to progress a Learner to be better able to cope with the events that they are likely to meet in their lives. A major part of that role is to record progress. So you should record situations you consider to be significant even if that means you have to do it during a break after the event.
What happens, as in your scenario, if a member of staff misses a significant occurrence?
Nothing happens; it is missed! If another person happens to witness it they can ask the staff member concerned to analyse what had just taken place but, if no one else witnessed it, it will be lost forever unless the Learner repeats the behaviour at another time when it is noticed and recorded.
83. T
84. U
85. V
86. W
87. Personally Caring about Personal Care

It is known that a lack of toileting skills is one of the difficulties that characterise IEPMLD and, thus, it is likely that support staff will be involved in personal care at least twice a day if not more frequently (Smith, 1996; Carnaby, & Cambridge, 2002; Matson et al., 2011). The quality of the personal care provided in any establishment is important not only to ensure the elimination of any possibility of abuse (Cambridge & Carnaby, 2000) but also to to try to ensure that such experiences are always positive. Furthermore, any regular occurrence, occupying more than a few minutes each day, is to be seen as an educational opportunity worthy of exploitation for cognitive amelioration. Thus, personal care should be viewed as an integral part of the educational curriculum for IEPMLD.
88. The Significance of Significant Others
"Supporting people with PMD involves many people who must cooperate intensively (Petry et al., 2007d; Vlaskamp, 1999; Zijlstra, 2003). This presupposes a shared responsibility and a full partnership between parents and professional support staff. Parents have acquired very important expertise with regard to their child, which is why it is important that their experience and expertise is exchanged with professional support staff and that it is taken seriously. It is necessary that parents and professional support staff pass on information to each other because of the person’s limited communicative abilities. In addition, parents want to have a say in the support process and to participate in deciding which objectives will be worked on and what shape and content will be given to their child’s support. Finally, sound communication between parents and professional support staff is essential for tuning the context of family, school and support in to one another and for enriching the parent’s and professional support staff’s competence in giving sensitive support to the person with PMD (Owen, Ware, & Barfoot, 2000)." (Petry & Maes, 2007)
How are Significant Others involved in the education provision of your place of work? Do they contribute on a regular basis?
How are Significant Others involved in the education provision of your place of work? Do they contribute on a regular basis?
89. It's Just a Symbolic Gesture ...
individuals with PMLD often possess limited interaction skills and may never be able to use symbolic communication strategies (Bloomberg, Johnson & West 2004).
90. Water, Water Everywhere but ...

This section is not about using water as a sensory medium (important though that may be), nor is it about the utilisation of water in hydrotherapy (definitely important), rather this section concerns itself with drinking water.
"If our bodies are 70% water, and if our brains are 75-80% water there must be a very good reason. Brains get 20% of the blood supply from every beat of the heart and they’re only about 2% of our body mass. This high investment in a single organ is important because water is an essential element in neurological transmissions." (Pugh, 2011a)
There is a growing amount of research evidence that supports the premise that the consumption of water is really important in cognitive functioning (Sharma et al, 1986; Gopinathan et al, 1988; Cian et al, 2000; Rogers et al, 2001; Wilson & Morley, 2003; Suhr et al, 2004; Bar-David et al, 2005; Szinnai et al, 2005; Baker et al, 2007; Grandjean, 2007; Lieberman, 2007; Tomporowski et al, 2007; Benton & Burgess, 2009; Edmonds et al, 2009; Suhr et al, 2010; EFSA, 2011; Ganio et al, 2011; Kempton et al, 2011; Armstrong et al, 2012; Booth et al, 2012; Fadda et al, 2012; Lieberman, 2012; Edmonds et al, 2013; Pawson et al. 2013; Masento et al, 2014; Hydration For Health, 2015). The following video from Dr. Michael Greger of NutritionFacts.org (YouTube https://www.youtube.com/watch?v=72Jcvsk3A-g) states the case concisely ...
"If our bodies are 70% water, and if our brains are 75-80% water there must be a very good reason. Brains get 20% of the blood supply from every beat of the heart and they’re only about 2% of our body mass. This high investment in a single organ is important because water is an essential element in neurological transmissions." (Pugh, 2011a)
There is a growing amount of research evidence that supports the premise that the consumption of water is really important in cognitive functioning (Sharma et al, 1986; Gopinathan et al, 1988; Cian et al, 2000; Rogers et al, 2001; Wilson & Morley, 2003; Suhr et al, 2004; Bar-David et al, 2005; Szinnai et al, 2005; Baker et al, 2007; Grandjean, 2007; Lieberman, 2007; Tomporowski et al, 2007; Benton & Burgess, 2009; Edmonds et al, 2009; Suhr et al, 2010; EFSA, 2011; Ganio et al, 2011; Kempton et al, 2011; Armstrong et al, 2012; Booth et al, 2012; Fadda et al, 2012; Lieberman, 2012; Edmonds et al, 2013; Pawson et al. 2013; Masento et al, 2014; Hydration For Health, 2015). The following video from Dr. Michael Greger of NutritionFacts.org (YouTube https://www.youtube.com/watch?v=72Jcvsk3A-g) states the case concisely ...
In addition, a drink of water has been shown to increase subjective happiness, memory, motor skills, improve attention, enhance arousal, increase alertness, speed reaction time, and decrease confusion (Neave et al, 2001; Benton & Burgess, 2009; Edmonds & Burford, 2009; Edmonds & Jeffes, 2009; Booth et al, 2012; Fadda et al, 2012; Edmonds, Crombie, & Gardner, 2013; Pawson et al, 2013; Pross et al, 2013) while a lack of water can result in fatigue, tiredness, and general inattention (D’anci et al, 2009; Shirreffs et al, 2004; Szinnai et al, 2005; Petri et al, 2006).
"Poor hydration at any time affects how well a child's brain operates and his or her learning ability. At school hydration is imperative to achieving a teacher’s learning objectives. If kids are slightly dehydrated they may appear tired, complain of headaches and have a reduced ability to concentrate, and if they are usually like this they might know no different and think they feel normal. If a child actually feels thirsty then his or her mental performance has already got to the level about 10 per cent lower than before and mental performance deteriorates
progressively as the degree of dehydration increases. " (Pugh, 2011a)
While water is good for us, too many sugary drinks, are not:
"All of the popular energy drinks in the market have different variations of caffeine, and most of these drinks are not considered healthy for the human body. Most of these energy drinks should be watched carefully due to the unbalanced ingredients, especially sugar and caffeine in their compositions (Miller, 2008). Most energy drinks also stimulate and trigger reactions that can increase blood pressure, heart rate or alter glycemic levels. These can often prevent normal sleep cycles and dehydrate the body." (González et al, 2012)
A 2017 study by Pase et al compared data from 4,000 participants and then divided them into two groups: The first group contained people who consumed one or two sugary drinks each day, which included fruit juice, soda, or other soft drinks. The second group did not drink any sugary beverages. The researchers found that those people who consumed up to two sugary drinks daily had reduced brain volume, a significantly smaller hippocampus, and performed worse on memory tests. Furthermore, the situation doesn't appear to get better if you switch to diet sodas, Pase et al (2017) found that older adults who drank artificially sweetened beverages regularly were more likely to have a stroke or develop Alzheimer's disease over 10 years.
However, limited intake of sugar can have beneficial effects:
"Avoiding tooth decay, diabetes, and obesity are all good reasons to limit consumption of sugar in the human diet. But sugar consumption, even in high amounts, does not contribute to hyperactivity, inattention, juvenile delinquency, reductions in cognitive performance, or other behavior problems in children or adults. Instead, a high level of glucose, or sugar, consumption actually improves athletic, academic, and cognitive performance, and may enhance self-control. Unless medically prescribed for non-behavioral reasons, dietary restriction of sugar intake is inappropriate and may have unintended behavioral effects (e.g., Fisher & Birch, 1999), create unnecessary interpersonal conflict, and be counterproductive by precluding consideration and implementation of proven effective interventions for behavioral and performance problems, such as behavior therapy as treatment for attention-deficit/hyperactivity disorder." (Flora & Polenick, 2013)
However (!), the above pertains to glucose and not to fructose (high fructose corn syrup) which tends to be the main sweetener in many sweetened beverages as it is cheap to produce in quantity. Sugar comes in many forms (the '-oses') glucose, fructose, sucrose, lactose, maltose, etc. There is a difference between the way glucose and fructose interact with the human body (Lustig, 2013) with fructose being compared to 'alcohol without the buzz' (Lustig, 2013b). Indeed, Lustig pulls no punches in calling it a 'toxin' (chapter 11, page 117, 2013) and a 'poison' (here). It's not just that high fructose corn syrup is the sweetener of choice to be found in the majority of soft drinks but that it is in almost every processed food on supermarket shelves; indeed it is difficult to find a product that does not contain it.
Most of us know that too much sugar is not good for our health. Indeed, back in 1972, John Yudkin warned us all of its danger in his book 'Pure, White, and Deadly'. In the updated version of the book (1986), Yudkin states that sugar consumption in Western society has risen to more than 20 times that of our ancestors with the average Westerner consuming more than 100 pounds of sugar every year (Lustig says it is now 130 pounds a year 2013). Given the fact that sugar is not good for health (see, for example, Johnson et al, 2009; Yudkin, 2012; Wang, 2014; Yang et al, 2014)
" ... if only a small fraction of what is already known about the effects of sugar were to be revealed in relation to any other material used as a food additive, that material would promptly be banned." (Yudkin, 1986)
and health is an important factor to IEPMLD, we should not be providing drinks or foodstuffs that are not conducive to good health. Thus, at breaks and at meal times, we should ensure that healthy options, especially water, are readily available and that unhealthy options are restricted if not eliminated altogether.
"Poor hydration at any time affects how well a child's brain operates and his or her learning ability. At school hydration is imperative to achieving a teacher’s learning objectives. If kids are slightly dehydrated they may appear tired, complain of headaches and have a reduced ability to concentrate, and if they are usually like this they might know no different and think they feel normal. If a child actually feels thirsty then his or her mental performance has already got to the level about 10 per cent lower than before and mental performance deteriorates
progressively as the degree of dehydration increases. " (Pugh, 2011a)
While water is good for us, too many sugary drinks, are not:
"All of the popular energy drinks in the market have different variations of caffeine, and most of these drinks are not considered healthy for the human body. Most of these energy drinks should be watched carefully due to the unbalanced ingredients, especially sugar and caffeine in their compositions (Miller, 2008). Most energy drinks also stimulate and trigger reactions that can increase blood pressure, heart rate or alter glycemic levels. These can often prevent normal sleep cycles and dehydrate the body." (González et al, 2012)
A 2017 study by Pase et al compared data from 4,000 participants and then divided them into two groups: The first group contained people who consumed one or two sugary drinks each day, which included fruit juice, soda, or other soft drinks. The second group did not drink any sugary beverages. The researchers found that those people who consumed up to two sugary drinks daily had reduced brain volume, a significantly smaller hippocampus, and performed worse on memory tests. Furthermore, the situation doesn't appear to get better if you switch to diet sodas, Pase et al (2017) found that older adults who drank artificially sweetened beverages regularly were more likely to have a stroke or develop Alzheimer's disease over 10 years.
However, limited intake of sugar can have beneficial effects:
"Avoiding tooth decay, diabetes, and obesity are all good reasons to limit consumption of sugar in the human diet. But sugar consumption, even in high amounts, does not contribute to hyperactivity, inattention, juvenile delinquency, reductions in cognitive performance, or other behavior problems in children or adults. Instead, a high level of glucose, or sugar, consumption actually improves athletic, academic, and cognitive performance, and may enhance self-control. Unless medically prescribed for non-behavioral reasons, dietary restriction of sugar intake is inappropriate and may have unintended behavioral effects (e.g., Fisher & Birch, 1999), create unnecessary interpersonal conflict, and be counterproductive by precluding consideration and implementation of proven effective interventions for behavioral and performance problems, such as behavior therapy as treatment for attention-deficit/hyperactivity disorder." (Flora & Polenick, 2013)
However (!), the above pertains to glucose and not to fructose (high fructose corn syrup) which tends to be the main sweetener in many sweetened beverages as it is cheap to produce in quantity. Sugar comes in many forms (the '-oses') glucose, fructose, sucrose, lactose, maltose, etc. There is a difference between the way glucose and fructose interact with the human body (Lustig, 2013) with fructose being compared to 'alcohol without the buzz' (Lustig, 2013b). Indeed, Lustig pulls no punches in calling it a 'toxin' (chapter 11, page 117, 2013) and a 'poison' (here). It's not just that high fructose corn syrup is the sweetener of choice to be found in the majority of soft drinks but that it is in almost every processed food on supermarket shelves; indeed it is difficult to find a product that does not contain it.
Most of us know that too much sugar is not good for our health. Indeed, back in 1972, John Yudkin warned us all of its danger in his book 'Pure, White, and Deadly'. In the updated version of the book (1986), Yudkin states that sugar consumption in Western society has risen to more than 20 times that of our ancestors with the average Westerner consuming more than 100 pounds of sugar every year (Lustig says it is now 130 pounds a year 2013). Given the fact that sugar is not good for health (see, for example, Johnson et al, 2009; Yudkin, 2012; Wang, 2014; Yang et al, 2014)
" ... if only a small fraction of what is already known about the effects of sugar were to be revealed in relation to any other material used as a food additive, that material would promptly be banned." (Yudkin, 1986)
and health is an important factor to IEPMLD, we should not be providing drinks or foodstuffs that are not conducive to good health. Thus, at breaks and at meal times, we should ensure that healthy options, especially water, are readily available and that unhealthy options are restricted if not eliminated altogether.
91. Literacy and Numeracy: Academic Skills

"The results of the present study suggest that some students with PMD who receive academic instruction may experience more “happiness” which presents a reasonable rationale to provide this type of instruction. Besides providing positive teacher-student interactions, academic instruction may also improve communication skills, increase social interactions, and increase desirable post school outcomes." (Bobzien, 2014) (PMD (USA) = PMLD (UK))
What! You can teach academic subjects to IEPMLD and they like it more?! Well, that's what this piece of research shows (read it for yourself). Yes, it was all female subjects. Yes, there were only four participants. Yes, the novelty of something 'new' may have had some impact on the outcome. However, it is still a little surprising! The biggest problem for me is that the results depend on outside observations of 'happiness' by others. As the Learner's themselves were not able (by definition) to report back to the research team ("Hey, I was happiest doing the math"!) and, as the research assistants had to record observations of displays of happiness (smiling, vocalisations, movements, etc), there is scope for incorrect readings (perhaps you can be inwardly happy but not necessarily show it on the outside? However, until we can do in situ brain scans, how else would we measure happiness?). Even, if we grant that there were more displays of 'happiness during the academic sessions, how do we know it was specifically as a result of the academia itself and not some other variable? Having said all of that (and not as a criticism of Professor Bobzien), I find the paper intriguing, enlightening, and more than worthy of a mention on this page as the subject of this section.
Let's assume that the study is indeed correct in it's finding that Individuals Experiencing PMLD are happier during academic type instruction session over functional instruction. Although we might ask, 'why should that be?', we should note that academic learning did not upset or turn off the Learners. They were more alert. This, in itself, should make us question our approach in special education classrooms around the world when working with IEPMLD.
The next thing to consider is what constitutes academic learning? In the Bobzien paper (2014), the academic learning comprised pre-literacy, pre-numeracy activities together with some basic science:
"For the duration of this instructional condition, students were instructed in pre-literacy skills (i.e., sight word identification, letter-sound identification), pre-numeracy skills (i.e., one-to-one correspondence, shape identification, calendar), and basic science facts (i.e., five senses, weather)." (Page 5)
If you return to the control chart in section one of this webpage, you will note that one branch of the 'seven Cs' refers to 'cognition; (including contingency awareness). Talksense has long championed the inclusion of cognitive approaches in equal measures with functional and sensory alternatives in the curriculum for IEPMLD. For me, academic equates to cognitive and although functional and sensory have cognitive elements (how could they not?) academic is definitely more cerebral!
What! You can teach academic subjects to IEPMLD and they like it more?! Well, that's what this piece of research shows (read it for yourself). Yes, it was all female subjects. Yes, there were only four participants. Yes, the novelty of something 'new' may have had some impact on the outcome. However, it is still a little surprising! The biggest problem for me is that the results depend on outside observations of 'happiness' by others. As the Learner's themselves were not able (by definition) to report back to the research team ("Hey, I was happiest doing the math"!) and, as the research assistants had to record observations of displays of happiness (smiling, vocalisations, movements, etc), there is scope for incorrect readings (perhaps you can be inwardly happy but not necessarily show it on the outside? However, until we can do in situ brain scans, how else would we measure happiness?). Even, if we grant that there were more displays of 'happiness during the academic sessions, how do we know it was specifically as a result of the academia itself and not some other variable? Having said all of that (and not as a criticism of Professor Bobzien), I find the paper intriguing, enlightening, and more than worthy of a mention on this page as the subject of this section.
Let's assume that the study is indeed correct in it's finding that Individuals Experiencing PMLD are happier during academic type instruction session over functional instruction. Although we might ask, 'why should that be?', we should note that academic learning did not upset or turn off the Learners. They were more alert. This, in itself, should make us question our approach in special education classrooms around the world when working with IEPMLD.
The next thing to consider is what constitutes academic learning? In the Bobzien paper (2014), the academic learning comprised pre-literacy, pre-numeracy activities together with some basic science:
"For the duration of this instructional condition, students were instructed in pre-literacy skills (i.e., sight word identification, letter-sound identification), pre-numeracy skills (i.e., one-to-one correspondence, shape identification, calendar), and basic science facts (i.e., five senses, weather)." (Page 5)
If you return to the control chart in section one of this webpage, you will note that one branch of the 'seven Cs' refers to 'cognition; (including contingency awareness). Talksense has long championed the inclusion of cognitive approaches in equal measures with functional and sensory alternatives in the curriculum for IEPMLD. For me, academic equates to cognitive and although functional and sensory have cognitive elements (how could they not?) academic is definitely more cerebral!
92. Jigsaws
I've witnessed too many young adults (18+) doing Thomas the Tank Engine type jigsaws in special education establishments and it always makes me question just what the staff are thinking! As the rule is 'preference and not deference' there should not be a stock of jigsaws designed for five year olds in adult educational environments to be provided by staff to fill an 'idle Learner moment'.
There are websites offering simple jigsaws for adults at varying levels of ability with pieces ranging from 10 to 500. Simply Google 'Simple jigsaws for adults' and see what comes up. While Talksense could provide links, companies offering such products come and go and therefore it is better if the search comes directly from you.
Although I found some suitable pictures, I was looking for 'pop star' images and the like that may be more motivating than English country scenes. These really are more diffiuclt to locate especially with a limit on the number of pieces. However, on Googling, 'make your own jigsaw', I came up with this website:
https://www.photobox.co.uk/shop/home-gifts/photo-jigsaw#page=details
The site offers to make jigsaws from personal photographs at varying levels of complexity including a 50 piece one (which it says is for children but it could be for any age depending on what picture is supplied) for just a few pounds. Thus, it would be possible to have a jigsaw of every student in a class individually or as a group for Learners to use as a meaningful age-appropriate activity.
Why is making a jigsaw a meaningful activity?
Many Learners will have a significant amount of leisure time on leaving full time education; not all will find a job, for example. It is extremely unlikely that IEPMLD will be in gainful amployment and thus they will need to find things that will occupy time in a pleasurable manner. While not every IEPMLD will be able to cope cognitively or physically with a jigsaw there may be a limited few that can. For those, jigsaws are:
My learners couldn't physically manage a jigsaw.
There will be many Learners who would not cope with this activity both for physical and or cognitive reasons. If that is the case then ignore this suggestion and move on! However, if a Learner has the physical capability to manipulate the pieces do not automatically assume that s/he will not cope cogntively; What have you got to lose by trying with something very simple?
Is training for Leisure a meanigful activity for IEPMLD at FE level?
Absolutely yes! FE concerns itself with preparation for a future 'career'. Career' does not simply mean a vocational pathway but rather should be seen in a broader definition that includes filling the day with any meaningful activity. This will incude a vocational aspect or an academic aspect or a leisure aspect or any comibination thereof
"A career is an individual's journey through learning, work and other aspects of life." ( Wikipedia 2016)
There are websites offering simple jigsaws for adults at varying levels of ability with pieces ranging from 10 to 500. Simply Google 'Simple jigsaws for adults' and see what comes up. While Talksense could provide links, companies offering such products come and go and therefore it is better if the search comes directly from you.
Although I found some suitable pictures, I was looking for 'pop star' images and the like that may be more motivating than English country scenes. These really are more diffiuclt to locate especially with a limit on the number of pieces. However, on Googling, 'make your own jigsaw', I came up with this website:
https://www.photobox.co.uk/shop/home-gifts/photo-jigsaw#page=details
The site offers to make jigsaws from personal photographs at varying levels of complexity including a 50 piece one (which it says is for children but it could be for any age depending on what picture is supplied) for just a few pounds. Thus, it would be possible to have a jigsaw of every student in a class individually or as a group for Learners to use as a meaningful age-appropriate activity.
Why is making a jigsaw a meaningful activity?
Many Learners will have a significant amount of leisure time on leaving full time education; not all will find a job, for example. It is extremely unlikely that IEPMLD will be in gainful amployment and thus they will need to find things that will occupy time in a pleasurable manner. While not every IEPMLD will be able to cope cognitively or physically with a jigsaw there may be a limited few that can. For those, jigsaws are:
- a fun option for leisure time;
- good for developing hand eye cordination;
- a means of improving spatial awareness.
My learners couldn't physically manage a jigsaw.
There will be many Learners who would not cope with this activity both for physical and or cognitive reasons. If that is the case then ignore this suggestion and move on! However, if a Learner has the physical capability to manipulate the pieces do not automatically assume that s/he will not cope cogntively; What have you got to lose by trying with something very simple?
Is training for Leisure a meanigful activity for IEPMLD at FE level?
Absolutely yes! FE concerns itself with preparation for a future 'career'. Career' does not simply mean a vocational pathway but rather should be seen in a broader definition that includes filling the day with any meaningful activity. This will incude a vocational aspect or an academic aspect or a leisure aspect or any comibination thereof
"A career is an individual's journey through learning, work and other aspects of life." ( Wikipedia 2016)
93. Choice Words
94. Diary

95. Dance Dance wherever you may be

96. Music Therapy

Music therapy is a process and form which combines the healing aspects of music with the issues of human need for the benefit of the individual and hence society. The music therapist serves as a resource person and guide, providing musical experiences which direct clients towards health and well being (Kenny 1982).
Music provides communication by activating different kinds of psychic phenomena and by bringing new material into the communication process…the individual is able to express and feel experiences which are non-verbal and non-discursive, such as bodily rhythms and unconscious and traumatic experiences which are anchored in the early childhood of the individual (Lehtonen 1993).
Music therapy is the scientific application of music or music activities to attain therapeutic goals. Music therapy can also be defined as the structured use of music to bring about desired changes in behaviour (Carter 1982).
Music provides communication by activating different kinds of psychic phenomena and by bringing new material into the communication process…the individual is able to express and feel experiences which are non-verbal and non-discursive, such as bodily rhythms and unconscious and traumatic experiences which are anchored in the early childhood of the individual (Lehtonen 1993).
Music therapy is the scientific application of music or music activities to attain therapeutic goals. Music therapy can also be defined as the structured use of music to bring about desired changes in behaviour (Carter 1982).
97. Pet Project

Research has shown that the interaction between humans and animals can have positive outcomes for those participating (Katcher, 1977; Serpell, 1991; Heimlich, 2001; Martin & Farnum, 2002; Foxall, 2002; Chandler, 2005; Scott, 2005; Boat, 2006; McNicholas & Collis, 2006; Morrison, 2007; Ming Lee Yeh, 2008; Pavlides, 2008; Shurtleff et al, 2009; Fine 2010; Herzog, 2011; O'Haire et al, 2013; Siewertsen et al, 2015).
"For example, among 11,000 German and Australian adults, pet owners were in better physical condition than non-pet owners, and they made 15% fewer doctor visits, a potential savings of billions of dollars in national health expenditures. And an epidemiological study of Chinese women found that pet owners exercised more, slept better, felt more physically fit, and missed fewer days from work than women without pets. Further, these effects were particularly strong for individuals who reported that they were very closely attached to their pets." (Herzog, 2011, page 238)
However, Herzog (op.cit.) goes on to state that while there are studies providing a positive bias there are equally studies that show the very opposite effect! Notwithstanding these issues, Herzog appears to rule the negative aspects out when considering the use of animals as therapeutic intervention for Individuals with Learning Difficulties:
"Note that the main focus of this article is on the effects of pets on the physical and mental health of their owners, not the efficacy of animals as therapeutic agents for disorders such as autism and attention-deficit/hyperactivity disorder." (Herzog, 2011, page 238)
The use of animals in further education organisations as part of the curriculum has been long established: there are colleges with dogs, horses, donkeys, fish, rabbits, as well as 'farm-type' livestock with the animals being used for educational, social, therapeutic, and vocational purposes. Even where there might not be such animals on the premises, many establishments will provide 'saddle therapy', regular horse riding sessions as a part of the curriculum. Indeed, in one establishment I visited in Hong Kong there was a room devoted to what they called 'hippotherapy' which involved no actual horse but rather a mechanical device which emulated the movements of a horse on which students could safely be seated and ride.
A number of beneficial claims have been made about the use of animals as a part of the curriculum. For example, the Riding For Disabled Association (RDA) on their website state:
"At RDA therapy is often disguised as an opportunity to have fun. In fact recent research into rider outcomes shows that after just 12 weeks 74% demonstrated physical improvement, 77% experienced greater confidence and 75% more enjoyment. 65% showed a greater willingness and ability to communicate, 72% showed improved relationship building skills and 78% demonstrated clear advances in horsemanship." (RDA website: RDA.org.uk, 2017)
although they do not quote the empirical source for these figures. However, there is evidence to support such claims:
"More specifically, compared to wait-listed participants in our control group, autistic children in the experimental group improved in critical areas such as sensory integration and directed attention. Participants also demonstrated improved social motivation and sensory sensitivity, as well as decreased inattention and distractibility." (Bass et al, 2009, page 1266) (see also: MacKinnon et al, 1995; MacPhail et al, 1998; Land et al, 2001; Sterba et al 2002; Benda et al, 2003; Bizub et al, 2003; Macauley & Guiterrez, 2004; Weber & Westmoquette, 2010; Coffey, 2014)
Riding for the disabled is but one branch of 'Animal Assisted Therapy':
"Animal-assisted therapy (AAT) is a form of therapy which aims to provide a therapeutic intervention for humans by involving animals in their treatment. Its focus is on augmenting behavioural, social, emotional, cognitive or physical functioning." (Maber-Aleksandrowicz, Avent, &
Hassiotis, 2016, page 323)
"Animal-assisted therapy includes deliberately planned pedagogic, psychological and socially integrative interventions with animals for children, youths, adults and senior citizens with cognitive, social-emotional and motoric disabilities, and behavioural problems, and for focused support. It also includes health-promoting, preventive and rehabilitative measures" (European Society for Animal Assisted Therapy, ESAAT, 2011, page 1)
AAT can be utilised in many ways in the special education curriculum for IEPMLD: For example, O'Haire et al (2013) showed how simple interaction with animals (in this instance, Guinea pigs) could have positive outcomes for those experiencing Learning Difficulties (see following video: YouTube)
"For example, among 11,000 German and Australian adults, pet owners were in better physical condition than non-pet owners, and they made 15% fewer doctor visits, a potential savings of billions of dollars in national health expenditures. And an epidemiological study of Chinese women found that pet owners exercised more, slept better, felt more physically fit, and missed fewer days from work than women without pets. Further, these effects were particularly strong for individuals who reported that they were very closely attached to their pets." (Herzog, 2011, page 238)
However, Herzog (op.cit.) goes on to state that while there are studies providing a positive bias there are equally studies that show the very opposite effect! Notwithstanding these issues, Herzog appears to rule the negative aspects out when considering the use of animals as therapeutic intervention for Individuals with Learning Difficulties:
"Note that the main focus of this article is on the effects of pets on the physical and mental health of their owners, not the efficacy of animals as therapeutic agents for disorders such as autism and attention-deficit/hyperactivity disorder." (Herzog, 2011, page 238)
The use of animals in further education organisations as part of the curriculum has been long established: there are colleges with dogs, horses, donkeys, fish, rabbits, as well as 'farm-type' livestock with the animals being used for educational, social, therapeutic, and vocational purposes. Even where there might not be such animals on the premises, many establishments will provide 'saddle therapy', regular horse riding sessions as a part of the curriculum. Indeed, in one establishment I visited in Hong Kong there was a room devoted to what they called 'hippotherapy' which involved no actual horse but rather a mechanical device which emulated the movements of a horse on which students could safely be seated and ride.
A number of beneficial claims have been made about the use of animals as a part of the curriculum. For example, the Riding For Disabled Association (RDA) on their website state:
"At RDA therapy is often disguised as an opportunity to have fun. In fact recent research into rider outcomes shows that after just 12 weeks 74% demonstrated physical improvement, 77% experienced greater confidence and 75% more enjoyment. 65% showed a greater willingness and ability to communicate, 72% showed improved relationship building skills and 78% demonstrated clear advances in horsemanship." (RDA website: RDA.org.uk, 2017)
although they do not quote the empirical source for these figures. However, there is evidence to support such claims:
"More specifically, compared to wait-listed participants in our control group, autistic children in the experimental group improved in critical areas such as sensory integration and directed attention. Participants also demonstrated improved social motivation and sensory sensitivity, as well as decreased inattention and distractibility." (Bass et al, 2009, page 1266) (see also: MacKinnon et al, 1995; MacPhail et al, 1998; Land et al, 2001; Sterba et al 2002; Benda et al, 2003; Bizub et al, 2003; Macauley & Guiterrez, 2004; Weber & Westmoquette, 2010; Coffey, 2014)
Riding for the disabled is but one branch of 'Animal Assisted Therapy':
"Animal-assisted therapy (AAT) is a form of therapy which aims to provide a therapeutic intervention for humans by involving animals in their treatment. Its focus is on augmenting behavioural, social, emotional, cognitive or physical functioning." (Maber-Aleksandrowicz, Avent, &
Hassiotis, 2016, page 323)
"Animal-assisted therapy includes deliberately planned pedagogic, psychological and socially integrative interventions with animals for children, youths, adults and senior citizens with cognitive, social-emotional and motoric disabilities, and behavioural problems, and for focused support. It also includes health-promoting, preventive and rehabilitative measures" (European Society for Animal Assisted Therapy, ESAAT, 2011, page 1)
AAT can be utilised in many ways in the special education curriculum for IEPMLD: For example, O'Haire et al (2013) showed how simple interaction with animals (in this instance, Guinea pigs) could have positive outcomes for those experiencing Learning Difficulties (see following video: YouTube)

It is also feasible that, by using a BIGmack, a dog could be taught to respond to the 'instructions' of an IEPMLD. Indeed, as the BIGmack would always give the command in exactly the same way (providing the initial recording was maintained) a dog should come to learn the command that much quicker. While the cartoon seems to suggest it might be possible to train a cat in a similar fashion, this is used merely to illustrate the topic; cats do not normally respond to such commands! However, if the BIGmack was always used to call a cat for food, it isn't impossible that even the most obstinate cat could respond to a Learner's commands.
Coping with loss and grief might be particularly difficult for an IEPMLD to understand. The death of an animal might be a means to explore this area and provide some insight for some Learners. The unexpected 'disappearance' of a relation or friend can be traumatic especially if a person is 'excluded' from the process because 'they won't understand'. This is a complex area and, as such, is dealt with in more detail on a separate webpage on this site: HERE.
There are many ways in which animals might be used within further education to promote learning and Leisure for IEPMLD. It is beyond the scope of this page to cover them all here. However, the bibliography section provides reference to several articles and books for follow up reading.
Coping with loss and grief might be particularly difficult for an IEPMLD to understand. The death of an animal might be a means to explore this area and provide some insight for some Learners. The unexpected 'disappearance' of a relation or friend can be traumatic especially if a person is 'excluded' from the process because 'they won't understand'. This is a complex area and, as such, is dealt with in more detail on a separate webpage on this site: HERE.
There are many ways in which animals might be used within further education to promote learning and Leisure for IEPMLD. It is beyond the scope of this page to cover them all here. However, the bibliography section provides reference to several articles and books for follow up reading.
98. Catch someone doing something well!
"Leadership is not something you do to people. It's something you do with people"
TalkSense has been invited into many Specialist Establishments across the world from America through the UK, Europe, Hong Kong, and Taiwan and has witnessed some amazing practice. There are dedicated teams across the globe all striving to provide a first class education for those in their charge. In a few instances, teams were working with less than perfect resources and yet their efforts and their practice was outstanding. However, in a few instances, in some places, TalkSense noted that staff morale was low. Indeed, staff were eager to report their concerns and would request a meeting or a talk somewhere in private. When asked for a private talk, the result was always the same: the person wanted to divulge information which was less than complimentary about the establishment or a person within the establishment or both. There are typically some common threads to such concerns, these include (but are not limited to) staff belief that:
TalkSense does not 'inspect' educational establishment, that function is left to the official inspection teams from within and without the establishment, rather TalkSense 'observes' practice. Following such observations TalkSense prepares reports detailing suggestions for policy, procedure and practice amendments. Unless specifically demanded by the establishment, TalkSense does not grade nor criticise any individual although outstanding practice is always highlighted. Our philosophy is to 'catch staff members doing something right' (see Blanchard & Johnson, 1983; Blanchard, 1999) and praise them. In fact, in many instances, just witnessing good practice and letting others know is reward in itself. We all feel better about ourselves when someone notices what we are doing and makes us aware they think it is good (see, for example, Mortenson & Witt,1998). TalkSense understands that there was a sign displayed in Lee Iaccoca’s office when he ran the Chrysler Corporation which read,
“We live by encouragement; we die without it, slowly, sadly and angrily.”
Encouragement helps staff to work more productively: sometimes we neither need a carrot nor a stick, we just need to make people feel good about themselves and the work that they are doing. When we feel good we tend to work more productively:
“People who feel good about themselves produce good results, and people who produce good results feel good about themselves.” (Blanchard, 1999)
The role of a manager is not an easy one. Like all involved in education, the work load is heavy. However, management should make a point of getting out of the office and noticing what is happening. When something is good, let it be known that it is good. Catch someone or some team doing something right.
"Also supervisorial feedback affects staff members’ behaviour. Staff members receive consequences mostly from their administrative tasks (Mansell & Elliot 2001). Furthermore, McConckey & Collins (2010) noted that staff members prioritize care tasks over social inclusion tasks. Therefore, supervisors’ feedback on which tasks should the staff members prioritise affects the client-staff member interactions (Cullen 1992). This also contributes to the staff members’ role clarity. When supervisors articulate clearly what is expected from staff during the workday, the staff members’ level of stress decreases (Hatton, Emerson, Rivers, Mason, Swarbrick, Mason, Kiernan, Reeves & Alborz 2001)" (Koski, 2014, page 22)
Catch the staff doing something right!
But that's what we pay them for!
I think you are missing the point!
I haven't got the time to be wandering the corridors trying to find if staff are doing something well.
You don't have to spend hours aimlessly wandering! You might aim to 'go walkabout' before the day starts - see who is in early and yet on task and comment on this. Additionally, you might repeat the process at the end of the day. Furthermore, one more walkabout during the day at a random time, in between your tasks to give yourself a well-earned break, is both good practice and, in addition, good for your health; sitting immobile at a desk all day is not recommended for your well-being. Indeed, the British Journal of Sports Medicine recommends that we should be on our feet for a minimum of 2 hours daily during working hours to reduce the health risks of too much sitting time (BMJ, 2015).
We have termly planned session observations with formal feedback. There's no requirement for more.
Session observations are not the same thing; staff will known about those and prepare for them in advance. As such you ought to be seeing good practice! 'Walkabouts' can catch staff when they are not expecting it and those 'throw away' positive comments can do a world of good for staff morale and for staff respect for the management team.
Does it have to be senior managers?
No, absolutely not! Any staff member who has a senior role to others can do it. Teachers in classrooms can (and should) make regular positive comments on supporting staff, for example. Equally, all staff members can positively comment on any other staff member, even a senior member ... 'I saw you working with NAME and I thought you were brilliant' ... who would object to that? Sure, we don't want to encourage sycophancy but it is easy to tell the difference between a genuine remark well made and one with an ulterior motive!
TalkSense has been invited into many Specialist Establishments across the world from America through the UK, Europe, Hong Kong, and Taiwan and has witnessed some amazing practice. There are dedicated teams across the globe all striving to provide a first class education for those in their charge. In a few instances, teams were working with less than perfect resources and yet their efforts and their practice was outstanding. However, in a few instances, in some places, TalkSense noted that staff morale was low. Indeed, staff were eager to report their concerns and would request a meeting or a talk somewhere in private. When asked for a private talk, the result was always the same: the person wanted to divulge information which was less than complimentary about the establishment or a person within the establishment or both. There are typically some common threads to such concerns, these include (but are not limited to) staff belief that:
- Management was out of touch with 'reality';
- Management does not listen to concerns;
- Management does not act on concerns;
- Management does not see what is going on;
- Current practice was not supporting student development;
- Lack of time to prepare, to make things happen;
- Working environment too stressful;
- Lack of resources;
- Staff turnover high;
- Staff asked to perform duties for which they felt ill-prepared;
- Quality of training and other training issues;
- ...
TalkSense does not 'inspect' educational establishment, that function is left to the official inspection teams from within and without the establishment, rather TalkSense 'observes' practice. Following such observations TalkSense prepares reports detailing suggestions for policy, procedure and practice amendments. Unless specifically demanded by the establishment, TalkSense does not grade nor criticise any individual although outstanding practice is always highlighted. Our philosophy is to 'catch staff members doing something right' (see Blanchard & Johnson, 1983; Blanchard, 1999) and praise them. In fact, in many instances, just witnessing good practice and letting others know is reward in itself. We all feel better about ourselves when someone notices what we are doing and makes us aware they think it is good (see, for example, Mortenson & Witt,1998). TalkSense understands that there was a sign displayed in Lee Iaccoca’s office when he ran the Chrysler Corporation which read,
“We live by encouragement; we die without it, slowly, sadly and angrily.”
Encouragement helps staff to work more productively: sometimes we neither need a carrot nor a stick, we just need to make people feel good about themselves and the work that they are doing. When we feel good we tend to work more productively:
“People who feel good about themselves produce good results, and people who produce good results feel good about themselves.” (Blanchard, 1999)
The role of a manager is not an easy one. Like all involved in education, the work load is heavy. However, management should make a point of getting out of the office and noticing what is happening. When something is good, let it be known that it is good. Catch someone or some team doing something right.
"Also supervisorial feedback affects staff members’ behaviour. Staff members receive consequences mostly from their administrative tasks (Mansell & Elliot 2001). Furthermore, McConckey & Collins (2010) noted that staff members prioritize care tasks over social inclusion tasks. Therefore, supervisors’ feedback on which tasks should the staff members prioritise affects the client-staff member interactions (Cullen 1992). This also contributes to the staff members’ role clarity. When supervisors articulate clearly what is expected from staff during the workday, the staff members’ level of stress decreases (Hatton, Emerson, Rivers, Mason, Swarbrick, Mason, Kiernan, Reeves & Alborz 2001)" (Koski, 2014, page 22)
Catch the staff doing something right!
But that's what we pay them for!
I think you are missing the point!
I haven't got the time to be wandering the corridors trying to find if staff are doing something well.
You don't have to spend hours aimlessly wandering! You might aim to 'go walkabout' before the day starts - see who is in early and yet on task and comment on this. Additionally, you might repeat the process at the end of the day. Furthermore, one more walkabout during the day at a random time, in between your tasks to give yourself a well-earned break, is both good practice and, in addition, good for your health; sitting immobile at a desk all day is not recommended for your well-being. Indeed, the British Journal of Sports Medicine recommends that we should be on our feet for a minimum of 2 hours daily during working hours to reduce the health risks of too much sitting time (BMJ, 2015).
We have termly planned session observations with formal feedback. There's no requirement for more.
Session observations are not the same thing; staff will known about those and prepare for them in advance. As such you ought to be seeing good practice! 'Walkabouts' can catch staff when they are not expecting it and those 'throw away' positive comments can do a world of good for staff morale and for staff respect for the management team.
Does it have to be senior managers?
No, absolutely not! Any staff member who has a senior role to others can do it. Teachers in classrooms can (and should) make regular positive comments on supporting staff, for example. Equally, all staff members can positively comment on any other staff member, even a senior member ... 'I saw you working with NAME and I thought you were brilliant' ... who would object to that? Sure, we don't want to encourage sycophancy but it is easy to tell the difference between a genuine remark well made and one with an ulterior motive!
99. Staff Training 1: What If ... We Think Outside The Box?

While all establishments invest some time in staff training, the quality of the training may vary across sessions, with some not being very inspiring at all. One different form of training that might be considered is the 'What If ...' approach (Kaufman, 2016). This form of training accesses the staff's divergent and creative thinking to provide new and innovative practice. In the 'what if' approach staff are asked to consider an imaginary scenario and to postulate possible outcomes. Scenarios should not be portrayed as good or bad but rather simply neutrally presented for further exploration. For example, in relation to a special Further Education establishment the scenario might be ... 'what if ... we had no fixed curriculum?'. While some might see that as a nightmarish situation others might nevertheless postulate some possible resulting positive phenomena. The idea is to generate a number of interesting ideas that can be explored, extended, evaluated and subsequently implemented or discarded.
Other examples of possible 'what if' scenarios might be:
As a training day, the 'what if' approach can yield some hereto unconsidered unique possibilities for future curriculum and management improvements. The staff are split into groups of at least 6 (maximum 12) people. If possible the staff should included everyone who comes into contact with students during the working day in the establishment including (but not limited to) the caretakers, the kitchen staff, the cleaning staff, the medical staff, the support staff, the teaching staff, and the therapy staff. Each team should include a diverse range of roles such that no one team comprises entirely support staff or teachers ... Each team is provided with up to three 'what if' statements (or you can ask each team to generate their own) to explore during the first session of the day. Before starting the process each team is given to sets of six cards (enough for one card per team member) which are blank on one side. The teams are instructed to shuffle the cards into random order and each team member selects one. On each card is a 'role' that the staff member must primarily play during the initial session. All staff are aware that each is playing a role but they do not know what the roles are other than their own. As staff are playing a role they cannot be criticised for being too negative, too imaginative, or too anything! The six roles are:
Session 1: Introduction (30 minutes)
Other examples of possible 'what if' scenarios might be:
- What if ... the college opened seven days a week?
- What if ... the college offered sessions in the evening?
- What if ... the college operated a one way system?
- What if ... students could choose what they did?
- What if ... we went to the student rather than the student coming to us?
- What if ... we ran our our sessions with two teaching staff?
- What if ... we gave staff one day a week free from teaching responsibility?
- What if ... we ran a staff bonus scheme?
- What if ... all staff were involved in observations?
- What if ... staff had to take a vow of silence for an entire week?
- What if ... staff had to work one morning a week while blindfolded?
- What if ... there was an anonymous staff whistle blowing system?
- What if ... all the staff were speech therapists?
- What if ... all the staff were physiotherapists?
- What if ... all the staff were occupational therapists?
- What if ... we ran a flexible working day?
- What if ... all students were expected to make their own way to the next session?
- What if ... Lady Gaga was a staff member?
- What if ... we took the students for a day trip to the moon?
- What if ... the students taught the staff?
- What if ... the PMLD group was entered in the Local Marathon?
- What if ... we taught outside when it was raining?
As a training day, the 'what if' approach can yield some hereto unconsidered unique possibilities for future curriculum and management improvements. The staff are split into groups of at least 6 (maximum 12) people. If possible the staff should included everyone who comes into contact with students during the working day in the establishment including (but not limited to) the caretakers, the kitchen staff, the cleaning staff, the medical staff, the support staff, the teaching staff, and the therapy staff. Each team should include a diverse range of roles such that no one team comprises entirely support staff or teachers ... Each team is provided with up to three 'what if' statements (or you can ask each team to generate their own) to explore during the first session of the day. Before starting the process each team is given to sets of six cards (enough for one card per team member) which are blank on one side. The teams are instructed to shuffle the cards into random order and each team member selects one. On each card is a 'role' that the staff member must primarily play during the initial session. All staff are aware that each is playing a role but they do not know what the roles are other than their own. As staff are playing a role they cannot be criticised for being too negative, too imaginative, or too anything! The six roles are:
- Administrative: Managing. What is the subject? What are we thinking about? What is the goal? Looking at the big picture.
- Background: Considering the available information. What are the facts behind it all?
- Creative: Thinking really creatively. Devising lots of ideas & statements of provocation and investigation. Both realistic and crazy.
- Discernment: Being cautious & conservative. Applying logic to identifying reasons to be realistic & practical.
- Emotional: Intuitive or instinctive gut reactions or statements of emotional feeling but without any justification.
- Favorable: Optimistic approach. logic applied to identifying benefits, seeking harmony. Looking for positive side of things.
Session 1: Introduction (30 minutes)
- Whole staff meet together;
- Day is detailed;
- Groups of 6 to 12 are generated;
- Group spokesperson is selected;
- Instruction sheet and role cards are given to group spokesperson (s/he does not look at the role cards);
- Each group relocates to a specific room in the establishment;
- Group rearrange furniture to allow for a reasonable debate;
- Spokesperson reads instruction sheet to other team members;
- Spokesperson shuffles cards;
- Each member selects a card at random and secretly reads their role for the session. The cards are placed face down on the table top;
- Spokesperson makes the 'what if' statement (there can be more than one 'what if' statement discussed during the session);
- The group debate the statement with each member paying special attention to their primary assigned role;
- The spokesperson records the main points of the debate for later feedback to the whole team.
- The spokesperson ensures correct timekeeping, For example, if there is a break, the spokesperson ensure all group return promptly.
- Groups meet in their own location;
- Spokesperson reads notes of morning debate;
- Group comment to add, amend or abrogate the notes.
- Whole staff meet up once again;
- Management read out first 'what if' statement;
- Each spokesperson in turn relates the groups thoughts, feelings, and ideas;
- Management collate the responses;
- At some later time, management review the responses and decide on implementation or course of action to follow.
100. Staff Training 2: Necessary Norms

"To be able to attune one’s actions to the above-mentioned support needs, support staff requires specialist knowledge and skills. High quality instruction and permanent training that is specifically oriented towards working with this target group may contribute to this." (Petry et al, 2007c, page 137)
There are some aspects of staff training that should not be neglected. However, TalkSense has encountered a number of establishments where such training has not taken place and where, perhaps, management has assumed that a 'common sense approach' would dictate staff practice and ensure a certain standard of provision. However, such practice is neither 'common' in that we have witnessed its absence, nor is it 'sense' in that some staff are not doing it. As such, some training is so important that it should be classified as a 'necessary norm' without which staff are not permitted to interact with Learners. Establishments should not simply assume, a new staff member, having several years experience in working in special education in another establishment, will meet an expected standard in a given area, rather, all staff should be considered as novices until 'necessary norm' training has been completed. What are the 'Necessary Norms'? These may vary slightly from establishment to establishment depending on the characteristics of the population being served but some are likely to be part of almost every special needs workplace.
For example: One such area of concern is 'wheelchair training', that is, good practice guidelines in working with and maneuvering Learners in wheelchairs. Here are just a few example of practices witnessed by Talksense while observing session around the world and around the UK:
An experiential event for wheelchair training would involve staff finding a partner and then one playing the role of a Learner and sitting in the wheelchair for the other one to take along a designated route (out of doors) which involved crossing at least one road, steps, and inside something like a local supermarket passing through a checkout before returning. On return the pair swap roles, repeating the route, such that each experience the role of staff member and learner. It is important that:
Training for wheelchairs might be best delivered by the therapy team (Physio, Occupational, and Speech and Language) coming together with the staff to review and update the policy and procedure document.
Necessary Norms might also include (in no particular order of relevance):
All necessary Norms should be detailed in their own Policy and Procedure document updated annually and made available to all staff via:
There are some aspects of staff training that should not be neglected. However, TalkSense has encountered a number of establishments where such training has not taken place and where, perhaps, management has assumed that a 'common sense approach' would dictate staff practice and ensure a certain standard of provision. However, such practice is neither 'common' in that we have witnessed its absence, nor is it 'sense' in that some staff are not doing it. As such, some training is so important that it should be classified as a 'necessary norm' without which staff are not permitted to interact with Learners. Establishments should not simply assume, a new staff member, having several years experience in working in special education in another establishment, will meet an expected standard in a given area, rather, all staff should be considered as novices until 'necessary norm' training has been completed. What are the 'Necessary Norms'? These may vary slightly from establishment to establishment depending on the characteristics of the population being served but some are likely to be part of almost every special needs workplace.
For example: One such area of concern is 'wheelchair training', that is, good practice guidelines in working with and maneuvering Learners in wheelchairs. Here are just a few example of practices witnessed by Talksense while observing session around the world and around the UK:
- pushing a student in a wheelchair without his/her permission/knowledge that this was about to happen;
- pushing a wheelchair with just one hand;
- pushing a wheelchair down a road while answering a personal call on a mobile phone;
- pushing a wheelchair with one hand while drinking coffee with the other;
- pushing a wheelchair forward such that it would move for a distance under its own momentum and letting go of the handles;
- allowing a wheelchair to freewheel downhill with no hands on the handles for short periods;
- pushing a wheelchair with one wheel on the pavement and one wheel on the road;
- stopping without apply the brakes and letting go of the chair;
- staff talking to other staff members and ignoring Learners for majority of journey;
- staff suddenly tipping wheelchairs backwards without warning to occupant;
- ...
An experiential event for wheelchair training would involve staff finding a partner and then one playing the role of a Learner and sitting in the wheelchair for the other one to take along a designated route (out of doors) which involved crossing at least one road, steps, and inside something like a local supermarket passing through a checkout before returning. On return the pair swap roles, repeating the route, such that each experience the role of staff member and learner. It is important that:
- for the outward part of the journey the staff member is completely silent but is allowed to talk about anything on the return route;
- the Learner is completely silent for the whole journey;
- Learners do not apply brakes at any time or assist in any way - they remain passive recipients of the actions of the other staff member;
- for part of the journey (perhaps a quarter of the route) the Learner wears a blindfold (other sensory deprivations may also be emulated);
- neither member discusses the experience until both have completed the task - then they can make notes to share with others performing the same task;
- all staff come together at the end to evaluate their experience and to discuss the policy and procedure document in light of their experiences and to make recommendations for any amendments;
- all new staff have such training before they can take any Learner anywhere in a wheelchair;
- all staff have refresher wheelchair training at least once every five years.
Training for wheelchairs might be best delivered by the therapy team (Physio, Occupational, and Speech and Language) coming together with the staff to review and update the policy and procedure document.
Necessary Norms might also include (in no particular order of relevance):
- dealing with behaviours that staff may find challenging;
- working with Objects Of Reference;
- providing choice;
- hoisting and transference from wheelchairs to ...;
- seizures and other medical issues;
- signing and other relevant AAC methodology;
- b
- c
All necessary Norms should be detailed in their own Policy and Procedure document updated annually and made available to all staff via:
- establishment network;
- hard printed copies kept in the staff room or in some other equally accessible position.
- discussing it with other staff team members;
- ensuring it complies with all relevant legislation (which may change over the years);
- the revised P&P is available in both hard and soft forms at all times;
- all staff are informed when a P&P has been modified.
- the Management Team are advised of any training implications of P&P modifications.
101. Free Special Educational Needs Resources and more ...

While not every program, etc on all of the sites listed here is suitable for IEPMLD or necessarily age appropriate, they are cost free (or, at least some aspects of the site are!) and, therefore, you will not have wasted any money if you find it isn't suitable. Click on the links to open a new window and access the software/program/resource. If you know of a source that is not listed please contact me at Talksense and let me know and I will add it to the list ([email protected]).
Please Note: At the time of building this webpage all the links were live but, as you might be viewing this months or even years later and because the web is pretty dynamic and changes from day to day, TalkSense cannot guarantee that each is still available. While TalkSense has visited each of the sites listed without issue, we cannot give any guarantee that they remain virus and malware free; as such, you should take necessary precautions. Good surfing!
http://www.oneswitch.org.uk/2/switch-downloads.htm
http://www.oneswitch.org.uk/2/sd-arcade.htm
http://www2.cliu.org/se/switch.aspx
https://www.senteacher.org/freeware/arts/
http://www.senteacher.org/files/
http://www.petewellssensorystories.com/
https://connectability.ca/visuals-engine/
http://www.doorwayonline.org.uk/
http://www.coloring4all.com/
http://themouseclub.co.uk/
http://www.fungooms.com/
https://www.bbc.co.uk/cbeebies/games
https://www.bbc.co.uk/cbeebies/shows/alphablocks
http://www.signedstories.com/
https://www.animaljam.com/welcome
http://www.wartgames.com/themes/list.html
http://www.sensoryworld.org/
http://papunet.net/games/games_of_precision
http://www.helpkidzlearn.com/creative/early-mouse-movements
http://www.helpkidzlearn.com/
http://www.roythezebra.com/index.html
http://www.ninjakiwi.com/Games/Bloons-Games/Bloons.html
http://www.ictgames.com/index.html
https://www.poissonrouge.com/
https://www.kneebouncers.com/games/
http://www.magickeys.com/books/color/
http://www.starfall.com/
http://www.slidescarnival.com/category/free-templates/playful-presentations
http://www.pppst.com/
http://www.sparklebox.co.uk/special-needs/#.WepKTFtSzX4
http://www.do2learn.com/
http://www.adaptingforautism.com/
http://atclassroom.blogspot.co.uk/
http://www.interventioncentral.org/
https://singinghands.co.uk/
http://hiyah.net/
https://www.bltt.org/software/greatfishrace/index.htm
The following download swf files. Your computer might warn you about these files but Talksense has downloaded, scanned them using Microsoft Security Essentials (no problems) and ran them (without any problems). So, we believe that they are OK.
www.maninthedark.com/
http://www.procreo.jp/labo/flower_garden.swf
http://www.jacksonpollock.org/
Do you know of other free resources that are suitable for Special Educational use? If so, why not make contact and let us know such that we can add it to this listing ([email protected]).
Please Note: At the time of building this webpage all the links were live but, as you might be viewing this months or even years later and because the web is pretty dynamic and changes from day to day, TalkSense cannot guarantee that each is still available. While TalkSense has visited each of the sites listed without issue, we cannot give any guarantee that they remain virus and malware free; as such, you should take necessary precautions. Good surfing!
http://www.oneswitch.org.uk/2/switch-downloads.htm
http://www.oneswitch.org.uk/2/sd-arcade.htm
http://www2.cliu.org/se/switch.aspx
https://www.senteacher.org/freeware/arts/
http://www.senteacher.org/files/
http://www.petewellssensorystories.com/
https://connectability.ca/visuals-engine/
http://www.doorwayonline.org.uk/
http://www.coloring4all.com/
http://themouseclub.co.uk/
http://www.fungooms.com/
https://www.bbc.co.uk/cbeebies/games
https://www.bbc.co.uk/cbeebies/shows/alphablocks
http://www.signedstories.com/
https://www.animaljam.com/welcome
http://www.wartgames.com/themes/list.html
http://www.sensoryworld.org/
http://papunet.net/games/games_of_precision
http://www.helpkidzlearn.com/creative/early-mouse-movements
http://www.helpkidzlearn.com/
http://www.roythezebra.com/index.html
http://www.ninjakiwi.com/Games/Bloons-Games/Bloons.html
http://www.ictgames.com/index.html
https://www.poissonrouge.com/
https://www.kneebouncers.com/games/
http://www.magickeys.com/books/color/
http://www.starfall.com/
http://www.slidescarnival.com/category/free-templates/playful-presentations
http://www.pppst.com/
http://www.sparklebox.co.uk/special-needs/#.WepKTFtSzX4
http://www.do2learn.com/
http://www.adaptingforautism.com/
http://atclassroom.blogspot.co.uk/
http://www.interventioncentral.org/
https://singinghands.co.uk/
http://hiyah.net/
https://www.bltt.org/software/greatfishrace/index.htm
The following download swf files. Your computer might warn you about these files but Talksense has downloaded, scanned them using Microsoft Security Essentials (no problems) and ran them (without any problems). So, we believe that they are OK.
www.maninthedark.com/
http://www.procreo.jp/labo/flower_garden.swf
http://www.jacksonpollock.org/
Do you know of other free resources that are suitable for Special Educational use? If so, why not make contact and let us know such that we can add it to this listing ([email protected]).
102. Book a TalkSense Observation of Your Practice

This page is titled '101 meaningful post-16 activities...' and yet here is number 102! Well, not quite, which is why it's the final section before the contact form and the bibliography. If you are impressed by this page and you would like TalkSense to come and observe your practice and give you a written comprehensive and objective opinion, then why not contact us using the form below or simply e-mail '[email protected]'. Talksense's observations are NOT critical of staff but rather highlight what is good and suggest ways of improving practice. TalkSense has witnessed practice in Special Education establishments around the world from America to Taiwan and right across the United Kingdom. The last observation report TalkSense produced ran to almost 30 pages of suggestions for practice with no criticisms of staff members although noting concerns were these were health and safety issues or practice which was falling below the accepted norm.
Bibliography and References

The Bibliography and Reference section of this page aims to be comprehensive and provide the details of all sources cited as well as to suggest further reading/study material.
Please note that items are arranged alphabetically by primary author and then by date order for each reference listed under that source.
Please note that items highlighted in blue provide a link to the original article such that you may read it for yourself. While the links were active at the time of composing this webpage they may become inactive at some future point; apologies if this is the case.
If TalkSense has cited a source on this webpage which is not referenced below please use the above contact form to let us know such that we may correct this issue.
Abery, B.H., Arndt, K., Greger, P., Tetu, L., Eggebeen, A., Barosko, J., & Rudrud, L. (1994). Self-determination for youth with disabilities: A family education curriculum. Minneapolis, MN: University of Minnesota, Institute on Community Integration
Abery, B.H., McGrew, K., & Smith, J. (1994). Validation of an ecological model of self-determination
for children with disabilities (Technical Report No. 2). Minneapolis, MN: University of Minnesota, Institute on Community Integration.
Abery, B.H., & Eggebeen, A. (1995). Findings from a field-test of a self-determination capacity building curriculum (Technical Report No. 3). Minneapolis, MN: University of Minnesota, Institute on Community Integration.
Abery, B.H., Stancliffe, R.J., Smith, J., McGrew, K., & Eggebeen, A. (1995a). Minnesota opportunities and exercise of self-determination scale - Adult edition. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living.
Abery, B.H., Stancliffe, R.J., Smith, J., McGrew, K., & Eggebeen, A. (1995b). Minnesota self-determination skills, attitudes, and knowledge evaluation scale - Adult edition. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living.
Abery, B.H., & Stancliffe, R.J. (1996). The ecology of self-determination. In D.J. Sands & M.L. Wehmeyer (Eds.), Self-determination
across the life span: Independence and choice for people with disabilities (pp. 111 – 145). Baltimore, MD: Paul H. Brookes.
Abery, B.H., Simunds, E., & Cady, R. (2002). The Minnesota health care self-determination scales. Minneapolis, MN: University of Minnesota, Institute on Community Integration.
Abery, B.H., & Stancliffe, R.J. (2003). A tripartite theory of self-determination. In M.L. Wehmeyer, B.H. Abery, D.E. Mithaug, & R.J.
Stancliffe (Eds.), Theory in self-determination: Foundations for educational practice (pp. 43 – 78). Springfield, IL: Charles C Thomas Publisher.
Abery, B.H., Simunds, E., & Cady, R. (2006). The impact of health care coordination on the lives of adults with physical disabilities (Technical Report No. 2). Minneapolis, MN: University of Minnesota, Institute on Community Integration.
Abery, B.H., & Ticha, R. (2012). Direct support professionals: Core competencies and their impact on self-determination. Paper presented
at the International Association for the Scientific Study of Intellectual Disabilities World Congress, Halifax, N.S., Canada
Adamek, M.S., & Darrow, A. (2005). Music in Special Education. Silver Springs: MD, The American Music Therapy Association
Adams, D. & Oliver, C. (2011). The expression and assessment of emotions and internal states in individuals with severe or profound intellectual disabilities. Clinical Psychology Review, Volume 31(3), pp. 293 – 306
Adams, G., Tallon, R., & Stangl, J. (1980). Environmental influences on self stimulatory behaviour. American Journal of Mental Deficiency, Volume 85, pp. 171 - 175
Adams, M., & Oldfield, A. (1990). The effects of music therapy on a group of profoundly mentally handicapped adults. Journal of Mental Deficiency Research, Volume 34(2), pp. 107 - 125.
Ager, A., & O’May, F. (2001). Issues in the definition and implementation of “best practice” for staff delivery of interventions for challenging behaviour. Journal of Intellectual and Developmental Disability, Volume 26(3), pp. 243 - 256
Agrotou, A. (1998). Psychodynamic Group Music Therapy with Profoundly Learning Disabled Residents and their Carers: Developing a Theory and Practice for Practice for the Realisation of Therapeutic Aims for Residents and the Acquirement of Therapist's Skills by Carers. Unpublished Doctoral Thesis. University of Sheffield.
Agrotou, A. (1999). Sounds and Meaning: Group Music Therapy with People with Profound Learning Difficulties and their Carers. London: Lumiere.
Aharoni, H. (2005). Adapted physical activities for the intellectually challenged adolescent: psychomotor characteristics and implications for programming and motor intervention. International Journal of Adolescent Medicine and Health, Volume 17(1), pp. 33 - 47
Aiken, J.M., & Salzberg, C.L. (1984). The effects of a sensory extinction procedure on stereotypic sounds of two autistic children. Journal of Autism and Developmental Disorders, Volume 14(3), pp. 291 - 299
Ainscow, M., & Tweddle, D. (1979). Preventing classroom failure: An objectives approach. Wiley
Aird, R. (2001). The Education and Care of Children with Severe, Profund and Multiple Learning Disabilities. David Fulton Publishers
Aitken, S., Buultjens, M., & Spungin, S. (Eds)(1990). Realities and Opportunities. Early Intervention with Visually Handicapped Infants and Young Children. American Foundation for the Blind: New York.
Aitken, S., & Buultjens, M. (1991). Visual Assessments of Children with Multiple Impairments: A Survey of Ophthalmologists. Journal of Visual Impairment and Blindness, Volume 85(4), Volume 170 - 173
Aitken, S., & Buultjens, M. (1992). Vision for Doing: Assessing Functional Vision of Learners who are Multiply Disabled. Sensory Series No. 2. Moray House Publications
Aitken, S., Buultjens, M., Clark, C., Eyre, J. T., & Pease, L. (2000). Understanding deafblindness. Teaching children who are deafblind: Contact communication and learning, pp. 1 - 34
Aldridge, D., Gustorff, D., & Neugebauer, L. (1995a). A preliminary study of creative music therapy in the treatment of children with developmental delay. The Arts in Psychotherapy, Volume 22(3), pp. 189 - 205.
Aldridge, D., Gustroff, D., & Neugebauer, L. (1995b). A pilot study of music therapy in the treatment of children with developmental delay. Complementary Therapies in Medicine, Volume 3(4), pp. 197 - 205.
Algozzine, B., Browder, D., Karvonen, M., Test, D.W., & Wood, W.M. (2001). Effects of interventions to promote self-determination for individuals with disabilities. Review of Educational Research, Volume 71(2), pp. 219 – 277.
All, A.C., Loving, G.L., & Crane, L.L. (1999). Animals, horseback riding, and implications for rehabilitation therapy. Journal of Rehabilitation, Volume 65(3), pp. 49 – 57
Allen, C. (2001). A Framework for Learning: For Adults with Profound and Complex Learning Difficulties. David Fulton
Allen, D., Mcdonald, L., Dunn, C., & Doyle, T. (1997). Changing care staff approaches to the prevention and management of aggressive behaviour in a residential treatment unit for persons with mental retardation and challenging behaviour. Research in Developmental Disabilities. Volume 18(2), pp.101 - 112
Alvin, J., & Warwick, A. (1991). Music Therapy for the Autistic Child. Oxford: Oxford University Press
Amaral, I., & Celizic, M. (2015). Quality indicators in the education of children with Profound Intellectual and Multiple Disabilities. Da Investigação às Práticas, Volume 5(2), pp. 112 - 125
Amen, D.G. (2010). Change your brain: Change your body. Three Rivers Press
Amen, D.G. (2016). Change Your Brain, Change Your Life: Revised and Expanded Edition: The breakthrough programme for conquering anxiety, depression, anger and obsessiveness. Piatkus
Amen, D.G. (2017). Memory Rescue: Supercharge Your Brain, Reverse Memory Loss, and Remember What Matters Most. Tyndale Momentum
Amsterdam, B. (1972). Mirror self-image reactions before the age 2. Developmental Psychobiology, Volume 5, pp. 297 – 305
Anderson, J.R. (1994). The monkey in the mirror: The strange conspecific. In Self-awareness in animals and humans: Developmental perspectives, ed. R. W. Mitchell, S.T. Parker, & M.L. Boccia, pp. 315 - 329. New York: Cambridge University Press
Angell, A. (2010). Selective Eaters and Tactile Sensitivity A Review of Classification and Treatment Methods That Address Anxiety and Support a Child’s Need for a Sense of Control. Childhood Obesity and Nutrition. Volume 2(5), pp. 299 - 303
Antaki, C., Finlay, W., Walton, C., & Pate, L. (2008). Offering choices to people with intellectual disabilities: an interactional study. Journal of Intellectual Disability Research, Volume 52(12), pp. 1165 - 1175
Apostolova, L.G., & Thompson, P.M. (2007). Brain Mapping as a Tool to Study Neurodegeneration. Neurotherapeutics: The Journal of the American Society for Experimental NeuroTherapeutics. Volume 4, pp. 387 – 400
Appleton, P.L., Mincham, P.E., Ellis, N.C., Elliott, C.E., Boll, V., & Jones, P. (1994). The self-concept of young people with spina bifida: A population-based study. Developmental Medicine and Child Neurology, Volume 36, pp. 198 - 215
Aquilla, P., Sutton, S., & Yack, E. (2003). Building Bridges Through Sensory Integration. Future Horizons.
Arendt, R., MacLean, W. E., Jr., & Baumeister, A. (1988). Critique of sensory integration therapy and its application in mental retardation.
American Journal on Mental Retardation, Volume 92, pp. 401 - 411
Ari, C., & D’Agostino, D.P. (2016). Contingency checking and self-directed behaviors in giant manta rays: Do elasmobranchs have self-awareness? Journal of Ethology, Volume 34(2), pp.167 – 174
Arkwright, N. (1998). An Introduction to Sensory Integration. San Antonio, Texas: therapy Skill Builders
Armstrong, L.E., Ganio M.S., Casa D.J., Lee E.C., McDermott B.P., Klau J.F., Jimenez L., Le Bellego L., Chevillotte E., & Lieberman H.R. (2012) Mild dehydration affects mood in healthy young women. Journal of Nutrition. Volume 142. pp. 382 - 388
Arthur, M., Hook, J., & Butterfield, N. (1995). Behavior state: Exploring issues in best practice for students with the most severe and multiple disabilities. Australasian Journal of Special Education, Volume 19, pp. 37 - 44
Arthur, M. (2000). Behavior states and a half-full glass: A response to Mudford, Hogg, and Roberts. American Journal on Mental Retardation, Volume 105(6), pp. 509 - 511
Arthur, M., & Foreman, P. (2002). Educational programming for students with high support needs: Report data from teachers, paraprofessionals and other professionals working in Australian schools. Developmental Disabilities Bulletin, Volume 30, pp.115 – 39
Arthur, M. (2003). Socio-communicative variables and behavior states in students with profound and multiple disabilities: Descriptive data from school settings. Education and Training in Developmental Disabilities, Volume 38(2), pp. 200 - 219
Arthur, M. (2004). Patterns amongst behavior states, sociocommunicative, and activity variables in educational programs for students with profound and multiple disabilities. Journal of Development and Physical Disabilities, Volume 16(2), pp. 125 - 149
Arthur-Kelly, M., Bochner, S., Center, Y., & Mok, M. (2007). Socio-communicative perspectives on research and evidence-based practice in the education of students with profound and multiple disabilities. Journal of Developmental and Physical Disabilities, Volume 19(3), pp. 161 – 76.
Arthur-Kelly, M., Foreman, P., Bennett, D., & Pascoe, S. (2008).Interaction, inclusion and students with profound and multiple disabilities: towards an agenda for research and practice. Journal of Research in Special Educational Needs, Volume 8(3), pp. 161 – 166
Arthur-Kelly, M., Bennett, D., Neilands, J., & Foreman, P. (2014). Case Reflections on Communication Support for Students with Multiple and Severe Disability in Australian General Classrooms. Journal of International Special Needs Education, Volume 17(2), pp. 70 - 78
Arthur-Kelly, M., Foreman, P., Maes, B., Colyvas, K., & Lyons, G. (2017). Observational Data on Socio-Communicative Phenomena in Classrooms Supporting Students with Profound Intellectual and Multiple Disability (PIMD): Advancing Theory Development on Learning and Engagement Through Data Analysis. Advances in Neurodevelopmental Disorders, pp. 1 - 13
Ashby, E. (2011). Resourceful, skillful and flexible: Art therapy with people who have severe learning disabilities and challenging behaviour. In - A. Gilroy (Ed.) Art therapy research in practice, pp.159 – 180. London: Routledge.
Ashby, M., Lindsay, W.R., Pitcaithly, D., Broxholme, S., & Geelen, N. (1995). Snoezelen: Its effects on concentration and responsiveness in people with profound multiple handicaps. British Journal of Occupational Therapy, Volume 58(7), pp. 303 - 307.
Association of Teachers and Lecturers (2013): Achievement For All: Working with children with special educational needs in mainstream schools and colleges, ATL
Augusta, C., Burd, C., Pica, M., & Schroeder, T. (2012). “Sing a song of six paints”: A collaborative approach to art and music in the classroom. Closing the Gap Magazine, Volume 30(6), pp. 24 - 28
Ault, M.M., Guy, B., Rues, J., Noto, L., & Guess, D. (1994). Some educational implications for students with profound disabilities at risk for inadequate nutrition and the nontherapeutic effects of medication. Mental Retardation, Volume 32(3), pp. 200 - 205
Ayres, A.J. (1963). The development of perceptual–motor abilities: A theoretical basis for treatment of dysfunction (Eleanor Clarke Slagle Lecture). American Journal of Occupational Therapy, Volume 17, pp. 221 – 225
Ayres, A.J. (1964). Tactile Functions: Their Relations to Hyperactive and Perceptual Motor Behaviour. American Journal of Occupation Therapy, Volume 18(1), pp. 221 - 225
Ayres, A.J. (1970). Sensory Integration and the Child. Western Psychological Services
Ayres, A.J. (1972). Improving academic scores through sensory integration. Journal of Learning Disabilities, Volume 5, pp. 338 – 343.
Ayres, A.J. (1973). Sensory Integration and Learning Disorders. Western Psychological Services.
Ayres, A.J. (1974). The Development of Sensory Integrative Theory and Practice: A Collection of the Works of A. Jean Ayres. Kendall/Hunt Publishing Co
Ayres, A.J. & Tickle, L. (1980). Hyper-responsivity to Touch and Vestibular Stimulation as a Predictor or Responsivity to sensory Integrative Procedure by Autistic Children. American Journal of Occupation Therapy, Volume 34, pp. 375 - 381
Ayres, A.J., Erwin, P.R., & Mailloux, Z. (2004). Love, Jean: Inspiration for Families Living With Dysfunction of Sensory Integration. Crestport Press
Azeredo, M. (2007). Real-time composition of image and sound in the (re)habilitation of children with special needs: A case study of a child with cerebral palsy. Digital Creativity, Volume 18(2), pp. 115 - 120.
Azrin, N.H., Hutchinson, R.R., & Sallery, R.D. (1964). Pain-aggression toward inanimate objects. Journal of the Experimental Analysis of Behavior, Volume 7, pp. 223 - 228.
Azrin, N.H., & Foxx, R.M. (1971). A rapid method of toilet training the institutionalized retarded. Journal of Applied Behavior Analysis, Volume 4, pp. 89 - 99
Azrin, N.H., Schaeffer, R.M., & Wesolowski, M.D. (1976). A rapid method of teaching profoundly retarded persons to dress by a reinforcement - guidance method. Mental Retardation. Volume 14(6), pp. 29 - 33
Bach-y-Rita, P., & Kercel, S.W. (2003). Sensory substitution and the human–machine interface. Trends in Cognitive Sciences, Volume 7(12), pp. 541 - 546
Bagadia, N., Berta, J., Kobs, R., Mahan, T., & Myers, K. (2001). Sensory Substitution for Vestibular Function Deficit. University of Wisconsin-Madison
Bailey, B.A. Hare, D.J., Hatton, C., & Limb, K. (2006). The response to challenging behaviour by care staff: Emotional responses, attributions of cause and observations of practice. Journal of Intellectual Disability Research, Volume 50(3), pp. 199 – 211
Bailey, J.S., & Meyersen, L. (1969). Vibration as a reinforcer with a profoundly retarded child. Journal of Applied Behavior Analysis, Volume 2, pp. 135 - 137
Bailey, M. (1983). Structuring a Curriculum for Profoundly Mentally Handicapped Children. Jordanhill Project. Glasgow
Baillargeon, R., Spelke, E.S., & Wasserman, S. (1985). Object permanence in five-month-old infants. Cognition, Volume 20(3), pp. 191 - 208
Baillargeon, R. (1987). Object permanence in 3½-and 4½-month-old infants. Developmental Psychology, Volume 23(5), pp. 655 - 664
Baker, D.J., Fox, J., & Albin, R.W. (1995). Staff support strategies to increase the involvement of individuals with disabilities in meal preparation. Behavioral Interventions, Volume 10(4), pp. 197 - 210
Baker, F.A., Berlowitz, D.J., Grocke, D., & Tamplin, J. (2014). Thematic analysis of the experience of group music therapy for people with chronic quadriplegia. Topics in Spinal Cord Injury Rehabilitation, Volume 20(3), pp. 236 - 247.
Baker, L.B., Conroy, D.E., & Kenney, W.L. (2007). Dehydration impairs vigilance-related attention in male basketball players. Medicine & Science in Sports & Exercise. Volume 39. pp. 976 - 983
Balcombe, J. (2016). What a Fish Knows: The Inner Lives of Our Underwater Cousins. Scientific American
Baldwin, J.M. (1895). Mental development in the child and the race: Methods and processes. New York: Macmillan
Bambara, L.M., Ager, C., & Koger, F. (1994). The effects of choice and task preference on the work performance of adults with severe disabilities. Journal of Applied Behavior Analysis, Volume 27(3), pp. 555 - 556.
Bandura, A. (1977). Self-efficacy: toward a unifying theory of behavioral change, Psychological Review, Volume 84(2), pp. 191 – 215
Bang, C. (2009). A world of sound and music: Music therapy for deaf, hearing impaired and multi-handicapped children and adolescents. Approaches: Music Therapy & Special Music Education, Volume 1(2), pp. 93 - 103.
Baniel, A., & Sharp, N. (2013). Leveraging the Power of the Brain to Change Itself to Transform Clinical Outcomes With Adults and Children With Special Needs With the Anat Baniel Method. Global Advances in Health and Medicine. Volume 2 (supplement). S96
Baniel, A.(2016). Keynote Address: Thinking Outside the Box: The Anat Baniel Method (ABM). 2016 Hemispherectomy Conference and Family Reunion. Omni Interlocken Resort. Broomfield, Colorado
Bannerman, D.J., Sheldon, J.B., Sherman, J.A., & Harchik, A.E. (1990). Balancing the right to habilitation with the right to personal liberties: The rights of people with developmental disabilities to eat too many doughnuts and take a nap. Journal of Applied Behavior Analysis, Volume 23, pp. 79 - 89.
Bannerman-Haig, S. (1997). Facilitating Change: Dance/Movement Therapy for Children and Adolescents with Profound and Multiple Learning Difficulties, Dance and the Child. UK Chapter, Journal 4, Focus on Dance Movement Therapy 2
Bannerman-Haig, S. (2006). Stretching, tension and kicking: Aspects of infantile movement in dance movement therapy with children and adolescents in special education, in Payne,H. Dance Movement Therapy. Theory, Research and Practice, 2nd Edition (First edition
published in 1992), pp. 87 - 100
Bar-David, Y., Urkin J., & Kozminsky, E. (2005) The effect of voluntary dehydration on cognitive functions of elementary school children. Acta Paediatrica. Volume 94. pp. 1667 - 1673
Baranek, G.T., & Berkson, G. (1994). Tactile Defensiveness in Children with Developmental Disabilities: responsiveness and habituation. Journal of Autism and Developmental Disorders, Volume 24(4), pp. 457 - 471
Baranek, G.T., Foster, L.G., & Berkson, G. (1997). Sensory Defensiveness in Persons With Developmental Disabilities. The Occupational Therapy Journal of Research, Volume 17(3), pp. 173 - 185
Baranek, G.T. (2002). Efficacy of Sensory and Motor Interventions for Children with Autism. Journal of Autism and Developmental Disorders, Volume (32(5), pp. 397 – 422
Barber, M. (1994). Contingency Awareness: putting research into the classroom. In - J. Coupe O’Kane & B. Smith (eds), Taking Control:enabling people with learning difficulties. London: David Fulton.
Barber, M. (2007). Imitation, interaction and dialogue using Intensive Interaction: tea party rules, Support for Learning, Volume 22 (3): pp.124 – 130.
Barksdale, A.L. (2003). Music therapy and leisure for persons with disabilities. Sagamore Publishing
Barnes, D. (1976). From Communication to Curriculum. Penguin
Baron-Cohen, S., Leslie, A., & Frith, U. (1985). Does the autistic child have a “theory of mind”? Cognition, Volume 21, pp. 37 - 46.
Baron-Cohen, S. (1989). The autistic child's theory of mind: A case of specific developmental delay. Journal of Psychology and Psychiatry, Volume 30, pp. 285 - 297.
Baron-Cohen, S. (2000). The cognitive neuroscience of autism: Evolutionary approaches. In The New Cognitive Neurosciences (2nd ed.), ed. M. Gazzaniga, pp. 1249 - 1257. Cambridge, MA: MIT press
Barrera, F.J., Violo, R.A., & Graver, E.E. (2007). On the form and function of severe self-injurious behavior. Behavioral Interventions, Volume 22(1), pp. 5 - 33
Bartheld, C.S., Bahney, J., & Herculano‐Houzel, S. (2016). The search for true numbers of neurons and glial cells in the human brain: a review of 150 years of cell counting. Journal of Comparative Neurology, Volume 524(18), pp. 3865 - 3895
Bartlo, P., & Klein, P.J. (2011). Physical activity benefits and needs in adults with intellectual disabilities: Systematic review of the literature. American Journal on Intellectual and Developmental Disabilities, Volume 116(3), pp. 220 – 232
Basil, C. (1986). Social interaction and learned helplessness in nonvocal severely handicapped children. Presentation at 4th Biennial Conference on AAC, Cardiff
Basil, C. (1992). Social interaction and learned helplessness in severely disabled children, AAC, Volume 8, pp. 188 - 199
Bass, M.M., Duchowny, C.A., & Liabra, M.M. (2009). The effect of therapeutic horseback riding on social functioning in children with autism. Journal of Autism and Developmental Disorders. Volume 39. pp.1261 – 1267
Battro, A.M., Fischer, K.W., & Lena, P.J. (Eds.)(2008). The Educated Brain: Essays in Neuroeducation. Cambridge University Press
Bauer, B. (1977a). Tactile sensitivity: development of a behavioral responses checklist. American Journal of Occupational Therapy, Volume 31(6), pp. 357 - 361
Bauer, B. (1977b). Tactile-sensitive behavior in hyperactive and non-hyperactive children. American Journal of Occupational Therapy, Volume 31(7), pp. 446 - 453
Baumeister, A.A., & MacLean, W.E. (1984). Deceleration of self-injurious and stereotypic responding by exercise. Applied Research in Mental Retardation, Volume 5, pp. 385 - 393
Baumeister, R.F. (1999). The nature and structure of the self: An overview. In R. Baumeister (Ed.), The self in social psychology (pp. 1–21). Philadelphia, PA: Psychology Press
Baumeister, R.F., & Vohs, K.D. (2007). Self-Regulation, Ego Depletion, and Motivation. Social and Personality. Psychology Compass, Volume 1(1). pp. 115 – 128
Beadle‐Brown, J., Hutchinson, A., & Whelton, B. (2012). Person‐Centred Active Support – Increasing Choice, Promoting Independence and Reducing Challenging Behaviour. Journal of Applied Research in Intellectual Disabilities, 2012, Volume 25(4), pp. 291 - 307
Beadle‐Brown, J., Leigh, J., Whelton, B., Richardson, L., Beecham, J., Baumker, T., & Bradshaw, J. (2016). Quality of life and quality of support for people with severe intellectual disability and complex needs. Journal of Applied Research in Intellectual Disabilities, Volume 29(5), pp. 409 - 421
Beange, H., Gale, L., & Stewart, L. (1995). Project renourish: a dietary intervention to improve nutritional status in people with multiple disabilities. Australia and New Zealand Journal of Developmental Disabilities, Volume 20(3), pp. 165 - 174
Beange, H., McElduff, A., & Baker, W. (1995). Medical disorders of adults with mental retardation: a population study. American Journal on Mental Retardation. Volume 99(6), pp. 595 - 604
Begley, A., & Lewis, A. (1998). Methodological issues in the assessment of the self-concept of children with Down syndrome. Child Psychology and Psychiatry Review, Volume 3, pp. 33 - 40
Begley, S. (2009). The Plastic Mind. Ballantine Books: New York
Belfiore, P.J., Browder, D.M., & Mace, F.C. (1993). Effects of community and center-based settings on the alertness of persons with profound mental retardation. Journal of Applied Behavior Analysis, Volume 26(3), pp. 401 - 402
Belfiore, P.J., Browder, D.M. & Mace, C.J. (1994). Assessing choice-making and preference in adults with profound mental retardation across community and center-based settings. Journal of Behavioral Education. Volume 4(2), pp. 217 – 226
Bellamy, G., Croot, L., Bush, A., Berry, H., & Smith, A. (2010). A study to define: profound and multiple learning disabilities (PMLD). Journal of Intellectual Disabilities, Volume 14, pp. 221 – 235
Belva, B.C., Matson, J.L., Sipes, M., & Bamburg, J.W. (2012). An examination of specific communication deficits in adults with profound intellectual disabilities. Research in Developmental Disabilities, Volume 33(2), pp. 525 - 529
Ben-Artzi, E., Mikulincer, M., & Glaubman, H. (1995) The multifaceted nature of self-consciousness: Conceptualization, measurement, and consequences, Imagination, Cognition and Personality, Volume 15(1), pp. 17 – 43
Benda, W., McGibbon, N.H., & Grant, K.L. (2003) Improvements in Muscle Symmetry in Children with Cerebral Palsy After Equine-Assisted Therapy (Hippotherapy). The Journal of Alternative and Complementary Medicine. Volume 9(6), pp. 817- 825.
Benson, G., Abbeduto, L., Short, K., Bibler-Nuccio, J., & Maas, F. (1993). Development of a theory of mind in individuals with mental retardation. American Journal on Mental Retardation, Volume 98, pp. 427 - 433
Benson, J.D., Beeman, E., Smitsky, D., & Provident , I. (2011). The Deep Pressure and Proprioceptive Technique (DPPT) Versus Nonspecific Child-Guided Brushing: A Case Study. Journal Of Occupational Therapy, Schools, & Early Intervention. Volume 4(3-4), pp. 204 - 214.
Benton, D., & Burgess, N. (2009) The effect of the consumption of water on the memory and attention of children. Appetite. Volume 53. pp. 143 - 146
Bergouignan, L., Nyberg, L., & Ehrsson, H.H. (2014). Out-of-body induced hippocampal amnesia. Proceedings of the National Academy of Sciences, Volume 111(12), pp. 4421 – 4426
Bergström, H., Hagströmer, M., Hagberg, J., & Elinder, L.S. (2013). A multi-component universal intervention to improve diet and physical activity among adults with intellectual disabilities in community residences: a cluster randomised controlled trial. Research in Developmental Disabilities, Volume 34(11), pp. 3847 - 3857
Berrol, C.F. (1981). A neurophysiologic approach to dance/movement therapy: Theory and practice. American Journal of Dance Therapy, Volume 4(1), pp. 72 - 84
Bersani, H.A., & Heifetz, I.J. (1985). Perceived stress and satisfaction of direct care staff members in community residences for mentally retarded adults. American Journal of Mental Deficiency, Volume 90, pp. 289 - 295
Bertolami, M.D., & Martino, L.A. (2002). Music therapy in a private school for visually impaired and multiply handicapped children. Voices: A World Forum for Music Therapy, Volume 2(1), Retrieved from https://normt.uib.no/index.php/voices/article/viewArticle/69/59.
Beveridge, M., & Berry, P. (1977). Observing interactions in severely mentally handicapped children. Research in Education. Volume 17, pp. 13 - 22
Beveridge, M., & Hurrell, P. (1979). Teachers' responses to severely mentally handicapped children. Journal of Child Psychiatry. Volume 21, pp. 175 - 181
Beveridge, M. (Ed.) (1982). Children thinking through language. London: Edward Arnold
Beveridge, M., & Conti- Ramsden, G. (1987). Children with language disabilities. Open University Press: ISBN 0-335-10279-4
Beveridge, M., Conti- Ramsden, G., & Leudar, I. (Eds.)(1988). Languages and communication in mentally handicapped people. London: Chapman and Hall
Bexkens, A., Ruzzano, L., Collot d'Escury‐Koenigs, A.M.L., Van der Molen, M.W., & Huizenga, H.M. (2014). Inhibition deficits in individuals with intellectual disability: a meta‐regression analysis. Journal of Intellectual Disability Research, Volume 58(1), pp. 3 - 16
Bhaumik, S., Watson, J.M., Thorp, C.F., Tyrer, F., & McGrother, C.W. (2008). Body mass index in adults with intellectual disability: distribution, associations and service implications: a population‐based prevalence study. Journal of Intellectual Disability Research, Volume 52(4), pp. 287 - 298
Bidabe, L., & Lollar, J.M. (1995). MOVE (Mobility Opportunities Via Education). 3rd edition. Kern Country Superintendent of Schools, Bakersfield.
Biddiss, E., Blain-Moraes, S., Chesser, S., Kingsnorth, S., & McKeever, P. (2013). Biomusic: A novel technology for revealing personhood of people with profound multiple disabilities. Augmentative and Alternative Communication, Volume 29(2), pp. 159 - 173
Bigby, C., Clement, T., Mansell, J., & Beadle-Brown, J. (2009). ‘It’s pretty hard with our ones, they can’t talk, the more able bodied can participate’: Staff attitudes about the applicability of disability policies to people with severe and profound intellectual disabilities. Journal of Intellectual Disability Research. Volume 53, pp. 363 – 376
Birch, T., Cross, A., Dumble, M., & Park, K. (2000): Switching on to Stories: AAC Use and Storytelling with Children with Severe and Profound Learning Disabilities. Communication Matters. Volume 14 (2), pp. 2 - 4
Birdi, K.S. (2005). No idea? Evaluating the effectiveness of creativity training. Journal of European Industrial Training, Volume 29(2), pp. 102 - 111
Biringer, F., & Anderson., J.R. (1993). Self-recognition in Alzheimer’s disease: Use of mirror and video techniques and enrichment. In Recent Advances in Aging Science (Volume 1), ed. I. Beregi, & K. Rajczi, pp. 697 - 705. Bologna: Monduzzi Editore.
Bizub, A.L., Ann, J., & Davidson, L. (2003). It’s like being in another world: Demonstrating the benefits of therapeutic horseback riding for individuals with psychiatric disability. Psychiatric Rehabilitation Journal, Volume 26(4), pp. 377 – 384
Blacher J., & McIntyre L.L. (2006). Syndrome specificity and behavioural disorders in young adults with intellectual disability: cultural differences in family impact. Journal of Intellectual Disability Research. Volume 50, pp. 184 – 98
Blades, M. (2000). Autism: an interesting dietary case history. Nutrition & Food Science, Volume 30(3), pp. 137 - 140
Blaich, C., Wise, K., Pascarella, E.T., & Roksa, J. (2016). Instructional Clarity and Organization: It's Not New or Fancy, But It Matters. Change: The Magazine of Higher Learning, Volume 48(4), pp. 6 - 13
Blakemore, S., & Frith, U. (2005). The Learning Brain: lessons for education. Blackwell Publishing
Blanchard, K., & Johnson, S. (1983). The One Minute Manager. Fontana
Blanchard, K., & Lorber, R. (1984). Putting the One Minute Manager to Work. Fontana
Blanchard, K., Zigarmi, P., & Zigarmi, D. (1987). Leadership and the One Minute Manager. Fontana
Blanchard, K. (1999). Catch People Doing Something Right. Executive Excellence Publications
Blank, M., & Marquis, M.S. (1987). Directing Discourse, (Communication Skill Builders) Winslow Press
Block, N. (1995). On a confusion about a function of consciousness. Behavioral and Brain Sciences, Volume 18, pp. 227 – 247
Bloomberg, K., West, D., & Iacono, T.A. (2003). Picture it: An evaluation of a training program for carers of adults with severe and multiple disabilities. Journal of Intellectual & Developmental Disability, Volume 28, pp. 260 – 282
BMJ (2015). Get up and stand up for at least 2 hours daily during working hours. British Journal of Sports Medicine. Press Release
Boat, B. (2006). Clinical approaches to assessing and utilising animal-related experiences in therapeutic interventions with children, adolescents and their caregivers. In - Fine A.H. (ed.), Handbook on Animal Assisted Therapy: Theoretical Foundations and Guidelines for Practice. (3rd ed.). Elsevier, London
Bobzien, J.L. (2011). A review of curricular approaches and quality of life indicators in the United States for individuals displaying profound multiple disabilities. Social Welfare: Interdisciplinary Approach, Volume 1(2), pp. 8 – 22
Bobzien, J.L. (2014). Academic or Functional Life Skills? Using Behaviors Associated with Happiness to Guide Instruction for Students with Profound/Multiple Disabilities. Education Research International. Volume 2014, Article ID 710816, 12 pages
Bodde A.E., & Dong-Chul S. (2009). A review of social and environmental barriers to physical activity for adults with intellectual disabilities. Disability and Health Journal, Volume 2, pp. 57 - 66
Boe, R.B. (1977). Economical procedures for the reduction of aggression in a residential setting. Mental Retardation, Volume 15, pp. 25 - 28
Bolte Taylor, J. (2008). My Stroke of Insight. Hodder and Stoughton
Booker, M. (2011). Developmental Drama: Dramatherapy Approaches for People with Profound or Severe Multiple Disabilities, Including Sensory Impairment. Jessica Kingsley Publishers
Booth, P., Taylor, B., & Edmonds, C.J. (2012) Water supplementation improves visual attention and fine motor skills in schoolchildren. Education and Health. Volume 30. pp. 75 - 79
Borthwick-Duffy, S.A., Eyman, R.K., & White, J.F. (1987). Client characteristics and residential placement patterns. American Journal of Mental Deficiency, Volume 92, pp. 24 - 30
Borthwick-Duffy, S.A. (1990). Quality of life of persons with severe or profound mental retardation. In R. L. Schalock (Ed.), Quality of life: Perspectives and issues (pp. 177 - 189). American Association on Mental Retardation.
Borthwick-Duffy, S.A. (1994).Prevalence of Destructive Behaviours. In T.Thompson & D.B. Gray (Eds.) Destructive Behaviour in Developmental Disabilities: Diagnoses and Treatment. pp. 3 - 23. Thousand Oaks: Sage.
Bosch, J.J., & Ringdahl, J. (2001). Functional Analysis of problem behaviour in children with mental retardation: what is it and why should pediatric nurses care?. The American Journal of Maternal/Child Nursing, Volume 26(6), pp. 307 - 311
Bott, C., Farmer, R., & Rhode, J. (1997). Behaviour problems associated with lack of speech in people with learning disabilities. Journal of Intellectual Disability Research. Volume 41, pp. 3 - 7
Bouhadiba, Z., Dacher, J., Monroe, M., Vanhulle, C., Menard, J., & Kalifa, G. (2000). MRI of the brain in the evaluation of children with developmental delay. European Journal of Radiology, Volume 81. pp. 870 – 873
Bower, T.G.R., & Wishart, J.G. (1972). The effects of motor skill on object permanence. Cognition, Volume 1(2-3), pp. 165 - 172
Bower, T.G.R., & Paterson, J.G. (1972). Stages in the development of the object concept. Cognition, Volume 1(1), pp. 47 - 55
Boxall, K., & Ralph, S. (2009) Research ethics and the use of visual images in research with people with intellectual disabilities. Journal of Intellectual and Developmental Disability, Volume 34(1), pp. 45 - 5.
Boxall, K. (2010). Involving people with profound and multiple learning difficulties in research: barriers and possibilities. Disability Studies Conference Proceedings, University of Lancaster, September
Boxhill, E.H. (1981). A continuum of awareness: Music therapy with the developmentally handicapped. Music Therapy, Volume 1(1), pp. 43 - 49
Boxhill, E.H. (1985). Music therapy for the developmentally disabled. Austin, TX: PRO-ED.
Bradley, A. & Ouvry, C. (1999). Unit Six: Planning for everyday good practice. In J. Harris (ed.), Better Choices: Fuller Lives. Working with people with profound learning disability and complex support needs. First Draft Publications. BILD
Bradley, H. (1998). Assessing and Developing Successful communication, in Lacey, P., & Ouvry, C. (1998). People with Profound and Multiple Learning Disabilities – A collaborative approach to meeting complex needs. London: David Fulton Publishers
Bradley, J. (2012). The effect of choice for people with learning disabilities: A systematic review, Journal of Applied Research in
Intellectual Disabilities
Bradshaw, J. (2001). Communication Partnerships with People with Profound and Multiple Learning Disabilities. Tizard Learning
Disability Review, Volume 6(2), pp. 6 – 15
Bradshaw, J. (2001b). Complexity of staff communication and reported level of understanding skills in adults with intellectual disability. Journal of Intellectual Disability Research, Volume 45, pp. 233 – 243
Braitenberg, V. (2001). Brain size and number of neurons: an exercise in synthetic neuroanatomy. Journal of Computational Neuroscience, Volume 10(1), pp. 71 - 77
Bray, N., & Turner, L. (1986):The rehearsal deficit hypothesis. in - International Review of Research in Mental Retardation, Volume 14, pp. 47 - 71, Ellis, N. & Bray N. (Eds.). New York: Academic Press
Bray, N., & Turner, L. (1987): Production anomalies (not strategic deficiencies) in mentally retarded individuals. Intelligence, Volume 11, pp. 49 - 60
Bray, N. (1990): A cognitive model for Minspeak, 5th Annual Minspeak conference proceedings. November 14th -15th, Seattle, Washington
Wooster, OH: PRC
Breau, L.M., Camfield, C.S., McGrath, P.J., & Finley, G.A. (2003). The incidence of pain in children with severe cognitive impairments. Archives of Pediatrics & Adolescent Medicine, Volume 157(12), pp. 1219 - 1226
Breau, L.M., Camfield, C.S., Symons, F.J., Bodfish, J. W., McKay, A., & Finley, G.A. (2003). Pain and self-injurious behaviour in neurologically impaired children. Journal of Pediatrics, Volume 142(5), pp. 498 - 503
Breau L.M., Camfield C.S., Symons F.J., Bodfish J.W., MacKay A., Finley G.A., & McGrath, P.J. (2003). Relation between pain and self-injurious behavior in nonverbal children with severe cognitive impairments. Journal of Pediatrics. Volume 142(5), pp. 498 – 503.
Breau, L.M., & Burkitt, C. (2009). Assessing pain in children with intellectual disabilities. Pain Research & Management: The Journal of the Canadian Pain Society, Volume 14(2), pp. 116 -120
Brett-Green, B.A., Miller, L.J., Schoen, S.M., & Nielson, D.M. (2010). An exploratory event-related potential study of multisensory integration in sensory over-responsive children. Brain Research, Volume 1321, pp. 67 – 77
Bright, T., Bittick, K., & Fleeman, B. (1981). Reduction of self injurious behavior using sensory integrative techniques. American Journal of Occupational Therapy, Volume 35, pp. 167 – 172
Briscoe, G. (2002). Language, inner speech, and consciousness. Paper presented at the Association for the Scientific Study of Consciousness. Barcelona, Spain
Brodin, J. (2005). Diversity of aspects on play in children with profound multiple disabilities. Early Child Development and Care, Volume 175, pp. 635 - 646
Brody, J.F., Thomas, J.A., Brody, D.M., & Kucherawy, D.A. (1977). Comparison of sensory integration and operant methods for production of vocalization in profoundly retarded adults. Perceptual and motor skills, Volume 44(3 supplement), pp. 1283 - 1296
Broesch, T., Callaghan, T., Henrich, J., Murphy, C., & Rochat, P. (2011). Cultural variations in children’s mirror self-recognition. Journal of Cross-Cultural Psychology, Volume 40(6), pp. 1019 - 1031
Brotherson, S.E. (2005). Understanding brain development in young children. Fargo, ND: NDSU Extension Service
Browder, D.M., Cooper, K.J., & Lim, L. (1998). Teaching adults with severe disabilities to express their choice of settings for leisure activities. Education and Training in Mental Retardation and Developmental Disabilities, Volume 33, pp. 228 - 238
Browder, D.M, Wakeman, S.Y., Spooner, F., Ahlgrim-Delzell, L., & Algozzine, B. (2006). Research on reading instruction for individuals with significant cognitive disabilities, Exceptional Children, Volume 72(4), pp. 392 – 408
Browder, D.M, Wakeman, S.Y., Flowers, C., Rickelman, R.J., Pugalee, D., & Karvonen, M. (2007). Creating access to the general curriculum with links to grade-level content for students with significant cognitive disabilities: an explication of the concept, Journal of Special Education, Volume 41(1), pp. 2 – 16
Browder, D.M., Gibbs, S., Ahlgrim-Delzell, L., Courtade, G.R.,. Mraz, M., & Flowers, C. (2009). Literacy for students with severe developmental disabilities: what should we teach and what should we hope to achieve? Remedial and Special Education, Volume 30(5), pp. 269 – 282
Browder, D.M., & Spooner, F. (2011). Teaching Students with Moderate and Severe Disabilities. Guilford Publications
Browder, D. M., Wood, L., Thompson, J., & Ribuffo, C. (2014). Evidence-based practices for students with severe disabilities (Document No. IC-3). Retrieved from University of Florida, Collaboration for Effective Educator, Development, Accountability, and Reform Center website: http://ceedar.education.ufl.edu/wp-content/uploads/2014/09/IC-3_FINAL_03-03-15.pdf
Brown, F. (1991). Creative daily scheduling: A nonintrusive approach to challenging behaviors in community residences. Journal of the Association for Persons with Severe Handicaps, Volume 16, pp. 75 - 84
Brown, F. Appel, C., Corsi, L. & Wenig, B. (1993). Choice diversity for people with severe disabilities. Education & Training in Mental Retardation, Volume 28, pp. 318 - 326.
Brown, F., Gothelf, C.R., Guess, D., & Lehr, D.H. (1998). Self-determination for individuals with the most severe disabilities: Moving beyond chimera. Journal of the Association for Person with Severe Handicaps, Volume 23, pp. 17 – 26
Brown, I., & Brown, R.I. (2003). Quality of Life and Disability.. Jessica Kingsley
Brown, I., & Brown, R.I. (2009). Choice as an aspect of quality of life for people with intellectual disabilities. Journal of Policy and Practice in Intellectual Disabilities, volume 6 (1), pp.11 - 18
Brown, J.D. (2009). The Self. Routledge
Brown, L., Falvey, M., Vincent, L., Kage, N., Johnson, F., Fettara-Pattish, P., & Gruenewald, L. (1980). Strategies for generating comprehensive, longitudinal and chronological age appropriate individual educational plans for adolescent and young severely handicapped students. In L. Brown, M. Falvey, D. Baumgart, I. Pumpian, J. Schroeder, & L. Gruenewald (Eds.), Strategies for teaching chronological age appropriate functional skills to adolescent and young adult severely handicapped students (pp. 10 - 34). Madison, WI: University of Wisconsin-Madison and Madison Metropolitan School District.
Brown, L.S., & Jellison, J.A. (2012). Music research with children and youth with disabilities and typically developing peers: A systematic review. Journal of Music Therapy, Volume 49(3), pp. 335 - 364
Brown, N., McLinden, M., & Porter, J. (1998). Sensory needs in P. Lacey & C. Ouvry (eds), People with Profound and Multiple Learning Disabilities: A collaborative approach to meeting complex needs. London: David Fulton, pp. 29 - 38
Brown, R.I., Bayer, M.B., & Brown, P.M. (1992). Empowerment and Developmental Handicaps: Choices and Quality of Life. Toronto: Captus Press
Brown, S. (1994). Autism and music therapy - is change possible and why music? Journal of British Music Therapy, Volume 8(1), pp. 15 - 25
Browning, M. (1983). Identifying the Needs of Profoundly Mentally Handicapped Children. Jordanhill Project. Glasgow
Brownson, T. (2012). Seventy amazing facts about your brain. Biak.us
Brouns, B., Tap, R., Waninge, A., & Van der Woude, L.H.V. (2015). Applicability of a measurement method to determine the degree of daily movement of children with intellectual disabilities. Dutch magazine for care for people with intellectual disabilities. Volume 2. pp.121 - 131
Bruce, D.J. (1958). The Effect of Listeners' Anticipations on the Intelligibility of Heard Speech. Language and Speech, Volume 1(2), pp. 79 - 97
Bruce, S.M., Trief, E., & Cascella, P.W. (2011). Teachers’ and Speech-Language Pathologists’ Perceptions about a Tangible Symbols
Intervention: Efficacy, Generalization, and Recommendations. Augmentative and Alternative Communication, Volume 27 (3) , Pages 172 - 182
Bruininks, R.H., Olsen, K.M., Larson, S.A., & Lakin, K.C. (1994). Challenging behavior among persons with mental retardation in residential settings. In T. Thompson & D.B. Gray (Eds.), Destructive Behavior in Developmenal Disabilties: Diagnosis and Treatment. pp. 24 - 48. Thousand Oaks: Sage
Brylewski J., & Wiggs, L. (1999). Sleep problems and daytime challenging behaviour in a community-based sample of adults with intellectual disability. Journal of Intellectual Disability Research. Volume 43, pp. 504 – 512
Bubic, A., Striem-Amit, E., & Amedi, A. (2010). Large-Scale Brain Plasticity Following Blindness and the Use of Sensory Substitution Devices, in M.J. Naumer, & J. Kaiser (eds.), Multisensory Object Perception in the Primate Brain, chapter 18, pp. 351 - 380, Springer Science+Business Media
Buie, T. (2013). The relationship of autism and gluten. Clinical Therapeutics, Volume 35(5), pp. 578 - 583
Bull, S., & O’Farrell, K. (Eds.). (2012). Art therapy and learning disability: ‘Don’t guess my happiness’. Hove, Routledge.
Bullivant, M. (2015). Self-injurious Behaviour in Cornelia de Lange Syndrome. PMLD Link. Volume 27(2), Issue 81, pp. 23 - 25
Bullivant, M., & Jones, A.P. (2016). Sensory Stories Webpage. TalkSense Website
Bundy, A.C., Lane, S.J., & Murray, E.A. (2002). Sensory Integration: Theory and Practice. Second Edition. Philadelphia: F.A. Davis
Bunnell, T. (2007). Music Makes a Difference: A Practical Guide to Developing Music Sessions with People with Learning Disabilities. Keswick: M&K Update.
Bunning, K. (1998). To engage or not to engage? Affecting the interactions of learning disabled adults. International Journal of Language and Communication Disorders, Volume 33(Supplement), pp. 386 - 391
Burton, M., Kagan, C. & Clements. P. (1995). Social Skills for People with Learning Disabilities. Therapy in Practice Volume 48. Chapman and Hall
Bustad, L.K., & Hines, L. (1984). Historical perspectives of the human-animal bond. In - Anderson. R.K., Hart, B.L., & Hart, L.A. (eds.). The Pet Connection: Its Influence on Our Health and Quality of Life. Minneapolis: Centre to Study Human-Animal Relationships and Environments. University of Minnesota, Minnesota. pp.15 - 29
Butté, C. (2007). An Inquiry into the Use of Interpersonal Touch in Dance Movement Therapy with Adults with Profound and Multiple Learning Difficulties/Disabilities. Unpublished Master's Thesis. Dissertation DMT045L407Y. Roehampton University, London
Butté, C., & Unkovich, G. (2009). Foundations of Dance Movement Psychotherapy Practice in Profound and Multiple Learning Difficulties. E-Motion, Volume 19(4), pp. 25 -33
Buultjens, M., & Aitken, S. (1987). Assessment of vision in multiply impaired children. British Journal of Special Education, Volume 14(3), pp. 112 - 114
Byers, R. (1996). Classroom Processes in B. Carpenter, R. Ashdown, & K. Bovair (eds), Enabling Access - effective teaching and learning for learners with learning difficulties. London: David Fulton.
Byers, R. (1998) Managing the learning environment. In: P. Lacey and C. Ouvry (eds.), People with Profound and Multiple Learning Disabilities: a collaborative approach to meeting complex needs. London: David Fulton Publishers.
Byers, R. (1999). Experience and achievement: initiatives in curriculum development for learners with severe and profound and multiple learning difficulties. British Journal of Special Education, Volume 26(4), pp. 184 - 188
Caldwell, P. (1991) Stimulating People with Profound Handicaps. How can we work together? British Journal of Mental Subnormality. Volume 37,(2), pp. 92 - 100
Caldwell, P. (1997). 'Getting in touch' with people with severe learning disabilities. British Journal of Nursing, Volume 6(13), pp. 751 - 756
Caldwell, P. (1998). Person to Person: Establishing Contact and Communication with People with Profound Disabilities. Pavilion Publishing (Brighton) Ltd
Caldwell, P. (2006a). Finding You Finding Me: Using Intensive Interaction to get in touch with people whose severe learning disabilities are combined with autistic spectrum disorder. London: Jessica Kingsley Publishers
Caldwell, P. (2006b). Speaking the other's language: Imitation as a gateway to relationship. Infant and Child Development, Volume 15, pp. 275 - 282
Cambridge, P., & Carnaby, S. (2000). A personal touch: managing the risks of abuse during intimate and personal care. The Journal of Adult Protection, Volume 2(4), pp. 4 - 16
Cameron, L. & Bell, D. (2001). Enhanced Interaction Training: A method of multi-disciplinary staff training in Intensive Interaction to reduce challenging behaviour in adults who have learning disabilities and who also have a severe communication disorder, Working with People who have a Learning Disability, Volume 18, (3), pp. 8 - 15
Cameron, L., & Murphy, J. (2002). Enabling young people with learning disability to make choices at a time of transition. British Journal of Learning Disabilities, Volume 30, pp. 105 – 112
Cammaerts, M.C., & Cammaerts, R. (2015). Are Ants (Hymenoptera, Formicidae) Capable of Self Recognition? Journal of Science. Volume 5(7), pp. 521 - 532
Campo, S.F., Sharpton, W.R., Thompson, B., & Sexton, D. (1997). Correlates of the quality of life of adults with severe or profound mental retardation. Mental Retardation, Volume 35(5), pp. 329 - 337
Cannella, H.I., O’Reilly, M.F., & Lancioni, G.F. (2005). Choice and preference assessment research with people with severe to profound developmental disabilities: a review of the literature. Research in Developmental Disabilities, Volume 26, pp.1 – 15
Carmeli, E., Orbach, I., Zinger-Vaknin, T., Morad, M., & Merrick, J. (2008) Physical training and well-being in older adults with mild intellectual disability: A residential care study, Journal of Applied Research in Intellectual Disabilities, Volume 21, pp. 457 – 465
Carnaby, S., & Cambridge, P. (2002). Getting personal: an exploratory study of intimate and personal care provision for people with profound and multiple intellectual disabilities. Journal of Intellectual Disability Research, Volume 46(2), 120 - 132
Carnaby, S., & Cambridge, P. (2006). Intimate and personal care with people with learning disabilities. Jessica Kingsley Publishers
Carnaby, S., & Pawlyn, J. (2009). Profound intellectual and multiple disabilities: meeting complex needs through complex means, in - J. Pawlyn & S. Carnaby (eds), Profound Intellectual and Multiple Disabilities: Nursing Complex Needs. Oxford: Wiley Blackwell
Carpenter, B., Egerton, J., Cockbill, B., Bloom, T., Fotheringham, J., Rawson, H., & Thistlewaite, J. (2015). Engaging Learners with Complex Learning Difficulties and Disabilities. Oxon: Routledge
Carpenter, B., Egerton, J., Cockbill, B., Bloom, T., Fotheringham, J., Rawson, H., & Thistlewaite, J. (2015). Mental health and children with Complex Learning Difficulties and Disabilities, in - Carpenter B. et al (Ed.), Engaging Learners with Complex Learning Difficulties and Disabilities. Oxon: Routledge
Carr, E.G., Newsom, C.D., & Binkoff, J.A. (1976). Stimulus control of self-destructive behavior in a psychotic child. Journal of Abnormal Child Psychology, Volume 4, pp. 139 - 153
Carr, E.G. (1977). The motivation of self-injurious behaviour: A review of some hypotheses. Psychological Bulletin, Volume 84 (4), pp. 800 –816
Carr, E.G., & McDowell, J.J. (1980). Social control of self-injurious behavior of organic etiology. Behavior Therapy, Volume 11, pp. 402 - 409
Carr, E.G., Newsom, C.D., & Binkoff, J.A. (1980). Escape as a factor in the aggressive behavior of two retarded children. Journal of Applied Behavior Analysis, Volume 13, 101 - 117
Carr, E.G., & Durand, V.M. (1985a). Reducing behavior problems through functional communication training. Journal of Applied Behavior Analysis, Volume 18(2), pp. 111 - 126
Carr, E.G., & Durand, V.M. (1985b). The social communicative basis of severe behaviour problems in children, in S. Reiss and R. Bootzin (Eds.), Theoretical Issues in Behaviour Therapy. Academic Press, New York, pp. 219 - 54
Carr, E.G., & Newsom, C.D. (1985). Demand-related tantrums: Conceptualisation and treatment. Behavior Modification, Volume 9, pp. 403 - 426
Carr, E.G., Robinson, S., & Palumbo, L.W. (1990). The wrong issue: Aversive versus nonaversive treatment. The right issue: Functional versus nonfunctional treatment. In A. Repp & N. Singh (Eds.), Perspectives on the use of nonaversive and aversive interventions for persons
with developmental disabilities, pp. 361-379. Sycamore, IL: Sycamore.
Carr, E.G., Robinson, S., Taylor, J.C., & Carlson, J.I. (1990). Positive approaches to the treatment of severe behavior problems in persons with developmental disabilities: A review and analysis of reinforcement and stimulus-based procedures. Monograph of the Association
for Persons with Severe Handicaps, Volume 4.
Carr, E.G., Taylor, J.C., & Robinson, S. (1991). The effects of severe behavior problems in children on the teaching behavior of adults. Journal of Applied Behavior Analysis, Volume 24, pp. 523 - 535
Carr, E.G., & Carlson, J.I. (1993). Reduction of severe behavior problems in the community using a multicomponent treatment approach. Journal of Applied Behavior Analysis, Volume 26, pp. 157 - 172
Carr, E.G. (1994). Emerging themes in the functional analysis of problem behavior. Journal of Applied Behavior Analysis. Volume 27(2), pp. 393 - 399
Carr, E.G., Levin, L., McConnachie, G., Carlson, J.I., Smith, C.E., & Kemp, D.C. (1994). Communication-based intervention for problem behavior. Baltimore: Paul H. Brookes.
Carr, E.G., Levin, L, McConnachie, G., Carlson, J.I., Kemp, D.C., & Smith, C.E. (1997). Communication-baased Intervention for Problem Behavior: A User's Guide for Producing Positive Change. Paul H. Brookes
Carr, E.G., Yarbrough, S.C., & Langdon, N.A. (1997). Effects of idiosyncratic stimulus variables on functional analysis outcomes. Journal of Applied Behavior Analysis. Volume 30(4), pp. 673 - 686
Carsrud, A.L., Carsrud, K.B., & Standifer, J.T. (1980). Social variables affecting mental health in the geriatric mentally retarded: An exploratory study. Mental Retardation, Volume 18, pp. 88 - 90
Carsrud, A.L. (1986). Effects of structured social interaction with geriatric mentally retarded clients: An exploratory study. Journal of Psychology and Aging, Volume 1(1), pp. 78 - 79
Carter, E.W., Lane, K.L., Pierson, M.R., & Glaeser, B. (2006). Self-determination skills and opportunities of transition-age youth with emotional disturbance and learning disabilities. Exceptional Children, Volume 72, pp. 333 – 346
Carter, S. (1982). Music Therapy for Handicapped Children: Mentally Retarded. Washington D.C.: National Association for Music Therapy.
Cartwright, C., & Wind-Cowie, S. (2005). Profound and Multiple Learning Difficulties. Continuum International Publishing
Case-Smith, J. (1991). The effects of tactile defensiveness and tactile discrimination on in-hand manipulation skills. American Journal of Occupational Therapy, Volume 45, pp. 811 – 825
Cataldo, M.F., & Harris, J. (1982). The biological basis for self-injury in the mentally retarded. Analysis and Intervention in Developmental Disabilities, Volume 2, pp. 21 - 39
Cavet, J.(1989). Occupational and Leisure Activities for People with Profound Retardation and Multiple Impairments: A study of Creative Activities to Facilitate Social Integration. Hester Adrian Research Centre. University of Manchester.
Cavet, J. (1995). Leisure provision in Europe. In - J. Hogg & J. Cavet (Eds), Making leisure provision for people with profound learning and multiple disabilities. London: Chapman & Hall, pp. 49 - 64
CDC (Centers for Disease Control and Prevention)(2003). Prevalence of physical activity, including lifestyle activities among adults – USA. Morbidity and Mortality Weekly Report, Volume 52(32). pp. 764 - 769
Cecchi, G.A., Petreanu, L.T., Alvarez-Buylla, A., & Magnasco, M.O. (2001). Unsupervised learning and adaptation in a model of adult neurogenesis. Journal of Computational Neuroscience, Volume 11(2), pp. 175 - 182
Çetrez İscan, G., Nurcin, E., & Fazlioglu, Y. (2016). Effect of most-to-least prompting procedure on dressing skill of students with Autism. Educational Research and Reviews, Volume 11(18), pp. 1766 - 1774
Chadwick, D.D., & Joliffe, J. (2009). A pilot investigation into the efficacy of a signing training strategy for staff working with adults with intellectual disabilities. British Journal of Learning Disabilities, Volume 37, pp. 34 - 42
Chadwick, O., Piroth, N., Walker, J., Bernard, S., & Taylor, E. (2000). Factors affecting the risk of behaviour problems in children with severe intellectual disability. Journal of Intellectual Disability Research, Volume 44, pp. 108 – 123
Chadwick, O., Kusel, Y., & Cuddy, M. (2008). Factors associated with the risk of behaviour problems in adolescents with severe intellectual disabilities. Journal of Intellectual Disability Research, Volume 52(10), pp. 864 – 876
Chambers, C.R., Wehmeyer, M.L., Saito, Y., Lida, K.M., Lee, Y., & Singh, V. (2007). Self-determination: What do we know? Where do we go? Exceptionality, Volume 15, pp. 3 – 15
Chan, J.S., & Yau, M.K. (2002). A study on the nature of interactions between direct care staff and persons with developmental disabilities in institutional care. The British Journal of Developmental Disabilities, Volume 48(94), pp. 39 - 51
Chan, J.S., & Chien, W.T. (2017). A randomised controlled trial on evaluation of the clinical efficacy of massage therapy in a multisensory environment for residents with severe and profound intellectual disabilities: a pilot study. Journal of Intellectual Disability Research, Volume 61(6), pp. 532 - 548
Chandler, C. (2005). Animal Assisted Therapy in Counselling. Routledge, Taylor and Francis Group, New York
Chao, W.L. (2007). Face Recognition. GICE, National Taiwan University
Chapman, J.W. (1988). Learning disabled children’s self-concepts. Review of Educational Research, Volume 58(3), pp. 347 - 371
Chase, K.M. (2004). Music therapy assessment for children with developmental disabilities: A survey study. Journal of Music Therapy, Volume 41(1), pp. 28 - 54
Chesebro, J.L. (2003). Effects of teaching clarity and nonverbal immediacy on student learning, receiver apprehension, and affect. Communication Education, Volume 52(2), pp. 135 - 147
Chesner, A. (1995). Dramatherapy for people with Learning Disabilities. Jessica Kingsley: London
Chiang, J.Y.K. (2008). Music therapy for young children who have special needs: The music Therapy experience from the perspectives of carers and professionals. Master's Degree Dissertation: New Zealand School of Music, Wellington
Cian, C., Koulmann, N., Barraud, P.A., Raphel, C., Jimenez, C., & Melin, B. (2000). Influences of variations in body hydration on cognitive function: Effect of hyper-hydration, heat stress, and exercise-induced dehydration. Journal of Psychophysiology. Volume 14. pp. 29 - 36
Cipani, E. (1981). Modifying food spillage behavior in an institutionalized retarded client. Journal of behavior therapy and experimental psychiatry, Volume 12(3), pp. 261 - 265
Clark, F.A., Miller, L.R., Thomas, J.A., Kucherway, O,A,, & Azin S.P. (1978). A comparison of operant and sensory integration methods on vocalizations and other developmental parameters in profoundly retarded adults. American Journal of Occupational Therapy, Volume 32, pp. 86 - 93
Clark, F.A., & Shuer, J. (1978). A clarification of sensory integrative therapy and its application to programming with retarded people. Mental Retardation, Volume 16, pp. 227 - 232
Clark, P. (1988). Adapting signs for deaf-blind children. Talking Sense, Volume 34(1), pp. 16 - 17
Clark, S. (1991). Children with Profound / Complex Physical and Learning Difficulties. NCSE (Reprint 1993 by NASEN)
Clayton, J., Burdge, M., Denham, A., Kleinert, H.L., & Kearns, J. (2006). A four-step process for accessing the general curriculum for students with significant cognitive disabilities, Teaching Exceptional Children, Volume 38(5), pp. 20 – 27
Clayton, K., Fleming, J.M., & Copley, J. (2003). Behavioral Responses to Tactile Stimuli in Children with Cerebral Palsy. Physical & Occupational Therapy In Pediatrics, Volume 23(1), pp. 43 - 62
Clement, T., & Bigby, C. (2009). Breaking out of a distinct social space: Reflections on supporting community participation for people with severe and profound intellectual disability. Journal of Applied Research in Intellectual Disability, Volume 22(3), pp. 264 - 275
Close, W., Carpenter, M., & Cibiri, S. (1986). An evaluation study of sensory motor therapy for profoundly retarded adults. Canadian Journal of Occupational Therapy, Volume 53(5), pp. 259 - 264
Cobb, B., Lehmann, J., Newman-Gonchar, R., & Alwell, M. (2009). Self-determination for students with disabilities: A narrative meta-synthesis. Career Development for Exceptional Individuals, Volume 32, pp. 108 – 114
Cobigo, V., Morin, D., & Lachapelle, Y. (2007). Assessing Work Task Preferences among Persons with Intellectual Disabilities: An Integrative Review of Literature. Education and Training in Developmental Disabilities, Volume 42(3), pp. 286 – 300
Codling, M., & MacDonald, N. (2009). Epilepsy: Implications for people with profound intellectual and multiple disabilities. In J. Pawlyn, & S. Carnaby (Eds.), Profound Intellectual and Multiple Disabilities Nursing Complex Needs. pp. 134 – 146. Oxford: Wiley-Blackwell,
Coffey, E. (2014). The Effect of Equine Assisted Therapy on the Social Functioning of Children with Autism. Dissertation psychology degree at Dublin Business School, School of Arts, Dublin.
Cole, C.L., & Levinson, T.R. (2002). Effects of within-activity choices on the challenging behavior of children with severe developmental disabilities. Journal of Positive Behavior Interventions, Volume 4(1), pp. 29 - 37
Coleman, M. (2002). Creating your own multisensory environment. Eye Contact, Volume 32, pp. 31 - 32
Collacott R.A., Cooper S.A., Branford D., & McGrother C. (1998). Epidemiology of self-injurious behaviour in adults with learning disabilities. British Journal of Psychiatry. Volume 173, pp. 428 – 432
Colley, A. (2013). Personalised Learning for Young People With Profound and Multiple Learning Difficulties. Jessica Kingsley
Conyers, C., Doole, A., Vause, T., Harapiak, S., Yu, C.T., & Martin, G.L. (2002). Predicting the relative efficacy of three presentation methods for assessing preferences of persons with developmental disabilities. Journal of Applied Behavior Analysis, Volume 35(1), pp. 49 – 58
Cook, J. (1996). Early sensory skills. Winslow Press
Cooke, J., & Williams, D.(1985). Working with children’s language. Winslow Press
Cooley, E.J., & Ayers, R.R. (1988). Self-concept and success-failure attributions of non-handicapped students and students with learning disabilities. Journal of Learning Disabilities, Volume 21(3), pp. 174 - 178
Coombes, K. (1986). Voice in cerebral palsied children. In - M. Fawcus (Ed.). Voice disorders and their management. Croom Helm
Cooper, S.A., Smiley, E., Jackson, A., Finlayson, J., Allan, L., Mantry, D., & Morrison, J. (2009). Adults with intellectual disabilities: prevalence, incidence and remission of aggressive behaviour and related factors. Journal of Intellectual Disability Research, Volume 53, pp. 217 - 232
Cornish, E. (2002). Gluten and casein free diets in autism: a study of the effects on food choice and nutrition. Journal of Human Nutrition and Dietetics, Volume 15(4), pp. 261 - 269
Corno, L, & Mandinach., E.B., (1983). The Role of Cognitive Engagement in Classroom Learning and Motivation, Educational Psychologist, Volume 18(2), pp. 88 - 108
Cortright, B. (2015). The Neurogenesis diet and lifestyle: Upgrade your brain, Upgrade your life. Psyche Media
Costandi, M. (2016). Neuroplasticity. MIT Press, Essential Knowledge Series
Coupe, J., Barton, L., Barber, M., Collins, L., Levy, D., & Murphy, D. (1985). Affective Communication Assessment. Manchester Education Committee
Coupe O'Kane, J., & Smith, B. (eds) (1994). Taking Control: Enabling People with Learning Difficulties. London: David Fulton.
Coupe O' Kane, J., & Goldbart, J. (1998). Communication Before Speech - Development and Assessment (2nd edition). London: David Fulton.
Courchesne, E., & Pierce, K. (2005). Why the frontal cortex in autism might be talking only to itself: local over-connectivity but long-distance disconnection. Current Opinion in Neurobiology, Volume 15(2), pp. 225 - 230
Courtemanche, A.B. (2010). Positive relationship development and the acquisition of communication and task compliance for individuals with profound intellectual developmental disabilities. Doctoral dissertation, University of Kansas
Crabbe, M. (2007). The Intensive Interaction research project… and beyond’, Royal College of Speech and Language Therapy Bulletin, August 2007, pp.12 - 13
Creber, P. (1972). Lost for words: Language and educational failure. Penguin Books
Creedon, M.P., & Baranek, G.T. (1988). Touch another way: Recognizing and managing tactile defensiveness at home and in the classroom. Proceedings of the Annual Conference of the Autism Society of America. pp. 49 – 54
Cripps, C., Tsiris, G., & Spiro, N. (Eds.). (2016). Research and resources for music therapy 2016: A compilation developed by the Nordoff Robbins research team. London: Nordoff Robbins
Croce, R., & Horvat, M. (1992). Effects of reinforcement based exercise on fitness and work productivity in adults with mental retardation. Adapted Physical Activity Quarterly, Volume 9(2), pp. 148 - 178
Crocker, A.G., Mercier, C., Lachapelle, Y., Brunet, A., Morin, D., & Roy, M.E. (2006). Prevalence and types of aggressive behaviour among adults with intellectual disabilities. Journal of Intellectual Disability, Volume 50, pp. 652 - 661
Crome, L. (1960). The brain and mental retardation. British Medical Journal, Volume 1(5177), pp. 897 - 904
Cromby, J.J., Standen, P.J., Newman, J., & Tasker, H. (1996). Successful transfer to the real world of skills practised in a virtual environment by students with severe learning difficulties. In - Proceedings 1st European Conference for Disability, Virtual Reality and Assoc. Tech., Maidenhead, UK.
Crosby, K.G., & Blatt, B. (1968). Attention and mental retardation. The Journal of Education, Volume 150(3), pp. 67 - 81
Crosby, K. (2002). Communication through music for pupils with profound and multiple learning difficulties. The SLD Experience, Volume 32. pp. 19 – 21
Csorba, J., Radvanyi, K., Regenyi, E., & Dinya, E. (2011). A study of behaviour profiles among intellectually disabled people in residential care in Hungary. Research in Developmental Disabilities, Volume 32(5), pp. 1757 – 1763
Culham, A. (2004). Getting in Touch with our Feminine Sides? Men's Difficulties and Concerns with Doing Intensive Interaction, British Journal of Special Education, Volume 31 (2), pp.81 - 88
Cullen, C. (1992). Staff training and management for intellectual disability services. International review of research in mental retardation, Volume 18, pp. 225 - 245
Cummins, R.A. (1991). Sensory Integration and Learning Disabilities: Ayres' Factor Analyses Reappraised. Journal of Learning Disabilities, Volume 24(3), pp. 160 - 168
Cunningham, C., & Glenn, S. (2004). Self-awareness in young adults with Down syndrome: I. Awareness of Down syndrome and disability. International Journal of Disability, Development and Education, Volume 51(4), pp. 335 - 361
Cunningham, R.D. (1996). Neuroimaging studies in children with developmental delay. Journal of Pediatrics. Volume 128(2), pp. 302
Cuskelly, M., & de Jong, I. (1996). Self-concept in children with Down syndrome. Down Syndrome: Research and Practice, Volume 4, pp. 59 - 64
Cuvo, A.J., May, M.M., & Post, T.M. (2001). Effects of living room, Snoezelen room, and outdoor activities on stereotypic behavior and engagement by adults with profound mental retardation. Research in Developmental Disabilities, Volume 22(3), pp. 183 - 204
Dairo, Y.M., Collett, J., Dawes, H., & Oskrochi, G.R. (2016). Physical activity levels in adults with intellectual disabilities: A systematic review. Preventive Medicine Reports, Volume 4, pp. 209 - 219
Dale, F.J. (1990). Stimulation Guide for Multi-Sensory Impaired Children. Chapman and Hall: London
Dalrymple, A.J. (1989). Sensory extinction of stereotyped object-dropping: Identification of a reinforcer for skill training. Behavioral Interventions. Volume 4(2), pp. 99 – 111
Dalton, P. (1994). Counselling people with communication problems. London: Sage Publications. ISBN 0-8039-8895-8
D’anci, K.E., Vibhakar, A., Kanter, J.H., Mahoney, C.R., & Taylor, H.A. (2009). Voluntary dehydration and cognitive performance in
trained college athletes. Perceptual and Motor Skills. Volume 109:. pp. 251 - 269
Dattilo, J., & Rusch, F.R. (1985). Effects of choice on leisure participation for persons with severe handicaps. Journal of the Association for Persons with Severe Handicaps, Volume 10(4), pp. 194 - 199
Dattilo, J. (1986). Computerized assessment of preference for severely handicapped individuals. Journal of Applied Behavior Analysis, Volume 19, pp. 445 - 448
Daveson, B., & Edwards, J. (1998). A role for music therapy in special education. International Journal of Disability, Development and Education, Volume 45(4), pp. 449 - 457
David, N., Newen, A., & Vogeley, K. (2008). The ‘‘sense of agency” and its underlying cognitive and neural mechanisms. Consciousness and Cognition. Volume 17, pp. 523 – 534
Davidson, P.W., Cain, N.N., Sloane-Reeves, J.E., Van Speybroech, A., Segel, J., Gutkin, J., Quijano, L.E., Kramer, B.M., Porter, B., & Shoham, I. (1994). Characteristics of community-based individuals with mental retardation and aggressive behavioral disorders. American Journal of Mental Retardation. Volume 98(6). pp. 704 - 716
Davidson, P.W., Houser, K.D., Cain, N.N., Sloane-Reeves, J., Quijano, L., Matons, L., Giesow, V., & Ladrigan, P.M. (1999). Characteristics of older adults with intellectual disabilities referred for crisis intervention. Journal of Intellectual Disability Research. Volume 43(1). pp. 38 - 46
Davies, C.A., & Jenkins, R. (1997). She has different fits to me: How people with learning difficulties see themselves. Disability and Society, Volume 12, pp. 95 - 109
Davies, L., & Oliver, C. (2013). Age related prevalence of aggression and self-injury in persons with an intellectual disability. Research in Developmental Disabilities, Volume 34, pp. 764 – 775
Davis, J. (2001). A Sensory Approach to the Curriculum: For Pupils with Profound and Multiple Learning Difficulties. David Fulton Publishers
Davis, P.K., Young, A., Cherry, H., Dahman,D., & Rehfeldt, R.A. (2004). Increasing the happiness of individuals with profound multiple disabilities: replication and extension, Journal of Applied Behavior Analysis, Volume 37(4), pp. 531 – 534
Davis, S., & Wehmeyer, M.L. (1991). Ten steps to independence: Promoting self-determination in the home. Arlington, TX: The Arc of the United States.
De Bildt, A., Sytema, S., Kraijer, D., Sparrow, S., & Minderaa, R. (2005). Adaptive functioning and behaviour problems in relation to level of education in children and adolescents with intellectual disability. Journal of Intellectual Disability Research, Volume 49(9), pp. 672 - 681
De Bono, E. (1985). Six Thinking Hats: An Essential Approach to Business Management. Little, Brown, & Company.
De Oliveira, M.F., Pinto, F.C.G., Nishikuni, K., Botelho, R.V., Lima, A.M., & Rotta, J.M. (2011). Revisiting hydrocephalus as a model to study brain resilience. Frontiers in human neuroscience, Volume 5, Article 181, pp. 1 - 4
De Vries, C., Yu, C.T., Sakko, G., Wirth, K.M., Walters, K.L., Carole, Marion, C. & Martin, G. (2005). Predicting the relative efficacy of verbal, pictorial, and tangible stimuli for assessing preferences of leisure activities. American Journal on Mental Retardation, Volume 110, pp. 145 – 154
De Waele, I., & Van Hove, G. (2005). Modern times: An ethnographic study on the quality of life of people with a high support need in a Flemish residential facility. Disability & Society, Volume 20(6), pp. 625 – 639
De Winter, C.F., Jansen, A.A.C., & Evenhuis, H.M. (2011). Physical Conditions and Challenging Behaviour in People with Intellectual Disability: A Systematic Review. Journal of Intellectual Disability Research. Volume 55(7), pp. 675 - 698
Dean, E.C., & Aitken, S. (1986). Functional communication in blind multiply-impaired children: a case study. Insight, Volume 4(1), pp. 7 - 11
Deb, S., Thomas, M., & Bright C. (2001). Mental disorder in adults with intellectual disability. 2: The rate of behaviour disorders among a community-based population aged between 16 and 64 years. Journal of Intellectual Disability Research, Volume 45, pp. 506 - 514
Dee, L., Byers, R., Hayhoe, H., & Maudslay, L. (2002). Enhancing Quality of Life – facilitating transitions for people with profound and complex learning difficulties: a literature review. London: Skill/Cambridge: University of Cambridge.
DeLeon, I.G., & Iwata, B.A. (1996). Evaluation of a multiple-stimulus presentation format for assessing reinforcer preferences. Journal of Applied Behavior Analysis, Volume 29, pp. 519 - 533
Delfour, F., & Marten, K. (2001). Mirror image processing in three marine mammal species: killer whales (Orcinus orca), false killer whales (Pseudorca crassidens) and California sea lions (Zalophus californianus), Behavioral Processes, Volume 53(3), pp. 181 - 190
deLissovoy, V. (1963). Head banging in early childhood: A suggested cause. Journal of Genetic Psychology, Volume 102, pp. 109 - 114
DeLong, G.R., & Heinz, E.R. (1997). The clinical syndrome of early-life bilateral hippocampal sclerosis. Annals of Neurology. Volume 42. pp. 11 – 17
Deng, W., Aimone, J.B., & Gage, F.H. (2010). New neurons and new memories: how does adult hippocampal neurogenesis affect learning and memory? Nature Reviews Neuroscience, Volume 11(5), pp. 339 - 350
Dennis, R. (2002). Nonverbal narratives: Listening to people with severe intellectual disability. Research and Practice for Persons with Severe Disabilities, Volume 27(4), pp. 239 - 249
Densem, J. F., Nuthall, G. A., Bushnell, J., & Horn, J. (1989). Effectiveness of a sensory integrative therapy program for children with perceptual-motor deficits. Journal of Learning Disabilities, Volume 22, pp. 221 - 229
Denton, D.M. (1970). Remarks in support of total communication. Communication symposium. Maryland school for the deaf. Frederick, MD.
Diamond, M.C., Krech, D., & Rosenzweig, M.R. (1964). The Effects of an Enriched Environment on the Histology of the Rat Cerebral Cortex. Journal of Comparative Neurology and Psychology. Volume 123. pp. 111 - 120
Diamond, M.C., Law, F., Rhodes, H., Lindner, B., Rosenzweig, M.R., Krech, D., & Bennett, E. (1966). Increases in cortical depth and glia numbers in rats subjected to enriched environment. Journal of Comparative Neurology. Volume 128 (1). pp. 117 – 125
Diamond, M.C., Rosenzweig, M.R., Bennett, E.L., Lindner, B., & Lyon, L. (1972). Effects of environmental enrichment and impoverishment on rat cerebral cortex. Journal of Neurobiology, Volume 3(1). pp. 47 - 64
Dickerson, L. (1995). Techniques for the integration of people who use alternative communication devices in the workplace. 3rd Annual Pittsburgh Employment Conference Proceedings. pp. 27 - 34. Pittsburgh: Shout Press
Didden, R., Korzilius, H., van Aperlo, B., van overloop, C., & de Vries, M. (2002). Sleep problems and daytime problem behaviours in children with intellectual disability. Journal of Intellectual Disability Research. Volume 46, pp. 537 – 547
Diego, M.A., Jones, N.A., Field, T., Hernandez-Reif, M., Schanberg, S., Kuhn, C., Galamaga, M., McAdam, V., & Galamaga, R. (1998). Aromatherapy positively affects mood, EEG patterns of alertness and math computations. International Journal of Neuroscience, Volume 96(3-4), pp. 217 - 224
Dieringer, S.T., Gumm, E., & Porretta, D. (2013). Using music therapy principles to enhance physical activity participation in children and adolescents with disabilities. PALAESTRA: Forum of Sport, Physical Education, and Recreation for Those with Disabilities, Volume 27(3), pp. 42 - 46
Dimaggio, G., Lysaker, P.H., Carcione, A., Nicolo, G., & Semerari, A. (2008). Know yourself and you shall know the other...to a certain extent: multiple paths of influence of self-reflection on mind reading, Consciousness and Cognition, Volume 17, pp. 778 – 789
Diorio, M.S., & Konarski, E.A. (1984). Evaluation of a method for teaching dressing skills to profoundly mentally retarded persons. American Journal of Mental Deficiency. Volume 89(3), pp. 307 - 309
Dixon-Ibarra, A., Lee, M., & Dugala, A. (2013). Physical activity and sedentary behavior in older adults with intellectual disabilities: a comparative study. Adapted Physical Activity Quarterly, Volume 30(1), pp. 1 - 19
Dobson, S., Dodsworth, S., & Miller, M. (2000). Problem solving in small multidisciplinary teams: a means of improving the quality of the communication environment for people with profound learning disability. British Journal of Learning Disability, Volume 28(1), pp. 25 - 30
Dobson, S., Upadhyaya, S., & Stanley, B. (2002). Using an interdisciplinary approach to training to develop the quality of communication with adults with profound learning disabilities by care staff. International Journal of Language & Communication Disorders, Volume 37(1), pp. 41 – 57
Doidge, N. (2007). The brain that changes itself: Stories of personal triumph from the frontiers of brain science. Penguin
Došen, A. (2007). Integrative treatment in persons with intellectual disability and mental health problems. Journal of Intellectual Disability Research, Volume 51(1), pp. 66 – 74
Dosman, C., Adams, D., Wudel, B., Vogels, L., Turner, J., & Vohra, S. (2013). Complementary, holistic, and integrative medicine: autism spectrum disorder and gluten-and casein-free diet. Pediatrics in Review:American Academy of Pediatrics, Volume 34(10), e36 - 41
Dote-Kwan, J., & Chen. D. (1999). Developing meaningful interventions. In D. Chen (Ed.), Essential elements in early communication visual impairments and multiple disabilities (pp. 287-336). New York: American Foundation for the Blind Press
Dowey, A., Toogood, S., Hastings, R.P., & Nash, S. (2007). Can brief workshop interventions change care staff understanding of challenging behaviours? Journal of Applied Research in Intellectual Disabilities, Volume 20(1), pp. 52 – 55
Dowling, J. (2011): Therapeutic storytelling, PMLD Link, Volume 23 (3), Issue 70. pp. 28 - 29
Dowling, S., Hassan, D., McConkey, R., & Breslin, G. (2012). Examining the relationship between physical activity and the health and wellbeing of people with intellectual disabilities: A literature review. Special Olympics Ireland and the University of Ulster
Downing, J.E. (Ed.) (2002). Including students with severe and multiple disabilities in typical classrooms: Practical strategies for
teachers (2nd ed.). Baltimore: Paul H. Brookes.
Downing, J.E., & Chen, D. (2003). Using tactile strategies with students who are blind and have severe disabilities. Teaching Exceptional Children, Volume 36(2), pp. 56 - 61
Downs, C., Morgan, M., Ouvry, C. & Porter, J. (2001). Interpreting the communication of people with profound and multiple learning
difficulties. British Journal of Learning Disabilities, Volume 29, pp. 12 - 16
Draganski, B., Gaser, C., Busch, V., Schuierer, G., Bogdahn, U., & May, A. (2004). Neuroplasticity: changes in grey matter induced by training. Nature, Volume 427(6972). pp.311 - 312
Draheim, C.C., Williams, D.P., & McCubbin, J.A. (2002). Prevalence of physical inactivity and recommended physical activity in community-based adults with mental retardation. Mental Retardation, Volume 40(6), pp. 436 – 444
Dubois, A., Capdevila, X., Bringuier, S., & Pry, R. (2010). Pain expression in children with intellectual disability. European Journal of Pain. Volume 14, pp. 654 – 660
Duggan, D. (1978). Goals and methods in dance therapy with severely multiply-handicapped children. American Journal of Dance Therapy. Volume 2(1), pp. 31 - 34
Duggan, D. (1995). The 4’s: A Dance Therapy Program for Learning-Disabled Adolescents, in Levy, F. J. (ed.), Dance and Other Expressive Arts Therapies: When Words are not enough, London: Routledge
Duggan, D., Stratton-Gonzalez, S., & Gallant, C. (2009). Dance Education for Diverse Learners: A Special Education Supplement to the Blueprint for Teaching and Learning in Dance. NYC Department of Education
Duker, P.C., & Jutten, W. (1997). Establishing gestural yes-no responding with individuals with profound mental retardation. Education and Training in Developmental Disabilities, Volume 32(1), pp. 62 - 75
Dunbar, R. (1996). Grooming, gossip and the evolution of language. Faber and Faber. ISBN 0-571-17396-9
Duncan, D., Matson, J.L., Bamburg, J.W., Cherry, K.E., & Buckley, T. (1999). The relationship of self-injurious behavior and aggression to social skills in persons with severe and profund learning disability. Research in Developmental Disabilities, Volume 20, pp. 441 - 448
Dunlap, G., Kern-Dunlap, L., Clarke, S., & Robbins, F.R. (1991). Functional assessment, curricular revision, and severe behavior problems. Journal of Applied Behavior Analysis, Volume 24, pp. 387 - 397
Dunn, W. (2001). The sensations of everyday life: Empirical, theoretical, and pragmatic considerations. American Journal of Occupational
Therapy, Volume 55, pp. 608 - 620.
Durand, V.M., & Kishi, G. (1987). Reducing severe behavior problems among persons with dual sensory impairments: An evaluation of a technical assistance model. Journal of the Association for Persons with Severe Handicaps, Volume 12, pp. 2 - 10
Durand, V.M., & Crimmins, D.B. (1988). Identifying the variables maintaining self-injurious behaviour. Journal of Autism and Developmental Disorders, Volume 18, 99 - 117
Durand, V.M., & Crimmins, D.B. (1991). Teaching functionally equivalent responses as an intervention for challenging behaviour, in B. Remington (Ed.), The Challenge of Severe Mental Handicap: a behaviour analytic approach. London: Wiley.
Dutt, A.S.K. (2010). The effects of skill training on preference for individuals with severe to profound multiple disabilities. PhD (Doctor of Philosophy) thesis, University of Iowa
Duval, S., & Wicklund, R.A. (1972). A Theory of Objective Self Awareness. New York: Academic Press.
Dyer, K., Schwartz, I.S., & Luce, S.C. (1984). A supervision program for increasing functional activities for severely handicapped students in a residential setting. Journal of Applied Behavior Analysis, Volume 17(2), pp. 249 - 259
Dyer, K., Dunlap, G., & Winterling, V. (1990). Effects of choice making on the serious problem behaviors of students with severe handicaps. Journal of Applied Behavior Analysis, Volume 23(4), pp. 515 - 524
Dykens, E.M., Rosner, B.A., Ly, T., & Sagun, J. (2005). Music and anxiety in Williams syndrome: A harmonious or discordant relationship? American Journal on Mental Retardation, Volume 110(5), pp. 346 - 358
Edmonds, C.J., & Burford, D. (2009) Should children drink more water?: the effects of drinking water on cognition in children. Appetite. Volume 52. pp. 776 - 779
Edmonds, C.J., & Jeffes, B. (2009). Does having a drink help you think? 6-7-Year-old children show improvements in cognitive performance from baseline to test after having a drink of water. Appetite. Volume 53. pp. 469 - 472
Edmonds, C.J., Crombie, R., & Gardner, M.R. (2013). Subjective thirst moderates changes in speed of responding associated
with water consumption. Frontiers in Human Neuroscience. Volume 7. Article 363
Edmonds, C.J., Crombie, R., Ballieux, H., Gardner, M.R., & Dawkins, L. (2013). Water consumption, not expectancies about water consumption, affects cognitive performance in adults. Appetite. Volume 60. pp. 148 - 153
Ehrsson, H.H. (2007). The experimental induction of out-of-body experiences. Science, Volume 317, pp. 1048 – 1048
Eiland, L., & Romeo R.D. (2013). Stress and the developing adolescent brain. Neuroscience, Volume 249. pp. 162 – 171
Einarsson, I.O., Ólafsson, Á., Hinriksdóttir, G., Jóhannsson, E., Daly, D., & Arngrímsson, S.A. (2015). Differences in physical activity among youth with and without intellectual disability. Medicine and Science in Sports and Exercise, Volume 47(2), pp. 411 - 418
Elbaum, B., & Vaughn, S. (2001). School-Based Interventions to Enhance the Self Concept of Students with Learning Disabilities: A Meta-Analysis. The Elementary School Journal, Volume 101(3), Special Issue: Instructional Interventions for Students with Learning Disabilities, pp. 303 - 329
Elder, J.H., Shankar, M., Shuster, J., Theriaque, D., Burns, S., & Sherrill, L. (2006). The gluten-free, casein-free diet in autism: results of a preliminary double blind clinical trial. Journal of autism and developmental disorders, Volume 36(3), pp. 413 - 420
Elder, J.H. (2008). The gluten-free, casein-free diet in autism: an overview with clinical implications. Nutrition in Clinical Practice, Volume 23(6), pp. 583 - 588
Elder, J.H., Kreider, C.M., Schaefer, N.M., & de Laosa, M.B. (2015). A review of gluten-and casein-free diets for treatment of autism: 2005–2015. Nutrition and Dietary Supplements, Volume 7, pp. 87 - 101
Elgie, S. & Maguire, N. (2001). Intensive Interaction with a woman with multiple and profound disabilities: a case study’, Tizard Learning Disability Review, Volume 6(3), pp.18 - 24
Elgie, S., & Hastings, R.P. (2002). Staff definitions of challenging behavior. Education and Training in Mental Retardation and Developmental Disabilities, Volume 37(2), pp. 202 – 208
Ellingford, J., James, I., Mackenzie, L., & Marsland, L. (2007): Using dolls to alter behaviour in patients with dementia. Nursing Times, Volume 103 (38). pp.36 - 37
Ellis, D. (Ed.)(1986). Sensory impairments in mentally handicapped people. Taylor & Francis.
Emerson, E., Barrett, S., Bell, C., Cummings, R., Hughes, H., McCool, C., Toogood, A., & Mansell, J. (1987). The Special Development Team: Developing Services for People with Severe Learning Difficulties and Challenging Behaviours. University of Kent at Canterbury
Emerson, E., Toogood, A., Mansell, J., Barrett, S., Bell, C., Cummings, R., & McCool, C. (1987). Challenging behaviour and community services: 1 Introduction and Overview, Mental Handicap, Volume 15, pp. 166 - 169
Emerson, E., Cummings, R., Barrett, S., Hughes, H., & McCool, C., & Toogood, A. (1988). Challenging Behaviour and community services: 2. Who are the people who challenge services? Mental Handicap, Volume 16, pp. 16 - 19
Emerson, E., Cummings, R., Hughes, H., Toogood, A., McCool, C., & Barrett, S. (1989). Challenging behaviour and community services. 6. Evaluation and overview. Mental Handicap, Volume 17, pp. 104 - 108
Emerson, E., & McGill, P. (1989). Normalisation and applied behaviour analysis: Values and technology in services for people with learning difficulties. Behavioural Psychotherapy, Volume 17, pp. 101 - 117
Emerson, E. (1990). Designing individualised community-based placements as an alternative to institutions for people with severe mental handicap and severe problem behaviour, in W.I. Fraser (Ed.), Key Issues in Mental Retardation Research. Routledge, London, pp. 395 - 404.
Emerson, E. (1992). Self-injurious behaviour: an overview of recent developments in epidemiological and behavioural research. Mental handicap Research. Volume 4, pp. 49 - 81
Emerson, E., Beasley, F., Offord, G., & Mansell, J. (1992) Specialised housing for people with seriously challenging behaviours. Journal of Mental Deficiency Research, Volume 36, pp. 291 - 307
Emerson, E., & McGill, P. (1993). Developing services for people with severe learning disabilities and seriously challenging behaviours: South East Thames Regional Health Authority, 1985-1991. In I. Fleming & B. Stenfert Kroese (Eds.), People with Severe Learning Difficulties who also Display Challenging Behaviour. Manchester: Manchester University Press
Emerson, E., McGill, P. and Mansell, J. (Eds.)(1994). Severe Learning Disabilities and Challenging Behaviours. London: Chapman and Hall.
Emerson, E. (1995). Challenging Behaviour: Analysis and Intervention in People with Learning Disabilities. Cambridge: Cambridge University Press.
Emerson, E., Cullen, C., Hatton, C. & Cross, B. (1996). Residential Provision for People with Learning Disabilities: Summary Report. Manchester: Hester Adrian Research Centre, Manchester University.
Emerson, E., Forrest, J., Cambridge, P., & Mansell, J. (1996). Community support teams for people with learning disabilities and challenging behaviours: results of a national survey. Journal of Mental Health, 5(4), pp. 395 - 406
Emerson, E., Alborz, A., Kiernan, C., Mason, H., Reeves, D., Swarbrick, R., & Mason, L. (1997). The Treatment & Management of Challenging Behaviour: HARC Challenging Behaviour Project Report 5. Manchester: Hester Adrian Research Centre.
Emerson, E., Robertson, J., Gregory, N., Hatton, C., Kessissoglou, S., Hallam, A., & Hillery, J. (2000). Treatment and Management of Challenging Behaviours in Residential Settings. Journal of Applied Research in Intellectual Disabilities, Volume 13(4), pp. 197 - 215
Emerson, E., Robertson, J., Gregory, N., Hatton, C., Kessissoglou, S., Hallam, A., Knapp, M., Jarbrink, K., Walsh, P.N., & Netten, A. (2000). The quality and costs of community-based residential supports, village communities and residential campuses in the United Kingdom. American Journal of Mental Retardation, Volume 105(2), pp. 81 - 102
Emerson, E., Robertson, J., Gregory, N., Kessissoglou, S., Hatton, C., Hallam, A., Knapp, M., Jarbrink, K., Netten, A. & Linehan, C. (2000). The quality and costs of community-based residential supports and residential campuses for people with severe and complex disabilities. Journal of Intellectual and Developmental Disability, Volume 25(4), pp. 263 - 279
Emerson, E. (2001). Challenging Behaviour: Analysis and Intervention in People with Severe Intellectual Disabilites. Second Edition. Cambridge University Press
Emerson, E., Kiernan, C., Alborz, A., Reeves, D., Mason, H., Swarbrick, R., Mason, L., & Hatton, C. (2001). The prevalence of challenging behaviors: a total population study. Research In Developmental Disabilities. Volume 22(1). pp. 77 - 93
Emerson, E. (2005). Underweight, obesity and exercise among adults with intellectual disabilities in supported accommodation in Northern England. Journal of Intellectual Disability Research, Volume 49(2), pp. 134 – 143
Emerson, E., & Baines, S. (2011). Health inequalities and people with learning disabilities in the UK. Tizard Learning Disability Review, Volume 16(1), pp. 42 - 48
Emerson, E., & Einfeld, S. (2011). Challenging Behaviour. Cambridge: Cambridge University Press
Erikson, E.H. (1950). Childhood and society. WW Norton & Company
European Food Safety Authority (2011). Scientific Opinion on the substantiation of health claims related to water and maintenance of normal physical and cognitive functions, maintenance of normal thermoregulation and basic requirement of all living things. Download http://www.efsa.europa.eu/en/efsajournal/pub/2075.htm
Evans, L. (1982). Total Communication: Structure and Strategy. Washington, DC: Galludet College Press
Evenhuis, H.M., & Nagtzaam, L.M.D. (1999). Onderzoeksprogramma chronisch zieken. Wetenschap en geneeskunde voor mensen met een verstandelijke handicap: Een nieuw ontgonnen gebied in de Nederlandse gezondheidszorg. Den Haag: NOW-MW
Evenhuis, H.M., Theunissen, M., Denkers, I., Verschuure, H., & Kemme, H. (2001). Prevalence of visual and hearing impairment in a Dutch institutionalized population with intellectual disability. Journal of Intellectual Disability Research, Volume 45(5), pp. 457 - 464
Eyman, R.K., & Call, T. (1977). Maladaptive behavior and community placement of mentally retarded persons. American Journal of Mental Deficiency, Volume 82, pp. 137 -144
Fadda, R., Rapinett, G., Grathwohl, D., Parisi, M., Fanari, R., Calo, C.M., & Schmitt, J. (2012). Effects of drinking supplementary water
at school on cognitive performance in children. Appetite. Volume 59. pp. 730 - 737
Fahey, A., & Carr, A. (2002). Prevention of adjustment difficulties in children with sensory impairments. In: A. Carr (ed.) Prevention: What works with Children and Adolescents? A Critical Review of Psychological Prevention Programmes for Children, Adolescents and their Families. East Sussex: Brunner-Routledge.
Farlow, L.J., & Snell, M.E. (2003). Teaching Basic Self-Care Skills. In - M. Snell & F. Brown (Eds.), Instruction of Students with Severe Disabilities. pp. 331 - 377. Ohio: Merill Prentice Hall, Colombus.
Farrell, M. (2006). The Effective Teacher's Guide to Moderate, Severe and Profound Learning Difficulties: Practical Strategies. Taylor & Francis
Farrell, P. (1991). Behavioural and interactive teaching for children with severe learning difficulties: Match or mismatch? Educational and Child Psychology, Volume 8(2), pp. 61 - 68
Farrell, P. (1997). Teaching Pupils with Learning Difficulties: Strategies and Solutions. London: Cassell.
Farrer, C., & Frith, C.D. (2002). Experiencing oneself vs another person as being the cause of an action: the neural correlates of the experience of agency, Neuroimage, Volume 15(3), pp. 596 – 603
Favell, J.E., & Cannon, P.R. (1976). Evaluation of entertainment materials for severely retarded persons. American Journal of Mental Deficiency, Volume 81, pp. 357 – 361
Favell, J.E., McGimsey, J.F., & Schell, R.M. (1982). Treatment of self-injury by providing alternate sensory activities. Analysis and Intervention in Developmental Disabilities, Volume 2, pp. 83 - 104
Favell, J.E., Realon, R.E., & Sutton, K.A. (1996). Measuring and increasing the happiness of people with profound mental retardation and physical handicaps. Behavioral Interventions, Volume 11(1), pp. 47 - 58
Felce, D., de Kock, U., & Repp, A.C. (1986). An eco-behavioural comparison of small community-based houses and traditional large hospitals for severely and profoundly mentally handicapped adults. Applied Research in Mental Retardation, Volume 7, pp. 393 - 408.
Felce, D., Saxby, H., de Kock, U., Repp, A., Ager, A., & Blunden, R. (1987). To what behaviors do attending adults respond?: A replication. American Journal of Mental Deficiency, Volume 91, pp.496 - 504
Felce, D., & Repp, A. (1992). The behavioral and social ecology of community houses. Research in Developmental Disabilities, Volume 13, pp. 27 - 42
Felce, D., Bowley, C., Baxter, H., Jones, E., Lowe, K., & Emerson, E. (2000). The effectiveness of staff support: evaluating active support training using a conditional probability approach. Research in Developmental Disabilities, Volume 21(4), pp. 243 - 255
Felce, D., Lowe, K., Beecham, J., & Hallam, A. (2000). Exploring the relationships between costs and quality of services for adults with severe intellectual disabilities and the most severe challenging behaviours in Wales: A multivariate regression analysis. Journal of Intellectual and Developmental Disability, Volume 25(4), pp. 307 - 326
Felce, D., Jones, E., & Lowe, K. (2002). Active support: planning daily activities and support for people with severe mental retardation. In S. Holburn & P.M. Vietze (Eds.), Person centered planning. Research, practice and future directions (pp.247-269). Baltimore: P.H.Brookes
Fernandez-Jaen, A. (2006). Attention deficit hyperactivity disorder and mental retardation. Revista de Neurologia, Volume 42, Supplement 2, 25 - 27
FEU/Mencap (1994). Learning for Life. FEU/Mencap; London.
Feuerstein, R., Feuerstein, R.S., Falik, L.H., & Rand, Y. (2006). Creating and Enhancing Cognitive Modifiability: The Feuerstein Instrumental Enrichment Program. Jerusalem, Israel: ICELP Press
Feuerstein, R., Feuerstein, R.S., & Falik, L.H. (2010). Beyond Smarter: Mediated Learning and the Brain’s Capacity to Change. New York: Teacher’s College Press
Feuillet, L., Dufour, H., & Pelletier, J. (2007). Brain of a white-collar worker. The Lancet, Volume 370(9583), pp. 262
Field, S. (1996). Self-determination instructional strategies for youth with learning disabilities. Journal of Learning Disabilities, Volume 29, pp. 40 – 52
Field, S., Martin, J.E., Miller, R.J., Ward, M.J., & Wehmeyer, M.L. (1998). A practical guide for teaching self-determination. Reston, VA: Council for Exceptional Children.
Field, S., Sarver, M.D., & Shaw, S.F. (2003). Self-determination: A key to success in post secondary education for students with learning disabilities. Remedial and Special Education, Volume 24, pp. 339 – 349.
Filipek, P.A. (1999). Neuroimaging in the developmental disorders: the state of the science. The Journal of Child Psychology and Psychiatry and allied disciplines. Volume 40(1), pp. 113 – 128
Filippi, C.G., Uluğ, A.M., Deck, M.D., Zimmerman, R.D., & Heier, L.A. (2002). Developmental delay in children: assessment with proton MR spectroscopy. American Journal of Neuroradiology, Volume 23(5), pp. 882 - 888
Fine, A. (Ed) (2010). Handbook on Animal Assisted Therapy: Theoretical Foundations and Guidelines for Practice (3rd ed). Elsevier, London
Finlay, W.M.L., & Lyons, E. (1998). Social identity and people with learning difficulties: Implications for self-advocacy groups. Disability and Society, Volume 13, pp. 37 - 51
Finlay, W.M.L., & Lyons, E. (2000). Social categorisations, social comparisons and stigma:Presentations of self in people with learning difficulties. British Journal of Social Psychology, Volume 39, pp. 129 - 146
Finlay, W.M.L., Antaki, C., Walton, C., & Stribling, P. (2008). The dilemma for staff in "playing a game" with a person with profound intellectual disabilities: empowerment, inclusion and competence in interactional practice. Sociology of Health & Illness, Volume 30(4), pp. 531 - 549
Finlayson, J., Jackson, A., Cooper, S.A., Morrison, J., Melville, C., Smiley, E., Allan, L., & Mantry, D. (2009). Understanding predictors of low physical activity in adults with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 22(3), pp. 236 - 247
Firth, G. (2006). Intensive Interaction – a Research Review’, Mental Health and Learning Disabilities Research and Practice, Volume 3(1), pp. 53 - 58
Firth, G. (2008). A Dual Aspect Process Model of Intensive Interaction, British Journal of Learning Disabilities, Volume 37, pp. 43 – 49
Firth, G., Elford, H., Leeming, C., & Crabbe, M. (2008). Intensive Interaction as a Novel Approach in Social Care: Care Staff’s Views on the Practice Change Process, Journal of Applied Research in Intellectual Disabilities, Volume 21, pp. 58 - 69
Fisch, L. (1969). Hearing loss and cerebral palsy. In - Blencowe, S. (Ed.). Cerebral palsy and the young child. Livingstone
Fisher, A.F., & Dunn, W.D. (1983). Tactile Defensiveness: Historical Perspectives, new Research – A Theory Grows. Sensory Integration Special Interest Section Newsletter, Volume 6(2), pp. 1 - 2
Fisher, D., & Frey, N. (2014). Checking For Understanding: Formative Assessment Techniques for your Classroom. ASCD
Fisher, A.V., Godwin, K.E., & Seltman, H. (2014). Visual environment, attention allocation, and learning in young children: When too much of a good thing may be bad. Psychological Science, Volume 25(7), pp. 1362 - 1370
Fisher, W.W., Piazza, C.C., Bowman, L.G., Hagopian, L.P., Owens, J.C., & Slevin, I. (1992). A comparison of two approaches for identifying reinforcers for persons with severe and profound disabilities. Journal of Applied Behavior Analysis, Volume 25, pp. 491 – 498
Fisher, W.W., Piazza, C.C., Bowman, L.G., & Amari, A. (1996). Integrating caregiver report with a systematic choice assessment to enhance reinforcer identification. American Journal on Mental Retardation, Volume 101, pp. 15 - 25
Fisher, W.W., Thompson, R.H., Piazza, C.C., Crosland, K., & Gotjen, D. (1997). On the relative reinforcing effects of choice and differential consequence. Journal of Applied Behavior Analysis, Volume 30, pp. 423 - 438
Flaherty, A.W. (2003). Writing like crazy: a word on the brain. Chronicle of Higher Education, Volume 50(13), pp. 1 - 6
Flaherty, A.W. (2004). The Midnight Disease. Press Release. Houghton Mifflin Company
Flaherty, A.W. (2015). The midnight disease: The drive to write, writer's block, and the creative brain. Houghton Mifflin Harcourt.
Flora, S.R., & Polenick, C.A. (2013). Effects of Sugar Consumption on Human Behavior and Performance. The Psychological Record, Volume 63, pp. 1 – 12
Fodstad, J., & Matson, J. (2008). A comparison of feeding and mealtime problems in adults with intellectual disabilities with and without autism. Journal of Developmental and Physical Disabilities, Volume 20(6), pp. 541 - 550
Foote, A.L., & Crystal, J.D. (2007). Metacognition in the Rat. Current Biology. Volume 17(6), pp. 551 – 555
Foreman, P., & Arthur, M. (2002). Parental perspectives on educational programmes for students with high support needs. European Journal of Special Needs Education, Volume 17, pp. 175 – 184
Foreman, P., Arthur-Kelly, M., Pascoe, S., & Smyth King, B. (2004). Evaluating the Educational Experiences of Students with Profound and Multiple Disabilities in Inclusive and Segregated Classroom Settings: An Australian Perspective. Research and Practice for Persons with Severe Disabilities, Volume 29(3), pp. 183 - 193
Foreman, P., Arthur‐Kelly, M., Bennett, D., Neilands, J., & Colyvas, K. (2014). Observed changes in the alertness and communicative involvement of students with multiple and severe disability following in‐class mentor modelling for staff in segregated and general education classrooms. Journal of Intellectual Disability Research, Volume 58(8), pp. 704 - 720
Forster, S., & Iacono, T. (2008). Disability support workers’ experience of interaction with a person with profound intellectual disability. Journal of Intellectual and Developmental Disability, Volume 33(2), pp. 137 - 147
Forster, S. (2010). Age-appropriateness: Enabler or barrier to a good life for people with profound intellectual and multiple disabilities? Journal of Intellectual & Developmental Disability, Volume 35(2): pp. 129 – 131
Forster, S. (2011). An ethical dilemma of too much listening and responding. PMLD Link, Volume 23(1). pp. 5 - 6
Forster, S., Gray, K.M., Taffe, J., Einfeld, S.L., & Tonge, B.J. (2011). Behavioural and emotional problems in people with severe and profound intellectual disability, Journal of Intellectual Disability Research, Volume 55(2), pp. 190 – 198
Fowler, C.H., Konrad, M., Walker, A.R., Test, D.W., & Wood, W.M. (2007). Self-determination interventions’ effects on the academic performance of students with developmental disabilities. Education and Training in Developmental Disabilities, Volume 42, pp. 270 – 285
Fowler, S. (2007). Sensory Stimulation. Jessica Kingsley Publishers
Fowler, S. (2008). Multisensory Rooms and Environments: Controlled Sensory Experiences for People with Profound and Multiple Disabilities: A Guide to Controlled Sensory Experiences. Jessica Kingsley Publishers
Fox, R.A., & Rotatori, A.F. (1982). Prevalence of obesity among mentally retarded adults. American Journal of Mental Deficiency. Volume 87(2), pp. 228 - 230
Fox, R.A., & Wade, E. (1998). Attention deficit hyperactivity disorder among adults with severe and profound mental retardation. Research in Developmental Disabilities, Volume 19(3), pp. 275 - 280
Foxall, E.L. (2002). The use of horses as a means of improving communication abilities of those with autism spectrum disorders: an investigation into the use and effectiveness of the horse as a therapy tool for improving communication in those with autism. Unpublished
manuscript. Coventry, UK: Coventry University.
Fragala, M.S., Beyer, K.S., Jajtner, A.R., Townsend, J.R., Pruna, G.J., Boone, C.H., Bohner, J.D., Fukuda, D.H., Stout, J.R., & Hoffman, J.R. (2014). Resistance exercise may improve spatial awareness and visual reaction in older adults. The Journal of Strength & Conditioning Research, Volume 28(8), pp.2079 - 2087
Fragkouli, A. (2013). Music therapy in special schools: The assessment of the quality of relationship. Approaches: Music Therapy & Special Music Education, Volume 5(2), pp. 152 - 165. Retrieved from: http://approaches.gr/musictherapy-in-special-schools-the-assessment-of-the-quality-of-relationship-aspasia-fragkouli/.
Francis, D., Diorio, J., Plotsky, P.M., & Meaney, M.J. (2002). Environmental enrichment reverses the effects of maternal separation on stress reactivity. Journal of Neuroscience, Volume 22(18), pp. 7840 - 7843
Fraser, W.I., Leudar, I., Gray, J., & Campbell, I. (1986) Psychiatric and behaviour disturbance in mental handicap. Journal of Mental Deficiency Research, Volume 30, pp. 49 - 57
Frey, G.C. (2004). Comparison of physical activity levels between adults with and without mental retardation. Journal of Physical Activity and Health, Volume 1(3), pp. 235 - 245
Frey G.C., Buchanan A.M., & Rosser Sandt D.D. (2005). ‘‘I’d Rather Watch TV’’ an examination of physical activity in adults with mental retardation. Mental Retardation. Volume 43, pp. 241 - 254
Frey G.C., Stanish H., & Temple V.A. (2008). Physical activity of youth with intellectual disability. Review and research agenda. Adapted Physical Activity Quarterly. Volume 25, pp. 95 – 117
Frymier, A.B., & Mongeau, P.A. (1997). Communicating with Touch in the Teacher/Student Relationship. Paper presented at the Annual Meeting of the Eastern Communication Association (Baltimore, MD, April 10-13)
Fuglestad, A.J., Rao, R., & Georgieff, M.K. (2008). The Role of Nutrition in Cognitive Development . In - C. Nelson & M. Collin (Eds), Handbook of Developmental Cognitive Neuroscience. pp. 623 - 641. MIT Press; 2nd revised edition
Fulton, K., Woodley, K. & Sanderson, H. (2008). Supported Decision Making: A guide for supporters, Paradigm
Furniss, F., & Biswas, A.B. (2012). Recent research on aetiology, development and phenomenology of self-injurious behaviour in people with intellectual disabilities: a systematic review and implications for treatment. Journal of Intellectual Disability Research, Volume 56(5), pp. 453 - 475
Fyson, R., & Cromby, J. (2010). Memory, sexual abuse and the politics of learning disability. In - Haaken, J. & Reavey, P., Memory Matters: contexts for understanding sexual abuse recollections, (pp. 157 - 174) Hove, Routledge
Fyson, R., & Cromby, J. (2013). Human rights and intellectual disabilities in an era of ‘choice’. Journal of Intellectual Disability Research, Volume 57(12), pp. 1164 - 1172
Gabrielli, O., Salvolini, U., Bonifazi, V., Ciferri, L., Lanza, R., Rossi, R., Coppa, G.V., & Giorgi, P.L. (1993). Morphological studies of the corpus callosum by MRI in children with malformative syndromes. Neuroradiology, Volume 35(2), pp. 109 - 112
Gabrielli, O., Coppa, G.V., Manzoni, M., Carloni, I., Kantar, A., Maricotti, M., & Salvolini, U. (1998). Minor cerebral alterations observed by magnetic resonance imaging in syndromic children with mental retardation. European Journal of Radiology, Volume 27(2), pp. 139 - 144
Gabrielli, O., Bruni, S., Coppa, G.V., Carloni, I., Polonara, G., Regnicolo, L., Salvolini, S., & Salvolini, U. (2002). White-matter alterations and callosal abnormalities in syndromic patients with mental retardation. Journal of Child Neurology, Volume 17(3), pp.164 - 168
Gaddes, W.H. (1985). Learning Disabilities and Brain Function: A Neuropsychological Approach. Second Edition. New York: Springer Science and Business Media
Gal, E., Dyck, M., & Passmore, A. (2009). The relationship between stereotyped movements and self-injurious behavior in children with developmental or sensory disabilities. Research in Developmental Disabilities, Volume 30(2), pp. 342 – 352
Gallagher, S. (2000). Philosophical conceptions of the self: Implications for cognitive science. Trends in Cognitive Sciences, Volume 4(1), pp. 14 – 21
Gallup, G.G., Jr. (1970). Chimpanzees: self-recognition. Science, Volume 167: pp. 86 - 87
Gallup, G.G., Jr., McClure, M.K., Hill, S.D., and Bundy, R.A. (1971). Capacity for self-recognition in differentially reared chimpanzees. Psychological Record, Volume 21: pp. 69 - 74
Gallup, G.G., Jr. (1979). Self-recognition in chimpanzees and man: A developmental and comparative perspective. New York: Plenum Press.
Gallup, G.G., Jr. (1982). Self-awareness and the emergence of mind in primates. American Journal of Primatology, Volume 2, pp. 237 - 248
Gallup, G.G. Jr. (1985). Do minds exist in species other than our own? Neuroscience and Biobehavioral Reviews, Volume 9, pp. 631 - 641
Gallup, G.G., Jr., and Suarez, S.D. (1986). Self-awareness and the emergence of mind in humans and other primates. In - J. Suls and A. Greenwald (eds.), Psychological Perspectives on the Self (Vol. 3), pp. 3-26. Hillsdale, N.J.: Erlbaum.
Gallup, G.G., Jr. (1987). Self-awareness. In J.R. Mitchell (ed.) Comparative Primate Biology, Behavior, Cognition, and Motivation, Volume 2B, pp. 3 - 16. New York: Liss.
Gallup, G.G., Jr. (1994). Self-recognition: research strategies and experimental design. In S.T. Parker, R.W. Mitchell & M.L. Boccia (Eds.),
Self-awareness in animals and humans: developmental perspectives, pp. 35-50. New York: Cambridge University Press.
Gallup, G.G., Jr., Povinelli, D.J., Suarez, S.D., Anderson, J.R., Lethmate, J., and Menzel, E. (1995). Further reflections on self-recognition in primates. Animal Behaviour, Volume 50: pp. 1525 - 1532
Ganio, M.S., Armstrong, L.E., Casa, D.J., McDermott, B.P., Lee, E.C., Yamamoto, L.M., Marzano, S., Lopez, R.M., Jimenez, L., Le. B.L., Chevillotte, E., & Lieberman, H.R. (2011). Mild dehydration impairs cognitive performance and mood of men. British Journal of Nutrition. Volume 106. pp. 1535 - 1543
Gardner, A. & Rikberg Smyly, S. (1997). How do we stop doing and start listening: responding to the emotional needs of people with learning disabilities, British Journal of Learning Disabilities, Volume 25, pp. 26 - 30
Gardner, J.M. (1985). Using microcomputers to help staff reduce violent behavior. Computers in Human Services, Volume 1, pp. 53 - 61
Garretson, M.D. (1976). Total Communication, In - A bicentennial monograph on hearing impairment: Trends in the USA, Frizina, D.R. (Ed.), pp. 88 - 95, Washington, DC: Alexander Graham Bell Association for the Deaf
Gaskell, G., Dockrell, J., & Rehman, H. (1995) Community care for people with challenging behaviors and mild learning disability: An evaluation of an assessment and treatment unit. British Journal of Clinical Psychology, Volume 34(3), pp. 383 - 395
Gaylord-Ross, R.J. (1982). Curricular considerations in treating behavior problems of severely handicapped students. In K.D. Gadow and I. Bialer (Eds.), Advances in Learning and Behavioral Disabilities, Volume 1. JAI Press, Greenwich CT, pp.193 - 224
Geake, J. (2009). The Brain at School, Educational Neuroscience in the classroom. Open University Press.
Geary, D.C. (2000). From infancy to adulthood: The development of numerical abilities. European Child & Adolescent Psychiatry, Volume 9 (Supplement 2), S11 - S16
George, M.S., Costa, D.C., Kouris, K., Ring, H.A., & Ell, P.J. (1992). Cerebral blood flow abnormalities in adults with infantile autism. The Journal of Nervous and Mental Disease, Volume 180(7), pp. 413 - 417
Gergely, G. (2001). The obscure object of desire: ‘Nearly but clearly not, like me’: Contingency preference in normal children versus children with autism. Bulletin of the Menninger Clinic, Volume 65, pp. 411 - 426
Gergely, G., & Watson, J.S. (1999). Early social-emotional development: Contingency perception and the social-biofeedback model. In P. Rochat (Ed.). Early social cognition: Understanding others in the first months of life (pp. 101 - 136). Mahwah, NJ: Erlbaum.
Gerrity, Kevin W., Hourigan, Ryan M., & Horton, Patrick W. (2013). Conditions that facilitate music learning among students with special needs: A mixed-methods inquiry. Journal of Research in Music Education, Volume61(2), 144 - 159
Ghaem, O., Mellet, E., Crivello, F., Tzourio, N., Mazoyer, B., Bethoz, A., & Denis, M. (1997). Mental navigation along memorized routes activates the hippocampus, precuneus, and insula. NeuroReport, Volume 8. pp. 739 – 744
Gilbert, D. (2006). Stumbling on to happiness. New York: Alfed. A. Knopf
Gleason, J.J. (1993). The creation of meaning: what persons with severe or profound multiple developmental disabilities do in context. Australia and New Zealand Journal of Developmental Disabilities, Volume 18(3), pp. 157 - 167
Gledhill, K. (2009). Life experience packages (LEPs). Information Exchange, Volume 79, pp. 21 - 22
Glenn, S. (1987). Interactive approaches to working with children with profound and multiple learning difficulties, In Smith, B. (Ed), Interactive Approaches to the Education of Children with Severe Learning Difficulties. Birmingham: Westhill College
Glenn, S.M., & Cunningham, C.C. (2001). Evaluation of self by young people with Down syndrome. International Journal of Disability, Development and Education, Volume 48, pp. 163 - 177
Glenn, S.M, & Cunningham, C.C. (2004). Self-awareness in Young Adults with Down Syndrome: II. Self-understanding. International Journal of Disability, Development and Education, Volume 51(4), pp. 363 - 381
Godwin, K.E., Almeda, M.V., Seltman, H., Kai, S., Skerbetz, M.D., Baker, R.S., & Fisher, A.V. (2016). Off-task behavior in elementary school children. Learning and Instruction, Volume 44, pp. 128 - 143
Goldbart, J. (1994). Opening the communication curriculum to students with PMLDs. In - Jean Ware (Ed.), Educating Children with Profound and Multiple Learning Difficulties. pp. 15 - 62. David Fulton Publishers
Golden, J., & Reese, M. (1996). Focus on communication: Improving interaction between staff and residents who have severe or profound mental retardation. Research in Developmental Disabilities, Volume 17(5), pp. 363 - 382
Goldsmith, H.H., Van Hulle, C.A., Arneson, C.L., Schreiber, J.E., & Gernsbacher, M.A. (2006). A Population-Based Twin Study of Parentally Reported Tactile and Auditory Defensiveness in Young Children. Journal of Abnormal Child Psychology, Volume 34(3), pp. 378 – 392
Gomez-Pinilla, F. (2008). Brain foods: The effects of nutrients on brain function, Nature Reviews Neuroscience. Volume 9. pp. 568 -578
González, M.J., Miranda-Massari, J.R., Rodríguez Gómez, J., Ricart, C.M. & Rodriguez-Pagán, D. (2012). Energy Drinks and Health: A Brief Review of their Effects and Consequences. Ciencias de la Conducta. Volume 27(1). pp. 23 - 34
Goode, D. (2010). A world without words: The social construction of children born deaf and blind. Temple University Press.
Goodman, K. (2007). Music Therapy Group work with Special Needs Children. Springfield, IL: Charles C Thomas
Goodman, L. (1990). Time and learning in the special education classroom. Suny Press
Goodwin, D.L., Krohn, J., & Kuhnle, A. (2004). Beyond the wheelchair: The experience of dance. Adapted Physical Activity Quarterly, Volume 21(3), pp. 229 - 247
Goodwin, M., & Edwards, C. (2009). I’m Creative Too. PMLD Link, Volume
Goodwin, M., & Edwards, C. (2012). Playing or Playing Up? Behaviours and Schema with Young People with Severe Learning Disabilities. Bristol: Share – Short Breaks Network Magazine
Goodwin, M. (2013). Listening and responding to children with PMLD – towards a framework and possibilities. SLD Experience, Volume 65, pp. 21 - 27
Goodyer, I. (1995). Parents who don’t want peace and quiet. Article in - Times Educational Supplement. September 15, 1995, no 4133, page 13
Goold, L., & Hummell, J. (1993). Supporting the receptive communication of individuals with Significant Multiple Disabilities: selective use of touch to enhance comprehension. North Rocks, Australia: North Rocks Press
Gopinathan, P.M., Pichan, G., & Sharma, V.M. (1988). Role of dehydration in heat stress-induced variations in mental performance. Archives of Environmental Health, Volume 43. pp.15 - 17
Goss, P. (2006). Meaning-led learning for pupils with severe and profound and multiple learning difficulties. British Journal of Special Education. Volume 33 (4), pp. 210 - 219
Goswami, U. (2008). Cognitive Development: The Learning Brain. Hove: Psychology Press
Got, I.L.S., & Cheng, S.T. (2008). The effects of art facilitation on the social functioning of people with developmental disability. Art Therapy: Journal of the American Art Therapy Association, Volume 25(1), pp. 32 – 37
Gourgouvelis, J., Yielder, P., & Murphy, B. (2017). Exercise Promotes Neuroplasticity in Both Healthy and Depressed Brains: An fMRI Pilot Study. Neural Plasticity, Volume 2017, 13 pages
Grace, J. (2014). Sensory Stories for Children and Teens with Special Educational Needs. Jessica Kingsley Publishers
Grace, J. (2017). Sensory-Being for Sensory Beings: Creating Entrancing Sensory Experiences. Routledge
Graham, A., & Reid, G. (2000). Physical fitness of adults with an intellectual disability: A 13-year follow-up study. Research Quarterly for Exercise and Sport, Volume 71(2), pp. 152 - 161
Graham, J. (2004). Communicating with the uncommunicative: music therapy with pre-verbal adults. British Journal Learning Disability, Volume 32(1), pp. 24 - 29
Grandgeorge, M., Tordjman, S., Lazartigues, A., Lemonnier, E., Deleau, M., & Hausberger, M. (2012). Does pet arrival trigger prosocial behaviors in individuals with autism? PLoS ONE, Series 7: e41739
Grandin, T. (1992). An inside view of autism. In E. Schopler & G.B. Mesibov (Eds), High Functioning Individuals with Autism. Plenum Press, New York.
Grandin, T. (1992). My Experiences with Visual Thinking Sensory Problems and Communication Difficulties. Center for the Study of Autism
Grandin, T. (1996). Thinking in Pictures. New York: Vintage Books, Random House.
Grandjean, A.C. (2007). Dehydration and cognitive performance. Journal of the American College of Nutrition. Volume 26 (Supplement). pp. 549 - 554
Granlund, M., & Olsson, C. (1991). Investigating communicative functions in profoundly retarded persons: A comparison of two methods of obtaining information about communicative behaviours. Mental Handicap Research, Volume 6(2), pp. 112 - 119
Granlund, M., Steensson, A.L., Sundin, M., & Olsson, C. (1992). Inservice training in collaborative problem solving and goal setting for special education teacher consultants working with profoundly impaired persons. British Journal of Mental Subnormality, Volume 38(Part 2), pp. 94 - 113
Granlund, M., Terneby, J., & Olsson, C. (1992a). Creating communicative opportunities through a combined in-service training and supervision package. European Journal of Special Needs Education, Volume 7(3), pp. 229 - 252
Granlund, M., Terneby, J., & Olsson, C. (1992b). Subject characteristics and the communicative environment of profoundly retarded adults. Scandinavian Journal of Educational Research, Volume 36(4), pp. 323 - 338
Granlund, M., Björck-Åkesson, E., Brodin, J., & Olsson, C. (1995). Communication intervention for persons with profound disabilities: A Swedish perspective. Augmentative and Alternative Communication, Volume 11(1), pp. 49 - 59
Granlund, M., & Olsson, C. (1999). Efficacy of communication intervention for pre-symbolic communicators. Augmentative and Alternative Communication, Volume 15, pp. 25 - 37
Grant, A. (2013). Give and Take: A Revolutionary Approach to Success. Viking Books
Grant, G.W.B., & Moores, B. (1977). Resident characteristics and staff behavior in two hospitals for mentally retarded adults. American Journal of Mental Deficiency, Volume 82(3), pp. 259 - 265
Gray, B., & Ridden, G. (1999). Lifemaps of people with learning disabilities, Jessica Kingsley Publishers
Gray, R., & McAnespie, L. (2004) Consulted or excluded? Learning Disability Practice, Volume 7 (6), pp. 30 - 32
Greathead, S., Yates, R., Hill, V., Kenny, L., Croydon, A., & Pellicano, E. (2016). Supporting Children With Severe-to-Profound Learning Difficulties and Complex Communication Needs to Make Their Views Known: Observation Tools and Methods. Topics in Language Disorders. Volume 36(3), pp. 217 - 244
Green, C.W., Reid, D.H., White, L.K., Halford, R.C., Brittain, D.P., & Gardner, S M. (1988). Identifying reinforcers for persons with profound handicaps: Staff opinion versus systematic assessment of preferences. Journal of Applied Behavior Analysis, Volume 21(1), pp. 31 - 43
Green, C.W., Reid, D.H., Canipe, V.S., & Gardner, S.M. (1991). A comprehensive evaluation of reinforcer identification processes for persons with profound multiple handicaps. Journal of Applied Behavior Analysis, Volume 24, pp. 537 - 552
Green, C W., Reid, D.H., Perkins, L.I., & Gardner, S.M. (1991). Increasing habilitative services for persons with profound handicaps: An application of structural analysis to staff management. Journal of Applied Behavior Analysis, Volume 24, pp. 459 – 471
Green, C.W., Gardner, S.M., Canipe, V.S., & Reid, D.H. (1994). Analyzing alertness among people with profound multiple disabilities: implications for provision of training. Journal of Applied Behavior Analysis, Volume 27(3), pp. 519 - 531
Green, C.W., & Reid, D.H. (1996). Defining, validating, and increasing indices of happiness among people with profound multiple disabilities. Journal of Applied Behavior Analysis, Volume 29(1), pp. 67 – 78
Green, C.W., Gardner, C.M., & Reid, D.H. (1997). Increasing indices of happiness among people with profound multiple disabilities: a program replication and component analysis. Journal of Applied Behaviour Analysis, Volume 30 (2) pp. 217 - 228
Green, C.W., & Reid, D.H. (1999). A behavioral approach to identifying sources of happiness and unhappiness among individuals with profound multiple disabilities, Behavior Modification, Volume 23(2), pp. 280 – 293
Green, C.W., Middleton, S., & Reid, D.H. (2000). Embedded evaluation of preferences sampled from person-centered plans for people with profound multiple disabilities. Journal of Applied Behavior Analysis, Volume 33 (4), pp. 639 - 642
Green, C.W., Reid, D.H., Rollyson, J.H. & Passante, S.C. (2005). An enriched teaching program for reducing resistance and indices of unhappiness among individuals with profound multiple disabilities. Journal of Applied Behavior Analysis, Volume 38(2), pp. 221 – 233
Greenspan, S.I. (1996). The Challenging Child: Understanding, Raising, and Enjoying the Five 'Difficult' Types of Children. Da Capo Press
Griffin, J.C., Ricketts, R.W.,& Williams, D.E. (1986). Reaction to Richmond et al.: propriety of mechanical restrainst and protective devices as tertiary techniques. In K.D. Gadow (Ed.), Advances in Learning and Behavioural Disabilities.(Volume 5. London, JAI Press
Griffiths, C.R. (2010). Attuning: A Theory of Interaction of People with Severe and Profound Intellectual and Multiple Disability and Their Carers. Doctoral dissertation, Trinity College Dublin
Griffiths, M. (1994). Transition to Adulthood: The Role of Education for Young People with Severe Learning Difficulties. David Fulton; London.
Griffiths, M., & Tennyson, C. (1997). The Extended Curriculum: Meeting the Needs of Young People. David Fulton Publishers
Gron, G., Wunderlich, A.P., Spitzer, M., Tomczak, R., & Riepe, M.W. (2000). Brain activation during human navigation: gender-different neural networks. Nature Neuroscience, Volume 3. pp. 404 – 408
Gross, D.W., Li, L.M., & Andermann, F. (1998) Catastrophic deterioration and hippocampal atrophy after childhood status epilepticus. Annals of Neurology, Volume 43(5). pp. 687- 692
Grove, N., Porter, J., Bunning, K., & Olsson, C. (1999). See What I Mean: Interpreting the Meaning of Communication by People with Severe and Profound Learning Difficulties: Theoretical and Methodological Issues. Journal of Applied Research in Intellectual Disabilities, Volume 12 (3), pp. 190 - 203
Grove, N. (2001). See What I Mean: Guidelines to Aid Understanding of Communication by People with Severe and Profound Learning Disabilities. BILD Publications
Guenther, K. (2016). ‘It’s All Done With Mirrors’: V.S. Ramachandran and the Material Culture of Phantom Limb Research. Medical History. Volume 60(3). pp. 342 - 358
Guess, D., Benson, H. A., & Siegel-Causey, E. (1985). Concepts and issues related to choice-making and autonomy among persons with severe disabilities. Journal of The Association for Persons with Severe Handicaps, Volume 10 (2), pp. 79 - 86
Guess, D., Mulligan-Ault, M., Roberts, S., Struth, J., Siegel-Causey, E., Thompson, B., Bronicki, G.B., & Guy, B. (1988). Implications of biobehavioral states for the education and treatment of students with the most profoundly handicapping conditions. Journal of the Association for Persons with Severe Handicaps, Volume 13(3), pp. 163 - 174
Guess, D., & Carr, E.G. (1991). Emergence and Maintenance of of stereotypy and self-injury. American Journal on Mental Retardation. Volume 96, pp. 299 - 319
Guess, D., Roberts, S., Siegel-Causey, E., Ault, M., Guy, B., & Thompson, B. (1993). Analysis of behavior state conditions and associated environmental variables among students with profound handicaps. American Journal on Mental Retardation, Volume 97(6), pp. 634 - 653
Guess, D., Roberts, S., Siegel-Causey, E., & Rues, J. (1995). Replication and extended analysis of behavior state, environmental events, and related variables among individuals with profound disabilities. American Journal on Mental Retardation, Volume 100(1), pp. 36 – 50
Guess, D., & Siegel-Causey, D. (1995). Attractor dimensions of behavior state changes among individuals with profound disabilities. American Journal on Mental Retardation, Volume 99(6), pp. 642 - 663
Guess, D., Roberts, S., & Rues, J. (2002). Longitudinal analysis of state patterns and related variables among infants and children with significant disabilities. Research and Practice for Persons with Severe Disabilities, Volume 27(2), pp. 112 – 124
Gunnar, M.R., & Vazquez, D. (2006). Stress neurobiology and developmental psychopathology. In D. Cicchetti & D. Cohen, (Eds.), Developmental psychopathology, volume 2: Developmental neuroscience (2nd edition). New York: John Wiley & Sons, Inc
Gunnar, M.R., & Quevedo, K. (2007). The Neurobiology of Stress and Development. Annual Review of Psychology. Volume 58. pp. 145 - 173
Gunsett, R.P., Mulick, J.A., Fernald, W.B., & Martin, J.L. (1989). Brief report: Indications for medical screening prior to behavioral programming for severely and profoundly mentally retarded clients. Journal of Autism and Developmental Disorders, Volume 19, pp. 167 - 172
Gupta, S.K., & Ratnam, B.V. (2009). Cerebral Perfusion Abnormalities in Children with Autism and Mental Retardation: A Segmental Quantitative SPECT Study. Indian Pediatrics. Volume 46. pp. 161 -164
Gutowski, S.J. (1996). Response acquisition for music or beverages in adults with profound multiple handicap. Journal of Developmental and Physical Disabilities. Volume 8(3), pp. 221 – 231
Hackett, S.S., & Critchley, S. (2012). From art therapy to arts in health: Bridging the gap for people with learning disabilities. Newsbriefing, November, pp. 12 – 13.
Hackett, S., Rothwell, K., Lyle, C., Bourne, J., Downing, L., & Morison, C.J. (2016). Art, drama and music therapies, In - Nigel Beail, (Ed.), Psychological therapies and people who have intellectual disabilities, Chapter 10, pp. 93 -98. Commissioning Team for the Faculties for Intellectual Disabilities of the Royal College of Psychiatrists and the Division of Clinical Psychology of the British Psychological Society
Hagopian, L.P., Long, E.S., & Rush, K.S. (2004). Preference assessment procedures for individuals with developmental disabilities. Behavior Modification, Volume 28(5), pp. 668 – 677
Haith, M.M. (1972). The forgotten message of the infant smile. Merrill-Palmer Quarterly, Volume 18, pp. 321 - 322
Hall, S., Oliver, C., & Murphy, G. (2001). The early development of self-injurious behaviour: An empirical study. Americal Journal on Mental Retardation, Volume 106, pp.189 - 199
Halle, J.W., & Spradlin, J.E. (1993). Identifying stimulus control of challenging behavior. In J. Reichle & D.P. Wacker (Eds.), Communicative
alternatives to challenging behavior: Integrating functional assessment and intervention strategies, pp. 83–109. Baltimore: Paul H. Brookes.
Hamilton, M.T., Hamilton, D.G., & Zderic, T.W. (2007). Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes, Volume 56, pp. 2655 – 2667
Hamlin, J.K., Wynn, K., & Bloom, P. (2007). Social evaluation by preverbal infants. Nature, Volume 450(7169), pp. 557 - 559
Happe, F.G., Brownell, H., Winner, E. (1999). Acquired "theory of mind" impairments following stroke. Cognition, Volume 70, pp. 211 - 240
Haring, N., Liberty, K., & White, O. (1981). An Investigation of Phases of Learning and Facilitating Instructional Events for the Severely/Profoundly Handicapped (final project report). Seattle: University of Washington College of Education.
Harlow, H.F. (1959). The development of learning in the rhesus monkey. American Scientist.
Harlow, H.F. (1964). Early social deprivation and later behavior in the monkey. In - Abrams, A., Gurner, H.H., & Tomal, J.E.P. (Eds.), Unfinished tasks in the behavioral sciences, pp.154 - 173, Baltimore: Williams & Wilkins
Harlow, H.F., Dodsworth, R.O., & Harlow, M.K. (1965). Total social isolation in monkeys. Proceedings of the National Academy of Sciences, Volume 54(1), pp. 90 - 97
Harlow, H.F., & Harlow, M.K. (1969). Effects of various mother-infant relationships on rhesus monkey behaviors. Determinants of Infant Behavior, Volume 4, pp. 15 - 36
Harlow, H.F., Harlow, M.K., & Suomi, S.J. (1971). From thought to therapy: lessons from a primate laboratory. American Scientist. Volume 59(5), pp. 538 – 549
Harlow, H.F., & Suomi, S.J. (1971). Social recovery by isolation-reared monkeys. Proceedings of the National Academy of Sciences, Volume 68(7), pp. 1534 - 1538
Harlow, H.F., & Suomi, S.J. (1974). Induced depression in monkeys. Behavioral Biology, Volume 12(3), pp. 273 - 296
Harris, C., & Card, B. (2012). A pilot study to evaluate nutritional influences on gastrointestinal symptoms and behavior patterns in children with Autism Spectrum Disorder. Complementary Therapies in Medicine, Volume 20(6), pp. 437 - 440
Harris, J., Cook, M., & Upton, G. (1996). Pupils with Severe Learning Difficulties who Present Challenging Behaviour: a whole school approach to assessment and intervention. Kidderminster: BILD.
Harris, L.P. (1977). Self-recognition among institutionalized profoundly retarded males: A replication. Bulletin of the Psychonomic Society, Volume 9, pp. 43 - 44
Harris, P. (1993). The nature and extent of aggressive behaviour among people with learning difficulties (mental handicap) in a single health district. Journal of Intellectual Disability Research. Volume 37, pp. 221 - 242
Harris, S.L., & Wolchik, S.A. (1979). Suppression of self stimulation: Three alternative strategies. Journal of Applied Behavior Analysis, Volume 12, pp. 185 – 198
Hart, J., Bock, K.A., Cartaxo, A., Converse, J., & Ferro, P. (2015). Round table Discussion: The impact of GI and nutritional issues on autism. Alternative and Complementary Therapies, Volume 21(2), pp. 84 - 89
Hart, P. (2006). Using imitation with congenitally deafblind adults: Establishing meaningful communication partnerships. Infant and Child Development, Volume 15, pp. 263 - 274
Harter, S. (1990). Self and identity development. In S. Feldman & G. Elliott (Eds.), At the threshold: The developing adolescent (pp. 352 –387). Cambridge: Harvard University Press.
Hassiotis, A.A. & Hall, I. (2008). Behavioural and cognitive behavioural interventions for outwardly directed aggressive behaviour in people with learning disabilities. Cochrane Database of Systematic Reviews (3), Art. No. CD003406.
Hastings, R.P.,& Remington, P.B. (1994). Staff behaviour and its implications for people with learning disabilities and challenging behaviours, British Journal of Clinical Psychology, Volume 33(4), pp. 423 – 438
Hastings, R.P., Remington, P.B., & Hopper, G.M. (1995). Experienced and inexperienced health care workers’ beliefs about challenging behaviours. Journal of Intellectual Disability Research, Volume 39(6), pp. 474 – 483
Hastings, R.P. (1997). Measuring staff perceptions of challenging behaviour: The Challenging Behaviour Attributions Scale (CHABA),
Journal of Intellectual Disability Research, Volume 41(6), pp. 495 – 501
Hastings, R.P. (2002). Do challenging behaviors affect staff psychological well-being? Issues of causality and mechanism. American Journal on Mental Retardation, Volume 107(6), pp. 455 – 467
Hastings, R.P., & Brown, T. (2002) Behavioural knowledge, causal beliefs and self-efficacy as predictors of special educator’s emotional reactions to challenging behaviour. Research in Developmental Disabilities. Volume 24, pp. 323 – 332
Hastings, R.P. (2005). Staff in special education settings and behaviour problems: Toward a framework for research and practice.
Educational Psychology, Volume 25(2/3), pp. 207 – 221
Hatch-Rasmussen, C. (1995). Sensory integration. Center for the Study of Autism at www. autism. org/si. html.
Hatton, C., Brown, R., Caine, A., & Emerson, E. (1995) Stressors, coping strategies and stress-related outcomes among direct care staff in staffed houses for people with learning disabilities. Mental Handicap Research, Volume 8(4), pp. 252 - 271
Hatton, C., Emerson, E., Robertson, J., Henderson, D., & Cooper, J. (1996). Factors associated with staff support and resident lifestyle in services for people with multiple disabilities: a path analytic approach. Journal of Intellectual Disability Research, Volume 40(5), pp. 466 - 477
Hatton, C., Emerson, E., Rivers, M., Mason, H., Swarbrick, R., Mason, L., Kiernan, C., Reeves, D., & Alborz, A. (2001). Factors associated with intended staff turnover and job search behaviour in services for people with intellectual disability. Journal of Intellectual Disability Research, Volume 45(3), pp. 258 - 270
Hatton, C. (2004). Choice. In E. Emerson, C. Hatton, T. Thompson, & T.R. Parmenter (Eds.), The international handbook of applied research in intellectual disabilities (pp. 335 – 351). Chichester: John Wiley & Sons
Hayashida, N., Hiramatsu, K., Katayama, S., Koga, M., Kudo, T., Mori, S., Orita, M., Shinkawa, T., Takamura, N., & Togo, M. (2012). Monitoring the autonomic nervous activity as the objective evaluation of music therapy for severely and multiply disabled children. The Tohoku Journal of Experimental Medicine, Volume 227(3), pp. 185 - 189
Hayes, T. (2016). Music Therapy in the Context of the Special School. In - J. Edwards (Ed.), Oxford Handbook of Music Therapy, pp. 176 - 185. Oxford: Oxford University Press
Healy, D., & Noonan Walsh, P. (2007). Communication among nurses and adults with severe and profound intellectual disabilities: predicted and observed strategies. Journal of Intellectual Disabilities, Volume 11(2), pp. 127 - 141
Healy, J. (1994). Your Child's growing Mind: A Practical Guide ot Brain Development from Birth to Adolescence. New York: Doubleday
Heath, G.W., & Fenten, P.H. (1997). Physical activity among persons with disabilities – a public health perspective. Exercise and Sports Science Reviews. Volume 25, pp. 195 – 234
Heaton, P., & Wallace, G.L. (2004). Annotation: The savant syndrome. Journal of Child Psychology and Psychiatry, Volume 45(5), pp. 899 - 911
Heimlich, K. (2001). Animal-assisted therapy and the severely disabled child: A quantitative study. Journal of Rehabilitation. Volume 67(4). pp. 48 - 54
Heller, S. (2004). Too Loud Too Bright Too Fast Too Tight: What to Do If You are Sensory Defensive in an Overstimulating World. Harper Collins: Reprint edition
Heller, S. (2015). Uptight & Off Center: How Sensory Processing Disorder Throws Adults Off Balance & How to Create Stability. Symmetry
Heller, T., Miller, A.B., & Factor, A. (1999). Autonomy in residential facilities and community functioning of adults with mental retardation. Mental Retardation, Volume 37(6), pp. 449 - 457
Helm, D.T. (2000). The measurement of happiness. The American Journal on Mental Retardation, Volume 105(5), pp. 326 – 335
Hemmings, C.P., Gravestock, S., Pickard, M., & Bouras, N. (2006). Psychiatric symptoms and problem behaviours in people with intellectual disabilities. Journal of Intellectual Disability Research, Volume 50, pp. 269 - 276
Henderson, E. (2005). Journeys Toward Communication. PMLD Link. Volume 17(1), Issue 50, pp. 19 - 21
Henry, D.B., Duvdevany, I., Keys, C.B., & Balcazar, F.E. (2004). Attitudes of American and Israeli staff toward people with intellectual disabilities. Mental Retardation, Volume 42(1), pp. 26 - 36
Herbert, M.R., & Buckley, J.A. (2013). Autism and dietary therapy: case report and review of the literature. Journal of Child Neurology, Volume 28(8), pp. 975 - 982
Hermelin, B., O’Connor, N., & Lee, S. (1987). Musical inventiveness of five idiot-savants. Psychological Medicine, Volume17(3), pp. 695 - 694
Hermelin, B., & O’Connor N. (1991). Talents and preoccupations in idiot-savants. Psychological Medicine, Volume 21(4), pp. 959 - 964
Herzog, H. (2011). The impact of pets on human health and psychological well-being: fact, fiction or hypothesis? Current Directions in Psychological Science. Volume 20(4), pp. 236 - 239
Hewett, D. (2006). The most important and complicated learning: that’s what play is for! ICAN Talking Point, March. www.talkingpoint.org.uk
Hewett, D. (2007). Do touch: physical contact and people who have severe, profound and multiple learning difficulties, Support for Learning, Volume 22 (3), pp.116 -123
Hewett, D. & Nind, M. (1988). Developing an Interactive Curriculum for Pupils with Severe and Complex Learning Difficulties, in Smith, B. (Ed), Interactive Approaches to the Education of Children with Severe Learning Difficulties. Birmingham: Westhill College.
Hewett, D. (1989). The Most Severe Learning Difficulties: Does Your Curriculum Go Back Far Enough?’ in Ainscow, M. (Ed), Special Education in Change. London: David Fulton.
Hewett, D., & Nind, M. (1989). Interaction as Curriculum at Harperbury School, PMLD Link 5.
Hewett, D., & Nind, M. (1989). Developing an interactive curriculum for pupils with severe and complex learning difficulties: a classroom process. In Interactive approaches to the education of children with severe learning difficulties. Smith, B. (Ed.). Birmingham: Westhill College
Hewett, D., & Nind, M. (1992). Returning to the Basics: A Curriculum at Harperbury Hospital School’, in: Booth, T., Swann, W., Masterton, M., & Potts, P. (Eds.), Curricula for Diversity in Education. London: Open University Press/Routledge
Hewett, D., & Nind, M. (1993). Access to Communication. Intensive Interaction: an approach to helping learners who are still in the pre-speech stages of communication learning, Information Exchange 37, May 1993.
Hewett, D. (1994). Understanding and writing a methodology of Intensive Interaction – teaching pre-speech communication abilities to learners with severe learning difficulties: a naturalistic inquiry using qualitative evaluation methods. Ph.D Thesis, Cambridge Institute of Education.
Hewett, D. (1996). How to do Intensive Interaction, in Collis, M. & Lacey, P. 1996 (eds) Interactive Approaches to Teaching: A Framework for INSET, London: David Fulton.
Hewett, D. & Nind, M. (2003). Severe Learning Difficulties: Intensive Interaction, Five to Eleven, Volume 2(10) pp.30 - 32
Hewett, D. (2007): Do touch: physical contact and people who have severe, profound and multiple learning difficulties. Support for Learning, Volume 22 (3), pp. 116 - 123
Higgins, E.T. (1987). Self-Discrepancy: A Theory Relating Self and Affect. Psychological Review. Volume 94(3), pp. 319 - 340
Hile, M.G., & Walbran, B.B. (1991). Observing staff-resident interactions: What staff do, what residents receive. Mental Retardation, Volume 29(1), pp. 35 - 41
Hilgenkamp, T.I.M., Reis, D., van Wijck, R., & Evenhuis, H.M. (2012). Physical activity levels in older adults with intellectual disabilities are extremely low. Research in Developmental Disabilities, Volume 33(2), pp. 477 – 483
Hill, B.K., & Bruininks, R.H. (1984). Maladaptive behavior of mentally retarded individuals in residential facilities. American Journal of Mental Deficiency, Volume 88, pp. 380 - 387
Hill, J., Brantner, J., & Spreat, S. (1989). The effect of contingent music on the in-seat behavior of a blind young woman with profound mental retardation. Education and Treatment of Children, Volume 12(2), pp. 165 - 173
Hill, S.D., & Tomlin, C. (1981). Self-recognition in retarded children. Child Development, Volume 52, pp. 145 - 150
Hillery, J. & Mulcahy, M. (1997). Self-injurious behaviour in persons with a mental handicap: an epidemiological study in an Irish population. Irish Journal of Psychological Medicine, Volume 14, pp. 12 - 15
Hirabuki, N., Fujita, N., Fujii, K., Hashimoto, T., & Kozuka, T. (1994). MR appearance of Virchow-Robin spaces along lenticulostriate arteries: spin-echo and two-dimensional fast low-angle shot imaging. American Journal of Neuroradiology, Volume 15(2), pp. 277 - 281
Hirama, H. (1989). Self-injurious behavior: A somatosensory treatment approach. Bethesda, MD: Chess Publications.
Hirstwood, R. (1998). Communication in multi-sensory rooms. Focus, Volume 23, pp. 20 - 31
Hobbs, V., How, R., & Lloyd, J. (2006). An Alternative curriculum. Insight, Volume 6. pp. 31 - 33
Hobbs, V. (2009). Maximising the progress of learners with profound and multiple learning difficulties. The SLD Experience. Volume 55(1), pp. 10 - 16
Hobbs, V. (2012). Where are the pupils with profound and multiple learning difficulties? The SLD Experience. Volume 64(1), pp. 24 - 28
Hobbs, V. (2012). Assessing the achievements of learners with PMLD, Education Today, Volume 61(3)
Hobbs, V. (2014). What do practitioners believe are the elements, conditions, factors and considerations that contribute to the provision of an appropriate and relevant learning environment for pupils with Profound and Multiple Learning Difficulties? Unpublished report for Associateship, Institute of Education
Hodgson, C., & Berry, M. (Eds.)(2011). Adventure Education: An Introduction. Taylor & Francis
Hoefkens, A., & Allen, D. (1990). Evaluation of a special behaviour unit for people with mental handicaps and challenging behaviour. Journal of Mental Deficiency Research, Volume 34, pp. 213 - 228
Hoehn, T.P., & Baumeister, A.A. (1994). A critique of the application of sensory integration therapy to children with learning disabilities.
Journal of Learning Disabilities, Volume 27, pp. 338 - 350
Hoffman, M.B., & Rand, Y. (2014). Instrumental enrichment, an intervention program for structural cognitive modifiability: Theory and practice. Thinking and Learning Skills: Volume 1: Relating Instruction To Research, Volume 43.
Hoge, G., & Dattilo, J. (1995). Recreation participation patterns of adults with and without mental retardation. Education and Training in Mental Retardation and Developmental Disabilities, Volume 30(4), pp. 283 - 298
Hogg, J., & Sebba, J. (1986a). Profound Retardation and Multiple Impairment. Volume I, Croom Helm
Hogg, J., & Sebba, J. (1986b). Profound Retardation and Multiple Impairment. Volume II, Croom Helm
Hogg, J., Sebba, J., & Lambe, L. (1990). Profound Retardation and Multiple Impairment. Volume III, Medical and Physical care and Managment. Chapman and Hall: London
Hogg, J. (1992). The administration of psychotropic and anticonvulsant drugs to children with profound intellectual disability and multiple
impairments. Journal of Intellectual Disability Research, Volume 36(6), pp. 473 - 488
Hogg, J. (1995). The Ecology of Leisure Provision:Context and Engagement, in Hogg, J., & Cavet, J. (Eds.), Making Leisure Provision for People with Profound and Multiple Disabilities, Chapman & Hall
Hogg, J., & Cavet, J. (Eds.) (1995). Making Leisure Provision for People with Profound and Multiple Disabilities. London:Chapman & Hall
Hogg, J., Cavet, J., Lambe, L., & Smeddle, M. (2001). The use of 'Snoezelen' as multisensory stimulation with people with intellectual disabilities: a review of the research. Research in Developmental Disabilities, Volume 22(5), pp. 353 - 372
Hogg, J., Reeves, D., Roberts, J., & Mudford, O.C. (2001). Consistency, context and confidence in judgements of affective communication in adults with profound intellectual and multiple disabilities. Journal of Intellectual Disability Research, Volume 45(1), pp. 18 - 29
Holburn, S. (1997). A renaissance in residential behavior analysis? A historical perspective and a better way to help people with challenging behavior. The Behavior Analyst, Volume 20(2), pp. 61 - 85
Holburn, S., & Vietze, P. (Eds.). (2002). Person-centered planning: Research, practice, and future directions. Paul H Brookes Publishing Company.
Holburn, S., Nguyen, D., & Vietze, P.M. (2004). Computer‐assisted learning for adults with profound multiple disabilities. Behavioral Interventions, Volume 19(1), pp. 25 - 37
Holland, T., & Murphy, G. (1990). Behavioural and psychiatric disorder in adults with mild learning difficulties. International Review of Psychiatry, Volume 2, pp. 117 - 136
Holmes, J., Gathercole, S.E., & Dunning, D.L. (2009). Adaptive training leads to sustained enhancement of poor working memory in children. Developmental Science, Volume 12(4), pp. F1 - F7
Holmes, J., & Gathercole, S.E. (2014). Taking working memory training from the laboratory into schools. Educational Psychology, Volume 34(4), pp. 440 - 450
Hong, E. & Perkins, P.G. (1997). Children's Responses to Self-Concept Questionnaires Administered in Differential Contexts. Child Study Journal, Volume 27(2), pp. 111 - 127
Hooper, J, & Lindsay, B. (1990). Music and the Mentally Handicapped - the Effect of Music on Anxiety. Journal of British Music Therapy, Volume 4, pp. 19 - 26
Hooper, J., Lindsay, B., & Richardson, I. (1991). Recreation and music therapy: An experimental study. Journal of British Music Therapy, Volume 5(2), pp. 10-13
Hooper, J., & Lindsay, B. (1992). Improving the quality of life through music: A case study. Mental Handicap, Volume 20(1), pp. 27 - 30
Hooper, J., & Lindsay, B. (1997). The Use of the Somatron on the Treatment of Anxiety Problems with Clients who Have Learning Disabilities. In - C.D.T. Wigram (Ed.), Music, Vibration and Health. Cherry Hill, NJ: Jeffrey Books
Hooper, J. (2001). Overcoming the problems of deinstitutionalization: Using music activities to encourage interaction between four adults with a developmental disability. Music Therapy Perspectives, Volume 19(2), pp. 121 - 127
Hooper, J. (2002). Using music to develop peer interaction: An examination of the response of two subjects with a learning disability. British Journal of Learning Disabilities, Volume 30, pp. 166 – 170
Hooper, J., McManus, A., & McIntyre, A. (2004). Exploring the link between music therapy and sensory integration: An individual case study. British Journal of Music Therapy, Volume 18(1), pp. 15 - 23
Hooper, J., Wigram, T., Carson, D., & Lindsay, B. (2011). The practical implication of comparing how adults with and without intellectual disability respond to music. British Journal of Learning Disabilities, Volume 39(1), pp. 22 - 28
Hoppestad, B.S. (2007). Inadequacies in computer access using assistive technology devices in profoundly disabled individuals: An overview of the current literature. Disability and Rehabilitation: Assistive Technology, Volume 2(4), pp. 189 - 199
Horak, F.B., Shumway‐Cook, A., Crowe, T.K., & Black, F.O. (1988). Vestibular function and motor proficiency of children with impaired hearing, or with learning disability and motor impairments. Developmental Medicine & Child Neurology, Volume 30(1), pp. 64 - 79
Horner, R.D. (1980). The effects of an environmental “enrichment” program on the behaviour of institutionalized profoundly retarded children. Journal of Applied Behaviour Analysis, Volume 13, pp. 473 – 491
Horner, R.H., Day, H.M., Sprague, J.R., O'Brien, M., & Heathfield, L.T. (1991). Interspersed requests: A nonaversive procedure for decreasing aggression and self injury during instruction. Journal of Applied Behavior Analysis, Volume 24, pp. 265 - 278
Horner, R.H., & O'Neill, R. (1992). Oregon Community Support: A two year analysis of community support for 11 people with histories of severe problem behaviour. Paper presented at the Association for Behavior Analysis, 18th Annual Convention, 25-28 May, 1992, San Francisco.
Horner, R.H., Close, D.W., Fredericks, H.D.B., O'Neill, R.E., Albin, R.W., Sprague, J.R., Kennedy, C.H., Flannery, K.B., & Heathfield, L.T. (1996). Supported living for people with severe problem behaviors: A demonstration. In D. H. Lehr & F. Brown (Eds.), Persons with disabilities who challenge the system. Baltimore: Paul H Brookes.
Hostyn, I., & Maes, B. (2009). Interaction between persons with profound intellectual and multiple disabilities and their partners: A literature review. Journal of Intellectual and Developmental Disability, Volume 34(4), pp. 296 - 312
Hostyn, I., Daelman, M., Janssen, M.J., & Maes, B. (2010). Describing dialogue between persons with profound intellectual and multiple disabilities and direct support staff using the scale for dialogical meaning making. Journal of Intellectual Disability Research, Volume 54(8), pp. 679 - 690
Hostyn, I., Neerinckx, H., & Maes, B. (2011): Attentional processes in interactions between people with profound intellectual and multiple disabilities and direct support staff. Research in Developmental Disability. Volume 32 (2): pp. 491 - 503
Houghton, J., Bronicki, G.J.B., & Guess, D. (1987). Opportunities to express preferences and make choices among students with severe disabilities in classroom settings. Journal of The Association for Persons with Severe Handicaps, Volume 12(1), pp. 18 – 27
Houwen, S., van der Putten, A., & Vlaskamp, C. (2014). A systematic review of the effects of motor interventions to improve motor, cognitive, and/or social functioning in people with severe or profound intellectual disabilities. Research in Developmental Disabilities, Volume 35, pp. 2093 – 2116
Hove, O. (2004). Weight survey on adult persons with mental retardation living in the community. Research in Developmental Disabilities, 25(1), pp. 9 - 17
Howe, M.B., Brittain, L.A., & McCathren, R.B. (2004). Meeting the Sensory Needs of Young Children in Classrooms. Young Exceptional Children. Volume 8(1), pp. 11 - 19
Howlin, P., Goode, S., Hutton, J., & Rutter, M. (2009). Savant skills in autism: psychometric approaches and parental reports. Philosophical Transactions of the Royal Society of London B: Biological Sciences, Volume 364(1522), pp. 1359 - 1367
Hsu, C.L., Lin, C.Y., Chen, C.L., Wang, C.M., & Wong, M.K. (2009). The effects of a gluten and casein-free diet in children with autism: a case report. Chang Gung Medical Journal, Volume 32(4), pp. 459 - 465
Huff, D.M., & Harris, S.C. (1987). Using sensorimotor integrative treatment with mentally retarded adults. American Journal of Occupational Therapy, Volume 41, pp. 227 - 231
Hughes, C., Pitkin, S.E., & Lorden, S.W. (1998). Assessing preferences and choices of persons with severe and profound mental
retardation. Education and Training in Mental Retardation and Developmental Disabilities, Volume 33(4), pp. 299 - 316
Hughes, M.W., Schuster, J.W., Nelson, C.M. (1993). The acquisition of independent dressing skills by students with multiple disabilities. Journal of Developmental and Physical Disabilities, Volume 5(4), pp. 233 - 252
Hughes, R.N. (1996). Drugs which induce anxiety: caffeine. New Zealand Journal of Psychology. Volume 25(1), pp. 36 - 42
Hui-chuan, Chu (2002). Functional Analysis and Assessment-based Interventions for Aberrant Behavior of Children with Developmental Disabilities. Journal of National Taipei Teachers College. Volume 15, pp. 387 - 432
Hulme, C., & Mackenzie, S. (1992). Working Memory and Severe Learning Difficulties. Hove: Lawrence Erlbaum Associates
Hulsegge, J., & Verheul, A. (1987). Snoezelen, another world. A practical book of sensory experience environments for the mentally handicapped. Chesterfield: Rompa
Humphries, K., Traci, M.A., & Seekins, T. (2009). Nutrition and adults with intellectual or developmental disabilities: systematic literature review results. Intellectual and Developmental Disabilities, Volume 47(3), pp. 163 - 185
Humphries, T., Wright, M., McDougall, B., & Vertes, J. (1990). The efficacy of sensory integration therapy for children with learning
disability. Physical and Occupational Therapy in Pediatrics, Volume 10(3), pp.1 - 17
Humphries, T., Wright, M., Snider, L., & McDougall, B. (1992). A comparison of the effectiveness of sensory integrative therapy and
perceptual-motor training in treating children with learning disabilities. Developmental and Behavioral Pediatrics, Volume 13(I), pp. 31 - 40
Humphries, T.W., Snider, L., & McDougall, B. (1993). Clinical evaluation of the effectiveness of sensory integrative and perceptual
motor therapy in improving sensory integrative function in children with learning disabilities. Occupational Therapy Journal of Research, Volume 13, pp. 163 - 182
Humphreys, M., Churchill, R., & Kerr, E. (2014). The Multi-Sensory Project: Art for all the Senses. PMLD Link, Volume 26(3), Issue 79, pp. 2 - 4
Hurwitz, S. (2013). The gluten-free, casein-free diet and autism: limited return on family investment. Journal of Early Intervention, Volume 35(1), pp. 3 - 19
Hutchinson, L.M., Hastings, R.P., Hunt, P.H., Bowler, C.L., Banks, M.E., & Totsika, V. (2014). Who's Challenging Who? Changing attitudes towards those whose behaviour challenges. Journal of Intellectual Disability Research, Volume 58(2), pp. 99 - 109
Hydration For Health (2015). Hydration, mood state and cognitive function. Hydration For Health Initiative. Danone Nutricia Research
Hylkema, T., & Vlaskamp, C. (2009). Significant improvement in sleep in people with intellectual disabilities living in residential settings by
non-pharmaceutical interventions. Journal of Intellectual Disability Research, Volume 53(8), pp. 695 - 703
Hyman, P., Oliver, C., & Hall, S. (2002). Self-Injurious Behaviour, Self-Restraint, and Compulsive Behaviors in Cornelia de Lange Syndrome. American Journal on Mental Retardation, Volume 107(2), pp. 146 – 154
Hyman, S.L., Stewart, P.A., Smith, T., Foley, J., Cain, U., Peck, R., Morris, D.D., & Wang, H. (2010). The gluten free and casein free (GFCF) diet: A double blind, placebo controlled challenge study. Presented at International Meeting for Autism Research, Philadelphia, PA.
Hyman, S.L., Stewart, P.A., Foley, J., Cain, U., Peck, R., Morris, D.D., Wang, H., & Smith, T. (2016). The gluten-free/casein-free diet: a double-blind challenge trial in children with autism. Journal of Autism and Developmental Disorders, Volume 46(1), pp. 205 - 220
Imray, P. (2005). Moving towards simple, understandable and workable definitions of severe learning difficulties and profound and multiple learning difficulties. SLD Experience, Volume 42: pp. 33 - 37
Imray, P., & Hinchcliffe, V. (2012). Not fit for purpose: a call for separate and distinct pedagogies as part of a national framework for those with severe and profound learning difficulties, Support for Learning, Volume 27(4), pp. 150 - 157
Imray, P., & Hinchcliffe, V. (2013). Curricula for Teaching Children and Young People with Severe or Profound and Multiple Learning Difficulties. David Fulton / Nasen
Inal, S. (2014). Competitive dance for individuals with disabilities. PALAESTRA: Forum of Sport, Physical Education, and Recreation for Those with Disabilities, Volume 28(1), pp. 32 - 35
Ionatamishvili, N.I., Tsverava, D.M., Loriya, M.S., Sheshaberidze, E.G., & Rukhadze, M.M. (2004). Riding therapy as a method of rehabilitation of children with cerebral palsy. Human physiology, Volume 30(5), pp. 561 - 565
Intagliata, J., & Willer, B. (1982). Reinstitutionalization of mentally retarded persons successfully placed into family-care and group homes. American Journal of Mental Deficiency, Volume 87(1), pp. 34 - 39
Irvin, D.S. (2006). Using analog assessment procedures for determining the effects of a gluten‐free and casein‐free diet on rate of problem behaviors for an adolescent with autism. Behavioral Interventions, Volume 21(4), pp. 281 - 286
Irvine, C. (1998). Addressing the needs of adults with profound and multiple learning disabilities in social services provision, in Hewett, D and Nind, M. (Eds.), Interaction in Action. David Fulton. London
Irvine, C. (2001). On the floor and playing…, Royal College of Speech and Language Therapy Bulletin, November, pp. 9 - 11
Irvine, C. (2002). Preliminary findings of an informal longitudinal study into the research/practice interface: noting the influence of extra trees in the wood rather than throwing the baby out with the bathwater, Speech and Language Therapy in Practice
Isaacs, E., & Oates, J. (2008). Nutrition and cognition: assessing cognitive abilities in children and young people. European Journal of Nutrition. Volume 47(Supplement 3). pp. 4 – 24
Ivancic, M.T., & Bailey, J.S. (1996). Current limits to reinforcer identification for some persons with profound multiple disabilities. Research in Developmental Disabilities, Volume 17(1), pp. 77 - 92
Ivancic, M.T., Barrett, G.T., Simonow, A., & Kimberly, A. (1997). A replication to increase happiness indices among some people with profound multiple disabilities. Research in Developmental Disabilities, Volume 18(1), pp. 79 - 89
Iwasaki, K., & Holm, M.B. (1989). Sensory treatment for the reduction of stereotypic behaviors in persons with severe multiple disabilities. Occupational Therapy Journal of Research, Volume 9, pp. 170 – 183
Iwata, B.A., Dorsey, M.F., Slifer, K.J., Bauman, K.E., & Richman, G.S. (1982). Toward a functional analysis of self-injury. Analysis and Intervention in Developmental Disabilities, Volume 2, pp. 3 - 20
Iwata, B.A., Pace, G., Kalsher, M., Cowdery, G., & Cataldo, M. (1990). Experimental analysis and extinction of self-injurous escape behavior. Journal of Applied Behavior Analysis, Volume 23, pp. 11 - 27
Jacobson, J.W. (1982). Problem behaviour and psychiatric impairment within a developmentally disabled population I: behaviour frequency. Applied Research in Mental Retardation, Volume 3, pp. 121 - 139
Jackson, J. (2014). ‘Sit with me, talk to me’: How the use of multi-media advocacy supported a brighter future for a nineteen year old learner
coping with PMLD and presenting challenging verbal behaviour. PMLD Link. Volume 26(3), Issue 79, pp. 39 - 44
Jackson, E., & Jackson, N. (1999). Helping people with a learning disability explore choice. London: Jessica Kingsley Publishers
Jackson, N., & Jackson, E. (1998). Choice making for people with a learning disability. Learning Disability Practice; Volume 1(3), pp. 22 – 25
Jacobson, J.W., Foxx, R.M., & Mulick J.A. (2005). Controversial therapies for developmental disabilities. Fad, fashion, and science in professional practice. Mahwah, New Jersey: Lawrence Erlbaum Associates, Publishers
Jambaqué, I., Hertz-Pannier, L., Mikaeloff, Y., Martins, S., Peudenier, S., Dulac, O., & Chiron, C. (2003). Severe memory impairment in a child with bihippocampal injury after status epilepticus. Developmental Medicine and Child Neurology. Volume 48(3). pp 223 - 226
James, J. (1996a). Dramatherapy with people with learning disabilities. In - S. Mitchell (Ed.), Dramatherapy: Clinical Studies. Jessica Kingsley: London. pp. 15 - 32
James, J. (1996b). Poetry in motion: drama and movement therapy with people with learning disabilities. In - J. Pearson (Ed.), Discovering the Self through Drama and Movement. Jessica Kingsley: London. pp. 209 - 221
Janicki, M.P., & Dalton, A.J. (1998). Sensory impairments among older adults with intellectual disability. Journal of Intellectual and Developmental Disability, Volume 23(1), pp. 3 - 11
Jansen, D.E., Krol, B., Groothoff, J.W., & Post, D. (2004). People with intellectual disability and their health problems: a review of comparative studies. Journal of Intellectual Disability Research, Volume 48(2), pp. 93 - 102
Jansma, P., McCubbin, J., Combs, S., Decker, J., & Ersing, W. (1987). Fitness and hygiene programming for the severely handicapped: A curriculum-embedded assessment guide. Worthington, OH: Moody's.
Janssen, M.J., Riksen-Walraven, J.M., & van Dijk, J.P.M. (2006). Applying the diagnostic intervention model for fostering harmonious interactions between deaf-blind children and their educators: A case study. Journal of Visual Impairment & Blindness, Volume 100(2), pp. 91 - 105
Jeffree, D., & McConkey, R. (1976). Let me speak. London: Human Horizons Series: Souvenir Press
Jellison, J.A. (1979). The music therapist in the educational setting: Developing and implementing curriculum for the handicapped. Journal of Music Therapy, Volume 16(3), pp. 126 - 137
Jenkins, J.R., Fewell, R., & Harris, S.R. (1983). Comparison of sensory integrative therapy and motor programming. American Journal
of Mental Deficiency, Volume 88, pp. 221 - 224
Jenkins, R., Rose, J., & Lovell, C. (1995). Psychological well-being of staff working with people who have challenging behaviour. Journal of Intellectual Disability Research, Volume 41, pp. 502 - 511
Jenson, C.C., Watson, L.S., DeWulf, M., Johnson, S.P., Davis, N.S., & Sottolano, D.C. (1992). Normalization of mealtime for persons with developmental disabilities: Implementation by professional and direct-care staff. Behavioral Residential Treatment, Volume 7, pp. 355 - 371
Jobling, A. (2001). Beyond sex and cooking: Health education for individuals with intellectual disability. Mental Retardation, Volume 39(4), pp. 310 - 321
Jobling, A., Virji-Babul, N., & Nichols, D. (2006). Children with Down Syndrome: Discovering the Joy of Movement. Journal of Physical Education, Recreation and Dance. Volume 77(6), pp. 34 - 38
Jockers, D. (2012). Is your brain getting enough of this nutrient? Natural News.com
Johnson, C.R., Handen, B.L., Zimmer, M., Sacco, K., & Turner, K. (2011). Effects of gluten free/casein free diet in young children with autism: a pilot study. Journal of Developmental and Physical Disabilities, Volume 23(3), pp. 213 - 225
Johnson, C.R., Turner, K., Stewart, P.A., Schmidt, B., Shui, A., Macklin, E., Reynolds, A., James, J., Johnson, S.L., Courtney, P.M., & Hyman, S.L. (2014). Relationships between feeding problems, behavioral characteristics and nutritional quality in children with ASD. Journal of Autism and Developmental Disorders, Volume 44(9), pp. 2175 - 2184
Johnson, H., Douglas, J., Bigby, C., & Iacono, T. (2012). Social Interaction with Adults with Severe Intellectual Disability: Having Fun and Hanging Out. Journal of Applied Research in Intellectual Disabilities, Volume 25(4), pp. 329 - 341
Johnson, R.K., Appel, L., Brands, M., Howard, B., Lefevre, M., Lustig, R., Sacks, F., Steffen, L., & Wyllie-Rosett, J. (2009). Dietary sugars intake and cardiovascular health: a scientific statement from the American Heart Association. Circulation, Volume 120(11), pp. 1011 - 1120
Johnson, W.L., & Day, R.M. (1992). The incidence and prevalence of self-injurious behavior. In J.K. Luiselli, J.L. Matson, & N.N. Singh (eds.), Self-Injurious Behavior: Analysis, Assessment and Treatment, pp. 21 -58. New York: Springer-verlag
Jones, A.P. (2016). String switch sessions. TalkSense Website (this webpage)
Jones, C., & Hastings, R.P. (2003). Staff reactions to self-injurious behaviours in learning disability services: Attributions, emotional responses and helping. British Journal of Clinical Psychology, Volume 42(2), pp. 189 – 203
Jones, E., Perry, J., Lowe, K., Felce, D., Toogood, S., Dunstan, F., Allen, D., & Pagler, J. (1999). Opportunity and the promotion of activity among adults with severe intellectual disability living in community residences: the impact of training staff in active support. Journal of Intellectual Disability Research, Volume 43(3), pp. 164 - 178
Jones, E., Perry, J., Lowe, K., Allen, D., Toogood, S., & Felce, D. (2009). Active Support: A handbook for supporting people with
learning disabilities to lead full lives. Welsh Centre for Learning Disabilities Applied Research Unit. University of Wales, Cardiff
Jones, F., Pring, T., & Grove, N. (2002). Developing communication in adults with profound and multiple learning difficulties using objects of reference. International Journal of Language and Communication Disorders, Volume 37(2), pp. 173 - 184
Jones, M.C., Walley, R.M., Leech, A., Paterson, M., Common, S., & Metcalf, C. (2007). Behavioral and psychosocial outcomes of a 16-week rebound therapy-based exercise program for people with profound intellectual disabilities. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(2), pp. 111 – 119
Jones, O., O’Neil, N., Pavlicevic, M., Powell, H., & Sampathianaki, E. (2014). Making music, making friends: Long-term music therapy with young adults with severe learning disabilities. Journal of Intellectual Disabilities, Volume 18(1), pp. 5 - 19
Jones, P. (2004). 'They are not like us and neither should they be': issues of teacher identity for teachers of pupils with profound and multiple learning difficulties. Disability and Society, Volume 19(2), pp. 159 - 169.
Jones, P. (2005). Teachers' views of their pupils with profound and multiple learning difficulties. European Journal of Special Needs Education, Volume 20(4), pp. 375 - 385
Jones, R. & Williams, H. (1998). Reducing Stereotyped Behaviour: an experimental analysis of Intensive Interaction, International Journal of Practical Approaches to Disability, Volume 22 (2/3), pp. 21 - 25
Jones, R.S.P., & Eayrs, C.B. (1993). Challenging Behaviour and Intellectual Disability: A Psychological Perspective. BILD
Jones, S., Cooper, S.A., Smiley, E., Allan, L., Williamson, A., & Morrison, J. (2008). Prevalence of, and factors associated with, problem behaviors in adults with intellectual disabilities. The Journal of Nervous and Mental Disease. Volume 196, pp. 678 – 686
Joseph, D. (1986). The morning. Communication Outlook. Volume 8(2), pp. 8
Kahn, J.V. (1978). Applications of the Piagetian literature to severely and profoundly retarded persons. Mental Retardation, Volume 17, pp. 273 - 280
Kahng, S., Boscoe, J.H., & Byrne, S. (2003). The use of an escape contingency and a token economy to increase food acceptance. Journal of Applied Behavior Analysis, Volume 36(3), pp. 349 - 353
Kapell, D., Nightingale, B., Rodriguez, A., Lee, J.H., Zigman, W.B., & Schupf, N. (1998). Prevalence of chronic medical conditions in adults with mental retardation: Comparison with the general population. Mental Retardation, Volume 36(4), pp. 269 - 279
Kaplan, H., Clopton, M., Kaplan, M., Messbauer, L., & McPherson, K. (2006). Snoezelen multi-sensory environments: Task engagement and generalization. Research in Developmental Disabilities, Volume 27(4), pp. 443 - 455
Karkou, V., & Sanderson, P. (1997). Dance Movement Therapy Approaches and Particular References to Children with Special Needs, in E. Antilla (ed.) The Seventh Conference of Dance and the Child International (daCI): The Call of Forests and Lakes. Proceedings, pp. 159 – 166. Kuopio, Finland: Dance and the Child International.
Karlan, G.R. (1980). The effects of preference for objects and repeated measure upon the assessed level of object permanence in severely handicapped students. Journal of the Association for the Severely Handicapped, Volume 5, pp. 174 - 193
Kastner, T., Walsh, K.K., & Fraser, M. (2001). Undiagnosed medical conditions and medication side effects presenting as behavioral/psychiatric problems in people with mental retardation. Mental Health Aspects of Developmental Disabilities. Volume 4, pp. 101 – 107
Katcher, A.H. (1977). Physiologic and behavioural responses to companion animals. Psychosomatic Medicine. Volume 39(3), pp.188 - 192
Kaufman, J.C., & Sternberg, R.J. (Eds.). (2010). The Cambridge handbook of creativity. Cambridge University Press.
Kaufman, J.C. (2016). Creativity 101. Springer Publishing
Kearney, C.A., & McKnight, T.J. (1997). Preference, choice and persons with disabilities: a synopsis of assessments, interventions and future directions. Clinical Psychology Review, Volume 17, pp. 217 – 238
Kearney, C.A., Bergan, K.P., & McKnight, T.J. (1998). Choice availability and persons with mental retardation: A longitudinal and regression analysis. Journal of Developmental and Physical Disabilities, Volume 10(3), pp. 291 - 305
Kellett, M. (2000). Sam’s story: evaluating Intensive interaction in terms of its effect on the social and communicative ability of a young child with severe learning difficulties, Support for Learning, Volume 15 (4), pp.165 - 171
Kellett, M. (2001). Implementing Intensive Interaction: an evaluation of the efficacy of Intensive Interaction in promoting sociability and communication in young children who have severe learning difficulties and of factors affecting its implementation in community schools. Ph.D Thesis, Oxford Brookes University.
Kellet, M., & Nind, M. (2002). Responding to individuals with severe learning difficulties and stereotyped behaviour. European Journal of
Special Needs Education, Volume 17(3),pp. 265 – 282
Kellett, M. (2003). Jacob’s Journey: developing sociability and communication in a young boy with severe and complex learning difficulties using the Intensive interaction teaching approach, Journal of Research in Special Educational Needs, March.
Kellet, M., & Nind, M. (2003). Implementing Intensive Interaction in Schools. London: David Fulton Publishers.
Kellett M. (2004). Intensive Interaction in the inclusive classroom: using interactive pedagogy to connect with students who are hardest to reach, Westminster Studies in Education, Volume 27, pp.175 – 188
Kellett, M. (2005). Catherine’s Legacy: social communication development for individuals with profound learning difficulties and fragile life expectancies, British Journal of Special Education, Volume 32 (3), pp.116 - 121
Kelley, M.F., Sexton, D., Burdg, N.B., & Haynes, M.D. (1988). Assessment of Self-Recognition in Young Children with Handicaps. Assessment for Effective Intervention. Volume 13(2-4), pp. 86 - 97
Kelly, L.E., Rimmer, J.H., & Ness, R.A. (1986). Obesity levels in institutionalized mentally retarded adults. Adapted Physical Activity Quarterly, Volume 3(2), pp. 167 - 176
Kempermann, G., & Gage, F.H. (1999). New nerve cells for the adult brain. Scientific American, Volume 280(5), pp. 48 - 53
Kempton, M.J., Ettinger, U., Foster, R., Williams, S.C., Calvert, G.A., Hampshire, A., Zelaya, F.O., O’Gorman, R.L., McMorris, T., Owen, A.M., & Smith, M.S. (2011). Dehydration affects brain structure and function in healthy adolescents. Human Brain Mapping. Volume 32. pp. 71 - 79
Kennedy, A. (2001). Intensive Interaction, Learning Disability Practice, Volume 4(3), pp.14 - 15
Kennedy, C.H., & Haring, T.G. (1993). Teaching Choice Making During Social Interactions to Students with Profound Multiple Disabilities. Journal of Applied Behavior Analysis, Volume 26(1), pp. 63 - 76
Kennedy, C.H., & Itkonen, T. (1993). Effects of setting events on the problem behavior of students with severe disabilities. Journal of Applied Behavior Analysis, Volume 26, pp. 321 - 327
Kennedy, C.H., & Meyer, K.A. (1996). Sleep deprivation, allergy symptoms, and negatively reinforced problem behaviour. Journal of Applied Behavior Analysis. Volume 29, pp. 133 – 135
Kennedy, H. (2011). What is video interactive guidance (V.I.G.). In H. Kennedy, M. Landor & L. Todd (Eds), Video Interactive Guidance: A
Relationship-Based Intervention to Promote Attunement, Empathy and Wellbeing. London: Jessica Kingsley.
Kennedy, H., Landor, M., & Todd. L. (2011). Video Interactive Guidance: A Relationship-Based Intervention to Promote Attunement, Empathy and Wellbeing. London: Jessica Kingsley.
Kennedy, M., McCombie, L., Dawes, P., McConnell, K.N., & Dunnigan, M.G. (1997). Nutritional support for patients with intellectual disability and nutrition/dysphagia disorders in community care. Journal of Intellectual Disability Research, Volume 41(5), pp. 430 - 436
Kenny, C.B. (1982). The Mythic Artery: The Magic of Music Therapy, Atascadero, California: Ridgeview Publishing Company.
Kerdegari, H., Kim, Y., & Prescott, T.J. (2016). Head-mounted sensory augmentation device: designing a tactile language, IEEE transactions on haptics, Volume 9 (3), pp. 376 - 386
Kern, L., Koegel, R.L., Dyer, K., Blew, P.A., & Fenton, L.R. (1982). The effects of physical exercise on self stimulation and appropriate responding in autistic children. Journal of Autism and Developmental Disorders, Volume 12, pp. 399 - 419
Kern, P., Wolery, M., & Aldridge, D. (2007). Use of songs to promote independence in morning greeting routines for young children with autism. Journal of Autism & Developmental Disorders, Volume 37(7), pp. 1264 - 1271
Kiernan, C. (1991). Professional ethics: Behaviour analysis and normalisation. In B. Remington (Ed.), The Challenge of Severe Mental Handicap: A Behaviour Analytic Approach. John Wiley and Sons, Chichester, pp. 369 - 392
Kiernan, C. (1993). Future directions. In S. Jones & C. Eayres (Eds), Challenging Behaviour and Intellectual Disability: a psychological perspective. Kidderminster: BILD.
Kiernan, C., & Qureshi, H. (1993). Challenging behaviour. In C. Kiernan (Ed.), Research to Practice? Implications of Research on the Challenging Behaviour of People with Learning Disabilities. pp. 53 - 87. Kidderminster: British Institute of Learning Disabilities Publications.
Kiernan, C., & Kiernan, D. (1994). Challenging behaviour in schools for pupils with severe learning difficulties. Mental Handicap Research, Volume 7, pp. 117 - 201
Kiernan, C., Reeves, D., & Alborz, A. (1995). The use of anti-psychotic drugs with adults with learning disabilities and challenging behaviour. Journal of Intellectual Disability Research, Volume 39, pp. 263 - 274
Kiernan, C., & Alborz, A. (1996). Persistence and change in challenging and problem behaviours of young adults with intellectual disability living in the family home. Journal of Applied Research in Intellectual Disabilities, Volume 3, pp. 181 - 193
Kimball, J.G. (1988). The emphasis is on integration, not sensory. American Journal of Mental Retardation, Volume 92, pp. 423 - 424
King, B. (2007). Psychopharmacology in intellectual disabilities. In Bouras, N. & Holt, G. (Eds.) Psychiatric and Behavioural Disorders in Intellectual and Developmental Disabilities. Cambridge: Cambridge University Press.
King, G.A., Shultz, I.Z., Steel, K., Gilpin, M., & Cathers, T. (1993). Self-evaluation and self-concept of adolescents with physical disabilities, American Journal of Occupational Therapy, Volume 47(2), pp. 132 - 140
Kingsley, J. (2009). First steps in intervention with your child with autism: Framework for communication. Philadelphia, PA. Jessica Kingsley
Kinnealey M. (1973). Aversive and non-aversive responses to sensory stimulation in mentally retarded children. American Journal of Occupational Therapy, Volume 27, pp. 464 – 471
Kinnealey, M. (1976). Aversive and non-aversive Responses to Sensory Stimulation in Mentally Retarded Children, In A.Price, E. Gilfoyle & C, Myers (Eds.) Research in Sensory Integrative Development (pp. 33 - 40). Rockville, MD: American Occupational Therapy Association
Kinnealey M., Oliver B., & Wilbarger P. (1995). A phenomenological study of sensory defensiveness in adults. American Journal of Occupational Therapy, Volume 49, pp. 444 – 451
Kinnealey, M., & Fuiek, M. (1999). The relationship between sensory defensiveness, anxiety, depression, and perception of pain in adults.
Occupational Therapy International, Volume 6, pp. 195 - 206
Kishi, G., Teelucksingh, B., Zollers, N., Park-Lee, S., & Meyer, L. (1988). Daily decision-making in community residences: A social comparison of adults with and without mental retardation. American Journal on Mental Retardation, Volume 92, pp. 430 - 435
Kitch, R. (1995). Creating success in the land of Oz and earthquakes. 3rd Annual Pittsburgh Employment Conference Proceedings. pp. 3 - 8
Kivitie-Kallio, S., Autti, T., Salonen, O., & Norio, R. (1998). MRI of the brain in the Cohen syndrome: a relatively large corpus callosum in patients with mental retardation and microcephaly. Neuropediatrics, Volume 29(06), pp. 298 - 301
Kjos, B.O., Umansky, R., & Barkovich, A.J. (1990). Brain MR imaging in children with developmental retardation of unknown cause: results in 76 cases. American Journal of Neuroradiology, Volume 11(5), pp. 1035 - 1040
Kleim, J.A. & Jones, T.A. (2008). Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. Supplement: Journal of Speech, Language, and Hearing Research, Volume 51(1), S225 - S239
Knight, C. (1991). Developing Communication through Interaction, in Watson, J. (ed) Innovatory Practice and Severe Learning Difficulties. Edinburgh: Moray House.
Knight, C. (1992). Speech therapy on the run: Creating opportunities for effective communication. Eye Contact. Volume 3. Royal National Institute for the Blind
Knill, C. (1983) Body awareness, communication and development: a programme employing music with the profoundly handicapped. International Journal of Rehabilitation Research, Volume 6(4), pp. 489 - 492
Kobe, F.H., Mulick, J.A., Rash, T.A., & Martin, J. (1994). Non-ambulatory persons with profound mental retardation: physical, developmental, and behavioural characteristics. Research in Developmental Disabilities. Volume 15, pp. 413 – 423
Koller, H., Richardson, S.A., Katz, M., & McLaren, J. (1982). Behaviour disturbance in childhood and the early adults years in populations who were and were not mentally retarded. Journal of Preventive Psychiatry, Volume 1, pp. 453 - 468
Konarski, E.A., Sutton, K., & Huffman, A. (1997). Personal characteristics asociated with episodes of injury in a residential facilty. American Journal of Mental Retardation. Volume 102, pp. 37 - 44
Konrad, M., Fowler, C.H., Walker, A.R., Test, D.W., & Wood, W.M. (2007). Effects of self-determination interventions on the academic skills of students with learning disabilities. Learning Disabilities Quarterly, Volume 30, pp. 89 – 113
Koomar, J., Kranowitz, C., Szklut, S., & Balzer-Martin, L. (2001). Answers to Questions Teachers Ask About Sensory Integration: Forms, Checklists, and Practical Tools. Future Horizons
Koski, K., Martikainen, K., Burakoff, K., & Launonen, K. (2010). Staff members' understandings about communication with individuals who have multiple learning disabilities: A case of Finnish OIVA communication training. Journal of Intellectual and Developmental Disability, Volume 35(4), pp. 279 - 289
Koski, K. (2014). Indirect Speech and Language Therapy for Individuals with Profound and Multiple Learning Disabilities: An Ecological Perspective. The Finnish Association on Intellectual and Developmental Disabilities
Koziol, L.F. & Ely Budding, D., & Chidekel, D. (2011). Sensory Integration, Sensory Processing, and Sensory Modulation Disorders: Putative Functional Neuroanatomic Underpinnings. Cerebellum, Volume 10. pp. 770 – 792
Kozma, A., Mansell, J., & Beadle-Brown, J. (2009). Outcomes in different residential settings for people with intellectual disability: a systematic review. American Journal on Intellectual and Developmental Disabilities, Volume 114(3), pp. 193 - 222
Kranowitz, C.S. (1998). The Out-of-Sync Child: Recognizing and Coping with Sensory Integration Dysfunction. New York: Perigee
Kranowitz, C.S., Szklut, S., Balzer-Martin, L., Haber, E., & Sava, D.I. (2002). Answers to questions teachers ask about sensory integration. Las Vegas, NM: Sensory Resources.
Kranowitz, C.S. (2003). The out-of-sync child has fun. New York: Berkley Publishing.
Kranowitz, C.S. (2005). The Out of Sync Child: Recognizing and Coping with Sensory Processing Disorder. New York: Perigee.
Krech, D., Rosenzweig, M.R., & Bennett, E.L. (1960). Effects of environmental complexity and training on brain chemistry. Journal of Comparative Physiological Psychology. Volume 53. pp. 509 - 519
Kršková, L., Talarovièová, A., & Olexová, L. (2010). Guinea pigs-The “small great” therapist for autistic children, or: Do guinea pigs have positive effects on autistic child social behavior? Society & Animals, Volume 18, pp. 139 – 151
Kuder, S.J., & Bryen, D.N. (1993). Conversational topics of staff members and institutionalized individuals with mental retardation. Mental Retardation, volume 31(3), pp. 148 - 153
Kuder, S.J. (2003). Teaching students with language and communication difficulties. Boston, MA: Allyn and Bacon
Kuhn, H.G., Palmer, T.D., & Fuchs, E. (2001). Adult neurogenesis: a compensatory mechanism for neuronal damage. European Archives of Psychiatry and Clinical Neuroscience, Volume 251(4), pp. 152 - 158
Kurtz, P.F., Boetler, E.W., Jarmolowicz, D.P., Chin, M.D., & Hagopian, L.P. (2011). An analysis of functional communication training as an empirically supported treatment for problem behaviors displayed by individuals with intellectual disabilities. Research in Developmental Disabilities, Volume 32(6), pp. 2935 - 2942
Kyselo, M. (2014). The body social: an enactive approach to the self. Frontiers in Psychology, Volume 5, Article 986. pp. 1 - 16
Lacey, P. (1996). The inner life of children with profound and multiple learning difficulties. In - Varma, V. (ed), The Inner Life of Children with Special Needs. London: Whurr.
Lacey, P. (1998). Meeting complex needs through multidisciplinary teamwork. In P. Lacey & C. Ouvry (Eds), People with Profound and Multiple Learning Disabilities: A Collaborative Approach to Meeting Complex Needs. London: David Fulton
Lacey, P., & Ouvry, C. (1998). People with Profound & Multiple Learning Disabilities: Collaborative Approach to Meeting Complex Needs. David Fulton
Lacey, P., & Porter, J. (1998). Enabling Teachers: in-service education in learning difficulties and challenging behaviour, Journal of In-Service Education, Volume 24(3), pp. 475 - 491
Lacey, P. (2001). Music. In - Carpenter, B., Ashdown, R., & Bovair, K. (eds), Enabling Access: Effective Teaching and Learning for Pupils with Learning Difficulties. London: David Fulton. 2nd Edition
Lacey, P. (2001b). The role of learning support assistants in the inclusive learning of pupils with severe and profound learning difficulties. Educational Review, Volume 53(2), pp. 157 - 167
Lacey, P. (2007). Start Where The Learner Is: Coaching For a Better Quality Of Life. PMLD Link, Volume 19(2), Issue 57, pp. 10 - 16
Lacey, P., Layton, L., Miller, C., Goldbart, J., & Lawson, H. (2007) ‘Literacy for children with severe learning difficulties: exploring conventional and inclusive literacy. Journal of Research in Special Educational Needs. Volume 7(3), pp. 149 - 160
Lacey, P. (2009). Developing The Thinking of Learners With PMLD. PMLD Link. Volume 21(2), Issue 63, pp. 15 - 19
Lacey, P. (2010). SMART and SCRUFFY Targets, SLD Experience, Volume 57, pp. 16 - 21
Lacey, P. (2011). Listening to challenging behaviour. PMLD Link. Volume 23(1), Issue 68, pp. 7 - 9
Lacey, P. (2015). Developing The Thinking of Learners With PMLD. PMLD Link. Volume 27(2), Issue 81, pp. 43 - 47
Lacey, P. , Ashdown, R., Jones, P., Lawson, H., & Pipe, M. (Eds) (2015). The Routledge Companion to Severe, Profound and Multiple Learning Difficulties. Routledge
Lachapelle, Y., Wehmeyer, M.L., Haelewyck, M.C., Courbois, Y., Keith, K.D., Schalock, R., & Walsh, P.N. (2005). The relationship
between quality of life and self-determination: An international study. Journal of Intellectual Disability Research, Volume 49, pp. 740 – 744.
LaFay L. (1987). That smarts! Accident leaves man with unforgettable gift. Virgina Pilot. Volume 17, pp. 31 - 33
Lahtinen, U., Rintala, P., & Malin, A. (2007). Physical performance of individuals with intellectual disability: A 30-year follow-up. Adapted Physical Activity Quarterly, Volume 24, pp. 125 – 143
Lakin, K.C., Hill, B.K., Hauber, F.A., Bruininks, R.H. & Heal, L.W. (1983). New admissions and re-admissions to a national sample of public residental facilties. American Journal of Mental Deficiency, Volume 88, pp. 13 - 20
Lakin, K.C., & Stancliffe, R.J. (2007). Residential supports for persons with intellectual and developmental disabilities. Developmental Disabilities Research Reviews, Volume 13(2), pp. 151 - 159
Lakin, K.C., Doljanac, R., Byun, S.Y., Stancliffe, R.J., Taub, S., & Chiri, G. (2008). Factors associated with expenditures for Medicaid home and community based services (HCBS) and intermediate care facilities for persons with mental retardation (ICF/MR) services for persons with intellectual and developmental disabilities. Intellectual and Developmental Disabilities, Volume 46(3), pp. 200 - 214
Lakin, K.C., Doljanac, R., Byun, S.Y., Stancliffe, R.J., Taub, S., & Chiri, G. (2008b). Choice-making among Medicaid HCBS and ICF/MR recipients in six states. American Journal on Mental Retardation, Volume 113(5), pp. 325 - 342
Lalli, J.S., Browder, D.M., Mace, F.C., & Brown, D.K. (1993). Teacher use of descriptive analysis data to implement interventions to decrease students' problem behaviors. Journal of Applied Behavior Analysis, 26, pp. 227 - 238
Lambe, L. (1990). Leisure Resource training Pack for People with Profound and Multiple Disabilities. Mencap: London
Lambe, L., & Hogg, J. (2000). Creative Arts and People with Profound and Multiple Learning Disabilities: Education, Therapy and Leisure. Pavilion Publishing (Brighton) Ltd
Lambrechts, G. Kuppens, S. & Maes, B. (2009). Staff variables associated with the challenging behaviour of clients with severe or profound intellectual disabilities. Journal of Intellectual Disability Research, Volume 53(7), pp. 620 – 632
Lamond, I.R. (2006). Two steps forward and One step back (Being a reflection on the impact of incorporating dance into the curriculum of Profound and Multiple Learning Difficulties pupils at a Special School). Unpublished Master's Thesis, Leeds Beckett University
Lamonde, M. (2017). Sensory Processing: Techniques, Tactics & SPD Games To Help Your Child With Sensory Processing Disorder. Create Space Independent Publishing Platform
Lancioni, G.E., O’Reilly M.F., & Emerson E. (1996). A review of choice research with people with severe and profound developmental disabilities. Research in Developmental Disabilities, Volume 17(5), pp. 391 – 411
Lancioni, G.E., & O'Reilly, M.F. (1998). A review of research on physical exercise with people with severe and profound developmental disabilities. Research in Developmental Disabilities, Volume 19(6), pp. 477 - 492
Lancioni, G.E., O’Reilly, M.F., Campodonico, F., & Mantini, M. (1998a). Task variation versus task repetition for people with profound developmental disabilities: An assessment of preferences. Research in Developmental Disabilities, Volume 19, 189 – 199
Lancioni, G.E., O’Reilly, M.F., Campodonico, F., & Mantini, M. (1998b). Mobility versus sedentariness in task arrangements for people with multiple disabilities: An assessment of preferences. Research in Developmental Disabilities, Volume 19(6), pp. 465 – 475
Lancioni, G.E., O’Reilly, M.F., Van Dijk, J., & Klaase, M. (1998). An environmental enrichment program to promote adaptive responding in two children with multiple disabilities. Scandinavian Journal of Behaviour Therapy, Volume 27(3), pp. 130 - 134
Lancioni, G.E., O'Reilly, M.F., & Basili, G. (1999). Review of strategies for treating sleep problems in persons with severe or profound mental retardation or multiple handicaps. American Journal on Mental Retardation, Volume 104(2), pp.170 - 186
Lancioni, G.E., O’Reilly, M.F., & Mantini, M. (1999). Activity arrangements with or without mobility and performance of persons with multiple
disabilities over long sessions. Irish Journal of Psychology, Volume 20(2), pp. 124 - 135
Lancioni, G.E., Dijkstra, A.W., & O’Reilly, M.F. (2000). Frequent versus nonfrequent verbal prompts delivered unobtrusively: Their impact on the task performance of adults with intellectual disability. Education and Training in Mental Retardation and Developmental Disabilities, Volume 35(4), pp. 428 - 433
Lancioni, G.E., Cuvo, A.J., & O'Reilly, M.F. (2002). Snoezelen: An overview of research with people with disabilities and dementia. Disability and Rehabilitation: An International, Multidisciplinary Journal, Volume 24(4), pp. 175 - 184
Lancioni, G.E., Abels, J., Wilms, E.H., Singh, N.N., O’Reilly, M.F., & Groeneweg, J. (2003). Microswitch responding and awareness of contingency in persons with profound multiple disabilities. Perceptual and Motor Skills, Volume 96(3), pp. 835 – 838
Lancioni, G.E., Singh, N.N., O'Reilly, M.F., Oliva,D., & Basili, G.(2005). An overview of research on increasing indices of happiness of people with severe/profound intellectual and multiple disabilities,” Disability and Rehabilitation, Volume 27(3), pp. 83 – 93
Lancioni, G.E., Singh, N.N., O’Reilly, M.F., Oliva, D., & Severini, L. (2005). Assessing a micro switch-based stimulation procedure for eye-blinking responses in a young woman with profound multiple disabilities. Perceptual and Motor Skills, Volume 101(1), pp. 212 - 216
Lancioni, G.E., O'Reilly, M.F., Singh, N.N., Sigafoos, J., Oliva, D., Campodonico, F., & Piazzolla, G. (2006). Promoting fluency of performance during morning dressing by two persons with multiple disabilities. Perceptual and Motor Skills, Volume 103, pp. 771 - 777
Lancioni, G.E., O'Reilly, M.F., Singh, N.N., Sigafoos, J., Oliva, D., Campodonico, F., & Groeneweg, J. (2007). Helping Three Persons with Multiple Disabilities Acquire Independent Dressing Through Assistive Technology. Journal of Visual Impairment & Blindness, Volume 101(12), pp. 768 - 773
Lancioni, G.E., Singh, N.N., O'Reilly, M.F., Sigafoos, J., Didden, R., Oliva, D., et al. (2007). Effects of microswitch-based programs on indices of happiness of students with multiple disabilities: A new research evaluation. American Journal on Mental Retardation, Volume 112(3), pp. 167 - 176
Lancioni, G.E., Singh, N.N., O’Reilly, M.F., Sigafoos, J., D’Amico, F., Buonocunto, F., Navarro, J., Lanzilotti, C., Fiore, P., Megna, M., & Damiani, S. (2015). Assistive technology to help persons in a minimally conscious state develop responding and stimulation control: Performance assessment and social rating. NeuroRehabilitation, Volume 37(3), pp. 393 - 403
Land, G., Errington-Povalac, E., & Paul, S. (2001). The effects of therapeutic horseback riding on sitting posture in individuals with disabilities. Occupational Therapy in Care, Volume 14(1), pp. 1 - 12
Lange, K.W., Hauser, J., & Reissmann, A. (2015). Gluten-free and casein-free diets in the therapy of autism. Current Opinion in Clinical Nutrition & Metabolic Care, Volume 18(6), 572 - 575
Langer, E.J., & Rodin, J. (1976). The Effect of Choice and Enhanced Personal Responsibility for the Aged: A Field Experiment in an
Institutional Setting. Journal of Personality and Social Psychology, Volume 34, pp.191 – 98
Langley, B., & Dubose, R.F. (1976). Functional Vision Screening for Severely Handicapped Children. Journal of Visual Impairment & Blindness. Volume 70(8), pp. 346 - 350
Larkey, S. (2007). Practical Sensory Programmes for Students with Autism Spectrum Disorder and Other Special Needs. London: Jessica Kingsley Publishers.
Larson, K.A. (1982). The Sensory History of developmentally Delayed Children With and Without Tactile Defensiveness. American Journal of Occupational Therapy, Volume 36, pp. 590 - 596
LaVigna, G.W., & Donellan, A.M. (1986). Alternatives to Punishment: Solving Behavior Problems with Non-Aversive Strategies. New York: Irvington
Lawes, C., & Woodcock, J. (2000). Music therapy and people with severe learning disabilities who exhibit self injurious behaviour. In - Wigram T, Saperston B, & West R (Eds), The art and science of music therapy. A handbook. Harwood Academic Publishers, Netherlands
Lawrence, M., & Wigram, T. (2005). Music therapy as a tool for assessing hand use and communicativeness in children with Rett Syndrome. Brain & Development, Volume 27, S95 - S96
L’Ecuyer, R. (1978). Le concept de soi [The self-concept], Paris: Presses de l’Universite de France.
Leaning, B., & Watson T. (2006). From the inside looking out – an Intensive Interaction group for people with profound and multiple learning disabilities, British Journal of Learning Disabilities, Volume 34, pp.103 - 109
Leary, M.R. (2004). The curse of the self: Self-awareness, egotism, and the quality of human life. Oxford University Press.
Lecavalier, L. (2006). Behavioral and emotional problems in young people with pervasive developmental disorders: Relative prevalence,
effects of subject characteristics, and empirical classification. Journal of Autism and Developmental Disorders, Volume 36(8), pp. 1101 – 1114
Lee, J., & McFerran, K. (2012). The improvement of non-verbal communication skills of five females with profound and multiple disabilities using song-choices in music therapy. Voices: A World Forum for Music Therapy, Volume 12(3), Retrieved from https://normt.uib.no/index.php/voices/article/viewArticle/644.
Lee, S.H., Wehmeyer, M.L., Soukup, J.H., & Palmer, S.B. (2010). Impact of curriculum modifications on access to the general education curriculum for students with disabilities. Exceptional Children, Volume 76, pp. 213 – 233
Lee, V., & Das Gupta, P. (Eds.)(1995). Children’s cognitive and language development. The Open University. Oxford: Blackwell Publishers
ISBN 0-631-19428-2
Legault, J.R. (1992) A study of the relationship of community living situation to independence and satisfaction on the lives of mentally retarded adults. Journal of Intellectual Disability Research. Volume 36, pp. 129 - 141
Lehtonen, K. (1993). Music Therapy in Finland. In Maranto, C.D., (Ed.), Music Therapy: International Perspectives, Pipersville, Pennsylvania: Jeffrey Books.
Lemke, H. (1974). Self-abusive behavior in the mentally retarded. American Journal of Occupational Therapy, Volume 28, pp. 94 – 98
Lenggenhager, B., Tadi, T., Metzinger, T., & Blanke, O. (2007). Video ergo sum: Manipulating bodily self-consciousness. Science, Volume 317, pp. 1096 – 1099
Lerer, R.J. (1981). An open letter to an occupational therapist. Journal of Learning Disability, Volume 14, pp. 3 - 4
Lerman, D.C., & Iwata, B.A. (1993). Descriptive and experimental analyses of variables maintaining self-injurious behavior. Journal of Applied Behavior Analysis, Volume 26, pp. 293 - 319
Levinger, B. (1992). Nutrition, health, and learning. School nutrition and health network monograph series, Number 1
Lewis, A., & Norwich, B. (2000). Mapping a pedagogy for special educational needs. Exeter : School of Education, University of Exeter.
Lewis, A., & Norwich, B. (2001). A critical review of systematic evidence concerning distinctive pedagogies for pupils with difficulties in learning. Journal of Research in Special Educational Needs, Volume 1(1), pp. 1 - 13
Lewis, A. ( 2002 June). The development of children’s ideas about others’ difficulties in learning, British Journal of Special Education, Volume 29(2), pp. 59 - 65
Lewis, A. ( 2002 August). Accessing, through research interviews, the views of children with difficulties in learning. Support for Learning, Volume 17(3), pp. 111 - 116
Lewis, A., & Norwich, B. (eds)(2005). Special Teaching for Special Children. Berkshire: Open University Press.
Lieberman, H.R. (2007). Hydration and cognition: a critical review and recommendations for future research. Journal of the American
College of Nutrition, Volume 26(5), Supplement, pp. 555 - 561
Lieberman, H.R. (2012). Methods for assessing the effects of dehydration on cognitive function. Nutrition Reviews. Volume 70(2), Supplement. pp.143 - 146
Light, J., McNaughton, D., & Parnes, P. (1986). A protocol for the assessment of the communicative interaction skills of nonspeaking severely handicapped adults and their facilitators. Toronto: Hugh Macmillan Medical Centre
Linderman, T.M., & Stewart, K.B. (1999). Sensory integrative based occupational therapy and functional outcomes in young children with pervasive developmental disorders: A single subject study. American Journal of Occupational Therapy, Volume 53, pp. 207 – 213
Lindsay, W.R., Pitcaithly, D., Geelen, N., Buntin, L., Broxholme, S., & Ashby, M. (1997). A comparison of the effects of four therapy procedures on concentration and responsiveness in people with profound learning disabilities. Journal of Intellectual Disability Research, Volume 41(3), pp. 201 - 207
Lindsay, W.R., Black, E., Broxholme, S., Pitcaithly, D., & Hornsby, N. (2001). Effects of four therapy procedures on communication in people with profound intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 14(2), pp. 110 - 119
Lindsey, J.P. (1996). The right to choose: Informed consent in the lives of adults with mental retardation and developmental disabilities. Education and Training in Mental Retardation and Developmental Disabilities. Volume 31, pp. 171 – 176
Little, T.D., Hawley, P.H., Henrich, C.C., & Marsland, K. (2002). Three views of the agentic self: A developmental synthesis. In E.
L.Deci & R.M.Ryan(Eds.), Handbook of self-determination research (pp. 389 – 404). Rochester, NY: University of Rochester Press.
Little, T.D., Snyder, C.R., & Wehmeyer, M.L. (2006). The agentic self: On the nature and origins of personal agency across the life span. In D. K. Mroczek & T. D. Little (Eds.), Handbook of personality development (pp. 61 – 80). Mahwah, NJ: Lawrence Erlbaum Associates.
Liutsko, L.N. (2013). Proprioception as a basis for individual differences. Psychology in Russia: State of the Art. Volume 6(3), pp. 107 -119
Lloyd, P. (2007). Let's All Listen: Songs for Group Work in Settings that Include Students with Learning Difficulties and Autism. London: Jessica Kingsley.
Logan, K.R., Jacobs, H.A., Gast, D.L., Murray, A.S., Daino, K. & Skala, C. (1998). The impact of typical peers on the perceived happiness of students with profound multiple disabilities. Journal of the Association for Persons with Severe Handicaps, Volume 23(4), pp. 309 – 318
Logan, K.R., & Gast, D.L. (2001). Conducting preference assessments and reinforcer testing for individuals with profound multiple disabilities: Issues and procedures. Exceptionality, Volume 9(3), pp. 123 - 134
Logan, K.R., Jacobs, H.A., Gast, D.L., Smith, P.D., Daniel, J., & Rawls, J. (2001). Preferences and reinforcers for students with profound multiple disabilities: can we identify them? Journal of Developmental and Physical Disabilities, Volume 13(2), pp. 97 - 122
Lohrmann-O'Rourke, S., & Browder, D.M. (1998). Empirically based methods to assess the preferences of individuals with severe disabilities. American Journal of Mental Retardation, Volume 103(2), pp. 146 - 161
Lohrmann-O'Rourke, S., & Yurman, B. (2001). Naturalistic assessment of and intervention for mouthing behaviors influenced by establishing operations. Journal of Positive Behavior Interventions, Volume 3(1), pp. 19 - 27
Lomas, H., & Hallas, P. (1998). It’s a mystery: Accounts of an art therapy group for people with learning disabilities. In - M. Rees (Ed.) Drawing on difference: Art Therapy with people who have learning difficulties, pp. 31–58. London: Routledge.
Longhorn, F. (1988). A Sensory Curriculum for Very Special People. Souvenir Press
Longhorn, F. (2009). Parachute play from Flo Longhorn. Information Exchange, Volume 79, pp. 9 - 10
Longley, S., & Collins, G.J. (1994). The development of a non-verbal satisfaction measure for use with people who have severe or profound learning disabilities. British Journal of Developmental Disabilities, Volume XL(79), pp. 143 - 149
Longo, M., Schüür, F., Kammers, M.P.M., Tsakiris, M., & Haggard, P. (2008). What is embodiment? A psychometric approach. Cognition, Volume 107, pp. 978 – 998
Longo, M.R., Schüür, F., Kammers, M.P., Tsakiris, M., & Haggard, P. (2009). Self awareness and the body image. Acta Psychologica,
Volume 132(2), pp. 166 – 172
Loots, G., & Malschaert, E. (1999). The use in Belgium of developmental movement according to the work of Veronica Sherborne: a developmental psychology view. European Journal of Special Needs Education, Volume 14(3), pp. 221 - 230
Lovaas, I., Freitag, G., Gold, V.J., & Kassorla, I.C. (1965). Experimental studies in childhood schitzophrenia: analysis of self-destructive behavior. Journal of Experimental Child Psychology. Volume 2, pp. 67 - 84
Lovaas, I., Newsom, C., & Hickman, C. (1987). Self-stimulatory behavior and perceptual reinforcement, Journal of Applied Behavior Analysis, Volume 20 (1), pp. 45 - 68
Lovell, D.M., Jones, R.S.P., & Ephraim, G. (1998). The effect of Intensive Interaction on the sociability of a man with severe intellectual disabilities,International Journal of Practical Approaches to Disability. Volume 22(2/3), pp. 3 - 9
Lowe, K., De Paiva, S., & Felce, D. (1993). Effects of a community-based service on adaptive and maladaptive behaviours: A longitudinal study. Journal of Intellectual Disability Research, Volume 37, pp. 3 - 22.
Lowe, K., Felce, D., & Orlowska, D. (1993). Evaluating services for people with challenging behaviour. In I. Fleming & B. Stenfert Kroese (Eds), People with Learning Disability and Severe Challenging Behaviour. Manchester: Manchester University Press.
Lowe, K. Felce, D., & Blackman, D. (1995). People with learning disabilities and challenging behaviour: The characteristics of those referred and not referred to specialist teams. Psychological Medicine, Volume 25(03), pp. 595 – 603
Lowe, K., Allen, D., Jones, E., Brophy, S., Moore, K., & James, W. (2007). Challenging behaviours: prevalence and topographies. Journal of Intellectual Disability Research, Volume 51(8), pp. 625 - 636
Lowe, K., Jones, E., Allen, D., Davies, D., James, W., Doyle, T., Andrew, J., Kaye, N., Jones, S., Brophy, S., & Moore K.(2007). Staff training in positive behaviour support: Impact on attitudes and knowledge. Journal of Applied Research in Intellectual Disabilities, Volume 20(1), pp. 30 – 40
Luijkx, J., van der Putten, A.A., & Vlaskamp, C. (2017). A valuable burden? The impact of children with profound intellectual and multiple disabilities on family life. Journal of Intellectual & Developmental Disability, pp. 1 - 6
Luiselli, J.K. (1992). Protective equipment. In J.K. Luiselli,J.L. Matson, N.N. Singh (Eds.), Self-Injurious behaviour: Analysis, assessment and Treatment. New York: Springer-Verlag
Lundqvist, L. (2013). Prevalence and risk markers of behaviour problems among adults with intellectual disabilities: A total population study in Örebro County. Sweden. Research in Developmental Disabilities, Volume 34(4), pp. 1346 – 1356
Lupien, S.J., McEwen, B.S., Gunnar, M.R., & Heim, C. (2009). Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nature Reviews Neuroscience, Volume 10, pp. 434 - 445
Lustig, R.H., Schmidt, L.A., & Brindis, C.D. (2012). The toxic truth about sugar. Nature. Volume 482. pp. 27 - 29
Lustig, R.H. (2013). Fat Chance: The Bitter Truth about Sugar. Hudson Street Press
Lustig, R.H. (2013b). Fructose: It’s 'Alcohol Without the Buzz'. Advances in Nutrition. Volume 4. pp. 226 - 235
Lyons, G. (2003). Life satisfaction for children with profound and multiple disabilities. (Doctoral dissertation). Newcastle: University of Newcastle, Faculty of Education and Arts.
Lyons, G. (2005). The Life Satisfaction Matrix: an instrument and procedure for assessing the subjective quality of life of individuals with profound multiple disabilities. Journal of Intellectual Disability Research, Volume 49(10), pp. 766 - 769
Lyons, G., & Cassebohm, M. (2012). The education of Australian school students with the most severe intellectual disabilities: where have we been and where could we go? a discussion primer, Australasian Journal of Special Education, Volume 34 (1). pp. 79 - 96
Maag, J.W., Wolchik, S.A., Rutherford, R.B., & Parks, B.T. (1986). Response covariation on self-stimulatory behaviors during sensory extinction procedures. Journal of Autism and Developmental Disorders, Volume 16(2), pp. 119 - 132
Maber-Aleksandrowicz, S., Avent,C., & Hassiotis, A. (2016). A Systematic Review of Animal-Assisted Therapy on Psychosocial Outcomes in People with Intellectual Disability. Research in Developmental Disabilities. Volume 49–50, pp. 322 – 338
Macauley, B.L., & Guiterrez, K.M. (2004). The effectiveness of hippotherapy for children with language-learning disabilities. Communication Disorders Quarterly, Volume 25(4), pp. 205 – 217
MacDonald, J. (1992). Dance? Of Course I can! Dance movement therapy for people with learning disabilities, in Payne, H. (Ed.), Dance Movement Therapy: Theory and Practice, London: Routledge, pp. 202 - 217 (First edition)
MacDonald, R., O’Donnell, P., & Davies, J. (1999). An empirical investigation into the effects of structured music workshops for individuals with intellectuals disabilities. Journal of Applied Research in Intellectual Disabilities. Volume 12, pp. 225 – 240
MacFarland, S. (1995). Teaching strategies of the van Dijk curricular approach. Journal of Visual Impairment & Blindness, Volume 89, pp. 222 - 228
Mackie, R.T., McCulloch, D.L., Saunders, K.J., Ballantyne, J., Day, R.E., Bradnam, M.S., & Dutton, G.N. (1995). Comparison of visual assessment tests in multiply handicapped children. Eye, Volume 9(1), pp. 136 - 141
MacKinnon, J.R., Noh, S., Lariviere, J., MacPhail, A., Allan, D.E., & Labiberte, D. (1995a). A study of therapeutic effects of horseback riding for children with cerebral palsy. Physical & Occupational Therapy in Pediatrics, Volume 15(1), pp. 17 - 34
MacKinnon, J.R., Noh, S., Lariviere, J., MacPhail, A., Allan, D.E., & Labiberte, D. (1995b). Therapeutic horse riding: A review of the literature. Physical & Occupational Therapy in Pediatrics, Volume 15(1), pp. 1 - 15
MacPhail, A.H.E., Edwards, J., Golding, J., Miller, K., Mosier, C., & Zwiers, T. (1998). Trunk postural reactions in children with and without cerebral palsy during therapeutic horseback riding. Pediatric Physical Therapy, Volume 10, pp.143 – 147
Madge, N. & Fassam, M. (1982): Ask the children. London: Batsford
Maes, B., Lambrechts, G., Hostyn, I., & Petry, K. (2007). Quality-enhancing interventions for people with profound intellectual and multiple disabilities: A review of the empirical research literature. Journal of Intellectual and Developmental Disability, Volume 32(3), pp. 163 – 178
Maestú, F., Arrazola, J., Fernández, A., Simos, P.G., Amo, C., Gil-Gregorio, P., Fernandez, S., Papanicolaou, A., & Ortiz, T. (2003). Do cognitive patterns of brain magnetic activity correlate with hippocampal atrophy in Alzheimer’s disease? The Journal of Neurology, Neurosurgery, and Psychiatry. Volume 74. pp. 208 – 212
Magee, W., & Bowen, C. (2008). Using music in leisure to enhance social relationships with patients with complex disabilities. NeuroRehabilitation, Volume 23(4), pp. 305 - 311
Mageshwari, U.S., & Minitha, S.J. (2006). Impact of dietary exclusion of casein and gluten on selected autistic children. Indian Journal of Nutrition and Dietetics, Volume 43, pp. 183 – 191
Maglieri, K.A., DeLeon, I.G., Rodriguez-Catter, V., & Sevin, B.M. (2000). Treatment of covert food stealing in an individual with Prader-Willi syndrome. Journal of Applied Behavior Analysis, Volume 33(4), pp. 615 - 618
Magne Tellevik, J., & Elmerskog, B. (2009). Activity-based intervention for multiple-disabled visually impaired people. The British Journal of Visual Impairment, Volume 27(3), pp. 204 - 220
Maguire, E.A., Frackowiak, R.S.J., & Frith, C.D. (1997). Recalling routes around London: activation of the right hippocampus in taxi drivers. Journal of Neuroscience, Volume 17, pp. 7103 – 7110
Maguire, E.A., Burgess, N., Donnett, J.G., Frackowiak, R.S.J., Frith, C.D., & O’Keefe, J. (1998). Knowing where and getting there: a human navigation network. Science, Volume 280. pp. 921 – 924
Maguire, E.A., Gadian, D.G., Johnsrude, I.S., Good, C.D., Ashburner, J., Frackowiak, R.S.J., & Frith, C.D. (2000). Navigation-related structural change in the hippocampi of taxi drivers. Proceedings of the National Academy of Sciences of the United States of America, Volume 97(8), pp. 4398 – 4403
Maguire, E.A., Spiers, H.J., Good, C.D., Hartley, T., Frackowiak,R.S.J., & Burgess, N. (2003). Navigation Expertise and the Human Hippocampus: A Structural Brain Imaging Analysis. Hippocampus. Volume 13. pp. 208 – 217
Maguire, E.A., Woollett, K., & Spiers, H.J. (2006). London taxi drivers and bus drivers: a structural MRI and neuropsychological analysis. Hippocampus. Volume 16(12). pp. 1091 - 1101
Maier, S.F., & Seligman, M. (1976). Learned helplessness: Theory and evidence. Journal of Experimental Psychology, Volume 105, pp. 3 - 46
Maisto, C.R., Baumeister, A.A., & Maisto, A.A. (1978). An analysis of variable related to self-injurious behavior among institutionalised retarded persons. Journal of Mental Deficiency Research. Volume 22, pp. 27 - 36
Mailloux, Z. (1992). Tactile Defensiveness: Some People are More Sensitive. Sensory Integration Quarterly, Vol 20(3), pp. 10 - 11
Mailloux, Z., Mulligan, S., Smith Roley, S., Blanche, E., Cermak, S., Geppert Coleman, G., Bodison, S., & Lane, C.J. (2011). Verification and Clarification of Patterns of Sensory Integrative Dysfunction, American Journal of Occupational Therapy, Volume 65, pp. 143 - 151
Manly, T., Dobler, V.B., Dodds, C.M., & George, M.A. (2005). Rightward shift in spatial awareness with declining alertness. Neuropsychologia, Volume 43(12), pp. 1721 - 1728
Mans, L., Cicchetti, D., & Sroufe, L.A. (1978). Mirror reactions of Down syndrome infants and toddlers: Cognitive underpinnings of self-recognition. Child Development, Volume 49, pp. 1247 - 1250
Mansell, J., Felce, D., de Kock, U., & Jenkins, J. (1982). Increasing purposeful activity of severely and profoundly mentally- handicapped adults. Behaviour Research and Therapy, Volume 20, 593 - 604
Mansell, J. (1984). The operation of regional special support services for people with mental handicap and behavioural problems. Croydon: South East Thames Regional Health Authority.
Mansell, J., Jenkins, J., Felce, D., & de Kock, U. (1984). Measuring the activity of severely and profoundly mentally handicapped adults in ordinary housing. Behaviour Research and Therapy, Volume 22(1), pp. 23 - 29
Mansell, J. (1985). Special services for people with severe mental handicap and severe behaviour problems. Croydon: South East Thames Regional Health Authority
Mansell, J., Felce, D., Jenkins, J., de Kock, U., & Toogood, A. (1987). Developing staffed housing for people with mental handicaps. Tunbridge Wells: Costello.
Mansell, J., & Beasley, F. (1990). Severe mental handicap and problem behaviour: Evaluating transfer from institutions to community care. In W. Fraser (Ed.), Key Issues in Mental Retardation Research. Routledge, London, pp. pp. 405 - 414
Mansell, J. (1994) Specialized group homes for persons with severe or profound mental retardation and serious problem behaviour in England. Research in Developmental Disabilities, Volume 15, pp. 371 - 388
Mansell, J., Hughes, H., & McGill, P. (1994) Maintaining local residential placements. In E. Emerson, P. McGill, & J. Mansell (Eds.), Severe Learning Disabilities and Challenging Behaviour: Designing High-Quality Services (pp. 260 - 281). London: Chapman and Hall.
Mansell, J. (1995). Staffing and staff performance in services for people with severe or profound learning disability and serious challenging behaviour. Journal of Intellectual Disability Research, Volume 39, pp. 3 - 14
Mansell, J., & Elliott, T. (2001). Staff members' prediction of consequences for their work in residential settings. American Journal on Mental Retardation, Volume 106(5), pp. 434 - 447
Mansell, J., McGill, P., & Emerson, E. (2001). Development and evaluation of innovative residential services for people with severe intellectual disability and serious challenging behaviour. In L.M. Glidden (Ed.), International Review of Research in Mental Retardation (pp.245-298). San Diego, CA: Academic Press.
Mansell, J., Elliott, T., Beadle-Brown, J., Ashman, B., & Macdonald, S. (2002). Engagement in meaningful activity and ‘active support’ of people with intellectual disabilities in residential care. Research in Developmental Disabilities, Volume 23(5), pp. 342 – 352
Mansell, J., Beadle-Brown, J., Macdonald, S., & Ashman, B. (2003). Resident involvement in activity in small community homes for people with learning disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 16(1), pp. 63 - 74
Mansell, J., & Beadle‐Brown, J. (2004). Person‐centred planning or person‐centred action? Policy and practice in intellectual disability services. Journal of Applied Research in Intellectual Disabilities, Volume 17(1), pp. 1 - 9
Mansell, J. (2010). Raising our Sights. How-to-Guide . What people do in the day. Mencap
Marcason, W. (2009). What is the current status of research concerning use of a gluten-free, casein-free diet for children diagnosed with autism? Journal of the American Dietetic Association, Volume 109(3), pp. 572
March, J. (1990). The use of peer students to facilitate Words Strategy training. 11th Southeast Annual Augmentative Communication Conference Proceedings, pp. 94 - 98, Birmingham, Alabama: SEAC
Margetts, L. (2010). ‘Hansel and Gretel’. Meaning and relevance in a therapeutic journey: An exploration of the relevance of fairy tales to work with older learning disabled clients who have been institutionalised. British Journal of Music Therapy, Volume 24, pp. 12 – 21
Marí-Bauset, S., Zazpe, I., Mari-Sanchis, A., Llopis-González, A., & Morales-Suárez-Varela, M. (2014). Evidence of the gluten-free and casein-free diet in autism spectrum disorders: a systematic review. Journal of Child Neurology, Volume 29(12), pp. 1718 - 1727
Markowitsch, H.J., & Staniloiu, A. (2011). Memory, autonoetic consciousness, and the self, Consciousness and Cognition, Volume 20(1), pp. 16 - 39
Marsh, H.W. (1994). Using the National Longitudinal Study of 1988 to evaluate theoretical models of self-concept: The Self-Description Questionnaire. Journal of Educational Psychology, Volume 86(3), pp. 439 - 456
Martell, K.A. (2012). Increasing Positive Interactions Between Staff and Individuals with Disabilities: The Impact of Training on
Acquisition and Maintenance. Dissertations. 660.
Martin, F., & Farnum, J. (2002). Animal assisted therapy for children with pervasive developmental disorders. Western Journal of Nursing Research, Volume 24, pp. 657 – 670
Martin, J.E., Marshall, L., Maxson, L.L., & Jerman, P. (1993). Self-Directed IEP. Longmont, CO: Sopris West.
Martin, J.E., Van Dycke, J.L., Christensen, W.R., Greene, B.A., Gardner, J.E., & Lovett, D.L. (2006). Increasing student participation in IEP meetings: Establishing the self-directed IEP as an evidenced-based practice. Exceptional Children, Volume 72, pp. 299 – 316
Martin, P.L., & Foxx, R.M. (1973). Victim control of the aggression of an institutionalized retardate. Journal of Behavior Therapy and Experimental Psychiatry, Volume 4, pp. 161 - 165
Martin, T.L., Martin, G.L., Spevack, S., Verbeke, A., & Yu, D.C.T. (2002). Does choice, independent of preference, improve behavior for persons with developmental disabilities? A review. Developmental Disabilities Bulletin, Volume 30, pp. 1 – 15
Martorell, A., Gutierrez-Recacha, P., Pereda, A., & Ayuso-Mateos, J.L. (2008). Identification of personal factors that determine work outcome for adults with intellectual disability. Journal of Intellectual Disability Research, Volume 52, pp. 1091 – 1101
Masento, N.A., Golightly, M., Field, D.T., Butler, L.T., & van Reekum, C.M. (2014). Effects of hydration status on cognitive performance and mood. British Journal of Nutrition. Volume 111. pp. 1841 - 1852
Mason, C., Field, S., & Sawilowsky, S. (2004). Implementation of self-determination activities and student participation in IEPs. Exceptional Children, Volume 70, pp. 441 – 451
Mason, S.A., & Iwata, B.A. (1990). Artifactual effects of sensory-integrative therapy on self-injurious behavior. Journal of Applied Behavior Analysis, Volume 23, pp. 361 – 370
Matson, J.L., Smiroldo, B.B., Hamilton, M., & Baglio, C.S. (1997). Do anxiety disorders exist in persons with severe and profound mental retardation? Research in Developmental Disabilities, Volume 18(1), pp. 39 - 44
Matson, J.L., Bielecki, J., Mayville, E.A., Smalls, Y., Bamburg, J.W., & Baglio, C.S. (1999). The Development of a Reinforcer Choice Assessment Scale for Persons with Severe and Profound Mental Retardation. Research in Developmental Disabilities, Volume 20(5). pp. 379 – 384
Matson, J.L., Bamburg, J.W., & Smalls, Y. (2004). An analysis of Snoezelen equipment to reinforce persons with severe or profound mental retardation. Research in Developmental Disabilities, Volume 25(1), pp. 89 - 95
Matson, J.L., & Boisjoli, J.A. (2007). Multiple versus maintaining factors of challenging behaviours as assessed by the QABF for adults with intellectual disabilities. Journal of Intellectual Disability Research. Volume 32, pp. 39 – 44
Matson, J.L., Neal, D., Hess, J.A., & Kozlowski, A.M. (2011). Assessment of toileting difficulties in adults with intellectual disabilities: An examination using the profile of toileting issues (POTI). Research in Developmental Disabilities, Volume 32(1), pp. 176 - 179
Matthews, T., Weston, N., Baxter, H., Felce, D., & Kerr, M. (2008). A general practice-based prevalence study of epilepsy among adults with intellectual disabilities and of its association with psychiatric disorder, behaviour disturbance and carer stress. Journal of Intellectual Disability Research. Volume 52, pp. 163 – 173
Mauer, D.A. (1999). Issues and Applications of Sensory Integration Theory and Treatment With Children With Language Disorders. Language, Speech, and Hearing Services in Schools. Volume 30, pp. 383 - 392
Maurice, P., & Trudel, G. (1982). Self-injurious behavior: prevalence and relationship to environmental events. In J.H. Hollis & C.E. Meyers, (Eds.), Life-Threatening Behavior: Analysis and Intervention. Washington, D.C.: American Association on Mental Deficiency.
May-Benson, T. (2011). Understanding the Occupational Therapy Needs of Adults With Sensory Processing Disorder. OT practice, Volume 16(10), pp.13 - 14,16 - 18
McAfee,J.K. (1987). Classroom density and the aggressive behavior of handicapped children. Education and Treatment of Children, Volume 10, pp. 134 - 145
McBride, K. (2003). Identifying Person Preference in Individuals With a Profound Learning Disability and High Support Needs. University of Hull
McBride, S.D., Perentos, N., & Morton, A.J. (2015). Understanding the concept of a reflective surface: Can sheep improve navigational ability through the use of a mirror? Animal Cognition, Volume 18, pp. 361 – 371
McBrien, J., & Weightman, J. (1980). The effect of room management procedures on engagement of profoundly handicapped children. British Journal of Mental Subnormality, Volume 26, pp. 38 - 53
McCall, R.B. (1972). Smiling and vocalization in infants as indices of perceptual-cognitive processes. Merrill-Palmer Quarterly, Volume 18, pp. 341 - 347
McCarty, B.C., McElfresh, C.T., Rice, S.V., & Wilson, S.J. (1978). The effect of contingent background music on inappropriate bus behaviour. Journal of Music Therapy, Volume 15(3), pp. 150 - 156
McClelland, J.L. (1996). Role of the Hippocampus In Learning and Memory: A Computational Analysis. In - Ono, T., McNaughton, B.L., Molotchnikoff, S., Rolls, E.T., & Nichijo, H. (Eds. ), Perception, Memory, and Emotion. pp. 601- 613. Frontier in Neuroscience. Oxford: Elsevier Science, Ltd.
McClintock, K., Hall, S., & Oliver, C. (2003). Risk markers associated with challenging behaviours in people with intellectual disabilities: A meta-analytic study. Journal of Intellectual Disability Research, Volume 47(6), pp. 405 - 416
McConkey, R., Morris, I., & Purcell, M. (1999). Communications between staff and adults with intellectual disabilities in naturally occurring settings. Journal of Intellectual Disability Research, Volume 43(3), pp. 194 - 205
McConkey, R., & Collins, S. (2010a). Using personal goal setting to promote the social inclusion of people with intellectual disability living in supported accommodation. Journal of Intellectual Disability Research, Volume 54(2), pp. 135 - 143
McConkey, R., & Collins, S. (2010b). The role of support staff in promoting the social inclusion of persons with an intellectual disability. Journal of Intellectual Disability Research, Volume 54(8), pp. 691 - 700
McCool, C., Barrett, S., Emerson, E., Toogood, A., Hughes, H., & Cummings, R. (1989). Challenging behaviour and community services. 5. Structuring staff and client activity. Mental Handicap, Volume 17, pp. 60 - 64
McDonnell, A., & Sturmey, P. (1993). Managing violent and aggressive behaviour: towards better practice. In S. Jones & C. Eayres (Eds), Challenging Behaviour and Intellectual Disability: psychological perspectives. Kidderminster: BILD
McEwen, B.S. (2012). Brain on stress: How the social environment gets under the skin. Proceedings of the National Academy of Sciences. Volume 109(2). pp. 17180 – 17185
McEwen, I.R. (1992). Assistive positioning as a control parameter of social-communicative interactions between students with profound multiple disabilities and classroom staff. Physical Therapy, Volume 72(9), pp. 634 - 644
McFerran, K., & Rickson, D. (2007). Music therapy in special education: Where are we now? The New Zealand Journal of Education, Volume 8(1), pp. 40 - 47
McFerran, K., & Shanahan, E. (2011). Music therapy practice in special education and children's hospice: A systematic comparison of two music therapists' strategies with three pre-adolescent boys. Music Therapy Perspectives, Volume 29(2), pp. 103 - 111
McFerran, K., & Elefant, C. (2012). A Fresh Look at Music Therapy in Special Education. In - G. McPherson & G. Velch (Eds.), The Oxford Handbook of Music Education, Vol. 2, pp. 51 - 64. Oxford: Oxford University Press.
McFerran, K., & Shoemark, H. (2013). How musical engagement promotes well-being in education contexts: The case of a young man with profound and multiple disabilities. International Journal of Qualitative Studies on Health & Well-Being, Volume 8, pp. 1 - 14
McGill, P., Emerson, E., & Mansell, J. (1994). Individually designed residential provision for people with seriously challenging behaviours. In E. Emerson, P. McGill, & J. Mansell (Eds.), Severe Learning Disabilities and Challenging Behaviour: Designing High-Quality Services. London: Chapman and Hall.
McGill, P., & Mansell, P. (1995). Community placements for people with severe and profound learning disabilities and serious challenging behaviour: Individual illustrations of issues and problems. Journal of Mental Health, Volume 4, pp. 183 - 198.
McGill, P., Bradshaw, J., & Hughes, A. (2007). Impact of extended education/training in positive behaviour support on staff knowledge, causal attributions and emotional responses. Journal of Applied Research in Intellectual Disabilities, Volume 20(1), pp. 41 – 51
McGimsey, J.F., & Favell, J.E. (1988). The effects of increased physical exercise on disruptive behavior in retarded persons. Journal of Autism and Developmental Disorders, Volume 18, pp. 167 - 179
McGuire, B.E. Daly, P., & Smyth, F. (2007). Lifestyle and health behaviours of adults with an intellectual disability. Journal of Intellectual Disability Research, Volume 51(7). pp. 497 - 510
McGuire, J., & McDonnell, J. (2008). Relationships between recreation and levels of self-determination for adolescents and young adults with disabilities. Career Development for Exceptional Individuals, Volume 31, pp. 154 – 163
McIntyre, L.L. Blacher, J., & Baker, B.L. (2002). Behaviour/mental health problems in young adults with intellectual disability: The impact on families. Journal of Intellectual Disability Research, Volume 46, pp. 239 – 249
McIntyre, L.L., Kraemer, B.R., & Blacher, J. Simmerman., S. (2004). Quality of life for young adults with severe intellectual disability: Mothers' thoughts and reflections. Journal of Intellectual and Developmental Disability, Volume 29, pp. 131 - 146
McKendrick, O. (1991). Assessment of Multi-handicapped Visually Impaired Children. Royal National Institute for the Blind.
McKenzie, K. (2011). Providing services in the United Kingdom to people with an intellectual disability who present behaviour which challenges: A review of the literature. Research in Developmental Disabilities, Volume 32(2). pp. 395 - 403
McKnight, T.J., & Kearney, C.A. (2001). Staff Training Regarding Choice Availability for Persons with Mental Retardation: A Preliminary Analysis. Journal of Developmental and Physical Disabilities, Volume 13(1), pp. 1 - 10
McLarty, M. (1991). Learning through real experience. Deafblind Education, Volume 7, pp. 10 - 13
McLean, J. E., McLean, L. K., Brady, N. C., & Etter, R. (1991). Communication profiles of two types of gesture using nonverbal persons with severe to profound mental retardation. Journal of Speech, Language, and Hearing Research, Volume 34(2), pp. 294 - 308
McLinden, M.. & McCall, S. (2002). Learning through Touch. Supporting Children with Visual Impairment and Additional Difficulties. London: David Fulton.
McNairn, P. (1995). Freedom and success. 3rd Annual Pittsburgh Employment Conference Proceedings. pp. 73 - 77
McNaughton, D., & Light, J. (1989). Teaching facilitators to support the communication skills of an adult with severe cognitive disabilities: A case study. Augmentative and Alternative Communication, Volume 5(1), pp. 35 - 41
McNicholas, J., Collis, G.M., & Morley, I.E. (1993). Psychological and physical effects of enforced pet loss on older people entering residential care. Journal of Companion Animal Studies. Volume 5(4)
McNicholas, J., Gilbey, A., Rennie, A., Ahmedzai, S., Dono, J., & Ormerod, E. (2005). Pet ownership and human health: a brief review of evidence and issues. British Medical Journal, Volume 7527, pp. 1252 - 1254
McNicholas. J., & Collis, G.M. (2006). Animals as social supports: insights for understanding animal assisted therapy. In - Fine, A. (ed.), Handbook on Animal-Assisted Therapy. Elsevier, San Diego:pp. 49 - 71
McVilly, K.R., Burton-Smith, R.M., & Davidson, J.A. (2000). Concurrence between subject and proxy ratings of quality of life for people with and without intellectual disabilities. Journal of Intellectual and Developmental Disability, Volume 25(1), pp. 19 - 39
Meador, D.M., & Osborn, R.G. (1992). Prevalence of severe behavior disorders in persons with mental retardation and treatment procedures used in community and institutional settings. Behavioral Residentiall Treatment. Volume 4, pp. 299 - 314
Medeiros, K., Rojahn, J., Moore, L.L., & Ingen, D.J. (2014). Functional properties of behaviour problems depending on level of intellectual disability. Journal of Intellectual Disability Research, Volume 58(2), pp. 151 - 161
Mednick, M. (2002). Supporting children with multiple disabilities. Birmingham: Questions Publishing.
Mehigan, P. (2004). Teaching contingency awareness in the classroom to pupils with very profound general learning disabilities, Unpublished Master's Thesis, St. Patrick's College, Dublin City University.
Mehigan, P. & Ware, J. (2004). Teaching Contingency-Awareness in the Classroom, Presentation at IASSID 12th World Congress, Montpellier, France.
Mehler, M.F. (2000). Brain dystrophin, neurogenetics and mental retardation. Brain Research Reviews, Volume 32(1), pp. 277 - 307
Mehrabian, A., & Ferris, S.R. (1967). Inference of attitudes from nonverbal communication in two channels. The Journal of Counselling Psychology. Volume 31(3), pp. 248 - 252
Mellstrom, B.P., Saunders, M.D., Saunders, R.R., & Olswang, L.B. (2005). Interaction of behavioural state and microswitch use in individuals with profound multiple impairments. Journal of Developmental and Physical Disabilities, Volume 17(1), pp. 35 – 53
Melville, C.A., Hamilton, S., Hankey, C.R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of obesity in adults with intellectual disabilities. Obesity Reviews, Volume 8(3), 223 - 230
Melville, C.A., Cooper, S.A., Morrison, J., Allan, L., Smiley, E., & Williamson, A. (2008). The prevalence and determinants of obesity in adults with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 21(5), pp. 425 - 437
Melville, C.A., Oppewal, A., Elinder, L.S., Freiberger, E., Guerra-Balic, M., Hilgenkamp, T.I., Einarsson, I., Izquierdo-Gómez, R., Sansano-Nadal, O., Rintala, P., & Cuesta-Vargas, A. (2017). Definitions, measurement and prevalence of sedentary behaviour in adults with intellectual disabilities - A systematic review. Preventive Medicine. Volume 97. pp. 62 - 71
Melville, H. (1853). Bartleby, The Scrivener: A Story Of Wall-street. Putnam's Monthly Magazine, two parts in November and December 1853
Mencap (2008). About Profound and Multiple Learning Disabilities, Mencap Publications
Mercer, C.D., & Snell, M.E. (1977). Learning theory research in mental retardation: Implications for teaching. Columbus, OH: Merrill.
Mercieca, D.P. (2012). Living Otherwise: Students with Profound and Multiple Learning Disabilities as Agents in Educational Contexts. Sense Publishers
Merino, J., Kones, R., Ferré, R., Plana, N., Girona, J., Aragonés, G., Ibarretxe, D., Heras, M., & Masana, L. (2013). Negative effect of a low-carbohydrate, high-protein, high-fat diet on small peripheral artery reactivity in patients with increased cardiovascular risk. British Journal of Nutrition. Volume 109(7). pp. 1241 - 1247
Messent, P.R., Cooke, C.B., & Long, J. (1998). Physical activity, exercise and health of adults with mild and moderate learning disabilities. British Journal of Learning Disabilities, Volume 26(1), pp. 17 – 22
Messent, P.R., Cooke, C.B., & Long, J. (1999). Primary and secondary barriers to physically active healthy lifestyles for adults with learning disabilities. Disability and Rehabilitation, Volume 21(9), pp. 409 - 419
Metell, M. (2014). Dis/Abling musicking: Reflections on a disability studies perspective in music therapy. Voices: A World Forum for Music Therapy, Volume 14(3), Retrieved from: https://voices.no/index.php/voices/article/view/786/657.
Milgram, N. (1973). Cognition and language in mental retardates: Distinctions and implications In - The experimental psychology of mental
retardation, Routh, D. (Ed.), pp. 157 - 230, London: Crosby Lockwood Staples (1974)
Miller, K. (2008) Wired: Energy drinks, jock identity, masculine norms, and risk taking. Journal American College Health, Volume 56(5), pp.
481 - 490
Miller, L.J. (2007). Sensational Kids: Hope and Help for Children with Sensory Processing Disorder. New York: Perigee.
Miller, L.K. (1999). The savant syndrome: intellectual impairment and exceptional skill. Psychological Bulletin, volume 125(1), pp. 31 - 46
Miller, S., & Aitken, S. (2003). Personal Communication Passports, Guidelines for Good Practice. Call Centre, Scotland
Millward, C., Ferriter, M., Calver, S.J., & Connell‐Jones, G.G. (2008). Gluten‐and casein‐free diets for autistic spectrum disorder. The Cochrane Library.
Ming Lee Yeh, A. (2008). Canine AAT model for autistic children. Tokyo Japan: At Taiwan International Association of Human-Animal Interaction International Conference.
Mirenda, P. (1993a). AAC: Bonding the uncertain mosaic. AAC, Volume 9(1), pp. 3 - 9
Mirenda, P. (1993b). Communication approaches for persons with severe intellectual disabilities. 14th Southeast Annual Augmentative
Communication Conference Proceedings, pp. 67 - 83, Birmingham, Alabama: SEAC
Misso, N. (2001). Guide to orientation and mobility for young children with vision impairments. RNIB
Mitchell, J., & van der Gaag, A. (2002). Through the eye of the Cyclops: Evaluating a multi-sensory intervention programme for people with complex disabilities. British Journal of Learning Disabilities, Volume 30(4), pp. 159 – 165
Mitchell, R.W. (2002). Subjectivity and self-recognition in animals, in M.R. Leary & J.P. Tangney (Eds.), Handbook of Self and Identity. pp. 567 - 595. New York: Guilford Press.
Mitchell, S.W. (1871). Phantom limbs, Lippincott’s Magazine of Popular Literature and Science. Volume 8, pp. 563 – 569
Mithaug, D.E., & Hanawalt, D.A. (1978). The validation of procedures to assess prevocational task preferences in retarded adults. Journal of Applied Behavior Analysis, Volume 11, pp. 153 - 162
Mithaug, D.E., & Mar, D. (1980). The relation between choosing and working prevocational tasks in two severely retarded young adults. Journal of Applied Behavior Analysis, Volume 13, pp. 177 – 182
Mithaug, D.E., Campeau, P.L., & Wolman, J.M. (2003). Assessing self-determination prospects among students with and without disabilities. In D.E. Mithaug, D.K. Mithaug, M. Agran, J.E. Martin, & M.L. Wehmeyer (Eds.), Self determined learning theory: Construction, verification, and evaluation (pp. 61 – 76). Mahwah, NJ: Lawrence Erlbaum.
Mithaug, D.K., & Mithaug, D.E. (2003). The effects of choice opportunities and self-regulation training on the self-engagement and learning of young children with disabilities, in: Self-Determined Learning Theory: Construction, Verification, and Evaluation, D.E. Mithaug, D.K. Mithaug, M. Agran, J.E. Martin, and M. Wehmeyer, eds pp. 141–157. Mahwah, NJ: Lawrence Erlbaum Associates, Inc, Publishers
Moffat V. (1996). Life Without Jargon: How to Help People with Learning Difficulties Understand What You Are Saying. Choice Press
Montello, L., & Coons, E.E. (1999). Effects of active versus passive group music therapy on pre-adolescents with emotional, learning, and behavioral disorders. Journal of Music Therapy, Volume 35(1), pp. 49 - 67
Montgomery, P., & Richer, E. (1977). Effect of sensory integrative therapy on the neuromotor development of retarded children. Physical
Therapy, Volume 57, pp. 799 - 807
Morin, A., & DeBlois, S. (1989). Gallup's mirrors: more than an operationalization of self-awareness in primates? Psychological Reports, Volume 65, pp. 287 - 291
Morin, A., & Everett, J. (1990). Inner speech as a mediator of self-awareness, self-consciousness, and self-knowledge: an hypothesis, New Ideas in Psychology, Volume 8(3), pp. 337 - 356
Morin, A. (2002). Right hemispheric self-awareness: A critical assessment. Consciousness and Cognition, Volume 11, pp. 396 – 401
Morin, A. (2003). Let’s face it. A review of Keenan, Gallup, & Falk’s book ‘‘The Face in the Mirror”. Evolutionary Psychology, Volume 1, pp. 161 – 171
Morin, A. (2004). A neurocognitive and socioecological model of self-awareness. Genetic, Social, and General Psychology Monographs, Volume 130, pp. 197 – 222
Morin, A. (2005). Possible links between self-awareness and inner speech: Theoretical background, underlying mechanisms, and empirical evidence. Journal of Consciousness Studies, Volume 12(4-5), pp.115 - 134
Morin, A. (2006). Levels of consciousness and self-awareness: A comparison and integration of various views. Consciousness and Cognition. Volume 15, pp. 358 – 371
Morin, A. (2007). Self-awareness and the left hemisphere: The dark side of selectively reviewing the literature (Commentary on Keenan et al., Cortex, 2005). Cortex, Volume 8, pp. 1068 – 1073
Morin, A., & Michaud, J. (2007). Self-awareness and the left inferior frontal gyrus: Inner speech use during in self-related processing. Brain Research Bulletin, Volume 74(6), pp. 387 – 396
Morin, A. (2009). Self-awareness deficits following loss of inner speech: Dr. Jill Bolte Taylor's case study. Consciousness and Cognition. Volume 18(2), pp. 524 - 529
Morin, A. (2010). Self-recognition, Theory-of-Mind, and self-awareness: what side are you on? Laterality, Volume 16(3), pp. 367 - 383
Morin, A. (2011). Self‐Awareness Part 1: Definition, Measures, Effects, Functions, and Antecedents. Social and Personality Psychology Compass. Volume 5(10). pp. 807 – 823
Morin, A., Uttl, B., & Hamper, B. (2011). Self-reported frequency, content, and functions of inner speech, Procedia-Social and Behavioral Journal, Volume 30, pp. 1714 - 1718
Morin, A. (2012). Inner speech, in W. Hirstein (ed), Encyclopedia of human behavior (2nd edition), pp. 436 - 443, Elsevier.
Morin, A. (2017). The self-reflective function of inner speech: Twelve years later. ResearchGate.Net
Morley, R. & Lucas, A. (1997). Nutrition and cognitive development. British Medical Bulletin. Volume 53(1). pp.123 - 134
Morningstar, M., & Wehmeyer, M.L. (2008). The role of families in enhancing transition outcomes for youth with learning disabilities. In G. Blalock, J. Patton, P. Kohler, & D. Bassett (Eds.), Transition and students with learning disabilities: Facilitating the movement from school to adult life (2nd ed., pp. 79 – 104). Austin, TX: ProEd Publishers.
Morris, R. & Fillenz, M. (eds) (2003). Neuroscience: the Science of the Brain. The British Neuroscience Association
Morrison, M.L. (2007). Health benefits of animal assisted interventions. Complementary Health Practice Review. Volume 12(1). pp. 51 - 62
Mortenson, B.P., & Witt, J.C. (1998). The use of weekly performance feedback to increase teacher implementation of prereferral intervention. School Psychology Review, Volume 27(4), pp. 613 - 627
Moss, C.V. (1972). Recovery with Aphasia. Illinois: University of Illinois Press.
Moss, J., Oliver, C., Hall, S., Arron, K., Sloneem, J., & Petty, J. (2005). The association between environmental events and self-injurious behaviour in Cornelia de Lange syndrome. Journal of Intellectual Disability Research, Volume 49, pp. 269 – 277
Mottron, L., Belleville, S., Stip,E., & Morasse, K. (1998). Atypical memory performance in an autistic savant. Memory, Volume 6(6), pp. 593 - 607
Mount, H., & Cavet, J. (1995). Multi‐sensory environments: an exploration of their potential for young people with profound and multiple learning difficulties. British Journal of Special Education, Volume 22(2), pp. 52 - 55
Mulford, H. (2001). A review of the curriculum for pupils with profound and multiple learning disabilities. Tizard Learning Disability Review, Volume 6(2), pp. 30 - 31
Mulick, J.A., Hoyt, P., Rojahn, J., & Schroeder, S.R. (1978). Reduction of a “nervous habit” in a profoundly retarded youth by increasing toy play. Journal of Behavior Therapy and Experimental Psychiatry, Volume 9, pp. 381 – 385
Mulligan, S. (1998). Patterns of sensory integration dysfunction: A confirmatory factor analyses. American Journal of Occupational Therapy, Volume 52, pp. 819 – 828.
Mulligan, S. (2002). Advances in sensory integration research. In A.C. Bundy, S. Lane, & E.A. Murray, (Eds.). Sensory integration: Theory and practice (2nd ed., pp. 397 – 411). Philadelphia: F. A. Davis.
Mulloy, A., Lang, R., O’Reilly, M., Sigafoos, J., Lancioni, G., & Rispoli, M. (2010). Gluten-free and casein-free diets in the treatment of autism spectrum disorders: A systematic review. Research in Autism Spectrum Disorders, Volume 4(3), pp. 328 – 339
Mulloy, A., Lang, R., O’Reilly, M., Sigafoos, J., Lancioni, G., & Rispoli, M. (2011). Addendum to “gluten-free and casein-free diets in treatment of autism spectrum disorders: A systematic review”. Research in Autism Spectrum Disorders, Volume 5(1), pp. 86 - 88
Munde, V.S., & Vlaskamp, C. (2010). Alertness observations in children with profound intellectual and multiple disabilities. International Journal of Child Health and Human Development, Volume 3(1), pp. 115 - 124
Munde, V.S., Vlaskamp, C., Ruijssenaars, A.J.J.M., & Nakken, H. (2009a). Alertness in individuals with profound intellectual and multiple disabilities: A literature review. Research in Developmental Disabilities, Volume 30(3), pp. 462 - 480
Munde, V.S., Vlaskamp, C., Ruijssenaars, A.J.J.M., & Nakken, H. (2009b). Experts discussing “alertness in individuals with PIMD”: A Concept Mapping procedure. Journal of Developmental and Physical Disabilities, Volume 21(4), pp. 263 - 277
Munde, V.S., Vlaskamp, C., Ruijssenaars, A., Maes, B., & Nakken, H. (2010). Alertness and Snoezelen in individuals with PIMD. Journal of Applied Research in Intellectual Disabilities. Vol. 23(5), pp. 499
Munde, V.S. (2011). Attention please!. Alertness in individuals with profound intellectual and multiple disabilities. Doctoral dissertation. Rijksuniversiteit Groningen, Groningen.
Munde, V.S., Vlaskamp, C., Ruijssenaars, A.J.J.M., & Nakken, H. (2011). Determining alertness in individuals with profound intellectual and multiple disabilities: The reliability of an observation list. Education and Training in Autism and Developmental Disabilities, Volume 46(1), pp. 116 - 123
Munde, V.S., Vlaskamp, C., Post, W.J., Ruijssenaars, A.J.J.M., Maes, B., & Nakken, H. (2012). Observing and influencing alertness in individuals with profound intellectual and multiple disabilities in multisensory environments. Journal of Cognitive Education and Psychology, Volume 11(1), pp. 5 - 19
Munde, V.S, Vlaskamp, C., Vos, P., Maes, B., & Ruijssenaars, W. (2012). Physiological measurements as validation of alertness observations: An exploratory case study of three individuals with profound intellectual and multiple disabilities. Intellectual & Developmental Disabilities, Volume 50(4), pp. 300 - 310
Munde, V.S., Vlaskamp, C., Maes, B., & Ruijssenaars, A.J.J.M. (2014). Catch the wave! Time‐window sequential analysis of alertness stimulation in individuals with profound intellectual and multiple disabilities. Child: Care, Health and Development, Volume 40(1), pp. 95 - 105
Munde, V.S, & Vlaskamp, C. (2015). Initiation of activities and alertness in individuals with profound intellectual and multiple disabilities. Journal of Intellectual Disability Research, Volume 59(3), pp. 284 - 292
Munde, V.S., & Vlaskamp, C. (2015b). Vestibular stimulation and alertness in individuals with profound intellectual and multiple disabilities. European Journal of Intellectual Disability. Volume 9
Murdoch, H. (1994). "He can hear when he wants to!" Assessment of Hearing Function for People with Learning Difficulties'. Volume 22. pp. 85 - 89
Murdoch, H. (1997). Stereotyped behaviours: how should we think about them? British Journal of Special Education, Volume 24(2), pp. 71 - 75
Murdoch, H., McMinn, R., Gopsill, S., McLinden, A., & Smith, G. (2009): A curriculum for multi-sensory impaired children, MSI Unit
Victoria School Birmingham, Sense Publications
Murphy, G.H., & Oliver, C. (1987). Decreasing undesirable behaviours. In W. Yule and J. Carr (Eds.), Behaviour Modification for People with Mental Handicaps, 2nd Edn. Croom Helm, London, pp. 102 - 142
Murphy, G.H., Oliver, C., Corbett, J., Crayton, L., Hales, J., Head, D., & Hall, S. (1993). Epidemiology of self-injury, characteristics of people with severe self-injury and initial treatment outcome. In C. Kiernan (ed.), Research to Practice? Implications of Research on the Challenging Behaviour of People with Learning Difficulties. pp. 1 - 35. Kidderminster. BILD
Murphy, G.H., Hall, S., Oliver, C., & Kissi-Debra, R. (1999). Identification of early self-injurious behaviour in young children with intellectual disability. Journal of Intellectual Disability Research. Volume 43, pp. 149 - 163
Murphy, G.H., Beadle-Brown, J., Wing, L., Gould, J., Shah, A., & Holmes, N. (2005). Chronicity of challenging behaviours in people with severe intellectual disabilities and/or autism: a total population sample. Journal of Intellectual Disability Research. Volume 35, pp. 405 – 418
Murphy, J., & Cameron, L. (2008). The effectiveness of Talking Mats with people with intellectual disability. British Journal of Learning Disabilities, Volume 36(4), pp. 232 - 241
Murphy, K.M., Saunders, M.D., Saunders, R.R., & Olswang, L.B. (2004). Effects of ambient stimuli on measures of bio-behavioral state and microswitch use in adults with profound multiple impairments, Research in Developmental Disabilities, Volume 25(4), pp. 355 - 370
Musselwhite, C.R., & St. Louis, K.W. (1988). Communication programming for persons with severe handicaps: Vocal and augmentative
strategies. San Diego: College-Hill Press
Nackley, V.L. (2001). Sensory diet applications and environmental modifications: A winning combination. Sensory Integration Special Interest Section Quarterly, Volume 24(1), pp. 1 - 4
Nafstad, A., & Rødbroe, I. (1999). Co-creating communication: Perspectives on diagnostic education for individuals who are congenitally deafblind and individuals whose impairments may have similar effects. Nord-Press.
Naish, L., Bell, J., & Clunies-Ross, L. (2004). Exploring access: how to audit your school environment, focusing on the needs of pupils who have multiple disabilities and visual impairment. RNIB
Nakken, H., & Vlaskamp, C. (2002). Joining forces: Supporting individuals with profound multiple learning disabilities. Tizard Learning Disability Review, Volume 7(3), pp. 10 - 15
Nakken, H., & Vlaskamp, C. (2007). A need for a taxonomy for profound intellectual and multiple disabilities. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(2), pp. 83 - 87
Narayan, J., Madhavan, T., Suryaprakasham, B. (1993). Self-awareness of people with mental handicap. International Journal of Rehabilitation Research. Volume 16(1), pp. 59 - 63
National Scientific Council on the Developing Child. (2005/2014). Excessive Stress Disrupts the Architecture of the Developing Brain: Working Paper 3. Center on the Developing Child at Harvard University
Nazni, P., Wesely, E., & Nishadevi, V. (2008). Impact of casein and gluten free dietary intervention on selected autistic children. Iranian Journal of Pediatrics, Volume 18(3), pp. 244 - 250
NCAC (2011). Making sense of it all – young children and sensory processing. Putting Children First. The magazine of the National Childcare Accreditation Council (NCAC). Volume 38. pp. 18 - 20
Neely-Barnes, S., Marcenko, M., & Weber, L. (2008). Does choice influence quality of life for people with mild intellectual disabilities? Intellectual and Developmental Disabilities, Volume 46, pp.12 – 26
Neerinckx, H., Vos, P., Van Den Noortgate, W., & Maes, B. (2014). Temporal analysis of attentional processes in spontaneous interactions between people with profound intellectual and multiple disabilities and their support workers. Journal of Intellectual Disability Research, Volume 58(8), pp. 721 - 733
Neerinckx, H., & Maes, B. (2016). Joint attention behaviours in people with profound intellectual and multiple disabilities: the influence of the context. Journal of Applied Research in Intellectual Disabilities, Volume 29(6), pp. 574 - 584
Nelson, C., van Dijk, J., & McDonnell, A. (2001). Child-guided Strategies for Understanding Children who are Deaf-blind or have Severe Multiple Disabilities: The van Dijk Approach to Assessment on Child-guided Strategies for Assessing Children who are Deaf-blind or have
Multiple Disabilities, C. Nelson & J. van Dijk. CD-ROM from Aap Noot Muis Productions/Instituut voor Doven/Cidv, Netherlands.
Nelson, C., van Dijk, J., McDonnell, A.P., & Thompson, K. (2002). A framework for understanding young children with severe and multiple disabilities: The van Dijk approach to assessment. Research and Practice for Persons with Severe Disabilities, Volume 27(2), pp. 97 - 111
Nelson, D., Anderson, V., & Gonzales, A. (1984). Music activities as therapy for children with autism and other pervasive developmental disorders. Journal of Music Therapy, Volume 21(3), pp. 100 - 116
Nelson, K. (2005). Emerging levels of consciousness in early human development. In H.S. Terrace & J. Metcalfe (Eds.), The missing link in cognition: Origins of self-reflective consciousness. Oxford: Oxford University Press, pp. 116–141
Neuman, C.J., & Hill, S.D. (1978). Self-recognition and stimulus preference in autistic children. Developmental Psychobiology, Volume 11, pp. 571 - 578
Newman, I., & Emerson, E. (1991). Specialised treatment units for people with challenging behaviours. Mental Handicap, Volume 19(3), pp. 113 - 119
Newton, J.S., Horner, R.H., & Lund, L. (1991). Honoring activity preferences in individualized plan development: A descriptive analysis. Journal of The Association for Persons with Severe Handicaps, Volume 16, pp. 207 - 212
Nguyen, T. (2010). Total number of synapses in the adult human neocortex. Undergraduate Journal of Mathematical Modeling: One+ Two, Volume 3(1), pp. 1 -13
Nicholls, T. (2002). Could I Play a Different Role?: Group Music Therapy with Severely Learning Disabled Adolescents. In - A. Davies & E. Richards (Eds.), Music Therapy and Group Work: Sound Company, pp. 231 - 246. London: Jessica Kingsley
Nielsen, L. (1979). The Comprehending Hand. Copenhagen: Socialstyrelsen.
Nielsen, L. (1990). Are you Blind? Promotion of the Development of Children who are Especially Developmentally Threatened. Copenhagen: Sikon.
Nielsen, L. (1991). Spatial relations in congenitally blind infants: a study. Journal of Visual Impairment and Blindness, Volume 85, pp. 11 - 16
Nielsen, L. (1992). Space and Self-Active learning by means of the Little Room. Copenhagen: Sikon.
Nielsen, L. (1993). Early Learning Step by Step. Copenhagen: Sikon.
Nijs, S., Penne, A., Vlaskamp, C., & Maes, B. (2016). Peer Interactions among Children with Profound Intellectual and Multiple Disabilities during Group Activities. Journal of Applied Research in Intellectual Disabilities, Volume 29(4), pp. 366 - 377
Nijs, S., Vlaskamp, C., & Maes, B. (2016). Children with PIMD in interaction with peers with PIMD or siblings. Journal of Intellectual Disability Research, Volume 60(1), pp. 28 - 42
Nijs, S., Vlaskamp, C., & Maes, B. (2016b). The nature of peer‐directed behaviours in children with profound intellectual and multiple disabilities and its relationship with social scaffolding behaviours of the direct support worker. Child: Care, Health and Development, Volume 42(1), pp. 98 - 108
Nind, M., & Hewett, D. (1988). Interaction as Curriculum, British Journal of Special Education, Volume 15(2), pp. 55 - 57
Nind, M., & Hewett, D. (1989). Teaching pupils with very severe learning difficulties by means of Intensive Interaction: some typical questions and answers, Portage Into the Nineties Papers from the 1989 National Portage Association Conference. The National Portage Association.
Nind, M. (1993). Access to Communication: Efficacy of Intensive Interaction Teaching for people with severe developmental disabilities who demonstrate ritualistic behaviours. Ph.D Thesis, Cambridge Institute of Education.
Nind, M., & Hewett, D. (1994). Access to communication - developing the basics of communication with people with severe learning
difficulties. David Fulton
Nind, M. (1996). Efficacy of Intensive Interaction: developing sociability and communication in people with severe and complex learning difficulties using an approach based on caregiver-infant interaction’, European Journal of Special Needs Education, Volume 11(1), pp.48 - 66
Nind, M., & Hewett, D. (1996). When age-appropriateness isn't appropriate, in Coupe-O'Kane, J & Goldbart, J. (eds) Whose choice? London: David Fulton.
Nind, M. (2000). Teachers understanding of interactive approaches in special education, International Journal of Disability, Development and Education, Volume 47(2), pp.184 - 199
Nind, M. (2000). Intensive Interaction and children with autism, in Powell, S. (ed) Helping Children with Autism to Learn. London: David Fulton.
Nind, M. & Powell, S. (2000). Intensive Interaction and autism: some theoretical concerns, Children and Society, Volume 14(2), pp.98 - 109
Nind, M. & Kellett, M. (2002). Responding to learners with severe learning difficulties and stereotyped behaviour: challenges for an inclusive era, European Journal of Special Needs Education, Volume 17(3), pp.265 - 282
Nind, M., Kellett, M. & Hopkins, V. (2001). Teachers’ talk styles: communication with learners with severe learning difficulties, Child Language, Teaching and Therapy, Volume 17(2), pp.143 - 159
Nind, M. & Kellett, M. (2002). Response to James Hogg, Juliet Goldbart and John Harris re 'Responding to individuals with severe learning difficulties and stereotyped behaviour: challenges for an inclusive era’, European Journal of Special Needs Education, Volume 17(3), pp. 299 - 300
Nind, M. & Cochrane, S. (2002). Inclusive curricula? Pupils on the margins of special schools, International Journal of Inclusive Education, Volume 6(2), pp.185 - 198
Nind, M. (2003). Enhancing the communication learning environment of an early years unit through action research, Educational Action Research, Volume 11(3), pp.347 - 363
Nissen, J.M.J.F., & Haveman, M.J. (1997). Mortality and avoidable death in people with severe self-injurious behaviour: Results of a Dutch study. Journal of Intellectual Disability Research, Volume 41, pp. 252 - 257
Nordoff, P., & Robbins, C. (1965). Music Therapy for Handicapped Children: Investigations and Experiences. New York: Rudolf Steiner Publications.
Nordoff, P., & Robbins, C. (1971). Therapy in Music for Handicapped Children. London: Gollancz.
Nordoff, P., & Robbins, C. (1977). Creative Music Therapy: Individualized Treatment for the Handicapped Child. New York: John Day & Co.
Northern Ireland Curriculum (2012). Quest For Learning
Norton, Y. (1975). Neuro-development and sensory integration for the profoundly retarded multiply handicapped child. American Journal of Occupational Therapy, Volume 29, pp. 93 - 100
Nota, L., Ferrari, L., Soresi, S., & Wehmeyer, M.L. (2007). Self determination, social abilities, and the quality of life of people with intellectual disabilities. Journal of Intellectual Disability Research, Volume 51, pp. 850 – 865
Nozaki, K., & Mochizuki, A. (1995). Assessing Choice Making of a Person With Profound Disabilities: A Preliminary Analysis. Journal of The Association for Persons with Severe Handicaps. Volume 20(3), pp. 196 - 201
Nunez, M. (2014). Joint attention in deafblind children: a multisensory path towards a shared sense of the world. Sense Research.
O’Brien, J. (2000). Self-determination—with strings attached. Mouth, Volume 10(5), pp. 36
O’Brien, Y., Glenn, S., & Cunningham, C. (1994). Contingency Awareness in Infants and Children with Severe and Profound Learning Disabilities, International Journal of Disability, Development and Education, Volume 41(3), pp. 231 - 243
O'Haire, M.E. (2010). Companion animals and human health: Benefits, challenges, and the road ahead. Journal of Veterinary Behavior: Clinical Applications and Research. Volume 5, pp. 226 – 234
O'Haire, M.E. (2012). Animal-assisted intervention for autism spectrum disorder: A systematic literature review. Journal of Autism and Developmental Disorders, Volume 43(7), pp. 1606 - 1622
O’Haire, M.E., McKenzie, S.J., Beck, A.M., & Slaughter, V. (2013). Social behaviors increase in children with autism in the presence of animals compared to toys. PLoS ONE, Volume 8(2), pp. N/A
O’Haire, M.E., McKenzie, S.J., McCune, S., & Slaughter, V. (2013). Effects of animal-assisted activities with guinea pigs in the primary school classroom. Anthrozoös: A Multidisciplinary Journal of the Interactions of People and Animals, Volume 26(3), pp. 445 - 458
O’Haire, M.E., McKenzie, S.J., Beck, A.M., & Slaughter, V. (2015). Animals may act as social buffers: Skin conductance arousal in children with autism spectrum disorder in a social context. Developmental Psychobiology, Volume 57(5), pp. 584 - 595
O’Reilly, M.F., & Lancioni, G. (2000). Response covariation of escape-maintained aberrant behaviour correlated with sleep deprivation. Research in Developmental Disabilities. Volume 21, pp. 125 – 136
Oakley, M. (1991). Quoted in ‘The Hidden Handicap’ by Darby S. Times Educational Supplement (No.3930), October 25 1991, page 38
Ockelford, A. (2000). Music in the Education of Children with Severe or Profound Learning Difficulties: Issues in Current UK Provision, a New Conceptual Framework, and Proposals for Research. Psychology of Music, Volume 28, pp.197 - 217
Ockelford, A., Welch, G., & Zimmermann, S. (2002). Music education for pupils with severe or profound and multiple difficulties - current provision and future need. British Journal of Special Education, Volume 29(4), pp. 178 - 192
Ockelford, A. (2008). Music for Children and Young People with Complex Needs. Oxford: Oxford University Press.
Ockelford, A. (2009). Sounds of intent. Information Exchange, Volume 79, pp. 6 - 7
Ockelford, A. (2012). Songs Without Words: Exploring How Music Can Serve as a Proxy Language in Social Interaction with Autistic Children. In - R. MacDonald, G. Kreutz, & L. Mitchell (Eds.), Music, Health, and Well-being, pp. 289 - 323. Oxford: Oxford University Press.
Ockelford, A., & Markou, K. (2012). Music Education and Therapy for Children and Young People with Cognitive Impairments: Reporting on a Decade of Research. In R. MacDonald, G. Kreutz & L. Mitchell (Eds.), Music, Health, and Well-being, pp. 383 - 404. Oxford: Oxford University Press.
Ockelford, A., & Welch, G. (2012). Mapping Musical Development in Learners with the Most Complex Needs: The Sounds of Intent Project. In - G. McPherson & G. Welch (Eds.), The Oxford Handbook of Music Education, Volume 2, pp. 11 - 30. Oxford: Oxford University Press.
Ojemann, G. (1986). Brain mechanisms for consciousness and conscious experience. Canadian Psychology, Volume 27, pp. 158 – 168
Oldfield, A, & Adams, M. (1990). The Effects of Music Therapy on a Group of Profoundly Mentally Handicapped Adults. Journal of Mental Deficiency Research, Volume 34, pp. 107 - 124
Oliver, C., Murphy, G.H., & Corbett, J.A. (1987). Self injurious behaviour in people with mental handicap: a total population survey. Journal of Mental Deficiency Research. Volume 31. pp. 147 - 162
Oliver, C., & Head, D. (1990). Self-injurious behaviour in people with learning difficulties: Determinants and interventions. International Review of Psychiatry, Volume 2, 101 - 116
Oliver, C. (1991a). The application of analogue methodology to the functional analysis of challenging behaviour. In B. Remington (Ed.), The Challenge of Severe Mental Handicap: A Behaviour Analytic Approach. John Wiley and Sons, Chichester, pp. 97 - 118
Oliver, C. (1991b). Self-injurious Behaviour in People with Mental Handicap: Prevalence, Individual Characteristics and Functional Analysis, unpublished Ph.D. Thesis, University of London.
Oliver, C. (1993). Self-injurious behaviour: from response to strategy. In C. Kiernan (Ed.), Research to Practice? Implications of Research on the Challenging Behavour of People with Learning Disabilities. pp. 135 - 188. Kidderminster; British Institute of Learning Disabilities
Oliver C., McClintock K., Hall S., Smith M., Dagnan D. & Stenfert-Kroese B. (2002). Assessing the severity of challenging behaviour: psychometric properties of the challenging behaviour interview. Journal of Applied Research in Intellectual Disabilities, Volume 16, pp. 53 – 61
Oliver, C., Moss, J., Petty, J., Arron, K., Sloneem, J., & Hall, S. (2003). Self-injurious behaviour in Cornelia de Lange Syndrome A Guide for Parents and Carers. Coventry: Trident Communication Ltd.
Oliver, C. (2004). The neglect of psychological disorder in people with severe and profound intellectual disability. Journal of Intellectual Disability Research, Volume 48(4-5), pp. 360
Oliver, C., Sloneem, J., Hall, S., & Arron, K. (2009). Self‐injurious behaviour in Cornelia de Lange syndrome: 1. Prevalence and phenomenology. Journal of Intellectual Disability Research, Volume 53(7), pp. 575 - 589
Oliver, C., & Richards, C. (2010). Self-injurious behaviour in people with intellectual disability. Current Opinion in Psychiatry, Volume 23(5), pp. 412 – 416
Oliveros, P., Miller, L., Heyen, J., Siddall, G., & Hazard, S. (2011). A musical improvisation interface for people with severe physical disabilities. Music and Medicine, Volume 3(3), pp. 172 - 181
Olney, M.F. (2001). Communication strategies of adults with severe disabilities: Supporting self-determination. Rehabilitation Counseling Bulletin. Volume 44 (2), pp. 88 - 91
Olsson, C. (2004). Dyadic interaction with a child with multiple disabilities: A system theory perspective on communication. Augmentative and Alternative Communication, Volume 20(4), pp. 228 - 242
Orita, M., Hayashida, N., Shinkawa, T., Kudo, T., Koga, M., Togo, M., Katayama S, Hiramatsu K, Mori S, & Takamura, N. (2012). Monitoring the autonomic nervous activity as the objective evaluation of music therapy for severely and multiply disabled children. The Tohoku Journal of Experimental Medicine, Volume 227(3), pp. 185 - 189
Orelove, F.P., & Sobsey, D. (1987). Educating children with multiple disabilities: A transdisciplinary approach. Baltimore: Paul H. Brookes
Ottenbacher, K. (1982). Sensory Integration Therapy: Affect or Effect? American Journal of Occupational Therapy, Volume 36(9), pp. 571 - 578
Ottenbacher, K., & Short, M.A. (1985). Sensory integrative dysfunction in children: A review of theory and treatment. Advances in Developmental and Behavioral Pediatrics, Volume 6, pp. 287 – 329
Ouvry, C. (1987). Educating Children with Profound Handicaps. British Institute of Mental Handicap, Kidderminster
Oviedo, G.R., Travier, N., & Guerra-Balic, M. (2017). Sedentary and physical activity patterns in adults with intellectual disability. International Journal of Environmental Research and Public Health, Volume 14(9), 14 pages
Owen, M.T., Ware, A.M., & Barfoot, B. (2000). Caregiver-mother partnership behavior and quality of caregiver-child and mother-child interactions. Early Childhood Research Quarterly, Volume 15, pp. 413 – 428
Owens, T.J., Mortimer, J.T & Finch, M.D. (1996) Self determination as a source of self esteem in adolescence. Social Forces, Volume 74 (4) pp. 1377 - 1404
Pace, G.M., Ivancic, M.T., Edwards, G.L., Iwata, B.A., & Page, T.J. (1985). Assessment of stimulus preference and reinforcer value with profoundly retarded individuals. Journal of Applied Behavior Analysis, Volume 18, pp. 249 – 255
Pagliano, P. (1998). Multi-sensory environment: an open-minded space. British Journal of Visual Impairment. Volume 16(3), pp. 105 - 109
Pagliano, P. (2001). Using a Multisensory Environment: A Practical Guide for Teachers. David Fulton
Pagliano, P. (2007). Where next for multisensory environments? Insight. Volume 10, pp. 36 - 38
Pagliano, P., & Cook, J. (2007). Understanding and using multisensory environments. Insight, Volume 11, pp. 30 - 31
Pagliano, P. (2007). Pleasure, happiness and learning in the multisensory environment. Insight. Volume 12, pp. 32 - 33
Pagliano, P. (2012). The Multisensory Handbook: A guide for children and adults with sensory learning disabilities. Routledge
Palmer, S.B. (2010). Self-determination: A life-span perspective. Focus on Exceptional Children, Volume 42 (6), pp. 1 – 16
Palmer, S.B., Wehmeyer, M.L., Shogren, K.A., Williams-Diehm, K., & Soukup, J. (2012). An evaluation of the Beyond High School model on the self-determination of students with intellectual disability. Career Development for Exceptional Individuals, Volume 35(2), pp. 76 – 84
Para-Cremer, J.A. (2008). The effects of staff training on the level of engagement with individuals with developmental disabilities within two day-habilitation settings. Masters thesis, University of Kansas
Paradiso, S., Andreasen, N.C., O'leary, D.S., Arndt, S., & Robinson, R.G. (1997). Cerebellar size and cognition: correlations with IQ, verbal memory and motor dexterity. Cognitive and Behavioral Neurology, Volume 10(1), pp. 1 - 8
Parham, L.D., & Mailloux, Z. (2005). Sensory integration. In J. Case-Smith, A.S. Allen, & P.N. Pratt (Eds.), Occupational Therapy for Children (5th ed., pp. 356 – 411). St. Louis, MO: Mosby.
Parham, L.D., Cohn, E.S., Spitzer, S., Koomar, J.A., Miller, L.J., Burke, J.P., Brett-Green, B., Mailloux, Z., May-Benson, T.A., Smith Roley, S., Schaaf, R.C., Schoen, S.A., & Summerset, C.A. (2007). Fidelity in sensory integration intervention research. American Journal of Occupational Therapy, Volume 61, pp. 216 – 227
Parsons, M.B., & Reid, D.H. (1990). Assessing food preferences among persons with profound mental retardation: Providing opportunities to make choices. Journal of Applied Behavior Analysis, Volume 23, pp. 183 - 195
Parsons, M.B., & Reid, D.H. (1993). Evaluating and improving residential treatment during group leisure situations: A program replication and refinement. Research in Developmental Disabilities, Volume 14(1), pp. 67 - 85
Parsons, M.B., Reid, D.H., & Green, C.W. (1993). Preparing direct service staff to teach people with severe disabilities: A comprehensive evaluation of an effective and acceptable training program. Behavioral Residential Treatment, Volume 8(3), pp. 163 - 185
Parsons, M.B., & Reid, D.H. (1995). Training residential supervisors to provide feedback for maintaining staff teaching skills with people who have severe disabilities. Journal of Applied Behavior Analysis, Volume 28(3), pp. 317 - 322
Parsons, M.B., Harper, V.N., Jensen, J.M., & Reid, D.H. (1997). Assisting older adults with severe disabilities in expressing leisure preferences: A protocol for determining choice-making skills. Research in Developmental Disabilities, Volume 18, pp. 113 – 126
Parsons, M.B., Reid, D.H., & Green, C.W. (1998). Identifying work preferences prior to supported work for an individual with multiple severe disabilities including deaf-blindness. Journal of the Association for Persons with Severe Handicaps, Volume 23, pp. 329 – 333
Parsons, M.B., Rollyson, J.H., & Reid, D.H. (2004). Improving day-treatment services for adults with severe disabilities: a norm-referenced application of outcome management. Journal of Applied Behavior Analysis, Volume 37(3), pp. 365 - 377
Parsons, M.B., Reid, D.H., Towery, D., & Darden, M. (2008). Remediating minimal progress on teaching programs by adults with severe disabilities in a congregate day setting. Behavior Analysis in Practice, Volume 1(2), pp. 59 - 67
Parsons, M.B., Rollyson, J.H., & Reid, D.H. (2012). Evidence-based staff training: A guide for practitioners. Behavior Analysis in Practice, Volume 5(2), pp. 2 - 11
Parsons, R., Reid, D., Reynolds, J., & Bumgarner, M. (1990). Effects of chosen versus assigned jobs on the work performance of persons with severe handicaps. Journal of Applied Behavior Analysis, Volume 23, pp. 253 – 258
Parush, S., Kaitz, M., Sohmer, H., & Steinberg, A. (1991).Electrophysiological and behavioral correlates of tactile defensiveness. Paper presented at the national conference of the American Occupational Therapy Association, Cincinnati, OH.
Parush, S., Sohmer, H., Steinberg, A. & Kaitz, M. (2007). Somatosensory function in boys with ADHD and tactile defensiveness. Physiology & Behavior, Volume 90(4), pp. 553 - 558
Pase, M.P., Himali, J.J., Beiser, A.S., Aparicio, H.J., Satizabal, C.L., Vasan, R.S., Seshadri, S., & Jacques, P.F. (2017). Sugar and Artificially Sweetened Beverages and the Risks of Incident Stroke and Dementia: A Prospective Cohort Study. Stroke. Volume 48(5). pp. 1139 - 1146
Pase, M.P., Himali, J.J., Jacques, P.F., DeCarli, C., Satizabal, C.L., Aparicio, H., Vasan, R.S., Beiser, A.S., & Seshadri, S. (2017). Sugary beverage intake and preclinical Alzheimer's disease in the community. Alzheimer's & Dementia. Volume 13(9). pp. 955 – 964
Patterson, F.G. (1978a). The gestures of a gorilla: language acquisition in another pongid. Brain and Language, Volume 5, pp. 72 - 97
Patterson, F.G. (1978b). Conversations with a gorilla. National Geographic. Volume 154(4), pp. 438 - 465
Patterson, F.G. (1978c). Human communication with gorillas. In - The spirit of enterprise, Stone, G. (Ed.), pp. 182 - 186. San Francisco: Freeman
Patterson, F.G. (1979a). Linguistic capabilities of a lowland gorilla. Unpublished doctoral dissertation
Patterson, F.G. (1979b). Linguistic capabilities of a lowland gorilla. In - Language intervention from ape to child. Schiefelbusch, R. & Hollis, J. (Eds.), pp. 325 - 356. Baltimore: University Park Press
Patterson, F.G. (1980a). Innovative uses of language by a gorilla: A case study. In - Children's Language, Volume 2. Nelson, K. (Ed.), pp. 497 - 561. New York: Gardner Press
Patterson, F.G. (1980b). In search of man: Experiments in primate communication. Michigan Quarterly Review. Volume 19, pp. 94 - 114
Patterson, F.G. (1981a). Can an ape create a sentence? Some affirmative evidence. Science, Volume 211, pp. 86 - 87
Patterson, F.G. (1981b). Ape language. Science, Volume 211: pp. 86 - 87
Patterson, F.G., & Linden, E. (1981). The education of Koko. New York: Holt, Reinhart and Winston
Patterson, F.G. (1985a). Direct-mail funding solicitation letter. Washington: The Gorilla Foundation
Patterson, F.G. (1985b). Koko's kitten. New York: Scholastic
Patterson, F.G. (1987). Koko's story. New York: Scholastic
Pavlides, M. (2008). Animal-assisted Interventions for Individuals with Autism. London: Jessica Kingsley Publishers.
Pawson, C., Gardner, M.R, Doherty, S., Martin, L., Soares, R., Edmonds, C.J. (2013). Drink Availability is Associated with Enhanced Examination Performance in Adults. Psychology Teaching Review. Volume 19. pp. 57 - 66
Pease, L. (2008). Curriculum success for learners with complex needs. Insight. Volume 13, pp. 10 - 13
Pechacek, T.F., Bell, K.F., Cleland, C.C., Baum, C., & Boyle, M. (1973). Self-recognition in profoundly retarded males, Bulletin of the Psychonomic Society. Volume 1, pp. 328 - 330
Pedersen, L., Parlar, S., Kvist, K., Whiteley, P., & Shattock, P. (2014). Data mining the ScanBrit study of a gluten-and casein-free dietary intervention for children with autism spectrum disorders: behavioural and psychometric measures of dietary response. Nutritional Neuroscience, Volume 17(5), pp. 207 - 213
Pellitteri, J. (2000). Music therapy in the special education setting. Journal of Educational and Psychological Consultation, Volume 11(3&4), pp. 379 - 391
Pennesi, C.M., & Klein, L.C. (2012). Effectiveness of the gluten-free, casein-free diet for children diagnosed with autism spectrum disorder: based on parental report. Nutritional Neuroscience, Volume 15(2), pp. 85 - 91
Perkins, E.A. (2007). Self- and proxy reports across three populations: Older adults, persons with Alzheimer’s disease, and persons with intellectual disabilities. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(1), pp. 1 - 10
Perretta, L. (2001). Brain Food. Hamlyn Publishers
Perrig, W.J., Hollenstein, M., & Oelhafen, S. (2009). Can we improve fluid intelligence with training on working memory in persons with intellectual disabilities. Journal of Cognitive Education and Psychology, Volume 8(2), pp. 148 - 164
Perry, M. (2003). Relating improvisational music therapy with severely and multiply disabled children to communication development. Journal of Music Therapy, Volume 40(3), pp. 227 - 246
Peterson, J.J., Janz, K.F., & Lowe, J.B. (2008). Physical activity among adults with intellectual disabilities living in community settings. Preventive Medicine, Volume 47, pp. 101 – 106
Petkova, V.I., & Ehrsson, H.H. (2008). If I were you: Perceptual illusion of body swapping. PloS one, Volume 3(12), e3832
Petri, N.M., Dropulić, N., & Kardum, G. (2006). Effects of Voluntary Fluid Intake Deprivation on Mental and Psychomotor Performance. Croatian Medical Journal. Volume 47(6). pp. 855 – 861
Petry, K., Maes, B., & Vlaskamp, C. (2001). Developing a procedure for evaluating quality of life for people with profound and multiple disabilities. Tizard Learning Disability Review, Volume 6(2), pp. 45 - 48
Petry, K., Maes, B., & Vlaskamp, C. (2005). Domains of quality of life of people with profound multiple disabilities: the perspective of parents and direct support staff, Journal of Applied Research in Intellectual Disabilities, Volume 18(1), pp. 35 – 46
Petry, K., & Maes, B. (2006). Identifying expressions of pleasure and displeasure by persons with profound and multiple learning disabilities Journal of Intellectual & Developmental Learning Disability, Volume 31(1), pp. 28 – 38
Petry, K., Maes, B., & Vlaskamp, C. (2007a). Operationalizing quality of life for people with profound multiple disabilities: a Delphi study. Journal of Intellectual Disability Research, Volume 51(5), pp. 334 - 349
Petry, K., Maes, B., & Vlaskamp, C. (2007b). Support characteristics associated with the quality of life of people with profound intellectual and multiple disabilities: The perspective of parents and direct support staff. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(2), pp. 104 - 110
Petry, K., & Maes, B., & Vlaskamp, C. (2007c). Description of the support needs of people with profound multiple disabilities using the 2002 AAMR system: An overview of literature. Education and Training in developmental Disabilities, pp. 130 - 143
Petry, K., Maes, B., & Vlaskamp, C. (2007d). Service features associated with quality of support for people with profound intellectual disability and complex health care needs: The perspective of parents and direct support staff. Journal of Policy and Practice in Intellectual Disabilities, Volume 4, pp. 104 - 110
Petry, K., Maes, B., & Vlaskamp, C. (2009). Measuring the quality of life of people with profound multiple disabilities using the QOL-PMD: First results. Research in Developmental Disabilities, Volume 30(6), pp. 1394 - 1405
Pfeiffer, B., & Kinnealey, M. (2003). Treatment of sensory defensiveness in adults. Occupational Therapy International, Volume 10, pp. 175 – 184
Philippi, C.L., Feinstein, J.S., Khalsa, S.S., Damasio, A., Tranel, D., Landini, G., Williford, K., & Rudrauf, D. (2012) Preserved Self-Awareness following Extensive Bilateral Brain Damage to the Insula, Anterior Cingulate, and Medial Prefrontal Cortices. PLoS ONE, Volume7(8): e38413.
Piaget, J. (1952). The origins of intelligence in children. New York: Norton
Piazza, C.C., Fisher, W.W., & Kahng, S.W. (1996). Sleep patterns in children and young adults with mental retardation and severe behaviour disorders. Developmental Medicine and Child Neurology. Volume 38, pp. 335 – 344
Pierson, M.R., Carter, E.W., Lane, K.L., & Glaeser, B.C. (2008). Factors influencing the self-determination of transition-age youth with
high-incidence disabilities. Career Development for Exceptional Individuals, Volume 31(2), pp. 115 – 125
Pinkney, L. (2001). Multisensory environments. Eye Contact, Volume 31, pp. 24 - 26
Place, K., & Hodge, S.R. (2001): Social Inclusion of Students With Physical Disabilities in General Physical Education: A Behavioral Analysis. Adapted Physical Activity Quarterly, Volume 18; pp, 389 - 404
Plotnik, J.M., de Waal, F.B.M., Moore, D., & Reiss, D. (2010). Self-recognition in the Asian elephant and future directions for cognitive research with elephants in zoological settings. Zoo Biology, Volume 29, pp. 179 – 191
Podboy, J.W., & Mallory, W.A. (1977). Caffeine reduction and behavior change in the severely retarded. Mental Retardation, Volume 15(6), pp. 40
Polatajko, H. J., Law, M., Miller, J., Schaffer, R., & Macnab, J. (1991). The effect of a sensory integration program on academic
achievement, motor performance, and self-esteem in children identified as learning disabled: Results of a clinical trial. Occupational Therapy
Journal of Research, Volume 11, pp. 155 - 176
Polatajko, H.J., Kaplan, B., & Wilson, B. (1992). Sensory integration treatment for children with learning disabilities: Its status 20 years
later. Occupational Therapy Journal of Research, Volume 12, pp. 323 - 341
Polednak, A. (1977). Post-mortem neuropathology in a mentally retarded population. The Lancet, Volume 309(8009), pp. 492 - 493
Poppes, P., van der Putten, A.A., & Vlaskamp, C. (2010). Frequency and severity of challenging behaviour in people with profound intellectual and multiple disabilities. Research in Developmental Disabilities, Volume 31(6), pp. 1269 - 1275
Poppes, P., van der Putten, A.A., & Vlaskamp, C. (2014). Addressing challenging behaviour in people with profound intellectual and multiple disabilities: Analyzing the effects of daily practice. Journal of Policy and Practice in Intellectual Disabilities, Volume 11(2), pp. 128 – 136
Porter, J., & Lacey, P. (1999). What Provision for Pupils with Challenging Behavior? A Report of a Survey of Provision and Curriculum Provided for Pupils with Learning Difficulties and Challenging Behaviour. British Journal of Special Education. Volume 26(1), pp. 23 - 28
Porter, J., Ouvry, C., Morgan, M., & Downs, C. (2001). Interpreting the communication of people with profound and multiple learning difficulties. British Journal of Learning Disability, Volume 29(1), pp. 12 - 16
Postman, N. (1969). Teaching as a Subversive Activity. Delacorte Press
Powers, L.E., Geenen, S., Powers, J., Pommier-Satya, S., Turner, A., Dalton, L., & Swand, P. (2012). My life: Effects of a longitudinal, randomized study of self-determination enhancement on the transition outcomes of youth in foster care and special education. Children and Youth Services Review, Volume 34, pp. 2179 – 2187
Price, A. (1977). Nationally Speaking - Sensory integration in occupational therapy. American Journal of Occupational Therapy. Volume 31, pp. 287 - 289
Prior, H., Schwarz, A., & Guentuerkuen, O. (2008). Mirror-induced behavior in the magpie (Pica pica): evidence of self-recognition. PLoS
Biology, Volume 6, pp. 1642 – 1650
Prior, M., Minnes, P., Coyne, T., Golding, B., Hendy, J., & McGillivary, J. (1979). Verbal interactions between staff and residents in an institution for the young mentally retarded. Mental Retardation. Volume 17, pp. 65 – 69
Pross, N., Demazieres, A., Girard, N., Barnouin, R., Santoro, F., Chevillotte, E., Klein, A, & Le, B.L. (2013) Influence of progressive
fluid restriction on mood and physiological markers of dehydration in women. British Journal of Nutrition. Volume 109. pp. 313 - 321
Pross, N., Demazieres, A., Girard, N., Barnouin, R., Metzger, D., Klein, A., Perrier, E., & Guelinckx, I. (2014). Effects of changes in
water intake on mood of high and low drinkers. PLoS One. Volume 9: e94754
Psaltopoulou, D., Micheli, M., & Kavardinas, N. (2012). Music Therapy Enhances Perceptive and Cognitive Development in People with
Disabilities. A Quantitative Research. Proceedings of the 12th International Conference on Music Perception and Cognition and the 8th Triennial Conference of the European Society for the Cognitive Sciences of Music, July 23 - 28, 2012, Thessaloniki, Greece. pp. 824 - 833
Pugh, D. (2011a). Water and Educating Your Child. http://braincompatibleeducation.com/
Pugh, D. (2011b). The Owner's Guide to the Teenage Brain. BookPal
Pulsifer, M.B. (1996). The neuropsychology of mental retardation. Journal of the International Neuropsychological Society, Volume 2(2), pp. 159 - 176
Quest For Learning (2007). Guidance Booklet. The Council for Curriculum, Examinations & Assessment
Quest For Learning (2009): Guidance and Assessment Materials: Profound and Multiple Learning Difficulties. Northern Ireland Curriculum
Questad, K. & Cullinen, T. (1987). A reinforcer driven, data base rehabilitation program for severely brain injured adults. Archives of Physical Medicine and Rehabilitation, Volume 68, pp. 674
Quigley, S.P., & Kretchmer, R.E. (1982). The education of deaf children: Issues, Theory, and Practice. London: Edward Arnold
Quine, L. (1991). Sleep problems in children with mental handicap. Journal of Mental Deficiency Research. Volume 35(4), pp. 269 – 290
Quine, L. & Wade, K. (1991). Sleep Problems In Children with Severe Learning Difficulties: An Examination and An Intervention Trial. Final Report to Rowntree Foundation, University of Kent, Canterbury
Quine, L. (1992). Severity of sleep problems in children with severe learning difficulties: description and correlates. Journal of Community & Applied Social Psychology, Volume 2(4), pp. 247 - 268
Quine, L. (2001). Sleep problems in primary school children: comparison between mainstream and special school children. Child: Care, Health and Development, Volume 27(3), pp. 201 - 221
Quine, N., & Pahl, J. (1985). Examining the causes of stress in families with mentally handicapped children. British Journal of Social Work, Volume 15, pp. 501 - 517
Quine, N., & Pahl, J. (1991). Stress and coping in mothers caring for a child with severe learning difficulties: A test of Lazarus's transactional model of coping. Journal of Communityand Applied Psychology, Volume 1, pp. 57 - 70
Qureshi, H. (1992). Young adults with learning difficulties and challenging behaviour: parents' views of services in the community. Social Work and Social Services Review, Volume 3, pp. 104 - 123
Qureshi, H., & Alborz, A. (1992). The epidemiology of challenging behaviour. Mental Handicap Research, Volume 5, pp. 130 - 145
Qureshi, H. (1993). Prevalence of challenging behaviour in adults. In I. Fleming & B. Stenfert Kroese (eds.), People with Learnign Disability and Severe Challenging Behaviour: New Developments in Services and Therapy. Manchester University Press
Qureshi, H. (1994). The size of the problem. In E. Emerson, P. McGill, & J. Mansell (Eds.), Severe Learning Disabilities and Challenging Behaviour: Designing HighQuality Services. London: Chapman and Hall.
Raab, M., & Dunst, C.J. (1997). Extended benefits of active learning for young children with severe disabilities. Presentation at the International Conference on Children with Special Needs, New Orleans, LA. November 1997
Raab, M., Dunst, C.J., Wilson, L.L., & Parkey, C. (2009). Early Contingency Learning and Child and Teacher Concomitant Social–Emotional Behavior, International Journal of Early Childhood Special Education, Volume 1 (1), pp. 1 -14
Rainey P.M.M. (2003). Relating improvisational music therapy with severely and multiply disabled children to communication development. Journal of Music Therapy, Volume 40(3), pp. 227 - 246
Rainforth, B., Giangreco, M.F., & Dennis, R. (1989). Motor skills. In - A. Ford, R. Schnorr, L. Meyer, L. Davern, J. Black, & P. Dempsey (Eds.), Syracuse community-referenced curriculum guide for students with moderate and severe disabilities (pp. 211 - 230). Baltimore, MD: Paul H. Brookes.
Rajagopalan, S.S., Dhall, A., & Goecke, R. (2013). Self-stimulatory behaviours in the wild for autism diagnosis, IEEE International Conference on Computer Vision. Australian National University, 1-8 December. New York: Institute of Electrical and Electronics Engineers.
Rajala, A.Z., Reininger, K.R., Lancaster, K.M., & Populin, L.C. (2010). Rhesus monkeys (Macaca mulatta) do recognize themselves in the mirror: implications for the evolution of self-recognition. PLoS 2 ONE. Volume 5: e12865
Ramachandran, V.S. (1994). Phantom limbs, neglect syndromes, repressed memories, and Freudian psychology. International Review of Neurobiology, Volume 37, pp. 291 - 333
Ramachandran, V.S. (1996). The Brain's Potential for Growth and Change. UCSD Decade of the Brain Symposium, October 21, 1996
Ramachandran, V.S., & Blakeslee, S. (1998). Phantoms in the Brain: Probing the Mysteries of the Human Mind. William Morrow publishers
Ramachandran, V.S., & Hirstein, W. (1998). The Perception of Phantom Limbs: The D.O. Hebb Lecture, Brain, Volume 121 (1998), pp. 1603 – 1630
Ramachandran, V.S. (2002). Encyclopedia of the Human Brain. Academic Press, San Diego.
Ramachandran, V.S. (2003). The Emerging Mind. BBC/Profile Books, London
Ramachandran, V.S. (2004). A Brief Tour of Human Consciousness: From Impostor Poodles to Purple Numbers. New York: Pi Press.
Ramachandran, V.S. (2005). Plasticity and functional recovery in neurology. Clinical medicine, Volume 5(4), pp. 368 - 373
Ramachandran, V.S., & Oberman, L.M. (2006). Broken mirrors: a theory of autism. Scientific American, Volume 295(5), 62 - 69
Ramachandran, V.S., & Rogers-Ramachandran, D. (2007). It’s All Done with Mirrors. Scientific American Mind, Volume 18(4), pp. 16 - 18
Ramachandran, V.S., & Altschuler, E. (2009). The Use of Visual Feedback, in particular Mirror Visual Feedback, in Restoring Brain Function, Brain, Volume 132(7), pp. 1693 – 1710
Ramachandran, V.S. (2011). The Tell-Tale Brain: A Neuroscientist's Quest for What Makes Us Human. New York: W. W. Norton & Company
Rapoff, M.A., Altman, K., & Christophersen, E.R. (1980). Suppression of self-injurious behaviour: Determining the least restrictive alternative. Journal of Mental Deficiency Research, Volume 24, pp. 37 - 46
Reader, M. (2011). Setting Students up for Success Through Self-Awareness and Self-Advocacy. Foothills academy
Realon, R.E., Bligen, R.A., La Force, A., Helsel, W.J., & Goldman, V. (2002). The effects of the positive environment program (PEP) on the behaviors of adults with profound cognitive and physical disabilities. Behavioral Intervention, Volume 17(1), pp. 1 - 13
Redding, H. (1999). Stimulate the senses. Special! Summer 1999, pp. 16 - 19
Redefer, L.A., & Goodman, J.F. (1989). Brief Report: Pet Facilitated Therapy With Autistic Children. Journal of Autism and Developmental Disorders. Volume 19(3), pp. 461 - 467
Reed, L. (1991). Games with a New Look for All Ability Levels. The Spastics Society, Meldreth, Herts.
Rees, K. (2014). Using Innovative Approaches to Addressing Challenging Behaviours. PMLD Link, Volume 26(3), Issue 79, pp. 21 - 23
Rees, M. (1995). Making sense of marking space: Researching art therapy with people who have severe learning difficulties. In C. Lee & A. Gilroy (Eds.) Art and music therapy research. London: Routledge.
Rees, M. (1998). Drawing on difference: Art therapy with people who have learning difficulties. London: Routledge.
Reese, G.M., & Snell, M.E. (1991). Putting on and Removing Coats and Jackets: The Acquisition and Maintenance of Skills by Children with Severe Multiple Disabilities. Education and Training in Mental Retardation. Volume 26(4), pp. 398 - 410
Reese, R.M. (1997). Biobehavioral analysis of self-injurious behavior in a person with profound handicaps. Focus on Autism and Other Developmental Disabilities, Volume 12(2), pp. 87 - 94
Reichelt, K.L., & Knivsberg, A.M. (2009). The possibility and probability of a gut-to-brain connection in autism. Annals of Clinical Psychiatry, Volume 21(4), pp. 205 - 211
Reichle, J., Sigafoos, J., & Piche, L. (1989). Teaching an adolescent with blindness and severe disabilities: A correspondence between requesting and selecting preferred objects. Journal of the Association for Persons with Severe Handicaps, Volume 14, pp. 75 – 80
Reichle, J. (1991a). Defining Decisions, In - Reichle, J., York, J., & Sigafoos, J. (Eds.), Implementing Augmentative and Alternative Communication: Strategies for Learners with Severe Disabilities. Paul H. Brookes Publishing
Reichle, J. (1991b). Developing communicative exchanges, In - Reichle, J., York, J., & Sigafoos, J. (Eds.), Implementing Augmentative and Alternative Communication: Strategies for Learners with Severe Disabilities. Paul H. Brookes Publishing
Reichle, J., & Sigafoos, J. (1991a). Establishing an initial repertoire of requesting In - Reichle, J., York,J., & Sigafoos,J. (Eds.), Implementing Augmentative and Alternative Communication: Strategies for Learners with Severe Disabilities. Paul H. Brookes Publishing
Reichle, J., & Sigafoos, J. (1991b). Establishing spontaneity and generalization In - Reichle, J., York,J., & Sigafoos,J. (Eds.), Implementing AAC: Strategies for learners with severe disabilities, pp. 157 - 171, Paul H. Brookes Publishing Co.
Reichle, J., & Sigafoos, J. (1991c). Bringing communicative behavior under the control of the appropriate stimuli In - Reichle, J., York,J., & Sigafoos,J. (Eds.), Implementing AAC: Strategies for learners with severe disabilities, pp. 193 - 213, Paul H. Brookes Publishing Co.
Reichle, J., York,J., & Sigafoos,J. (Eds.) (1991). Implementing Augmentative and Alternative Communication: Strategies for Learners with Severe Disabilities. Paul H. Brookes Publishing
Reid, D.H., & Parsons, M.B. (1991). Making choice a routine part of mealtimes for persons with profound mental retardation. Behavioral Residential Treatment, Volume 6, pp. 249 - 261
Reid, D.H., Phillips, J.F., & Green, C.W. (1991). Teaching persons with profound multiple handicaps: A review of the effects of behavioral research. Journal of Applied Behavior Analysis, Volume 24(2), pp. 319 - 336
Reid, D.H., Everson. J.M., & Green, C.W. (1999). A systematic evaluation of preferences identified through person-centred planning for people with profound multiple disabilities. Journal of Applied Behavior Analysis, Volume 32(4), pp. 467 – 477
Reid, D.H., Parsons, M.B., & Green, C.W. (2001). Evaluating the functional utility of congregate day treatment activities for adults with severe disabilities. American Journal on Mental Retardation, Volume 106(5), pp. 460 - 469
Reid, D.H., Green, C.W., & Parsons, M.B. (2003). An outcome management program for extending advances in choice research into choice opportunities for supported workers with severe multiple disabilities. Journal of Applied Behavior Analysis, Volume 36(4), pp. 575 – 578
Reimer, A., & Siemonsma-Boom, M. (2013). Motoriek en visuele beperkingen [Motoric and visual impairments]. In - R. van Empelen, R. Nijhuis-van der Sanden, & A. Hartman (Eds.), Kinderfysiotherapie . pp. 639 – 659. Amsterdam, the Netherlands: Reed Business Education.
Reisman, J. (1993). Using a sensory integrative approach to treat self-injurious behavior in an adult with profound mental retardation. American Journal of Occupational Therapy, Volume 47, pp. 403 – 411
Reiss, D., & Marino, L. (2001). Mirror self-recognition in the bottle-nose dolphin: a case of cognitive convergence. Proceedings of the National Academy of Sciences of the United States of America, Volume 98, pp. 5937 – 5942
Reiss S. & Rojahn J. (1993). Joint occurrence of depression and aggression in children and adults with mental retardation. Journal of Intellectual Disability Research, Volume 37, pp. 287 – 294
Remington, B. (1996). Assessing the occurrence of learning in children with profound intellectual disability: A conditioning approach. International Journal of Disability, Development and Education, Volume 43(2), pp. 101 - 118
Repp, A.C., Felce, D., & de Kock, U. (1987). Observational studies of staff working with mentally retarded persons: a review. Research in Developmental Disabilities, Volume 8(2), pp. 331 - 350
Repp, A.C., Felce, D., & Barton, L.E. (1988). Basing the treatment of stereotypic and self-injurious behaviors on hypotheses of their causes. Journal of Applied Behavior Analysis, Volume 21, pp. 281 - 289
Resman, M.H. (1981). Effect of sensory stimulation on eye contact in a profoundly retarded adult. American Journal of Occupational Therapy, Volume 35, pp. 31 - 35
Reynolds, A. (2012). Pets as therapy: where is the evidence? Nursing & Residential Care, Volume 14(9), pp. 478 - 481
Reynolds, F. (2002). A survey of opportunities and barriers to creative leisure activity for people with learning disabilities. British Journal of Learning Disabilities, Volume 30 (2), pp. 63 - 67
Rhodes, J., & Hewett, D. (2010). The Human Touch: physical contact and making a social world available for the most profoundly disabled. PMLD Link. Volume 22(2), pp. 11 - 14
Richmond, G., Schroder, S.R., & Bickel, W. (1986). Tertiary prevention of attrition related to self-injurious behaviours. In K.D. Gadow (Ed.), Advances in Learning and Behavioural Disabilities, Volume 5. London: JAI Press
Rickson, D.J. (1997). The music therapist working in New Zealand schools with children who have disabilities. Annual Journal of the New Zealand Society for Music Therapy, 1997 edition, pp. 44 - 53
Rickson, D.J. (2001). A Music Therapy Practice in Special Education Settings in New Zealand. New Zealand Society for Music Therapy, 2001 edition, pp. 26 - 47
Rickson, D.J. (2006). Reflections on the nature of relationship in brief music therapy encounters with children who have developmental difficulties. New Zealand Journal of Music Therapy, Volume 4, pp. 23 - 45
Rickson, D.J. (2007). Music Therapy in Special Education: Do We Need More Evidence? A response to K. McFerran & J. Stephenson. British Journal of Music Therapy, Volume 21(1), pp. 28 - 29
Rickson, D.J., & McFerran K. (2007). Music Therapy in Special Education: Where are we now? New Zealand Journal of Educational Practice, Volume 8(1), pp. 40 - 47
Rickson, D.J. (2008). The potential role of music in special education (The Promise) - New Zealand music therapists consider collaborative consultation. New Zealand Journal of Music Therapy, Volume 6, pp. 76 - 97
Rickson, D.J. (2010). The development of a music therapy school consultation protocol for students with high or very high special educational needs. Thesis: Doctor of Philosophy in Music. New Zealand School of Music, Wellington,
Rimmer, J.H., Braddock, D., & Fujiura, G. (1993). Prevalence of obesity in adults with mental retardation: implications for health promotion and disease prevention. Mental Retardation, Volume 31(2), pp. 105 - 110
Rimmer, J.H. (1994). Fitness and rehabilitation programs for special populations. McGraw-Hill Humanities, Social Sciences & World Languages.
Rimmer, J.H., Braddock, D., & Marks, B. (1995). Health characteristics and behaviors of adults with mental retardation residing in three living arrangements. Research in Developmental Disabilities, Volume16(6), pp. 489 - 499
Rimmer, J.H., & Wang, E. (2005). Obesity prevalence among a group of Chicago residents with disabilities. Archives of Physical Medicine and Rehabilitation, Volume 86(7), pp. 1461 - 1464
Rimmer, J.H., & Yamaki, K. (2006). Obesity and intellectual disability. Developmental Disabilities Research Reviews, Volume 12(1), pp. 22 - 27
Rimmer, J.H., Yamaki, K., Lowry, B.M., Wang, E., & Vogel, L.C. (2010). Obesity and obesity‐related secondary conditions in adolescents with intellectual/developmental disabilities. Journal of Intellectual Disability Research, Volume 54(9), pp. 787 - 794
Rincover, A., Newsom, C.D., Lovaas, 0.I., & Koegel, R.L. (1977). Some motivational properties of sensory reinforcement in psychotic children. Journal of Experimental Child Psychology, Volume 24, pp. 312 - 323
Rincover, A. (1978). Sensory extinction: a procedure for eliminating self-stimulatory behavior in developmentally disabled children. Journal of Abnormal Child Psychology, Volume 6(3), pp. 229 - 310
Rincover, A., Cook, R., Peoples, A., & Packard, D. (1979). Sensory extinction and sensory reinforcement principles for programming multiple adaptive behavior change. Journal of Applied Behavior Analysis, Volume 12(2), pp. 221 - 233
Rincover, A., Newsom, C.D., & Carr, E.G. (1979). Using sensory extinction procedures in the treatment of compulsive like behavior of developmentally disabled children. Journal of Consulting and Clinical Psychology, Volume 47(4), pp. 695 - 701
Rincover, A. (1981). How to Use Sensory Extinction. Pro Ed
Rincover, A., & Devaney, J. (1982). The application of sensory extinction procedures to self-injury. Analysis and Intervention in Developmental Disabilities, Volume 2, pp. 67 - 81
Risley, T.R. (1996). Get a life! Positive behavioral intervention for challenging behaviour through life arrangement and life coaching. In L.K. Koegel, R.L. Koegel, & G. Dunlap (Eds.), Positive behavioral support : including people with difficult behavior in the community. Baltimore: Brookes
Ritchie, F. (1993). Opening Doors: The Effects of Music Therapy with People who have Severe Learning Difficulties and Display Challenging Behaviour. In Heal, M., & Wigram, T., (Eds.) Music Therapy in Health and Education, London: Jessica Kingsley.
Roberts, M. (2001). Off-task behavior in the classroom: Applying FBA and CBM. National Association of School Psychologists and The Guidance Channel (www.guidancechannel.com)
Roberts, S., & Rues, J. (1999). Using cueing strategies and behavior state analysis to increase alertness and responsiveness among infants with severe cognitive and multiple disabilities. (Model Demonstration Project, H324M990015) Washington, DC: U.S. Department of Education.
Roberts, S., Arthur-Kelly, M., Foreman, P., & Pascoe, S. (2005). Educational approaches for maximizing arousal in children with multiple and severe disability: New directions for research and practice in early childhood contexts. Pediatric Rehabilitation, Volume 8(2), pp. 88 - 91
Robertson, J., Emerson, E., Gregory, N., Hatton, C., Turner, S., Kessissoglou, S., & Hallam, A. (2000). Lifestyle related risk factors for poor health in residential settings for people with intellectual disabilities. Research in Developmental Disabilities, Volume 21(6), pp. 469 – 486
Rochat, P. (2003). Five levels of self-awareness as they unfold early in life. Consciousness and Cognition, Volume 12, pp. 717 – 731
Rochat, P., Broesch, T., & Jayne, K. (2012). Social awareness and early self-recognition. Consciousness and Cognition, Volume 21, pp. 1491 - 1497
Rochefort, C., Gheusi, G., Vincent, J.D., & Lledo, P.M. (2002). Enriched Odor Exposure Increases the Number of Newborn Neurons in the Adult Olfactory Bulb and Improves Odor Memory. The Journal of Neuroscience, Volume 22(7). pp. 2679 – 2689
Rodin, J. & Langer, E.J. (1977). Long-Term Effects of a Control-Relevant Intervention with the Institutional Aged. Journal of Personality and Social Psychology, Volume 35, pp. 897 – 902
Rogers, B., Stratton, P., Victor, J., Kennedy, B., & Andres, M. (1992). Chronic regurgitation among persons with mental retardation: a need for combined medical and interdisciplinary strategies. American Journal of Mental Retardation. Volume 96, pp. 522 – 527
Rogers P.J., Kainth, A., & Smit, H.J. (2001). A drink of water can improve or impair mental performance depending on small differences in thirst. Appetite. Volume 36. pp. 57 - 58
Rojahn, J., & Sisson, L. (1990). Stereotyped behaviour. In Matson, J (Ed.), Handbook of Behaviour Modification with the Mentally Retarded. pp. 181 - 223. New York: Springer US
Rojahn, J. (1994). Epidemiology and topographic taxonomy of self-injurious behavior. In T. Thompson & D.B. Gray (eds.), Destructive Behavior in Developmental Disabilities: Diagnosis and Treatment, pp. 49 - 67. Thousand oaks: Sage
Rojahn, J., Matson, J.L., Lott, D., Esbensen, A.J., & Smalls, Y. (2001). The behaviour problems inventory: An instrument for the assessment of self-injury, stereotyped behavior, and aggression/destruction in individuals with developmental disabilities. Journal of Autism and Developmental Disorders, Volume 31(6), pp. 577 – 588
Rojahn, J., Schroeder, S., & Hoch, T. (2008). Self-Injurious Behaviour in Intellectual Disabilities. Oxford: Elsevier.
Rojahn, J., Rowe, E.W., Kasdan, S., Moore, L.,& van Ingen, D.J. (2011). Psychometric properties of the Aberrant Behaviour Checklist, the Anxiety, Depression and Mood Scale, the Assessment of Dual Diagnosis and the Social Performance Survey Schedule in adults with intellectual disabilities. Research in Developmental Disabilities, Volume 32, pp. 2309 - 2320
Rojahn, J., Barnard-Brak, L., Richman, D., Dotson, W., Medeiros, K., Wei, T., & Abby, L. (2012). Behavior Problems in Individuals with Cornelia de Lange Syndrome: Population-Specific Validation of the Behavior Problem Inventory-01. Journal of Developmental and Physical Disabilities, Volume 25, pp. 505 – 515
Rowland, C., & Schweigert, P. (1989). Tangible symbols: Symbolic communication for individuals with multisensory impairments. Augmentative and Alternative Communication, Volume 5(4), pp. 226 - 234
Rolandelli, P.S., & Dunst, C.J. (2003). Influences of hippotherapy on the motor and social-emotional behavior of young children with disabilities. Bridges, Volume 2(1), pp. 1 - 5
Rose, S., & Massey, P. (1993). Adventurous Outdoor Activities: An Investigation into the benefits of Adventure for Seven People with Severe Learning Difficulties. Mental Handicap Research. Volume 6. pp. 287 - 301
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton, NJ: Princeton University Press.
Ross E. & Oliver C. (2002). The relationship between levels of mood, interest and pleasure and challenging behaviour in adults with severe and profound intellectual disability. Journal of Intellectual Disability Research, Volume 42, pp. 191 – 197
Rokvic, V. (2007). The Meaning and Role of Touch with an Adult with Profound Learning Disability in Dance Movement Therapy, Unpublished MA dissertation, Goldsmith University
Rosenzweig, M.R., Krech, D., Bennett, E.L., & Diamond, M.C. (1962). Effects of environmental complexity and training on brain chemistry and anatomy: A replication and extension. Journal of Comparative and Physiological Psychology, Volume 55(4), pp. 429 - 437
Rosenzweig, M.R., & Bennett, E.L. (1972). Cerebral changes in rats exposed individually to an enriched environment. Journal of Comparative and Physiological Psychology, Volume 80(2), pp. 304 - 313
Rowland, C.M., & Schweigert, P. (1989). Tangible symbols: symbolic communication for individuals with multisensory impairments. Augmentative and Alternative Communication, Volume 6(4), pp. 226 - 234
Rowland, C.M., & Schweigert, P. (2000). Tangible symbols, tangible outcomes. Augmentative and Alternative Communication, Volume 16, pp. 61 - 78
Royeen, C.B. (1985). Domain specification of the construct tactile defensiveness. American Journal of Occupational Therapy, Volume 39, pp. 596 – 599
Royeen, C.B. (1986). The development of a touch scale for measuring tactile defensiveness in children. American Journal of Occupational Therapy, Volume 40, pp. 414 – 418
Royeen, C.B. (1987a). Redefining tactile defensiveness. Paper presented at the Tactile Defensiveness Treatment, Research and Theory Workshop, Boston.
Royeen, C.B. (1987b). TIP-Touch inventory for preschoolers: A pilot study. Physical & Occupational Therapy in Pediatrics, Volume 7, pp. 29 – 40
Royeen, C.B., Miller, L.J., & Fortune, J. (1987). An analysis of tactile defensiveness and measures of development in elementary school aged children. Paper presented at the research forum of the annual meeting of the American Occupational Therapy Association, Indianapolis.
Royeen, C.B., & Lane, S.J. (1991). Tactile processing and sensory defensiveness. In A.G. Fisher, E.A. Murray, & A.C. Bundy. (Eds.), Sensory Integration: Theory and Practice (pp. 108-136). Philadelphia: F. A. Davis.
Rues, J. (1986). Developing basic motor skills in infants and children with severe handicaps: An experimental analysis with implications for education and treatment. Final report. Kansas: Kansas University
Rusalova, M.N. (2005). Characteristics of inter-hemisphere interactions at different levels of consciousness. Neuroscience and Behavioral Physiology, Volume 35, pp. 821 – 827
Rusch, R.G., Hall, J.C., & Griffin, H.C. (1986). Abuse provoking characteristics of institutionalized mentally retarded individuals. American Journal of Mental Deficiency. Volume 90(6). pp. 618 - 624
Sacks, O. (1989). Seeing Voices. University of California press. Picador Edition (1991). ISBN 0-330-31716-4
Salmento, M., & Bambara, L.M. (2000). Teaching staff members to provide choice opportunities for adults with multiple disabilities. Journal of Positive Behavior Interventions, Voulme 2(1), pp. 12 - 21
Saloviita, T. (2000). The structure and correlates of self-injurious behavior in an institutional setting. Research in Developmental Disabilities, Volume 21, pp. 501 - 511
Salzen, E.A. (1998). Emotion and self-awareness, Applied Animal Behaviour Science, Volume 57, pp. 299 - 313
Sams, M.J., Fortney, E.V., & Willenbring, S. (2006). Occupational therapy incorporating animals for children with autism: A pilot investigation. The American Journal of Occupational Therapy, Volume 60(3), pp. 268 – 274
Samuel, J. (2001a). Intensive Interaction, Clinical Psychology Forum, Volume 148, pp. 22 - 25
Samuel, J. (2001b). Intensive Interaction in context, Tizard Learning Disability Review, Volume 6(3), pp. 25 - 30
Samuel, J., & Pritchard, M. (2001). The ignored minority: Meeting the needs of people with profound learning disability. Tizard Learning Disability Review, Volume 6(2), pp. 34 - 44
Samuel, J. (2003). An Evaluation of Intensive Interaction in Community Living Settings for Adults with Profound Learning Disability, DclinPsychol thesis, Open University/BPS.
Samuel, J., Nind, M., Volans, A. & Scriven, I. (2008) ‘An evaluation of Intensive Interaction in community living settings for adults with profound intellectual disabilities’, Journal of Intellectual Disabilities, Volume 12(2), pp.111 - 126
Sandiford, P.J. (1997). A positive Outlook on Challenging Behaviour. National Children's Bureau
Sandler, A.G., & Voogt, K. (2001). Vestibular stimulation: Effects on visual and auditory alertness in children with multiple disabilities. Journal of Developmental and Physical Disabilities, Volume 13(4), pp. 333 - 341
Sasso, G.M., Reimers, T.M., Cooper, L.J., Wacker, D., Berg, W., Steege, M., Kelly, L., & Allaire, A. (1992). Use of descriptive and experimental analyses to identify the functional properties of aberrant behavior in school settings. Journal of Applied Behavior Analysis, Volume 25, pp. 809 - 821
Saunders, M.D., Questad, K.A., Kedziorski, T.L., Boase, B.C., Patterson, E.A., & Cullinan, T.B. (2001). Unprompted mechanical switch use in individuals with severe multiple disabilities: An evaluation of the effects of body position. Journal of Developmental and Physical Disabilities, Volume 13(1), pp. 27 - 39
Saunders, M.D., Smagner, J.P., & Saunders, R.R. (2003). Improving methodological and technological analyses of adaptive switch use of individuals with profound multiple impairments. Behavioral Interventions, Volume 18, pp. 227 - 243
Saunders, M.D., Timler, G.R., Cullinan, T.B., Pilkey, S., Questad, K.A., & Saunders, R.R. (2003). Evidence of contingency awareness in people with profound multiple impairments: response duration versus response rate indicators. Research in Developmental Disabilities, Volume 24(4), pp. 231 - 245
Saunders, M.D., Saunders, R.R., Mulugeta, A., Henderson, K., Kedziorski, T., Hekker, B., & Wilson, S. (2005). A novel method for testing learning and preferences in people with minimal motor movement. Research in Developmental Disabilities, Volume 26(3), pp. 255 - 266
Saunders, R.R., McEntee, J.E., & Saunders, M.D. (2005). Interaction of reinforcement schedules, a behavioral prosthesis, and work-related behavior in adult with mental retardation. Journal of Applied Behavior Analysis, Volume 38(2), pp. 163 - 176
Savage, L.M., Buzzetti, R.A., & Ramirez, D.R. (2004). The effects of hippocampal lesions on learning, memory, and reward expectancies.
Neurobiology of Learning and Memory. Volume 82(2), pp. 109 - 119
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1977). Initial acquisition of symbolic skills via the Yerkes computerized language analogue system, Presentation at Nonspeech Language Intervention Conference, Gulf Shores, Al, March 1977
Savage-Rumbaugh, E.S., Wilkerson, B., & Bakeman, R. (1977). Spontaneous gestural communication among conspecifics in the pygmy chimpanzee. In - Progress in ape research, Bourne, G. (Ed.) , pp. 97 - 116. New York: Academic Press
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1978). Symbolization, language, and chimpanzees: A theoretical reevaluation based on initial language acquisition processes in four young pan troglodytes. Brain and Language, Volume 6, pp. 265 - 300
Savage-Rumbaugh, E.S., Rumbaugh, D., & Boysen, S. (1978a). Linguistically mediated tool use and exchange by chimpanzees. Behavioral and Brain Sciences. Volume 1, pp. 539 - 554
Savage-Rumbaugh, E.S., Rumbaugh, D., & Boysen, S. (1978b). Symbolic communication between two chimpanzees. Science, Volume 201: pp. 641 - 644
Savage-Rumbaugh, E.S. (1979). Symbolic communication - its origins and early development in the chimpanzee. New Directions for Child Development. Volume 3, pp. 1 - 15
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1980a). Language analogue project, phase II: Theory and tactics. In - Children's language, Nelson, K. (Ed.), pp. 267 - 307. New York: Gardner Press
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1980b). Requisites of symbolic communication - Or, are words for birds? The Psychological Record, Volume 30, pp. 305 - 315
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1980c). A response to Herbert Terrace's paper, "Linguistic apes". The Psychological Record.
Volume 30, pp. 315 - 318
Savage-Rumbaugh, E.S., Rumbaugh, D., & Boysen, S. (1980). Do apes use language? American Scientist, Volume 68, pp. 49 - 61
Savage-Rumbaugh, E.S., Rumbaugh, D., Smith, S.T., & Lawson, J. (1980). Reference: The linguistic essential. Science. Volume 210, pp. 922 - 924
Savage-Rumbaugh, E.S. (1981). Can apes use symbols to represent their world? In - The Clever Hans Phenomenon: Communication with horses, whales, apes, and people, Sebeok, T. & Rosenthal, R. (Eds.). pp. 35 - 59. Annals of the New York Academy of Sciences, Volume 364
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1982). Ape language research is alive and well: A reply. Anthropos, Volume 77: pp. 568 - 573
Savage-Rumbaugh, E.S., Pate, J., Lawson, J., Smith, S.T., & Rosenbaum, S. (1983). Can a chimpanzee make a statement? Journal of Experimental Psychology: General. Volume 112. pp. 457 - 492
Savage-Rumbaugh, E.S., Romski, M.A., Sevcik, R.A., & Pate, J. (1983). Assessing symbol usage versus symbol competency. Journal of Experimental Psychology: General. Volume 112, pp. 508 - 512
Savage-Rumbaugh, E.S. (1984a). Verbal behaviour at a procedural level in the chimpanzee. Journal of Experimental Analysis of Behaviour
Volume 41, pp. 223 - 250
Savage-Rumbaugh, E.S. (1984b). Pan paniscus and Pan troglodytes: Contrasts in preverbal communicative competence. In - The pygmy chimpanzee: Evolutionary biology and behavior, Susman, R. (Ed.). pp. 395 - 413. New York: Plenum
Savage-Rumbaugh, E.S. (1986). Ape language: From conditioned response to symbol. Oxford: Oxford University Press. New York: Columbia University Press
Savage-Rumbaugh, E.S., McDonald, K., Sevcik, R.A., Hopkins, W., & Rubert, E. (1986). Spontaneous symbol acquisition and
communicative use by pygmy chimpanzees. Journal of Experimental Psychology: General. Volume 115, pp. 211 - 235
Savage-Rumbaugh, E.S. (1987). Communication, symbolic communication, and Language: Reply to Seidenberg and Petitto. Journal of Experimental Psychology: General. Volume 116, pp. 288 - 292
Savage-Rumbaugh, E.S. (1998). A new look at ape language: Comprehension of vocal speech and syntax. In - Comparative perspectives in modern psychology. Nebraska Symposium on Motivation. Leger, D.W. (Ed.) . pp. 201 - 255. Lincoln, Nebraska: University of Nebraska Press
Savage-Rumbaugh, E.S., Sevcik, R., Brakke, K., Rumbaugh, D. & Greenfield, P. (1990). Symbols: Their communicative use, combination, and comprehension by Bobobos (pan paniscus). In - Advances in infancy research (Volume 6, pp. 221-278). Lipsett, L. & Rovee-Collier, C. (Eds). Norwood, NJ: Ablex
Savage-Rumbaugh, E.S. (1992). Pan to man: The language link. Presentation at the American Association for the Advancement of Science, February 8, 1992, Chicago
Savage-Rumbaugh, E.S., & Lewin, R. (1994). Kanzi: The ape at the brink of the human mind. London: Doubleday
Savarimuthu, D., & Bunnell, T. (2002). The effects of music on clients with learning disabilities: a literature review. Complementary Therapies in Nursing & Midwifery. Volume 8, pp. 160 -165
Saxby, H., Thomas, M., Felce, D., & De Kock, U. (1986). The use of shops, cafes and public houses by severely and profoundly mentally handicapped adults. British Journal of Mental Subnormality, Volume 32, pp. 69 - 81
Saxby, H, & Morgan, H. (1993). Behaviour Problems in Children with Learning Disabilities: to what extent do they exist and are they a problem? Child Care, Health and Development, Volume 19, pp. 149 - 157
Scarborough, D.R., Boyce, S., McCain, G., Oppenheimer, S., August, A., & Strinjas, J.N. (2006). Abnormal physiological responses to touch among children with persistent feeding difficulties. Developmental Medicine & Child Neurology. Volume 48, pp. 460 464
Scarth, S.B. (2001). Dance Movement therapy with adults with severe learning difficulties and behaviours that challenge. ADMT quarterly,
Volume 12(3), pp. 9 - 17
Schaaf, R.C., & Miller, L.J. (2005). Occupational therapy using a sensory integrative approach for children with developmental disabilities. Mental Retardation and Developmental Disabilities Research Reviews, Volume 11, pp. 143 – 148
Schaffer, R. (1984). Sensory integration therapy with learning disabled children: A critical review. Canadian Journal of Occupational
Therapy, Volume 51, pp. 73 - 77.
Schalock, R.L., Harper, R.S., & Genung, T. (1981). Community integration of mentally retarded adults: Community placement and program success. American Journal of Mental Deficiency, Volume 85(5), pp. 478 - 488.
Schalock, R.L., Brown, I., Brown, R., Cummins, R.A., Felce, D., Matikka, L., Keith K.D., & Parmenter, T. (2002). Conceptualization, measurement, and application of quality of life for people with intellectual disabilities: Report of an international panel of experts. Mental Retardation, Volume 40(6), pp. 457 – 470
Schalock, R.L., & Verdugo, M.A. (2002). Handbook on quality of life for human service practitioners. Washington, DC: American Association on Mental Retardation.
Schalock, R.L. (2004). The concept of quality of life: what we know and do not know. Journal of Intellectual Disability Research, Volume 48(3), pp. 203 – 216
Schalock, R.L., Verdugo, M.A., Jenaro, C., Wang, M., Wehmeyer, M., Xu, J., & Lachapelle, Y. (2005). A cross-cultural study of quality of life indicators. American Journal on Mental Retardation, Volume 110(4), pp. 298 – 311
Schalock, R.L. (2010). The measurement and use of quality of life-related personal outcomes, in - Enhancing the Quality of Life of People with Intellectual Disabilities, R. Kober, Ed., pp. 3 – 17, Springer, Dordrecht, The Netherlands
Schalock, R.L. & Verdugo, M.A. (2012). A leadership guide for today’s disabilities organizations. Baltimore, MD: Paul H. Brookes.
Schellingerhout, R., Smitsman, A.W., & Cox, R.F.A. (2005). Evolving patterns of haptic exploration in visually impaired infants. Infant Behavior & Development, Volume 28, pp. 360 – 388
Schepis, M.M., & Reid, D.H. (1994). Training direct service staff in congregate settings to interact with people with severe disabilities: A quick, effective and acceptable program. Behavioral Interventions, Volume 9(1), pp. 13 – 26
Schepis, M.M., & Reid, D.H. (1995). Effects of a voice output communication aid on interactions between support personnel and an individual with multiple disabilities. Journal of Applied Behavior Analysis, Volume 28(1), pp. 73 – 77
Schmitt, J.A.J., Benton, D., & Wolfgang Kallus, K. (2005). General methodological considerations for the assessment of nutritional influences on human cognitive functions. European Journal of Nutrition. Volume 44. pp. 459 – 464
Schneider, M.J., Bijam-Schulte, A.M., Janssen, C.G.C., & Stolk, J. (1995). The origin of self-injurious behaviour of children with mental retardation. British Journal of Developmental Disabilities. Volume 42, pp. 136 - 148
Schneider, R.S. (2016). Making Sense: A Guide to Sensory Issues. Future Horizons
Schroeder, S.R., Schroeder, C.S., Smith, B., & Dalldorf, J. (1978). Prevalence of self-injurious behaviors in a large state facility for the retarded: a three year follow-up. Journal of Autism and Childhood Schizophrenia, Volume 8, pp, 261 - 269
Schrojenstein Lantman‐de Valk, H.V., Akker, M.V.D., Maaskant, M.A., Haveman, M.J., Urlings, H.F.J., Kessels, A., & Crebolder, H.F.J. (1997). Prevalence and incidence of health problems in people with intellectual disability. Journal of Intellectual Disability Research, Volume 41(1), pp. 42 - 51
Schulz, R., & Hanusa, B.H. (1978). Long-Term Effects of Control and Predictability-Enhancing Interventions: Findings and Ethical
Issues. Journal of Personality and Social Psychology, Volume 36. pp. 1202 – 1012
Schwartz, B. (2005). The Paradox of Choice: Why More Is Less. Harper Perennial; New edition edition.
Schwartzman, L., Yu, C.T., & Martin, G.L. (2003). Choice responding as a function of choice presentation method and level of preference in persons with developmental disabilities. International Journal of Disability, Community & Rehabilitation, Volume 1, pp. 1 - 7
Schwartzman, L., Martin, G.L., Yu, C.T., & Whiteley, J. (2004). Choice, Degree of Preference, and Happiness Indices with Persons with Intellectual Disabilities: A Surprising Finding. Education and Training in Developmental Disabilities, Volume 39(3), pp 265 - 269
Scott, N. (2005). Special needs, special horses. A guide to the benefits of therapeutic riding. University of North Texas Press
Scott, R.C., King, M.D., Gadian, D.G., Neville, B.G., & Connelly, A. (2003). Hippocampal abnormalities after prolonged febrile convulsion: a longitudinal MRI study. Brain. Volume 126. pp. 2551 – 2557
Scoggins, A. (2016). The Effects of Positive-Interactions Staff Training on the Behavior of Staff and Clients during Small Groups in a Center-Based Program of Adult Day Services. (Doctoral dissertation, University of Kansas).
Sears, C.J. (1981). The Tactilely Defensive Child. Academic Therapy, Volume 16(5), pp. 563 - 569
Sears, C.J. (1994). Recognizing and coping with tactile defensiveness in young children. Infants & Young Children. Volume 6(4). pp. 46 - 53
Seay, B., & Harlow, H.F. (1965). Maternal separation in the rhesus monkey. The Journal of Nervous and Mental Disease, Volume 140(6), pp. 434 - 441
Sebba, J. (1988). The Education of People with Profound and Multiple Handicaps. Resource Material for Staff Training. Manchester University Press
Sebba, J., Byers, R., & Rose, R. (1995). Redefining the Whole Curriculum for Pupils with Learning Difficulties (revised edition). London: David Fulton Publishers
Seifert, M. (2002). Menschen mit schwerer Behinderung in Heimen. Ergebnisse der Ko¨lner Lebensqualita¨t-Studie [Humans with severe handicap in homes. Results of the Cologne quality of life study]. Geistige Behinderung, Volume 3, pp. 203 - 222
Seltzer, M.M., & Krauss, M.W. (2001). Quality of life of adults with mental retardation / developmental disabilities who live with family.
Mental Retardation and Developmental Disabilities Research Reviews, Volume 7, pp. 105 – 114
Serpell, J. (1991). Beneficial effects of pet ownership on some aspects of human health and behaviour. Journal of the Royal Society of Medicine. Volume 84(12). pp. 717 - 720
Seung, H., Rogalski, Y., Shankar, M., & Elder, J. (2007). The gluten-and casein-free diet and autism: Communication outcomes from a preliminary double-blind clinical trial. Journal of Medical Speech Language Pathology, Volume 15(4), pp. 337 - 345
Seys, D., Duker, P., Salemink, W., & Franken-Wijnhoven, J. (1998). Resident behaviors and characteristics as determinants of quality of residential care: An observational study. Research in Developmental Disabilities, Volume 19(3), pp. 261 – 273
Shapiro, M., Parush, S., Green, M., & Roth, D. (1997). The efficacy of the "Snoezelen" in the management of children with mental retardation who exhibit maladaptive behaviours. British Journal of Developmental Disabilities, Volume 43(2), pp. 140 - 155
Sharma, V.M., Sridharan, K., Pichan, G., & Panwar, M.R. (1986). Influence of heat-stress induced dehydration on mental functions. Ergonomics. Volume 29, pp. 791 - 799
Sheehy, K., & Nind, M. (2005). Emotional well-being for all: mental health and people with profound and multiple learning disabilities. British Journal of Learning Disabilities, Volume 33, pp. 34 - 38
Shenk, D. (2003). Concept of Information Overload, Encyclopedia of International Media and Communications, Volume 2, pp. 395 - 405
Shentoub, S.A., Soulairac, A., & Rustin, E. (1955). Compartement de l'enfant arriere devant Ie mirior. Enfance. Volume 7, pp. 333 - 340
Shere, B., & Kastenbaum, R. (1966). Mother child interaction in cerebral palsy: Environment and psychosocial obstacles to cognitive development, Genetic Psychology Monographs, Volume 73, pp. 255 - 335
Sheridan, M.D. (1964). Development of auditory attention and language symbols in young children. In - Renfrew, C. & Murphy, K.(Eds.), The child who does not talk. Clinics in developmental medicine. Spastics Society Medical Educational & Information Unit. William Heinemann medical books Ltd.
Shevin, M., & Klein, N.K. (1984). The importance of choice-making skills for students with severe disabilities. Journal of The Association for Persons with Severe Handicaps, Volume 9, pp. 159 - 166
Shirreffs, S.M., Merson, S.J., Fraser, S.M., & Archer, D.T. (2004). The effects of fluid restriction on hydration status and subjective
feelings in man. British Journal of Nutrition. Volume 91. pp. 951 - 958
Shogren, K.A., Lopez, S.J., Wehmeyer, M.L., Little, T.D., & Pressgrove, C.L. (2006). The role of positive psychology constructs in
predicting life satisfaction in adolescents with and without cognitive disabilities: An exploratory study. Journal of Positive Psychology, Volume 1, pp. 37 – 52
Shogren, K.A., Wehmeyer, M.L., Palmer, S.B., Soukup, J.H., Little, T.D., Garner, N., & Lawrence, M. (2007). Examining individual
and ecological predictors of the self-determination of students with disabilities. Exceptional Children, Volume 73, pp. 488 – 509
Shogren, K.A., Wehmeyer, M.L., Palmer, S.B., Soukup, J.H., Little, T., Garner, N., & Lawrence, M. (2008). Understanding the
construct of self-determination: Examining the relationship between the arc’s self-determination scale and the American Institute for
Research self-determination scale. Assessment for Effective Instruction, Volume 33, pp. 94 – 107
Shogren, K.A., Palmer, S.B., Bovaird, J., & Wehmeyer, M.L. (2010). Locus of control orientations in students with Intellectual Disability, Learning Disabilities, and no disabilities: A latent growth curve analysis. Research and Practice for Persons with Severe Disabilities, Volume 35(3-4), pp. 80 - 92
Shogren, K.A., Palmer, S.B., Wehmeyer, M.L., Williams-Diehm, K., & Little, T.D. (2012). Effect of intervention with the self-determined learning model of instruction on access and goal attainment. Remedial and Special Education, Volume 33, pp. 320 – 330
Shogren, K.A., Wehmeyer, M.L., Palmer, S.B., Rifenbark, G.G., & Little, T.D. (2015). Relationships between self-determination and post-school outcomes for youth with disabilities. Journal of Special Education. Volume 48(4), pp. 256 – 267
Shonkoff, J.P. (2011). Protecting brains, not simply stimulating minds. Science, Volume 333(6045), pp. 982 - 983
Shurtleff, T.L., Standeven, J.W., & Engsberg, J.R. (2009). Changes in Dynamic Trunk/Head Stability and Functional Reach After Hippotherapy. Archives of Physical Medical Rehabilitation, Volume 90, pp. 1185 - 1195
Siegel-Causey, E., Guy, B., & Guess, D. (1995). Severe and Multiple Disabilities. In - E.L. Meyen and T.M. Skrtic (Eds.), Special Education and Student Disability: an Introduction. Traditional, Emerging and Alternative Perspectives (4th ed.). Denver: Love Publishing.
Siegel-Causey, E., & Bashinski, S.M. (1997). Enhancing initial communication and responsiveness of learners with multiple disabilities: A tri-focus framework for partners. Focus on Autism and Other Developmental Disabilities, Volume 12(2), pp. 105 - 120
Siewertsen, C., French, E., & Teramoto, M. (2015). Autism Spectrum Disorder and Pet Therapy. Advances in Mind - Body Medicine, Volume 29(2), pp. 22 - 25
Sigafoos, J., & Dempsey, R. (1992). Assessing choice making among children with multiple disabilities. Journal of Applied Behavior Analysis, Volume 25, pp. 747 – 756
Sigafoos, J., Roberts, D., Couzens, D., & Caycho, L. (1992). Improving instruction for adults with developmental disabilities: Evaluation of a staff training package. Behavioral Interventions, Volume 7(4), pp. 283 - 297
Sigafoos, J., Roberts, D., Couzens, D., & Kerr, M. (1993). Providing opportunities for choice-making and turn-taking to adults with multiple disabilities. Journal of Developmental and Physical Disabilities, Volume 5, pp. 297 - 310
Sigelman, C.K., Schoenrock, C.J., Spanhel, C.L., Hromas, S.G., Winer, J.L., Budd, E.C., & Martin, P.W. (1980). Surveying Mentally Retarded Persons: Responsiveness and Response Validity in Three Samples. American Journal of Mental Deficiency, Volume 84 (5), pp. 479 - 486
Sigelman, C.K., Budd, E.C., Spanhel, C.L. & Schoenrock, C.J. (1981a) When in doubt say yes: acquiescence in interviews with mentally retarded persons. Mental Retardation. Volume 19, pp. 53 - 58
Sigelman, C.K., Budd, E.C., Spanhel, C.L. & Schoenrock, C.J. (1981b). Asking questions of mentally retarded persons: a comparison of yes-no and either-or formats, Applied Research in Mental Retardation, Volume 2, pp. 347 - 357
Sigelman, C.K., Schoenrock, C.J.,Winer, J.L., Spanhel, C.L., Hromas, S.G., Martin, P.W., Budd, E.C., & Bensberg, G.J. (1981). Issues in interviewing mentally retarded persons: An empirical study. In R.H. Bruininks, C.E. Meyers, B.B. Sigford, & K.C. Lakin (Eds.), Deinstitutionalization and community adjustment of mentally retarded people (Monograph No. 4). Washington, D.C.: American Association on Mental Deficiency.
Sigelman, C.K., Budd, E.C., Winer, J.L., Schoenrock, C.J., & Martin, P.W. (1982). Evaluating Alternative Techniques of Questioning Mentally Retarded Persons. American Journal of Mental Deficiency, Volume 86(5), 1982, pp. 511 - 518
Sigelman, C.K., Winer, J.L. & Schoenrock, C.J. (1982). The responsiveness of mentally retarded persons to questions. Education and Training of the Mentally Retarded, Volume 17, pp. 120 - 124
Sigelman, C.K., Schoenrock, C.J., Budd, E.C., Winer, J.L., Spanhel, C.L., Martin, P.W., Hromas, S.G., & Bensberg, G.J. (1983). Communicating with Mentally Retarded Persons: Asking Questions and Getting Answers, Research and Training Center in Mental Retardation, Texas Tech University
Sigelman, C.K., & Budd, E.C. (1986). Pictures as an aid in questioning mentally retarded persons, Rehabilitation Counselling Bulletin, Volume 29, pp. 173 - 181
Silva, K., Correia, R., Lima, M., Magalhães, A., & de Sousa, L. (2011). Can dogs prime autistic children for therapy? Evidence from a single case study. Journal of Alternative and Complementary Medicine, Volume 17, pp. 1 – 5
Simeon, D.T., & Grantham-McGregor, S,M. (1990). Nutritional deficiencies and children's behaviour and mental development. Nutrition Research Reviews. Volume 3. pp. 1 - 24
Simmons, B, & Watson, D. (2014). Challenging the Developmental Reductionism of ‘Profound and Multiple Learning Disabilities’ Through
Academic Innovation. PMLD Link, Volume 26(3), Issue 79, pp. 25 - 27
Simon, T.J., Hespos, S.J., & Rochat, P. (1995). Do infants understand simple arithmetic? A replication of Wynn (1992). Cognitive Development, Volume 10(2), pp. 253 - 269
Singer, W. (2008). Epigenesis and brain plasticity in education. In - A. Battro, K. Fischer, & P. Léna (Eds.), The Educated Brain: Essays in Neuroeducation (pp. 97-109). Cambridge: Cambridge University Press.
Singh, N.N., Lancioni, G.E., O’Reilly, M.F., Molina, E.J., Adkins, A.D., & Oliva, D. (2003). Self-determination during mealtimes through microswitch choice-making by an individual with complex multiple disabilities and profound mental retardation. Journal of Positive Behavior Interventions, Volume 5(4).
Singh, N.N., Lancioni, G.E., Winton, A.S.W., Wahler, R.G., Singh, J., & Sage, M. (2003). Mindful caregiving increases happiness among individuals with profound multiple disabilities. Research in Developmental Disabilities, Volume 25(2), pp. 207 – 218
Singh, N.N., Lancioni, G.E., Winton, A.S.W., Molina, E.J., Sage, M., Brown, S., et al. (2004). Effects of Snoezelen room, activities of daily living skills training, and vocational skills training on aggression and self-injury by adults with mental retardation and mental illness. Research in Developmental Disabilities, Volume 25(3), pp. 285 - 293
Singh, N.N., Lancioni, G.E., Winton, A.S.W., Wahler, R.G., Singh, J., & Sage, M. (2004). Mindful care-giving increases happiness among individuals with profound multiple disabilities. Research in Developmental Disabilities, Volume 25(2), pp. 207 - 218
Singh, V., & Ghai, A. (2009). Notions of self: Lived realities of children with disabilities. Disability and Society, Volume 24(2), pp.129 - 145
Sisson, L.A., Kilwein, M.L., & Van Hasselt, V.B. (1988). A graduated guidance procedure for teaching self-dressing skills to multi-handicapped children. Research in Developmental Disabilities. Volume 9(4), pp. 419 - 432
Skeja, E. (2014). The impact of cognitive intervention program and music therapy in learning disabilities. Procedia Social and Behavioral Sciences, Volume 159, pp. 605 - 609
Skinner, B.F. (1938). The Behavior of Organisms:An Experimental Analysis, New York: Appleton-Century-Crofts
Slater, A., Mattock, A., & Brown, E. (1990). Size constancy at birth: Newborn infants' responses to retinal and real size. Journal of Experimental Child Psychology, Volume 49(2), pp. 314 - 322
Slater, A., Morison, V., Somers, M., Mattock, A., Brown, E., & Taylor, D. (1990). Newborn and older infants' perception of partly occluded objects. Infant Behavior and Development, Volume 13(1), pp. 33 - 49
Slater, A., Mattock, A., Brown, E., & Bremner, J.G. (1991). Form perception at birth: Revisited. Journal of Experimental Child Psychology, Volume 51(3), pp. 395 - 406
Sloneem, J., Arron, K., Hall, S.S., & Oliver, C. (2009). Self-injurious behaviour in Cornelia de Lange syndrome: 2. association with environmental events’. Journal of Intellectual Disability Research, Volume 53, pp. 590 – 603
Sloper, P., Knussen, C.,Turner, S., & Cunningham, C. (1991). Factors relating to stress and satisfaction with life in families of children with Down's syndrome. Journal of Child Psychology and Psychiatry, Volume 32, pp. 655 - 676
Smidt, A., Balandin, S., Reed, V., & Sigafoos, J. (2007). A communication training programme for residential staff working with adults with challenging behaviour: Pilot data on intervention effects. Journal of Applied Research in Intellectual Disabilities, Volume 20 (1), pp. 16 – 29
Smith, A.M., Roux, S., Naidoo, N.T., & Venter, D.J.L. (2005). Food choices of tactile defensive children. Nutrition. Volume 21(1), pp. 14 – 19
Smith, B., Moore, Y., & Phillips, C.J. (1983). Education with understanding? Special Education; Forward Trends, Volume 10(2): pp. 21 - 24
Smith, B. (1994). Handing over control to people with learning difficulties. In J. Coupe-O'Kane and B. Smith - Taking Control: Enabling people with learning difficulties. David Fulton Publishers
Smith, B. (1996). Discussion: Age-appropriate or Developmentally appropriate Activities? In - Coupe O’Kane, J. & Goldbart, J. (eds)
Whose Choice? - Contentious Issues For Those Working With People With Learning Difficulties. London: David Fulton.
Smith, K.A., & Gouze, K.R. (2004). The Sensory-Sensitive Child. Collins
Smith, L.J. (1996). A behavioural approach to the treatment of non‐retentive encopresis in adults with learning disabilities. Journal of Intellectual Disability Research, Volume 40(2), pp. 130 - 139
Smith, L. (2001). Communication Partnerships with People with Profound and Multiple Learning Disabilities. Tizard Learning Disability
Review, Volume 6(2), pp.16 - 21
Smith, M.D. (1985). Managing the aggressive and self-injurious behavior of adults disabled by autism. Journal of the Association for Persons with Severe Handicaps, Volume 10, pp. 228 - 232
Smith, P. (2006). Choice and control: What families want from school and community supports. Paper presented at the Annual conference of TASH, Baltimore, MD.
Smith, P., & Routel, C.R. (2010). Transition failure: The cultural bias of self-determination and the journey to adulthood for people with disabilities. Disability Studies Quarterly, Volume 30(1), pp. 1 – 22
Smith, R.B., Morgan, M., & Davidson, J. (2005). Does the daily choice making of adults with intellectual disability meet the normalisation
principle? Journal of Intellectual & Developmental Disability. Volume 30(4), pp. 226 – 235
Smith, S.A., Press, B., Koenig, K.P., & Kinnealey, M. (2005). Effects of sensory integration intervention on self-stimulating
and self-injurious behaviors. American Journal of Occupational Therapy, Volume 59, pp. 418 – 425
Smith Roley, S., Mailloux, Z., Miller-Kuhaneck, H., & Glennon, T. (2007). Understanding Ayres' Sensory Integration. OT Practice. Volume 12(7)
Snell, M., & Brown, F. (eds.) (2000). Instruction of Students with Severe Disabilities. (5th edition). Upper Saddle River, NJ: Merril.
Snow, E. Langdon, P., & Reynolds, E.S. (2007). Care staff attributions toward self-injurious behaviour exhibited by adults with intellectual disabilities. Journal of Intellectual Disabilities, Volume 11(1), pp. 47 – 63
Snyder A.W., & Thomas M. (1997). Autistic artists give clues to cognition, Perception, Volume 26, pp. 93 - 96
Snyder A.W., & Mitchell D.J. (1999). Is integer arithmetic fundamental to mental processing? The mind’s secret arithmetic. Proceedings of the Royal Society of London B: Biological Sciences, Volume 266(1419), pp. 587 - 592
Snyder A.W. (2001). Paradox of the savant mind, Nature, Volume 413, pp. 251 - 252
Snyder, A.W., Mulcahy, E., Taylor, J.L., Mitchell, D.J., Sachdev, P., & Gandevia, S.C. (2003). Savant-like skills exposed in normal people by suppressing the left fronto-temporal lobe. Journal of Integrative Neuroscience, Volume 2(02), pp. 149 - 158
Snyder, A.W., Bossomaier, T., & Mitchell, D.J. (2004). Concept formation: 'object' attributes dynamically inhibited from conscious awareness. Journal of Integrative Neuroscience, Volume 3(01), pp. 31 - 46
Snyder, A.W. (2009). Explaining and inducing savant skills: privileged access to lower level, less-processed information. Philosophical Transactions of the Royal Society of London B: Biological Sciences, Volume 364(1522), pp. 1399 - 1405
Soto-Ares, G., Joyes, B., Lemaître, M.P., Vallée, L., & Pruvo, J.P. (2003). MRI in children with mental retardation. Pediatric Radiology, Volume 33(5), pp. 334 - 345
Sousa, D. (2007). How the Special Needs Brain Learns. Crown Press/Sage, CA USA.
Sowers, J., & Powers, L. (1995). Enhancing the participation and independence of students with severe physical and multiple disabilities in
performing community activities. Mental Retardation, Volume 33, pp. 209 – 220
Spevack, S., Martin, T.L., Hiebert, R., Yu, C.T., & Martin, G.L. (2004). Effects of choice of work tasks on on-task, aberrant, happiness and unhappiness behaviors of persons with developmental disabilities. Journal on Developmental Disabilities, Volume 11, pp. 79 – 98
Spiker, D., & Ricks, M. (1984). Visual Self-recognition in autistic children: Developmental relationships. Child Development, Volume 55: pp. 214 - 225
Spooner, F., Dymond, S.K.., Smith, A., & Kennedy, C.H. (2006). What we know and need to know about accessing the general curriculum for students with significant cognitive disabilities. Research and Practice for Persons with Severe Disabilities, Volume 31(4), pp. 277 – 283
Spragg, M. (2015). Music Therapy within a Multidisciplinary Special Education Team. In - C. Miller (Ed.), Arts Therapists in Multidisciplinary Settings: Working Together for Better Outcomes, pp. 83-95. Jessica Kingsley Publishers
Spreat, S., Lipinski, D. Hill, J., & Halpin, M.E. (1986). Safety indices associated with the use of contingent restraint procedures. Applied Research in Mental Retardation. Volume 1000, pp. 528 - 532
Spreat, S., Lamina, J., Jefferys, J., Axelrod, S., Murphy, B.J., & McGuffin, P. (1990). The impact of environmental noise on mealtime social interactions in a residential facility for persons with mental retardations. Behavioral Residential Treatment, Volume 5(1), pp. 1 - 13
Srinivasan, P. (2009). A review of dietary interventions in autism. Annals of Clinical Psychiatry: Official Journal of the American Academy of Clinical Psychiatrists, Volume 21(4), pp. 237 - 247
Stafford, A.M. (2005). Choice Making: A Strategy for Students With Severe Disabilities. Teaching Exceptional Children. Volume 37(6), pp. 12 - 17
Stagnitti, K., Raison, P., & Ryan, P. (1999). Sensory defensiveness syndrome: A paediatric perspective and case study. Australian Occupational Therapy Journal. Volume 46(4), pp. 175 – 187
Stalker, K., & Harris, P. (1998). The Exercise of Choice by Adults with Intellectual Disabilities: A Literature Review. Journal of Applied Intellectual Disabilities, Volume 11, pp. 60 - 76
Stamatis, P.J. (2011). Non verbal communication in classroom interactions: A pedagogical perspective of touch. Electronic Journal of Research in Educational Psychology, Volume 9(3), pp. 1427 - 1442
Stamenovic, M. (2009). Engagement in Music Therapy: a detailed study of communication between the therapist and client presenting with severe and multiple handicaps. Master of Music Therapy Thesis: New Zealand School of Music, Wellington
Stancliffe, R.J. (1995). Assessing opportunities for choice-making: A comparison of self- and staff reports. American Journal on Mental Retardation, Volume 99, pp. 418 – 429
Stancliffe, R.J., & Wehmeyer, M.L. (1995). Variability in the availability of choice to adults with mental retardation. The Journal of Vocational Rehabilitation, Volume 5, pp. 319 – 328
Stancliffe, R.J. (1997). Community living-unit size, staff presence and resident’s choice making. Mental Retardation, Volume 35, pp. 1 – 9
Stancliffe, R.J., & Abery, B.H. (1997). Longitudinal study of deinstitutionalization and the exercise of choice. Mental Retardation, Volume 35, pp. 159 – 169
Stancliffe, R.J., & Lakin, K.C. (1998). Analysis of expenditures and outcomes of residential alternatives for persons with developmental disabilities. American Journal on Mental Retardation, Volume 102(6), pp. 552 – 568
Stancliffe, R.J., Abery, B.H., & Smith, J. (2000). Personal control and the ecology of community living settings: Beyond living-unit size and
type. American Journal on Mental Retardation, Volume 105, pp. 431 – 454
Stancliffe, R.J., Abery, B.H., Springborg, H., & Elkin, S. (2000). Substitute decision making and personal control: Implications for self determination. Mental Retardation. Volume 38(5), pp. 407 - 421
Stancliffe, R.J. (2001). Living with support in the community: Predictors of choice and self determination. Mental Retardation and Developmental Disabilities Research Reviews, Volume 7, pp. 91 – 98
Stancliffe, R.J., & Lakin, K.C. (2005). Costs and outcomes of community services for people with intellectual disabilities. Paul H Brookes Publishing.
Stancliffe, R.J., Lakin, K.C., Larson, S., Engler, J., Bershadsky, J., Taub, S., Fortune, J., & Ticha, R. (2011). Overweight and obesity among adults with intellectual disabilities who use intellectual disability/developmental disability services in 20 US States. American Journal on Intellectual and Developmental Disabilities, Volume 116(6), pp. 401 - 418
Stanish, H.I., & Draheim, C.C. (2005). Assessment of walking activity using a pedometer and survey in adults with mental retardation. Adapted Physical Activity Quarterly, Volume 22(2), pp. 136 - 145
Stanton, D., Wilson, P., Foreman, N., & Duffy, H. (2000). Virtual environments as spatial training aids for children and adults with physical disabilities. 3rd International Conference on Disability, Virtual Reality and Associated Technologies.
Steege, M.W., Wacker, D.P., Cigrand, K.C., Berg, W.K., Novak, C.G., Reimers, T.M., Sasso, G.M. and DeRaad, A. (1990). Use of negative reinforcement in the treatment of self-injurious behavior. Journal of Applied Behavior Analysis, Volume 23, pp. 459 - 467
Stein, Z., & Susser, M. (1985). Effects of early nutrition on neurological and mental competence in human beings. Psychological Medicine. Volume 15. pp. 717 - 726
Steiner, H. (2012). Sensational Journeys: 48 Personal Stories of Sensory Processing Disorder. Future Horizons
Stenfert Kroese, B., & Fleming, I. (1992). Staff attitudes and working conditions in community-based group homes of people with learning difficulties, Mental Handicap Research, Volume 5, pp. 82 - 91
Stephenson, J. (2006). Music therapy and the education of students with severe disabilities. Education and Training in Developmental Disabilities (formerly Education and Training in Mental Retardation and Developmental Disabilities), Volume 41(3), pp. 290 - 299
Sterba, J.A., Rogers, B.T., France, A.P., & Vokes, D.A. (2002). Horseback riding in children with cerebral palsy: Effect on gross
motor function. Developmental Medicine and Child Neurology, Volume 44, pp. 301 – 308
Stern, D.N. (1985). The Interpersonal World of the Infant: A View from Psychoanalysis and Developmental Psychology: A View from Psychoanalysis and Development Psychology. Karnac Books
Sternberg, L. (1994). Individuals with Profound Disabilities: Instructional and Assistive Strategies (3rd edition), PRO-ED Inc., Austin, Texas
Stevenson, K. (2003). Music therapy assisted communication with children with severe disabilities. The New Zealand Journal of Music Therapy, Volume 1, pp. 82 - 92
Stewart, L., Beange, H., & Mackerras, D. (1994). A survey of dietary problems of adults with learning disabilities in the community. Journal of Applied Research in Intellectual Disabilities, Volume 7(1), pp. 41 - 50
Stock, S.E., Davies, D.K., Secor, R.R., & Wehmeyer, M.L. (2003). Self-directed career preference selection for individuals with intellectual disabilities: using computer technology to enhance self determination. Journal of Vocational Rehabilitation, Volume 19, pp. 95 – 103
Stolker, J.J., Scheifes, A., Egberts, A.C., & Heerdink, E.R. (2008). Inappropriate prescribing of antipsychotics to people with a mental disability and aggressive behavioural disorders. Nederlands Tijdschrift voor Geneeskunde, Volume 152, pp. 1501 – 1502
Stone, V.E., Baron-Cohen, S., & Knight, R.T. (1998). Frontal lobe contributions to theory of mind. Journal of Cognitive Neuroscience, Volume 10, pp. 640 - 656
Stonefelt, L.L., & Stein, F. (1998). Sensory integrative techniques applied to children with learning disabilities: An outcome study. Occupational Therapy International, Volume 5, pp. 252 – 272
Stores, R, Stores, G., Fellows, B.& Buckley, S. (1998). Daytime behaviour problems and maternal stress in children with Down's syndrome, their siblings, and non-intellectually disabled and other intellectually disabled peers. Journal of Intellectual Disability Research, Volume 42, pp. 228 - 237
Storey, K., Bates, P., McGhee, N., & Dycus, S. (1984). Reducing the self-stimulatory behavior of a profoundly retarded female through sensory awareness training. American Journal of Occupational Therapy, Volume 38, pp. 510 – 516
Strange, J. (2013). Improvised music to support interaction between profoundly learning-disabled teenagers and their learning support assistants. Doctoral dissertation, Anglia Ruskin University
Strnadova, I., & Evans, D. (2012). Subjective Quality of Life of Women with Intellectual Disabilities: The Role of Perceived Control over Their Own Life in Self-Determined Behaviour. Journal of Applied Research in Intellectual Disabilities, Volume 25(1), pp.71 - 79
Strupp, M., Arbusow, V., Dieterich, M., Sautier, W., & Brandt, T. (1998). Perceptual and oculomotor effects of neck muscle vibration in vestibular neuritis. Ipsilateral somatosensory substitution of vestibular function. Brain: a Journal of Neurology, Volume 121(4), pp. 677 - 685
Stuss, D.T., Gallup, G.G., Jr., & Alexander, M.P. (2001). The frontal lobes are necessary for theory of mind. Brain, Volume 124, pp. 279 - 286
Sugden, D. (1989). Cognitive Approaches in Special Education. Lewes: Falmer Press.
Suhr, J.A., Hall, J., Patterson, S.M., & Niinisto, R.T. (2004). The relation of hydration status to cognitive performance in healthy older adults. International Journal of Psychophysiology. Volume 53. pp. 121 - 125
Suhr, J.A., Patterson, S.M., Austin, A.W., & Heffner, K.L. (2010). The relation of hydration status to declarative memory and working memory in older adults. Journal of Nutrition, Health & Aging. Volume 14. pp. 840 - 843
Sullivan, M., & Lewis, M. (2000). Assistive technology for the very young: Creating responsive environments. Infants and Young Children, Volume 12 (4), pp. 34 - 52
Sullivan, M. W., & Lewis, M. (1990). Contingency intervention: A program portrait. Journal of Early Intervention, Volume 14, pp. 367 - 375
Sun, J., Chen, Q., Zhang, Q., Li, Y., Li, H., Wei, D., Yang, W., & Qiu, J. (2016). Training your brain to be more creative: brain functional and structural changes induced by divergent thinking training. Human Brain Mapping, Volume 37(10), pp. 3375 - 3387
Sutcliffe, J. (1990). Adults with learning difficulties: Education for choice and empowerment. National Institute for Adult Continuing Education (NIACE) in association with the Open University Press
Sutherland, G., Couch, M.A., & Iacono, T. (2002). Health issues for adults with developmental disability. Research in Developmental Disabilities, Volume 23(6), 422 - 445
Suzuki, W.A. (2015). Healthy Brain, Happpy Life. Dey Street Books
Suzuki, W.A. (2016). How Body Affects Brain. Cell Metabolism, Volume 24, pp. 192 - 193
Swanson, H.L. (2000). What Instruction Works for Students with Learning Disabilities? Summarizing the Results from a Meta-Analysis of Intervention Studies. In: R. Gersten, E.P. Schille, & S. Vaughn (eds). Contemporary Special Education Research: Syntheses of the
Knowledge Base on Critical Instructional Issues, pp. 1-30, Mahwah, NJ: Lawrence Erlbaum.
Sweeney, L.A. (1989). Reducing learned dependency in potential and early augmentative communication users. Southeast Augmentative Communication Conference Proceedings
Sweeney, L.A. (1991). Learned dependency and co-dependency among potential users of augmentative communication, American Speech Language Hearing Association Miniseminar, Atlanta, Georgia
Sweeney, L.A. (1993). Helplessness, Dependency, an explanatory style as variables of employment potential among Augmented Communicators, First Annual Pittsburgh Employment Conference for Augmented Communicators Proceedings, August 20-22: Shout Press: Pittsburgh
Sylwester, R. (1986). Synthesis of Research on Brain Plasticity: The Classroom Environment and Curriculum Enrichment. Educational Leadership, Volume 44(1), pp. 90 - 93
Symons, F.J., Davis M.L., & Thompson, T. (2000). Self-injurious behaviour and sleep disturbance in adults with developmental disabilities. Research in Developmental Disabilities. Volume 21, pp. 115 – 23
Symons, F.J., Sperry, L.A., Dropik, P.L., & Bodfish, J.W. (2005). The early development of stereotypy and self-injury: a review of research methods. Journal of Intellectual Disability Research, Volume 49(2), pp. 144 - 158
Symons, F.J., Harper, V.N., McGrath, P.J., Breau L.M., & Bodfish, J.W. (2009). Evidence of increased non-verbal behavioural signs of pain in adults with neurodevelopmental disorders and chronic self-injury. Research in Developmental Disabilities. Volume 30, pp. 521 – 528
Synofzik, M., Vosgerau, G., & Newen, A. (2008). I move, therefore I am: A new theoretical framework to investigate agency and ownership. Consciousness and Cognition, Volume 17, pp. 411 – 424
Szinnai, G., Schachinger, H., Arnaud, M.J., Linder, L., & Keller, U. (2005). Effect of water deprivation on cognitive-motor performance in healthy men and women. American Journal of Physiology. Regulatory, Integrative and Comparative Physiology. Volume 289. pp. 275 - 280
Szpunar, K.K. (2010). Episodic future thought: an emerging concept, Perspective in Psychological Science, Volume 5, pp. 142 – 162
Tadema, A.C., & Vlaskamp, C. (2010). The time and effort in taking care for children with profound intellectual and multiple disabilities: A study on care load and support. British Journal of Learning Disabilities, Volume 38(1), pp. 41 - 48
Takeuchi, E. (1994). Incidence of obesity among school children with mental retardation in Japan. American Journal on Mental Retardation.
Volume 99(3), pp. 283 - 288
Tammet, D. (2007). Born on a blue day: Inside the extraordinary mind of an autistic savant. Simon and Schuster.
Tammet, D. (2009). Embracing the wide sky: a tour across the horizons of the mind. Simon and Schuster.
Tanabe, H., Hashikawa, K., Nakagawa, Y., Ikeda, M., Yamamoto, H., Harada, K., Tsumoto, T., Nishimura, T., Shiraishi, J., & Kimura, K. (1991). Memory loss due to transient hypoperfusion in the medial temporal lobes including hippocampus. Acta Neurologica Scandinavica. Volume 84. pp. 22 - 27
Tang, Y., Nyengaard, J.R., De Groot, D.M., & Gundersen, H.J.G. (2001). Total regional and global number of synapses in the human brain neocortex. Synapse, Volume 41(3), pp. 258 - 273
Tate, B.G., & Baroff, G.S. (1966). Aversive control of self-injurious behavior in a psichotic boy. Behavior Research and Therapy. Volume 4, pp. 281 - 287
Taylor, J.C., & Carr, E.G. (1992a). Severe behavior problems related to social interaction. I: Attention seeking and social avoidance. Behavior Modification, Volume 16, pp. 305 - 335.
Taylor, J.C., & Carr, E.G. (1992b). Severe behavior problems related to social interaction. II: A systems analysis. Behavior Modification, Volume 16, pp. 336 - 371
Taylor, J.C., Sisson, L.A., McKelvey, J.L., & Trefelner, M.F. (1993). Situation specificity in attention-seeking problem behavior. Behavior Modification, Volume 17, pp. 474 - 497
Temple, V.A., & Walkley, J.W. (2003). Physical activity of adults with intellectual disability. Journal of Intellectual & Developmental Disability, Volume 28, pp. 342 – 352
Temple, V.A., Frey, G.C., & Stanish, H.I. (2006). Physical activity of adults with mental retardation: Review and research needs. American Journal of Health Promotion, Volume 21(1), pp. 2 – 12
Ten Brug, A., Van der Putten, A.A., & Vlaskamp, C. (2013). Learn and apply: Using multi-sensory storytelling to gather knowledge about preferences and abilities of children with profound intellectual and multiple disabilities – three case studies. Journal of Intellectual Disabilities, Volume 17(4), pp. 339 - 360
Ten Brug, A., Munde, V.S., van der Putten, A.A., & Vlaskamp, C. (2015). Look closer: the alertness of people with profound intellectual and multiple disabilities during multi-sensory storytelling, a time sequential analysis. European Journal of Special Needs Education, Volume 30(4), pp. 535 - 550
Ten Brug, A., Van der Putten, A.A., Penne, A., Maes, B., & Vlaskamp, C. (2015). Factors Influencing Attentiveness of People With Profound Intellectual and Multiple Disabilities to Multisensory Storytelling. Journal of Policy and Practice in Intellectual Disabilities, Volume 12(3), pp. 190 - 198
Ten Brug, A., Van der Putten, A.A., Penne, A., Maes, B., & Vlaskamp, C. (2016). Making a difference? A comparison between multi‐sensory and regular storytelling for persons with profound intellectual and multiple disabilities. Journal of Intellectual Disability Research, Volume 60(11), pp. 1043 - 1053
Tenneij, N.H., & Koot, H.M. (2008). Incidence, types and characteristics of aggressive behaviour in treatment facilities for adults with mild intellectual disability and severe challenging behaviour. Journal of Intellectual Disability Research. Volume 52, pp.114 – 124
Test, D.W., Karvonen, M., Wood, W.M., Browder, D., & Algozzine, B. (2000). Choosing a self-determination curriculum: Plan for the future. Teaching Exceptional Children, Volume 33(2), pp. 48 – 54
Test, D.W., Mason, C., Hughes, C., Konrad, M., Neale, M., & Wood, W.M. (2004). Student involvement in individualized education program meetings. Exceptional Children, Volume 70, pp. 391 – 412
Thoma, C.A., Pannozzo, G.M., Fritton, S.C., & Bartholomew, C.C. (2008). A qualitative study of pre-service teachers’ understanding of self-determination for students with significant disabilities. Career Development for Exceptional Individuals, Volume 31, pp. 94 – 105
Thompson, B., & Guess, D. (1989). Students who experience the most profound disabilities: Teacher perspectives. In Brown, F., Lehr, D. (Eds.), Persons with profound disabilities: Issues and practices, pp. 3 - 41, Baltimore: Paul H. Brookes
Thompson, J.R., Bradley, V.J., Buntinx, W.H., Schalock, R.L., Shogren, K.A., Snell, M.E., Wehmeyer, M.L., Borthwick-Duffy, S., Coulter, D.L., Craig, E.M., Gomez, S.C., Lachapelle, Y., Luckasson, R.A., Reeve, A., Spreat, S., Tassé, M. J., Verdugo, M.A., & Yeager, M.H. (2009). Conceptualizing supports and the support needs of people with intellectual disability. Intellectual and Developmental Disabilities, Volume 47(2), pp. 135 – 146
Thye, M.D., Bednarz, H.M., Herringshaw, A.J., Sartin, E.B. & Kana, R.K. (2017). The impact of atypical sensory processing on social impairments in autism spectrum disorder. Developmental Cognitive Neuroscience, In Press
Tierney, E., Quinlan, D., & Hastings, R.P. (2007). Impact of a 3 day training course on challenging behaviour on staff cognitive and emotional responses. Journal of Applied Research in Intellectual Disabilities, Volume 20(1), pp. 58 – 63
Tilstone, C. (ed)(1991). Teaching Pupils with Severe Learning Difficulties. London: David Fulton Publishers.
Timmeren, E.A., Putten, A.A.J., Schrojenstein Lantman‐de Valk, H.M.J., Schans, C.P., & Waninge, A. (2016). Prevalence of reported physical health problems in people with severe or profound intellectual and motor disabilities: a cross‐sectional study of medical records and care plans. Journal of Intellectual Disability Research, Volume 60(11), pp. 1109 - 1118
Tipple, R. (1992). Art therapy with people who have severe learning difficulties. In - D. Waller & A. Gilroy (Eds.), Art therapy: A handbook, pp.105 – 124. Buckingham: Open University Press
Tipple, R. (1993). Challenging assumptions: The importance of transference processes in work with people with learning difficulties. Inscape: Journal of the British Association of Art Therapists, Volume 2, pp. 2 – 9.
Tohill, C., & Laverty, A. (2001). Sunshine, diet and mobility for healthy bones: an intervention study designed to implement these standards into the daily routine in an at risk population of adults with intellectual disability. Journal of Intellectual & Developmental Disability, Volume 26, pp. 217 - 231.
Tomlinson, J., Derrington, P., & Oldfield, A. (Eds.). (2012). Music Therapy in Schools: Working with Children of All Ages in Mainstream and Special Education. London: Jessica Kingsley.
Tomporowski, P.D., Beasman, K., Ganio, M.S., & Cureton, K. (2007). Effects of dehydration and fluid ingestion on cognition.
International Journal of Sports Medicine. Volume 28. pp. 891 - 896
Toolan, P., & Coleman, S. (1994). Music therapy, a description of process: Engagement and avoidance in five people with learning disabilities. Journal of Intellectual Disability Research, Volume 38, pp. 433 - 444.
Toolan, P., & Coleman, S. (1995). Music therapy, adscription of process: Engagement and avoidance in five people
with learning disabilities. British Journal of Music Therapy, Volume 9(1), pp. 17 - 24
Tota, A., Lancioni, G.E., Singh, N.N., O'reilly, M.F., Sigafoos, J., & Oliva, D. (2006). Evaluating the applicability of optic microswitches for eyelid responses in students with profound multiple disabilities. Disability and Rehabilitation: Assistive Technology, Volume 1(4), pp. 217 - 223
Totsika, V., Toogood, S., Hastings, R.P., & Lewis, S. (2008). Persistence of challenging behaviours in adults with intellectual disability over a period of 11 years. Journal of Intellectual Disability Research. Volume 52, pp. 446 – 457
Totsika, V., Felce, D., Kerr, M., & Hastings, R.P. (2010). Behavior problems, psychiatric symptoms, and quality of life for older adults with intellectual disability with and without autism. Journal of Autism and Developmental Disorders, 40(10), pp. 1171 – 1178
Touchette, P.E., MacDonald, R.F., & Langer, S.N. (1985). A scatter plot for identifying stimulus control of problem behavior. Journal of Applied Behavior Analysis, Volume 18, pp. 343 – 351
Trachtenberg, J.T., Chen, B.E., Knott, G.W., Feng, G., Sanes, J.R., Welker, E., & Svoboda, K. (2002). Long term in vivo imaging of experience-dependent synaptic plasticity in adult cortex. Nature, Volume 420(6917), pp. 788 – 795
Treffert, D.A. (1988). The idiot savant: A review of the syndrome. American Journal of Psychiatry, Volume 145(5), pp. 563 - 572
Treffert, D.A. (1989). Extraordinary people. Bantam Press
Trief, E. (2007). Research report: the use of tangible cues for children with multiple disabilities and visual impairments. Journal of Visual Impairment and Blindness, Volume 10 (10), pp. 613 – 619
Trief, E., Bruce, S.M., Cascella, P.W., & Ivy S. (2009). The development of a universal tangible symbol system. Journal of visual impairment & blindness. July 2009. pp. 425 - 431
Trief, E., Bruce, S.M., & Cascella, P.W. (2010). The selection of tangible symbols by educators of students with visual impairments and additional disabilities. Journal of Visual Impairment & Blindness. Volume 104 (8): pp. 499 - 504
Trief, E. (2013). STACS: Standardized tactual augmentative communication system. Louisville: American Printing House for the Blind.
Trief, E., Cascella, P.W., & Bruce, S.M. (2013). A Field Study of a Standardized Tangible Symbol System for Learners Who Are Visually Impaired and Have Multiple Disabilities, Journal of Visual Impairment & Blindness, May-June 2013. pp. 180 - 191
Trott, M., Laurel, M. K., & Windeck, S.L. (1993). SenseAbilities: Understanding Sensory Integration. Tucson: Therapy Skill Builders
Tsakiris, M. (2017). The multisensory basis of the self: From body to identity to others. The Quarterly Journal of Experimental Psychology, Volume 70(4), pp. 597 - 609
Tsiouris J.A., Mann R., Patti P.J. & Sturmey P. (2003). Challenging behaviours should not be considered as depressive equivalents in individuals with intellectual disability. Journal of Intellectual Disability Research, Volume 47, pp. 14 – 21
Turnbull, A.P., Turnbull, H.R., Erwin, E.J.,Soodak, L.C., & Shogren, K.A. (2010).Families, professionals, and exceptionality: A special partnership (3rd ed.). Upper Saddle River,NJ: Merrill/Prentice Hall.
Turner, F., & Shepherd, M. (2014). Doll Therapy in Dementia Care: A review of current literature. Communicare. Volume 1 (1)
Tyler, H. (2002). Working, Playing and Relating - Issues in Group Music Therapy for Children with Special Needs. In - A. Davies & E. Richards (Eds.), Music Therapy and Group Work: Sound Company, pp. 216 - 230. London: Jessica Kingsley.
Tynan, H., & Allen, D. (2002). The impact of service user cognitive level on carer attributions for aggressive behaviour. Journal of Applied Research in Intellectual Disabilities, Volume 15(3), pp. 213 – 223
Tyrer, F., McGrother, C. W., Thorp, C. F., Donaldson, M., Bhaumik, S., Watson, J. M., & Hollin, C. (2006). Physical aggression towards others in adults with learning disabilities: Prevalence and associated factors. Journal of Intellectual Disability Research, Volume 50, pp. 295 -
304
Tzu-Wei, Lin, & Yu-Min, Kuo (2013). Exercise Benefits Brain Function: The Monoamine Connection. Brain Sciences. Volume 3, pp. 39 - 53
Ullman, L., & Krasner, L. (Eds.) (1965). Case Studies in Behaviour Modification. New York: Holt, Rinehart and Winston
United Cerebral Palsy Associations, Inc. (1992). UCPA policy on communication access and free speech rights of Americans with disabilities. United Cerebral Palsy Associations, Inc. Policy manual. Washington, DC: UCPA
Utley Adelizzi, J., & Goss, D.B. (2001). Parenting Children with Learning Disabilities, Bergin and Garvey
Uyanik, M., Bumin, G., & Kayihan, H. (2003). Comparison of different therapy approaches in children with Down syndrome. Pediatrics International, Volume 45, pp. 68 – 73
Valdovinos M.G., Caruso M., Roberts C., Kim G., & Kennedy C.H. (2005). Medical and behavioural symptoms as potential side effects in adults with developmental disabilities. American Journal of Mental Retardation, Volume 110, pp. 164 – 70
Van De Sande, M.M., van Buul, V.J., & Brouns, F.J. (2014). Autism and nutrition: the role of the gut–brain axis. Nutrition Research Reviews, Volume 27(2), pp. 199 - 214
Van Delden, R., Reidsma, D., van Oorsouw, W., Poppe, R., van der Vos, P., Lohmeijer, A., Embregts, P., Evers, V., & Heylen, D. (2014). Towards an interactive leisure activity for people with PIMD. In - International Conference on Computers for Handicapped Persons, pp. 276 - 282. Springer, Cham.
Van den Broek, E.G.C., Janssen, C.G.C., van Ramhorst, T., & Deen, L. (2004). Mensen met een (zeer) ernstige meervoudige beperking en slechtziendheid. Een inventariserend onderzoek naar het visueel functioneren (People with a (very) multiple severe limitation and poor eyesight. A survey of visual functioning). Nederlands Tijdschrift voor de Zorg aan personen met verstandelijke beperkingen, Volume 30, pp. 254 – 266
Van der Gaag, A. (1988). The development of a communication assessment procedure for use with adults with a mental handicap - an interim report. The British Journal of Mental Subnormality, Volume 34(66), pp. 62 - 68
Van der Gaag, A. (1988). CASP: The Communication Assessment Profile for Adults with a Mental Handicap. Speech Profiles Limited
Van der Putten, A., Reynders, K., Vlaskamp, C., & Nakken, H. (2004). A functionally focused curriculum for children with profound multiple disabilities: A goal analysis. Journal Applied Research in Intellectual Disabilities, Volume 17(2), pp. 71 - 75
Van der Putten, A. (2005). Moving Toward Independence?: Evaluation of the" Mobility Opportunities Via Education" Curriculum with Children with Profound Intellectual and Multiple Disabilities. Rijksuniversiteit Groningen.
Van der Putten, A., Vlaskamp, C., Reynders, K., & Nakken, H. (2005). Children with profound intellectual and multiple disabilities: The effects of functional movement activities. Clinical Rehabilitation, Volume 19(6), pp. 613 – 620
Van der Putten, A., Vlaskamp, C., Reynders, K., & Nakken, H. (2005b). Movement skill assessment in children with profound multiple disabilities: a psychometric analysis of the Top Down Motor Milestone Test. Clinical Rehabilitation, Volume 19(6), pp. 635 - 643
Van der Putten, A., Vlaskamp, C., & Poppes, P. (2009). The content of support of persons with profound intellectual and multiple disabilities: An analysis of the number and content of goals in the educational programmes. Journal of Applied Research in Intellectual Disabilities, Volume 22, pp. 391 – 394.
Van der Putten, A., & Vlaskamp, C. (2011). Pain assessment in people with profound intellectual and multiple disabilities; a pilot study into the use of the pain behaviour checklist in everyday practice. Research in Developmental Disabilities, Volume 32(5), pp. 1677 – 1684
Van der Putten, A., & Vlaskamp, C. (2011b). Day services for people with profound intellectual and multiple disabilities: An analysis of thematically organized activities. Journal of Policy and Practice in Intellectual Disabilities, Volume 8(1), pp. 10 - 17
Van der Putten, A., Bossink, L.W.M., Frans, N., Houwen, S., & Vlaskamp, C. (2017). Motor activation in people with profound intellectual and multiple disabilities in daily practice, Journal of Intellectual & Developmental Disability, Volume 42(1), pp. 1 - 11
Van Dijk, J. (1965). Motor development in the education of deaf-blind children. Proceedings of the Conference on the deaf-blind, Refsnes, Denmark (pp. 41–47). Boston: Perkins School for the Blind.
Van Dijk, J. (1967). The non-verbal deaf-blind child and his world: His outgrowth towards the world of symbols. Proceedings of the Jaaverslag Institute voor Doven, 1964–1967 (pp. 73–110). Sint-Michielsgestel: Holland.
Van Dijk, J. (1986). An educational curriculum for deaf-blind multi-handicapped persons. In - D. Ellis (Ed.). Sensory Impairments in Mentally Handicapped People. London: Croom Helm
Van Hanegem, E., Enkelaar, L., Smulders, E., & Weerdesteyn, V. (2014). Obstacle course training can improve mobility and prevent falls in people with intellectual disabilities. Journal of Intellectual Disability Research, Volume 58(5), pp. 485 - 492
Van Oorsouw, W.M., Embregts, P.J., Bosman, A.M., & Jahoda, A. (2009). Training staff serving clients with intellectual disabilities: A meta-analysis of aspects determining effectiveness. Research in Developmental Disabilities, Volume 30, pp. 503 - 511
Van Timmeren, E.A., Van der Putten, A.A.J., Schrojenstein Lantman-de Valk, H.M.J., Schans, C. P., & Waninge, A. (2016). Prevalence of reported physical health problems in people with severe or profound intellectual and motor disabilities: A cross-sectional study of medical records and care plans. Journal of Intellectual Disability Research, Volume 60(11), pp. 1109 – 1118
Vargas, S., & Camilli, G. (1999). A meta-analysis of research on sensory integration treatment. American Journal of Occupational
Therapy, Volume 53, pp. 189 - 198
Veit, S.W., Allen, G.J., & Chinsky, J.M. (1976). Interpersonal interactions between institutionalized retarded children and their attendants. American Journal of Mental Deficiency, Volume 80(5), pp. 535 - 542
Vernon, M. (1972). Mind over mouth: A rationale for 'total communication'. Volta Review, Volume 74, pp. 529 - 540
Vernon, M. (1987). Sensory Impairments in Mentally Handicapped People. American Annals of the Deaf, Volume 132(1), pp. 4 - 4
Vinter, A., Mounoud, P., & Husain, O. (1983). Accuracy and Stability of Self-Image of Mentally Retarded Adults. American Journal of Mental Deficiency, Volume 87(6), pp. 583 - 590
Vlaskamp, C. (1999). Een eigen perspectief. Een programma voor mensen met ernstige meervoudige beperkingen (Your own perspective. A program for people with severe multiple disabilities). Assen: Van Gorcum.
Vlaskamp, C., & Nakken, H. (1999). Missing in execution therapies and activities for individuals with profound multiple disabilities. British Journal of Developmental Disabilities, Volume 45(2), pp. 99 - 109
Vlaskamp, C., & Verkerk, M.A. (2000). Zorg als proces – over zorgpraktijken en zorgvocabulaires (Care as a process - about care practices and care vocabularies). Dutch Journal of Care for persons with intellectual disabilities, Volume 26, pp. 4 – 16
Vlaskamp, C., & Oxener, G. (2002). Communicatie bij mensen met ernstige meervoudige beperkingen: Een overzicht van assessment en interventie methoden (Communication in people with severe multiple disabilities: An overview of assessment and intervention methods). Dutch Journal of Care for persons with intellectual disabilities, Volume 28, pp. 226 - 237
Vlaskamp, C., de Geeter, K.I., Huijsmans, L.M., & Smit, I.H. (2003). Passive activities: the effectiveness of multisensory environments on the level of activity of individuals with profound multiple disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 16(2), pp. 135 - 143
Vlaskamp, C. (2005). Assessing people with profound intellectual and multiple disabilities. In J. Hogg & A. Langa (Eds.), Assessing adults with intellectual disability: A service provider’s guide (pp. 152 - 163). Blackwell Publishers: Oxford.
Vlaskamp, C., Fonteine, H., & Tadema, A. (2005). Handleiding bij de lijst 'Alertheid van kinderen met zeer ernstige verstandelijke en meervoudige beperkingen. [Manual of the list 'Alertness in children with profound intellectual and multiple disabilities']. Groningen: Stichting Kinderstudies.
Vlaskamp, C., & Cuppen-Fonteine, H. (2007). Reliability of assessing the sensory perception of children with profound intellectual and multiple disabilities: A case study. Child Care, Health and Development, Volume 33(5), pp. 547 - 551
Vlaskamp, C., Hiemstra, S.J., & Wiersma, L.A. (2007). Becoming aware of what you know or need to know: Gathering client and context characteristics in day services for persons with profound intellectual and multiple disabilities. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(2), pp. 97 - 103
Vlaskamp, C., Hiemstra, S.J., Wiersma, L.A., & Zijlstra, B.J.H. (2007). Extent, duration, and content of day services' activities for persons with profound intellectual and multiple disabilities. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(2), pp. 152 - 159
Vlaskamp, C., & Nakken, H. (2008). Therapeutic interventions in the Netherlands and Belgium in support of people with profound intellectual and multiple disabilities. Education and Training in Developmental Disabilities, Volume 43(3), pp. 334 - 341
Vlaskamp, C., & Van der Putten, A. (2009). Focus on interaction: The use of an Individualized Support Program for persons with profound intellectual and multiple disabilities. Research in Developmental Disabilities, Volume 30(5), pp. 873 – 883
Vlaskamp, C., Fonteine, H., Tadema, A., & Munde, V.S. (2010). Manual for the “Alertness in people with profound intellectual and multiple disabilities” checklist. Groningen: Stichting Kinderstudies.
Vogeley, K., & Fink, G. R. (2003). Neural correlates for first-person perspective. Trends in Cognitive Sciences, Volume 7(1), pp. 38 – 42
Vogiatzoglou, A., Ockelford, A., Welch, G., & Himonides, E. (2011). Sounds of intent: Interactive software to assess the musical development of children and young people with complex needs. Music and Medicine, Volume 3(3), pp. 189 - 195
Von Tetzchner, S., & Martinsen, H. (1992). Introduction to Sign Teaching and the Use of Communication Aids. Whurr Publishers
Vos, P. de Cock, P., Petry, K., van den Noortgate, W., & Maes, B. (2010). What makes them feel like they do? Investigating the subjective well-being in people with severe and profound disabilities, Research in Developmental Disabilities, Volume 31(6), pp. 1623 – 1632
Vos, P., De Cock, P., Petry, K., Van den Noortgate, W., & Maes, B. (2010b). Do you know what I feel? A first step towards a physiological measure of the subjective well-being of persons with profound intellectual and multiple disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 23(4), pp. 366 - 378
Vos, P., de Cock, P., Munde, V., Neerinckx, H., Petry, K., Van Den Noortgate, W., & Maes, B. (2013). The role of attention in the affective life of people with severe or profound intellectual disabilities. Research in Developmental Disabilities, Volume 34(3), pp. 902 - 909
Vos, P. de Cock, P., Petry, K., van den Noortgate, W., & Maes, B. (2013). Investigating the relationship between observed mood and emotions in people with severe and profound intellectual disabilities, Journal of Intellectual Disability Research, Volume 57(5), pp. 440 – 451
Voss, M.W., Nagamatsu, L.S., Liu-Ambrose, T., & Kramer, A.F. (2011). Exercise, brain, and cognition across the life span. Journal of Applied Physiology, Volume 111, pp. 1505 – 1513
Vygotsky, L.S. (1993). The fundamentals of defectology. Translated by J.E. Knox & C.B. Stevens. In - Rieber, R.W. & Cartov, A.S. (Eds.).
The collected works of L.S. Vygotsky. New York and London: Plenum
Wachs, T.D., Moussa, W., Bishry, Z., Yunis, F., Sobhy, A.; McCabe, G., Jerome, N., Galal, O., Harrison, G, & Kirksey A. (1993). Relations between nutrition and cognitive performance in Egyptian toddlers. Intelligence. Volume 17(2). pp. 151 - 172
Walsh, R. (1997). When having means losing: Music therapy with a young adolescent with a learning disability and emotional and behavioural difficulties. British Journal of Music Therapy, Volume 11(1), pp. 13 - 19
Wang, J. (2014). Consumption of added sugars and development of metabolic syndrome components among a sample of youth at risk of obesity. Applied Physiology, Nutrition, and Metabolism, Volume 39(4), page 512
Waninge, A. (2011). Measuring physical fitness in persons with severe or profound intellectual and multiple disabilities. University of Groningen
Waninge, A., Evenhuis I.J., van Wijck, R., & Van der Schans, C.P. (2011). Feasibility and reliability of two different walking tests in people with severe intellectual and sensory disabilities. Journal of Applied Research in Intellectual Disabilities. Volume 24(6). pp. 518 - 527
Waninge, A., van der Putten, A.A., Stewart, R.E., Steenbergen, B., van Wijck, R., & van der Schans, C.P. (2013). Heart rate and physical activity patterns in persons with profound intellectual and multiple disabilities. Journal of Strength and Conditioning Research. Volume 27(11), pp. 3150 - 3158
Warburg, M. (1975). Blindness in mentally retarded children. Documenta Ophthalmologica, Volume 39(2), pp. 343 - 349
Warburg, M. (2001). Visual impairment in adult people with intellectual disability: literature review. Journal of Intellectual Disability Research, Volume 45(5), pp. 424 - 438
Ward, L., & Townsley, R. (2005). ‘It’s about a dialogue’: working with people with learning difficulties to develop accessible information. British Journal of Learning Disabilities, Volume 33 (2), pp. 59 - 64
Ward, M.J. (1988). The many facets of self-determination. National Information Center for Handicapped Children and Youth with handicaps:
Transition Issues, Volume 5, pp. 2 - 3
Ward, M.J. (1991). Self-determination revisited: Going beyond expectations. National Information Center for Handicapped Children and Youth with Handicaps: Transition Summary, Volume 7, pp. 3 - 5
Ward, M.J. (1996). Coming of age in the age of self-determination: A historical and personal perspective. In D. J. Sands & M. L. Wehmeyer (Eds.), Self-determination across the life span: Independence and choice for people with disabilities (pp. 1-14). Baltimore: Paul H. Brookes.
Ward, M.J., & Kohler, P. (1996). Promoting self-determination for individuals with disabilities: Content and process. In L. E. Powers, G. H. S. Singer, & J. Sowers (Eds.), Making our way: Building self-competence among children and youth with disabilities (pp. 275-290). Baltimore: Paul H. Brookes.
Ward, M.J., & Meyer, R.N. (1999). Self-determination for people with developmental disabilities and autism. Focus on Autism and Other Developmental Disabilities, Volume 14(3), pp. 133 – 139
Ware, J. (Ed.)(1994). Educating of Children With Profound and Multiple Learning Difficulties. London: David Fulton
Ware, J. (2003). Creating a responsive environment (second edition), David Fulton Publishers
Ware, J. (2004). Ascertaining the views of people with profound and multiple learning disabilities. British Journal of Learning Disabilities, Volume 32 (4), pp. 175 - 179
Ware, J., & Donnelly, V. (2004). Assessment for Learning for Pupils with PMLD – the ACCAC Insight Project, PMLD Link, Volume 16(3), Issue 49, pp. 12 - 17
Ware, J. (2005). Profound and Multiple Learning Difficulties. In: Lewis, A. and Norwich, B. (eds). Special Teaching for Special Children. Berkshire: Open University Press, pp. 67 - 80
Ware, J., Julian, G., & McGee, P. (2005). Education for children with severe and profound general learning disabilities in Ireland: factors influencing teachers’ decisions about teaching these pupils. European Journal of Special Needs Education. Volume 20(2), pp. 179 - 194
Ware, J. (2010). Understanding and promoting access for people with learning difficulties: seeing the opportunities and challenges of risk, European Journal of Special Needs Education. Volume 25(1), pp. 107 - 109
Warner, C. (2005). Music therapy with adults with learning difficulties and severe challenging behaviour. PhD, University of the West of
England. Available from: http://eprints.uwe.ac.uk/24593
Warren, S.A., & Mondy, L.W. (1971). To what behaviors do attending adults respond? American Journal of Mental Deficiency, Volume 75(4), pp. 419 - 455
Watson Genna, C. (2001). Tactile Defensiveness and Other Sensory Modulation Difficulties. Leaven, Volume 37(3), pp. 51 - 55
Watson, J., & Knight, C. (1991). An evaluation of intensive interaction teaching with pupils with severe learning difficulties, Child language, Teaching and Therapy, Volume 7(3) pp.10 - 25
Watson, J. (1994). Using Intensive Interaction in the education of pupils with PMLDs (ii) Intensive Interaction: two case studies, in Ware, J. (Ed.) Educating Children with Profound and Multiple Learning Difficulties. London: David Fulton.
Watson, J., & Fisher, A. (1997). Evaluating the effectiveness of Intensive Interactive teaching with pupils with profound and complex learning difficulties, British Journal of Special Education, Volume 24(2), pp. 80 - 87
Watson, J.S. (1972). Smiling, cooing, and 'The Game.' Merrill-Palmer Quarterly, Volume 18, pp. 323 - 339
Watson, T. (2002). Music Therapy with Adults with Learning Disabilities. In Bunt, L., & Hoskyns, S., (Eds.). The Handbook of Music Therapy, London: Routledge.
Watson, T., & Vickers, L. (2002). A Music and Art Therapy Group for People with Learning Disabilities. In Davies, A., & Richards, E., (Eds.) Music Therapy and Group Work: Sound Company, London: Jessica Kingsley.
Watson, T. (Ed.). (2007). Music Therapy with Adults with Learning Disabilities. Hove: Routledge.
Watson, T. (2007b). Working with people with profound and multiple learning disabilities in music therapy. In - Watson, T. (Ed.). Music Therapy with Adults with Learning Disabilities. Chapter 8, pp. 98 - 111. Hove: Routledge.
Weber, Y., & Westmoquette, K. (2010). Equine-Assisted Therapy as a Treatment Method for Children with Autism Spectrum Disorders
- a qualitative study. Department of Neurobiology, Care Sciences and Society, Karolinska Institute
Webster, M. (2008). Scientist finds fish are as clever as mammals - In Sarah Knapton article, Daily Telegraph, 29 Aug 2008
Wehman, P. (2013). Life beyond the classroom:Transition strategies for young people with disabilities (5th ed.). Baltimore, MD: Paul H. Brookes.
Wehmeyer, M.L., & Berkobien, R. (1991). Self-determination and self-advocacy: A case of mistaken identity. The Association for Persons with Severe Handicaps Newsletter, Volume 7(4)
Wehmeyer, M.L. (1992a). Self-determination and the education of students with mental retardation. Education and Training in Mental Retardation, Volume 27, pp. 302 - 314
Wehmeyer, M.L. (1992b). Self-determination: Critical skills for outcome oriented transition services. The Journal for Vocational Special Needs Education, Volume 15, pp. 3 - 9
Wehmeyer, M.L. (1993). Perceptual and psychological factors in career decision making of adolescents with and without cognitive disabilities. Career Development for Exceptional Individuals, Volume16, pp. 135 - 146
Wehmeyer, M.L. (1994). Perceptions of self-determination and psychological empowerment of adolescents with mental retardation. Education & Training in Mental Retardation & Developmental Disability, Volume 29 (1), pp. 9 - 21
Wehmeyer, M.L., & Kelchner, K. (1994). Interpersonal cognitive problem-solving skills of individuals with mental retardation. Education Training in Mental Retardation, Volume 29, pp. 265 - 278
Wehmeyer, M.L. (1995). A career education approach: Self-determination for youth with mild cognitive disabilities. Intervention in School and Clinic, Volume 30 (3), pp. 157 - 163
Wehmeyer, M.L., & Kelchner, K. (1995). The Arc's self-determination scale. Arlington, TX: The Arc National Headquarters.
Wehmeyer, M.L., & Kelchner, K. (1995). Interpersonal cognitive problem solving skills of individuals with mental retardation. Education and Training in Mental Retardation and Developmental Disabilities, Volume 29, pp. 265 - 278
Wehmeyer, M.L., & Metzler, C.A. (1995). How self-determined are people with mental retardation? The national consumer survey. Mental
Retardation, Volume 33 (2), pp. 111 - 119
Wehmeyer, M.L., Kelchner, K., & Richards, S. (1995). Individual and environmental factors related to the self-determination of adults with mental retardation. Journal of Vocational Rehabilitation, Volume 5, pp. 291 - 305
Wehmeyer, M.L., & Ward, M.J. (1995). The spirit of the IDEA mandate: Student involvement in transition planning. Journal of Vocational Special Needs Education, Volume 17, pp. 108 - 111
Wehmeyer, M.L. (1996a). Self-determination as an educational outcome: Why is it important to children, youth and adults with disabilities? In D.J. Sands & M.L. Wehmeyer (Eds.), Self determination across the life span: Independence and choice for people with disabilities (pp. 15 – 34). Baltimore, MD: Brookes.
Wehmeyer, M.L. (1996b). Student self-report measure of self-determination for students with cognitive disabilities. Education and Training in Mental Retardation and Developmental Disabilities, Volume 31, pp. 282 – 293
Wehmeyer, M.L., & Kelchner, K. (1996). Perceptions of classroom environment, locus of control and academic attributions of adolescents with and without cognitive disabilities. Career Development for Exceptional Individuals, Volume 19(1), pp. 15 - 29
Wehmeyer, M.L., Kelchner, K., & Richards, S. (1996). Essential characteristics of self-determined behaviors of adults with mental retardation and developmental disabilities. American Journal on Mental Retardation, Volume 100, pp. 632 - 642
Wehmeyer, M.L., & Schwartz, M. (1997). Self-determination and positive adult outcomes: A follow-up study of youth with mental retardation or learning disabilities. Exceptional Children, Volume 63, pp. 245 – 255
Wehmeyer, M.L. (1998). Self-determination and individuals with significant disabilities: Examining meanings and misinterpretations. Journal of The Association for Persons with Severe Handicaps, Volume 23 (1), pp. 5 - 16
Wehmeyer, M.L., & Sands, D.J. (1998). Making it happen: Student involvement in education planning, decision making, and instruction. Baltimore: Paul H. Brookes.
Wehmeyer, M.L., & Schwartz, M. (1998). The relationship between self-determination and quality of life for adults with mental retardation. Education and Training in Mental Retardation and Developmental Disabilities, Volume 33(1), pp. 3 – 12
Wehmeyer, M.L. (1999). A functional model of self-determination: Describing development and implementing instruction. Focus on Autism and Other Developmental Disabilities, Volume 14 (1), pp. 53 - 61
Wehmeyer, M.L., & Bolding, N. (1999). Self-determination across living and working environments: A matched-samples study of adults with mental retardation. Mental Retardation, Volume 37, pp. 353 – 363
Wehmeyer, M.L., Agran, M., & Hughes, C. (2000). A national survey of teacher's promotion of self-determination and student-directed learning. Journal of Special Education, Volume 34, pp. 58 - 68
Wehmeyer, M.L., Palmer, S.B., Agran, M., Mithaug, D.E., & Martin, J.E. (2000). Promoting causal agency: The self determined learning model of instruction. Exceptional Children, Volume 66, pp. 439 – 453
Wehmeyer, M.L., & Bolding, N. (2001). Enhanced self-determination of adults with intellectual disabilities as an outcome of moving to community-based work or living environments. Journal of Intellectual Disabilities Research, Volume 45, pp. 371 – 383
Wehmeyer, M.L, & Schalock, R.L. (2001). Self-Determination and Quality of Life: Implications for Special Education Services and Supports, Focus on Exceptional Children.
Wehmeyer, M.L., Abery, B., Mithaug, D.E., & Stancliffe, R.J.(2003). Theory in self-determination: Foundations for educational practice. Springfield, IL: Charles C Thomas.
Wehmeyer, M.L., & Garner, N.W. (2003). The impact of personal characteristics of people with intellectual and developmental disability on self-determination and autonomous functioning. Journal of Applied Research in Intellectual Disabilities, Volume 16, pp. 255 – 265
Wehmeyer, M.L., & Palmer, S.B. (2003). Adult outcomes from students with cognitive disabilities three years after high school: The impact of self-determination. Education and Training in Developmental Disabilities, Volume 38, pp. 131 – 144
Wehmeyer, M.L., Field, S.I., Doren, B., Jones, B., & Mason, C. (2004). Self-determination and student involvement in standards-based reform. Exceptional Children, Volume 70, pp. 413 - 425
Wehmeyer, M.L., Lawrence, M., Kelchner, K., Palmer, S., Garner, N., & Soukup, J. (2004). Whose Future Is It Anyway? A student directed transition planning process (2nd ed.). Lawrence, KS: Beach Center on Disability.
Wehmeyer, M.L. (2005). Self-determination and individuals with severe disabilities: Reexamining meanings and interpretations. Research and Practice for Persons with Severe Disabilities, Volume 30, pp. 113 – 120
Wehmeyer, M.L., Agran, M., Hughes, C., Martin, J., Mithaug, D.E., & Palmer, S.B. (2007). Promoting self-determination in students with intellectual and developmental disabilities. New York: Guilford.
Wehmeyer, M.L., & Field, S. (2007). Self-determination: Instructional and assessment strategies. Thousand Oaks, CA: Corwin Press.
Wehmeyer, M.L. (2008). The impact of disability on adolescent identity. In M. Sadowski (Ed.), Adolescents at school: Perspectives on youth, identity, and education (2nd ed., pp. 167 – 184). Cambridge: Harvard Education Press.
Wehmeyer, M.L., & Shogren, K.A. (2008). Self-determination and learners with autism spectrum disorders. In R. Simpson & B. Myles (Eds.), Educating children and youth with autism: Strategies for effective practice (2nd ed., pp. 433 – 476). Austin, TX: Pro-Ed.
Wehmeyer, M.L., Palmer, S.B., Lee, Y, Williams-Diehm, K.L., & Shogren, K.A. (2011). A randomized-trial evaluation of the effects of Whose Future is it Anyway? on self-determination. Career Development for Exceptional Individuals, Volume 34, pp. 45 - 56
Wehmeyer, M.L., Fields, S., & Thoma, C. (2012). Self-determination in adolescent transition education. In M. L. Wehmeyer & K. A. Webb (Eds.), Handbook of Adolescent Transition for Youth with Disabilities (pp. 171 - 190). New York: Routledge.
Wehmeyer, M.L., & Shogren, K.A. (2012). Self-determination: Getting students involved in leadership. In P. Wehman (Ed.), Life beyond the classroom: Transition strategies for young people with disabilities (5th ed., pp. 39 - 66). Baltimore: Paul H. Brookes.
Wehmeyer, M.L., Shogren, K.A., Palmer, S.B., Williams-Diehm, K.L., Little, T.D., & Boulton, A.(2012). The impact of the self-determined learning model of instruction on student self-determination. Exceptional Children, Volume 78, pp. 135 – 153
Wehmeyer, M.L., & Smith, T.E.C. (2012). Promoting self-determination and social inclusion: A review of research-based practices. In D. Zagar, M. L. Wehmeyer, & R. Simpson (Eds.), Educating students with autism spectrum disorders: Research-based principles and practices (pp. 227 - 246). New York: Taylor & Francis.
Wehmeyer, M.L., Tasse, M., Davies, D., & Stock, S. (2012). Support needs of adults with intellectual disability across domains: The role of technology. Journal of Special Education Technology, Volume 27 (2), pp.11 - 22
Wehmeyer, M.L. (2013). Self-determination: The most natural support. In M. L. Heward (Ed.), Exceptional children: An introductory survey of special education (10th ed., pp. 132 - 133). Upper Saddle River, NJ: Merrill/Prentice Hall.
Wehmeyer, M.L., & Abery, B.H. (2013). Self-Determination and Choice. Intellectual and Developmental Disabilities. Volume 51 (5), pp. 399 – 411
Wehmeyer, M.L., & Shogren, K.A. (2013). Self-determination and student involvement. In P. Wehman (Ed.), Life beyond the classroom: Transition strategies for young people with disabilities (5th ed., pp. 41 - 68). Baltimore: Paul H. Brookes.
Wehmeyer, M.L., & Little, T.D. (2013). Self-determination, positive psychology, and disability. In M.L. Wehmeyer (Ed.), Handbook of positive psychology and disability (pp. 116 - 136). Oxford, UK: Oxford University Press.
Wehmeyer, M.L., Palmer, S.B., Shogren, K.A., Williams-Diehm, K., & Soukup, J. (2013). Establishing a causal relationship between interventions to promote self-determination and enhanced student self-determination. Journal of Special Education, Volume 46(4), pp. 195 –210
Wehmeyer, M.L. (2014). Self-Determination: A Family Affair. Family Relations, Volume 63 (February): pp. 178 – 184
Wells, M.E., & Smith, D.W. (1983). Reduction of self-injurious behavior of mentally retarded persons using sensory integrative techniques. American Journal of Mental Deficiency, Volume 87, pp. 664 – 666
Welsh Assembly Government (2006). Routes for Learning: Assessment Materials for Learners with Profound Learning Difficulties and Additional Disabilities. Cardiff: Welsh Assembly Government
Werner, E.E., & Smith, R.S. (1980). An epidemiologic perspective on some antecedents and consequences of childhood mental health problems and learning disabilities. In S. Chess and A. Thomas (Eds.), Annual Progress in Child Psychiatry and Development. Brunner/Mazel, New York, pp.133 - 147
Werner, S. (2012). Individuals with Intellectual Disabilities: A Review of the Literature on Decision-Making since the Convention on the Rights of People with Disabilities (CRPD), Public Health Reviews,Volume 34 (2), pp. 1 - 27
Wertheimer, A. (ed.) (2000) Everyday Lives; Everyday Choices. London: The Foundation for People with Learning Disabilities.
Westergaard, G.C., & Hyatt, C.W. (1994). The responses of bonobos (Pan paniscus) to their mirror images: Evidence of self recognition.
Human Evolution, Volume 9(4), pp. 273 – 27
Wheeler, B.L. (1999). Experiencing Pleasure in Working with Severely Disabled Children. Journal of Music Therapy, Volume 36(1), pp. 56 - 80
Whitaker, S. (1989). Quality of life and people with a very profound handicap. British Journal of Mental Subnormality, Volume 35, pp. 3 - 7
White, B. (2015). ‘What sound can you make?’ A case study of a music therapy group for children with autism, learning disabilities and challenging behaviours. Approaches: An Interdisciplinary Journal of Music Therapy, Volume 7(2), pp. 197 - 206
Whiteley, P., Rodgers, J., Savery, D., & Shattock, P. (1999). A gluten-free diet as an intervention for autism and associated spectrum disorders: preliminary findings. Autism, Volume 3(1), pp. 45 - 65
Whiteley, P., Haracopos, D., Knivsberg, A.M., Reichelt, K.L., Parlar, S., Jacobsen, J., Seim, A., Pedersen, L., Schondel, M.. & Shattock, P. (2010). The ScanBrit randomised, controlled, single-blind study of a gluten-and casein-free dietary intervention for children with autism spectrum disorders. Nutritional Neuroscience, Volume 13(2), pp. 87 - 100
Whiteley, P., Shattock, P., Knivsberg, A.M., Seim, A., Reichelt, K.L., Todd, L., Carr, K., & Hooper, M. (2013). Gluten-and casein-free dietary intervention for autism spectrum conditions. Frontiers in Human Neuroscience. Volume 6, article 344, pp. 1 - 8
Whiteley, P. (2015). Nutritional management of (some) autism: a case for gluten-and casein-free diets? Proceedings of the Nutrition Society, Volume 74(3), pp. 202 - 207
Whitman, T.L. (1990). Self-regulation and mental retardation. American Journal on Mental Retardation, Volume 94 (4), pp. 347 - 362
Whittle, H., & Townend, S. (1995). Communication and technology for students with profound and multiple learning disabilities (PMLD) within the classroom setting. Communication Matters, Volume 9(2), pp. 15 - 16
Wier, K., Cooney, M., Walter, M., Moss, C., & Carter, E.W. (2011). Fostering self-determination among children with disabilities: Ideas
from parents for parents. Madison, WI: Natural Supports Project, Waisman Center, University of Wisconsin-Madison
Wiggs, L., & Stores, G. (1996) Severe sleep disturbance and daytime challenging behaviour in children with severe learning disabilities. Journal of Intellectual Disability Research. Volume 40(6), pp. 518 – 528
Wiggs, L., & Stores, G. (1998). Behavioural treatment for sleep problems in children with severe learning disabilities and challenging daytime behaviour: effect on sleep patterns of mother and child. Journal of Sleep Research, Volume 7(2), pp. 119 - 126
Wiggs, L., & Stores, G. (2004). Sleep patterns and sleep disorders in children with autistic spectrum disorders: insights using parent report and actigraphy. Developmental Medicine and Child Neurology, Volume 46(6), pp. 372 - 380
Wigram, A.L. (1988). Music therapy: Developments in mental handicap. Psychology of Music, Volume 16, pp. 42 – 51
Wigram, T., & DeBacker, J. (Eds.). (1999). Clinical Applications of Music Therapy in Developmental Disability, Pediatrics and Neurology. London: Jessica Kingsley.
Wigram, T., Pederson, I. N. & Bonde, L.O. (2002). A Comprehensive Guide to Music Therapy: Theory, Clinical Practice, Research and Training. London: Jessica Kingsley Publishers.
Wigram, T., & Lawrence, M. (2005). Music therapy as a tool for assessing hand use and communicativeness in children with Rett Syndrome. Brain & Development, Volume 27, pp. 95 - 96
Wilbarger P., & Wilbarger J. (1991). Sensory defensiveness in children. Santa Barbara, CA: Avanti Educational Programs.
Wilder, J., & Granlund, M. (2003). Behaviour style and interaction between seven children with multiple disabilities and their caregivers. Child: care, health and development, Volume 29(6), pp. 559 - 567
Wilkens, J. (2017). Photographic Memory: Photographic Memory Training, Advanced Techniques to Improve Your Memory & Strategies to Learn Faster. Create Space Independent Publishing Platform
Wilkinson, C. (1994). Teaching pupils with profound and multiple learning difficulties to exert control, in J. Coupe O’Kane & B. Smith (eds) Taking Control: enabling people with learning difficulties, London: David Fulton
Williams, C.A., Peters, S.U., & Calculator, S.N. (2009). Facts About Angelman Syndrome, 7th Edition, January 1, 2009. Angelman Syndrome Foundation
Williams, M. (2010). Meaningful participation for people with PMLD. PMLD Link. Volume 22(2), Issue 66, pp. 23
Williams, R.K. (1991). Choices, communication, and control: A call for expanding them in the lives of people with severe disabilities. In L. Meyer, C. Peck, L. Brown (Eds.), Critical Issues In The Lives Of People With Severe Disabilities (pp. 543 - 544). Baltimore: Paul H. Brookes.
Williams, S. Dagnan, D. Rodgers, J., & McDowell, K. (2012). Changes in attributions as a consequence of training for challenging and complex behaviour for carers of people with learning disabilities: A systematic review. Journal of Applied Research in Intellectual Disabilities, Volume 25(3), pp. 203 – 216
Williams-Diehm, K., Wehmeyer, M.L., Palmer, S., Soukup, J.H., & Garner, N. (2008). Self-determination and student involvement in
transition planning: A multivariate analysis. Journal on Developmental Disabilities, Volume 14(1), pp. 25 – 36
Willink, M., Widdershoven, G., van Schrojenstein Lantman-de Valk, H., Metsemakers, J. & Dinant, G. (2009). Autonomy in relation to health among people with intellectual disability: a literature review. Journal of Intellectual Disability Research, Volume 53(9), pp. 816 - 826
Willis, D., Grace, P.J., & Roy, C. (2008). A central unifying focus for the discipline: Facilitating humanization, meaning, choice, quality of life, and healing in living and dying. Advances in Nursing Science, Volume 31(1), pp. 28 - 40
Willner, P., Bailey, R., Parry, R., & Dymond, S. (2010). Performance in temporal discounting tasks by people with intellectual disabilities reveals difficulties in decision-making and impulse control. American Journal on Intellectual and Developmental Disabilities. Volume 115, pp. 157 - 171
Willoughby-Booth, S. & Pearce, J. (1998). On the edge: Art therapy for people with learning difficulties and disordered personalities. In M. Rees (Ed.), Drawing on difference: Art therapy with people who have learning difficulties, pp.63 – 78. London: Routledge.
Wilson, E.B. (1975). Sensory integration therapy for children with learning disorders. Rehabilitation in Australia, Volume 12, 27 – 29
Wilson, M.M., & Morley, J.E. (2003). Impaired cognitive function and mental performance in mild dehydration. European Journal of Clinical Nutrition. Volume 57(2), Supplement. pp. 24 - 29
Wilson, P.G., Reid, D.H., Phillips, J.F., & Burgio, L.D. (1984). Normalization of institutional mealtimes for profoundly retarded persons: Effects and non-effects of teaching family-style dining. Journal of Applied Behavior Analysis, Volume 17, pp. 189 - 201
Wilson, P.G., Reid, D.H., & Green, C.W. (2006). Evaluating and increasing in-home leisure activity among adults with severe disabilities in supported independent living. Research in Developmental Disabilities, Volume 27(1), pp. 93 - 107
Wilson, T.D. (2009). Know thyself, Perspectives in Psychological Science, Volume 4, pp. 384 – 389
Winchel, R.M., & Stanley, M. (1991). Self-injurious behaviour: a review of the behaviour and biology of self-mutilation. The American Journal of Psychiatry, Volume 148(3), pp. 306 - 317
Windsor, J., Piche, L.M. & Locke, P.A. (1994). Preference testing: a comparison of two presentation methods. Research in Developmental Disabilities, 15, pp. 439 - 455
Winefield, A.H. (1983). Cognitive performance deficits induced by exposure to response-independent positive outcomes. Motivation and Emotion, Volume 7, pp. 145 - 155
Wise, J. (2011). Shared decision making must move from rhetoric to reality, says King’s Fund. BMJ, 2011; 343: d4734
Wolf, J., & Joannou, K. (2012), Choice Making and Individuals with Significant Disabilities, University of Kansas
Wolf-Schein, E. (1998). Considerations in Assessment of Children with Severe Disabilities including Deaf-blindness and Autism. International Journal of Disability, Development and Education, Volume 45(1). pp. 35 - 55
Wong, J.G., Clare, I.C.H., Holland, A.J., Watson, P.C., & Gunn, M. (2000). The capacity of people with a ‘mental disability’ to make a health care decision. Psychological Medicine, Volume 30, pp. 295 - 306
Wood, D., Wood, H., Griffiths, A., & Howarth, A. (1986). Teaching and talking with deaf children. J. Wiley and Sons
Wood, W.M., Fowler, C.H., Uphold, N., & Test, D.W. (2005). A review of self- determination interventions with individuals with severe disabilities. Research & Practice for Persons with Severe Disabilities, Volume 30 (3), pp. 121 - 146
Woodcock, J., & Lawes, C. (1995). Music Therapy and People with Severe Learning Difficulties who Exhibit Self-injurious Behaviour. In: Wigram, T., Saperston, B., & West, R., (Eds.),The Art and Science of Music Therapy: a Handbook, London: Harwood Academic Press.
Woollett, K. & Macguire, E.A. (2011). Acquiring “the Knowledge” of London's Layout Drives Structural Brain Changes. Current Biology. Volume 21(24-2). pp. 2109 – 2114
Wragg, T. (1996). Year of the twerp and big chief I-spy. Last Word. Times Educational Supplement. No. 4138, Friday January 5th, page 64
Wyatt, M. (2001). The Disabled Enclave: Issues in the Dance Movement Therapist’s Counter transference with Severely Handicapped Adolescents. Master of Arts in Dance Movement Therapy, Unpublished Dissertation presented to the faculty of Laban Centre, London. Goldsmith, University of London
Wylie, M.E. (1983). Eliciting Vocal Responses in Severely and Profoundly Mentally Handicapped Subjects. Journal of Music Therapy, Volume 20(4), pp. 190 - 200
Wyman, R. (1986). Multiply handicapped children. Souvenir Press
Wyman, R. (2000). Making Sense Together: Practical approaches to supporting children who have multisensory impairments. Second Edition. Human Horizons Series
Wynn, K. (1992). Addition and subtraction by human infants. Nature, Volume 358(6389), pp. 749 - 750
Yack, E., Sutton, S., & Aquilla, P. (1998). Building bridges through sensory integration. Willowdale, Ontario: Special Needs Project.
Yamaki, K. (2005). Body weight status among adults with intellectual disability in the community. Mental Retardation, Volume 43(1), pp. 1 - 10
Yang, L.J. (2003). Combination of extinction and protective measures in the treatment of severely self-injurious behaviour. Behavioural Interventions, Volume 18, pp. 109 - 121
Yang, Q., Zhang, Z., Gregg, E., Flanders, D., Merritt, R., & Hu, F. (2014). Added Sugar Intake and Cardiovascular Diseases Mortality Among US Adults. JAMA Internal Medicine, Volume 174 (4), pp. 516 - 524
Yasuhara, A., & Sugiyama, Y. (2001). Music therapy for children with Rett syndrome. Brain & Development, Volume 23, pp. 82 - 84.
York, J., Nietupski, J., & Hamre-Nietupski, S. (1985). A decision making process for using microswitches. Journal of the Association for the Severely Handicapped, Volume 10, pp. 214 - 223
Yu, C.T., Spevack, S., Hiebert, R., Martin, T.L., Goodman, R., Martin, T.G., Harapiak, S. & Martin, G.L. (2002). Happiness indices among persons with profound and severe disabilities during leisure and work activities. Education and Training in Mental Retardation and Developmental Disabilities. Volume 37(4), pp. 421 – 426
Yu, C.T., & Martin, G.L. (2003). Tangibles, Pictures, and Verbal Descriptions: Which Should Be Used in Choice Presentations? Journal on Developmental Disabilities. Volume 10(1), pp. 137 -140
Yudkin, J. (1972). Pure, White and Deadly: The Problem of Sugar. London: Davis-Poynte
Yudkin, J. (2012). Pure, White and Deadly: The Problem of Sugar (revised edition). Penguin
Zainuddin, M.S.A., & Thuret, S. (2012). Nutrition, adult hippocampal neurogenesis and mental health. British Medical Bulletin. Volume 103(1). pp. 89 -114
Zangari, C., Lloyd, L., & Vicker, B. (1994). AAC: An historic perspective, AAC, March 1994, Volume 10 (1), pp. 27 - 59
Zeedyk, M.S., Davies, C.E., Parry, S., & Caldwell, P. (2009).Fostering social engagement in Romanian children with communicative impairments: The experiences of newly trained practitioners of Intensive Interaction, British Journal of Learning Disabilities, Volume 37(3), pp.186 - 196
Zeedyk, M.S., Caldwell, P., & Davies, C.E. (2009). How rapidly does Intensive Interaction promote social engagement for adults with profound learning disabilities and communicative impairments? European Journal of Special Needs Education, Volume 24(2), pp.119 – 137
Zeng Y., Zhao Y., & Bai J. (2016). Towards Robot Self-consciousness (I): Brain-Inspired Robot Mirror Neuron System Model and Its Application in Mirror Self-recognition. In - Liu CL., Hussain A., Luo B., Tan K., Zeng Y., Zhang Z. (Eds.). Advances in Brain Inspired Cognitive Systems. Lecture Notes in Computer Science, Volume 10023. Springer, Cham
Zhang, D., Wehmeyer, M.L, & Chen, L. (2005). Parent and teacher engagement in fostering the self-determination of students with disabilities: A comparison between the United States and the Republic of China. Remedial and Special Education, Volume 26, pp. 55 - 64
Zhang, J., Mayton, M. R., & Wheeler, J.J. (2013). Effectiveness of gluten-free and casein-free diets for individuals with autism spectrum disorders: An evidence-based research synthesis. Education and Training in Autism and Developmental Disabilities, Volume 48(2), pp. 276 - 287
Zhou, L., Iwata, B.A., Goff, G.A., & Shore, B.A. (2001). Longitudinal analysis of leisure-item preferences. Journal of Applied Behavior Analysis, Volume 34, pp. 179 – 184
Zijlstra, H.P., Vlaskamp, C., & Buntinx, W.H. (2001). Direct-care staff turnover: An indicator of the quality of life of individuals with profound multiple disabilities. European Journal on Mental Disability, Volume 22, pp. 39 – 56
Zijlstra, R. (2003). Dancing with elephants. A study of the implementation of the education program in the care for people with severe multiple disabilities. Groningen: Stichting Kinderstudies.
Zijlstra, R., & Penning, C. (2004). People with severe intellectual and multiple disabilities. In - M. Kersten & D. Flikweert (Eds.), Onderzoek over grenzen thematische rapportages en beschouwingen naar aanleiding van het 12de IASSID, Montpellier 2004 (pp. 49 – 63). Utrecht: NGBZ en LKNG/NIZW
Zijlstra, H.P., & Vlaskamp, C. (2005). Leisure provision for persons with profound intellectual and multiple disabilities: quality time or killing time? Journal of Intellectual Disability Research, Volume 49(6), pp. 434 - 448
Zijlstra, H.P., & Vlaskamp, C. (2005b). The impact of medical conditions on the support of children with profound intellectual and multiple disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 18(2), pp. 151 - 161
Zilbovicius, M., Garreau, B., Tzourio, N., Mazoyer, B., Bruck, B., Martinot, J.L., Raynaud, C., Samson, Y., Syrota, A., & Lelord, G. (1992). Regional cerebral blood flow in childhood autism: a SPECT study. American Journal of Psychiatry, Volume 149(7), pp. 924 - 930
Zissermann, L. (1992). The effects of deep pressure on self stimulating behaviors in a child with autism and other disabilities. American Journal of Occupational Therapy, Volume 46, pp. 547 – 551
Ziviani, J., Poulsen, A., & O'Brien, A. (1982). Effect of a sensory integrative/neurodevelopmental programme on motor and academic
performance of children with learning disabilities. Australian Occupational Therapy Journal, Volume 29, pp. 27 - 33
Zuckerman, M., Porac, J., Lathin, D., & Deci, E.L. (1978). On the Importance of Self‐Determination for Intrinsically‐Motivated Behavior. Personality and Social Psychology Bulletin, Volume 4 (3), pp. 443 ‐ 446
Zull, J.E. (2004). The art of changing the brain. Educational Leadership, Volume 62(1), 68 - 72
Please note that items are arranged alphabetically by primary author and then by date order for each reference listed under that source.
Please note that items highlighted in blue provide a link to the original article such that you may read it for yourself. While the links were active at the time of composing this webpage they may become inactive at some future point; apologies if this is the case.
If TalkSense has cited a source on this webpage which is not referenced below please use the above contact form to let us know such that we may correct this issue.
Abery, B.H., Arndt, K., Greger, P., Tetu, L., Eggebeen, A., Barosko, J., & Rudrud, L. (1994). Self-determination for youth with disabilities: A family education curriculum. Minneapolis, MN: University of Minnesota, Institute on Community Integration
Abery, B.H., McGrew, K., & Smith, J. (1994). Validation of an ecological model of self-determination
for children with disabilities (Technical Report No. 2). Minneapolis, MN: University of Minnesota, Institute on Community Integration.
Abery, B.H., & Eggebeen, A. (1995). Findings from a field-test of a self-determination capacity building curriculum (Technical Report No. 3). Minneapolis, MN: University of Minnesota, Institute on Community Integration.
Abery, B.H., Stancliffe, R.J., Smith, J., McGrew, K., & Eggebeen, A. (1995a). Minnesota opportunities and exercise of self-determination scale - Adult edition. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living.
Abery, B.H., Stancliffe, R.J., Smith, J., McGrew, K., & Eggebeen, A. (1995b). Minnesota self-determination skills, attitudes, and knowledge evaluation scale - Adult edition. Minneapolis, MN: University of Minnesota, Institute on Community Integration, Research and Training Center on Community Living.
Abery, B.H., & Stancliffe, R.J. (1996). The ecology of self-determination. In D.J. Sands & M.L. Wehmeyer (Eds.), Self-determination
across the life span: Independence and choice for people with disabilities (pp. 111 – 145). Baltimore, MD: Paul H. Brookes.
Abery, B.H., Simunds, E., & Cady, R. (2002). The Minnesota health care self-determination scales. Minneapolis, MN: University of Minnesota, Institute on Community Integration.
Abery, B.H., & Stancliffe, R.J. (2003). A tripartite theory of self-determination. In M.L. Wehmeyer, B.H. Abery, D.E. Mithaug, & R.J.
Stancliffe (Eds.), Theory in self-determination: Foundations for educational practice (pp. 43 – 78). Springfield, IL: Charles C Thomas Publisher.
Abery, B.H., Simunds, E., & Cady, R. (2006). The impact of health care coordination on the lives of adults with physical disabilities (Technical Report No. 2). Minneapolis, MN: University of Minnesota, Institute on Community Integration.
Abery, B.H., & Ticha, R. (2012). Direct support professionals: Core competencies and their impact on self-determination. Paper presented
at the International Association for the Scientific Study of Intellectual Disabilities World Congress, Halifax, N.S., Canada
Adamek, M.S., & Darrow, A. (2005). Music in Special Education. Silver Springs: MD, The American Music Therapy Association
Adams, D. & Oliver, C. (2011). The expression and assessment of emotions and internal states in individuals with severe or profound intellectual disabilities. Clinical Psychology Review, Volume 31(3), pp. 293 – 306
Adams, G., Tallon, R., & Stangl, J. (1980). Environmental influences on self stimulatory behaviour. American Journal of Mental Deficiency, Volume 85, pp. 171 - 175
Adams, M., & Oldfield, A. (1990). The effects of music therapy on a group of profoundly mentally handicapped adults. Journal of Mental Deficiency Research, Volume 34(2), pp. 107 - 125.
Ager, A., & O’May, F. (2001). Issues in the definition and implementation of “best practice” for staff delivery of interventions for challenging behaviour. Journal of Intellectual and Developmental Disability, Volume 26(3), pp. 243 - 256
Agrotou, A. (1998). Psychodynamic Group Music Therapy with Profoundly Learning Disabled Residents and their Carers: Developing a Theory and Practice for Practice for the Realisation of Therapeutic Aims for Residents and the Acquirement of Therapist's Skills by Carers. Unpublished Doctoral Thesis. University of Sheffield.
Agrotou, A. (1999). Sounds and Meaning: Group Music Therapy with People with Profound Learning Difficulties and their Carers. London: Lumiere.
Aharoni, H. (2005). Adapted physical activities for the intellectually challenged adolescent: psychomotor characteristics and implications for programming and motor intervention. International Journal of Adolescent Medicine and Health, Volume 17(1), pp. 33 - 47
Aiken, J.M., & Salzberg, C.L. (1984). The effects of a sensory extinction procedure on stereotypic sounds of two autistic children. Journal of Autism and Developmental Disorders, Volume 14(3), pp. 291 - 299
Ainscow, M., & Tweddle, D. (1979). Preventing classroom failure: An objectives approach. Wiley
Aird, R. (2001). The Education and Care of Children with Severe, Profund and Multiple Learning Disabilities. David Fulton Publishers
Aitken, S., Buultjens, M., & Spungin, S. (Eds)(1990). Realities and Opportunities. Early Intervention with Visually Handicapped Infants and Young Children. American Foundation for the Blind: New York.
Aitken, S., & Buultjens, M. (1991). Visual Assessments of Children with Multiple Impairments: A Survey of Ophthalmologists. Journal of Visual Impairment and Blindness, Volume 85(4), Volume 170 - 173
Aitken, S., & Buultjens, M. (1992). Vision for Doing: Assessing Functional Vision of Learners who are Multiply Disabled. Sensory Series No. 2. Moray House Publications
Aitken, S., Buultjens, M., Clark, C., Eyre, J. T., & Pease, L. (2000). Understanding deafblindness. Teaching children who are deafblind: Contact communication and learning, pp. 1 - 34
Aldridge, D., Gustorff, D., & Neugebauer, L. (1995a). A preliminary study of creative music therapy in the treatment of children with developmental delay. The Arts in Psychotherapy, Volume 22(3), pp. 189 - 205.
Aldridge, D., Gustroff, D., & Neugebauer, L. (1995b). A pilot study of music therapy in the treatment of children with developmental delay. Complementary Therapies in Medicine, Volume 3(4), pp. 197 - 205.
Algozzine, B., Browder, D., Karvonen, M., Test, D.W., & Wood, W.M. (2001). Effects of interventions to promote self-determination for individuals with disabilities. Review of Educational Research, Volume 71(2), pp. 219 – 277.
All, A.C., Loving, G.L., & Crane, L.L. (1999). Animals, horseback riding, and implications for rehabilitation therapy. Journal of Rehabilitation, Volume 65(3), pp. 49 – 57
Allen, C. (2001). A Framework for Learning: For Adults with Profound and Complex Learning Difficulties. David Fulton
Allen, D., Mcdonald, L., Dunn, C., & Doyle, T. (1997). Changing care staff approaches to the prevention and management of aggressive behaviour in a residential treatment unit for persons with mental retardation and challenging behaviour. Research in Developmental Disabilities. Volume 18(2), pp.101 - 112
Alvin, J., & Warwick, A. (1991). Music Therapy for the Autistic Child. Oxford: Oxford University Press
Amaral, I., & Celizic, M. (2015). Quality indicators in the education of children with Profound Intellectual and Multiple Disabilities. Da Investigação às Práticas, Volume 5(2), pp. 112 - 125
Amen, D.G. (2010). Change your brain: Change your body. Three Rivers Press
Amen, D.G. (2016). Change Your Brain, Change Your Life: Revised and Expanded Edition: The breakthrough programme for conquering anxiety, depression, anger and obsessiveness. Piatkus
Amen, D.G. (2017). Memory Rescue: Supercharge Your Brain, Reverse Memory Loss, and Remember What Matters Most. Tyndale Momentum
Amsterdam, B. (1972). Mirror self-image reactions before the age 2. Developmental Psychobiology, Volume 5, pp. 297 – 305
Anderson, J.R. (1994). The monkey in the mirror: The strange conspecific. In Self-awareness in animals and humans: Developmental perspectives, ed. R. W. Mitchell, S.T. Parker, & M.L. Boccia, pp. 315 - 329. New York: Cambridge University Press
Angell, A. (2010). Selective Eaters and Tactile Sensitivity A Review of Classification and Treatment Methods That Address Anxiety and Support a Child’s Need for a Sense of Control. Childhood Obesity and Nutrition. Volume 2(5), pp. 299 - 303
Antaki, C., Finlay, W., Walton, C., & Pate, L. (2008). Offering choices to people with intellectual disabilities: an interactional study. Journal of Intellectual Disability Research, Volume 52(12), pp. 1165 - 1175
Apostolova, L.G., & Thompson, P.M. (2007). Brain Mapping as a Tool to Study Neurodegeneration. Neurotherapeutics: The Journal of the American Society for Experimental NeuroTherapeutics. Volume 4, pp. 387 – 400
Appleton, P.L., Mincham, P.E., Ellis, N.C., Elliott, C.E., Boll, V., & Jones, P. (1994). The self-concept of young people with spina bifida: A population-based study. Developmental Medicine and Child Neurology, Volume 36, pp. 198 - 215
Aquilla, P., Sutton, S., & Yack, E. (2003). Building Bridges Through Sensory Integration. Future Horizons.
Arendt, R., MacLean, W. E., Jr., & Baumeister, A. (1988). Critique of sensory integration therapy and its application in mental retardation.
American Journal on Mental Retardation, Volume 92, pp. 401 - 411
Ari, C., & D’Agostino, D.P. (2016). Contingency checking and self-directed behaviors in giant manta rays: Do elasmobranchs have self-awareness? Journal of Ethology, Volume 34(2), pp.167 – 174
Arkwright, N. (1998). An Introduction to Sensory Integration. San Antonio, Texas: therapy Skill Builders
Armstrong, L.E., Ganio M.S., Casa D.J., Lee E.C., McDermott B.P., Klau J.F., Jimenez L., Le Bellego L., Chevillotte E., & Lieberman H.R. (2012) Mild dehydration affects mood in healthy young women. Journal of Nutrition. Volume 142. pp. 382 - 388
Arthur, M., Hook, J., & Butterfield, N. (1995). Behavior state: Exploring issues in best practice for students with the most severe and multiple disabilities. Australasian Journal of Special Education, Volume 19, pp. 37 - 44
Arthur, M. (2000). Behavior states and a half-full glass: A response to Mudford, Hogg, and Roberts. American Journal on Mental Retardation, Volume 105(6), pp. 509 - 511
Arthur, M., & Foreman, P. (2002). Educational programming for students with high support needs: Report data from teachers, paraprofessionals and other professionals working in Australian schools. Developmental Disabilities Bulletin, Volume 30, pp.115 – 39
Arthur, M. (2003). Socio-communicative variables and behavior states in students with profound and multiple disabilities: Descriptive data from school settings. Education and Training in Developmental Disabilities, Volume 38(2), pp. 200 - 219
Arthur, M. (2004). Patterns amongst behavior states, sociocommunicative, and activity variables in educational programs for students with profound and multiple disabilities. Journal of Development and Physical Disabilities, Volume 16(2), pp. 125 - 149
Arthur-Kelly, M., Bochner, S., Center, Y., & Mok, M. (2007). Socio-communicative perspectives on research and evidence-based practice in the education of students with profound and multiple disabilities. Journal of Developmental and Physical Disabilities, Volume 19(3), pp. 161 – 76.
Arthur-Kelly, M., Foreman, P., Bennett, D., & Pascoe, S. (2008).Interaction, inclusion and students with profound and multiple disabilities: towards an agenda for research and practice. Journal of Research in Special Educational Needs, Volume 8(3), pp. 161 – 166
Arthur-Kelly, M., Bennett, D., Neilands, J., & Foreman, P. (2014). Case Reflections on Communication Support for Students with Multiple and Severe Disability in Australian General Classrooms. Journal of International Special Needs Education, Volume 17(2), pp. 70 - 78
Arthur-Kelly, M., Foreman, P., Maes, B., Colyvas, K., & Lyons, G. (2017). Observational Data on Socio-Communicative Phenomena in Classrooms Supporting Students with Profound Intellectual and Multiple Disability (PIMD): Advancing Theory Development on Learning and Engagement Through Data Analysis. Advances in Neurodevelopmental Disorders, pp. 1 - 13
Ashby, E. (2011). Resourceful, skillful and flexible: Art therapy with people who have severe learning disabilities and challenging behaviour. In - A. Gilroy (Ed.) Art therapy research in practice, pp.159 – 180. London: Routledge.
Ashby, M., Lindsay, W.R., Pitcaithly, D., Broxholme, S., & Geelen, N. (1995). Snoezelen: Its effects on concentration and responsiveness in people with profound multiple handicaps. British Journal of Occupational Therapy, Volume 58(7), pp. 303 - 307.
Association of Teachers and Lecturers (2013): Achievement For All: Working with children with special educational needs in mainstream schools and colleges, ATL
Augusta, C., Burd, C., Pica, M., & Schroeder, T. (2012). “Sing a song of six paints”: A collaborative approach to art and music in the classroom. Closing the Gap Magazine, Volume 30(6), pp. 24 - 28
Ault, M.M., Guy, B., Rues, J., Noto, L., & Guess, D. (1994). Some educational implications for students with profound disabilities at risk for inadequate nutrition and the nontherapeutic effects of medication. Mental Retardation, Volume 32(3), pp. 200 - 205
Ayres, A.J. (1963). The development of perceptual–motor abilities: A theoretical basis for treatment of dysfunction (Eleanor Clarke Slagle Lecture). American Journal of Occupational Therapy, Volume 17, pp. 221 – 225
Ayres, A.J. (1964). Tactile Functions: Their Relations to Hyperactive and Perceptual Motor Behaviour. American Journal of Occupation Therapy, Volume 18(1), pp. 221 - 225
Ayres, A.J. (1970). Sensory Integration and the Child. Western Psychological Services
Ayres, A.J. (1972). Improving academic scores through sensory integration. Journal of Learning Disabilities, Volume 5, pp. 338 – 343.
Ayres, A.J. (1973). Sensory Integration and Learning Disorders. Western Psychological Services.
Ayres, A.J. (1974). The Development of Sensory Integrative Theory and Practice: A Collection of the Works of A. Jean Ayres. Kendall/Hunt Publishing Co
Ayres, A.J. & Tickle, L. (1980). Hyper-responsivity to Touch and Vestibular Stimulation as a Predictor or Responsivity to sensory Integrative Procedure by Autistic Children. American Journal of Occupation Therapy, Volume 34, pp. 375 - 381
Ayres, A.J., Erwin, P.R., & Mailloux, Z. (2004). Love, Jean: Inspiration for Families Living With Dysfunction of Sensory Integration. Crestport Press
Azeredo, M. (2007). Real-time composition of image and sound in the (re)habilitation of children with special needs: A case study of a child with cerebral palsy. Digital Creativity, Volume 18(2), pp. 115 - 120.
Azrin, N.H., Hutchinson, R.R., & Sallery, R.D. (1964). Pain-aggression toward inanimate objects. Journal of the Experimental Analysis of Behavior, Volume 7, pp. 223 - 228.
Azrin, N.H., & Foxx, R.M. (1971). A rapid method of toilet training the institutionalized retarded. Journal of Applied Behavior Analysis, Volume 4, pp. 89 - 99
Azrin, N.H., Schaeffer, R.M., & Wesolowski, M.D. (1976). A rapid method of teaching profoundly retarded persons to dress by a reinforcement - guidance method. Mental Retardation. Volume 14(6), pp. 29 - 33
Bach-y-Rita, P., & Kercel, S.W. (2003). Sensory substitution and the human–machine interface. Trends in Cognitive Sciences, Volume 7(12), pp. 541 - 546
Bagadia, N., Berta, J., Kobs, R., Mahan, T., & Myers, K. (2001). Sensory Substitution for Vestibular Function Deficit. University of Wisconsin-Madison
Bailey, B.A. Hare, D.J., Hatton, C., & Limb, K. (2006). The response to challenging behaviour by care staff: Emotional responses, attributions of cause and observations of practice. Journal of Intellectual Disability Research, Volume 50(3), pp. 199 – 211
Bailey, J.S., & Meyersen, L. (1969). Vibration as a reinforcer with a profoundly retarded child. Journal of Applied Behavior Analysis, Volume 2, pp. 135 - 137
Bailey, M. (1983). Structuring a Curriculum for Profoundly Mentally Handicapped Children. Jordanhill Project. Glasgow
Baillargeon, R., Spelke, E.S., & Wasserman, S. (1985). Object permanence in five-month-old infants. Cognition, Volume 20(3), pp. 191 - 208
Baillargeon, R. (1987). Object permanence in 3½-and 4½-month-old infants. Developmental Psychology, Volume 23(5), pp. 655 - 664
Baker, D.J., Fox, J., & Albin, R.W. (1995). Staff support strategies to increase the involvement of individuals with disabilities in meal preparation. Behavioral Interventions, Volume 10(4), pp. 197 - 210
Baker, F.A., Berlowitz, D.J., Grocke, D., & Tamplin, J. (2014). Thematic analysis of the experience of group music therapy for people with chronic quadriplegia. Topics in Spinal Cord Injury Rehabilitation, Volume 20(3), pp. 236 - 247.
Baker, L.B., Conroy, D.E., & Kenney, W.L. (2007). Dehydration impairs vigilance-related attention in male basketball players. Medicine & Science in Sports & Exercise. Volume 39. pp. 976 - 983
Balcombe, J. (2016). What a Fish Knows: The Inner Lives of Our Underwater Cousins. Scientific American
Baldwin, J.M. (1895). Mental development in the child and the race: Methods and processes. New York: Macmillan
Bambara, L.M., Ager, C., & Koger, F. (1994). The effects of choice and task preference on the work performance of adults with severe disabilities. Journal of Applied Behavior Analysis, Volume 27(3), pp. 555 - 556.
Bandura, A. (1977). Self-efficacy: toward a unifying theory of behavioral change, Psychological Review, Volume 84(2), pp. 191 – 215
Bang, C. (2009). A world of sound and music: Music therapy for deaf, hearing impaired and multi-handicapped children and adolescents. Approaches: Music Therapy & Special Music Education, Volume 1(2), pp. 93 - 103.
Baniel, A., & Sharp, N. (2013). Leveraging the Power of the Brain to Change Itself to Transform Clinical Outcomes With Adults and Children With Special Needs With the Anat Baniel Method. Global Advances in Health and Medicine. Volume 2 (supplement). S96
Baniel, A.(2016). Keynote Address: Thinking Outside the Box: The Anat Baniel Method (ABM). 2016 Hemispherectomy Conference and Family Reunion. Omni Interlocken Resort. Broomfield, Colorado
Bannerman, D.J., Sheldon, J.B., Sherman, J.A., & Harchik, A.E. (1990). Balancing the right to habilitation with the right to personal liberties: The rights of people with developmental disabilities to eat too many doughnuts and take a nap. Journal of Applied Behavior Analysis, Volume 23, pp. 79 - 89.
Bannerman-Haig, S. (1997). Facilitating Change: Dance/Movement Therapy for Children and Adolescents with Profound and Multiple Learning Difficulties, Dance and the Child. UK Chapter, Journal 4, Focus on Dance Movement Therapy 2
Bannerman-Haig, S. (2006). Stretching, tension and kicking: Aspects of infantile movement in dance movement therapy with children and adolescents in special education, in Payne,H. Dance Movement Therapy. Theory, Research and Practice, 2nd Edition (First edition
published in 1992), pp. 87 - 100
Bar-David, Y., Urkin J., & Kozminsky, E. (2005) The effect of voluntary dehydration on cognitive functions of elementary school children. Acta Paediatrica. Volume 94. pp. 1667 - 1673
Baranek, G.T., & Berkson, G. (1994). Tactile Defensiveness in Children with Developmental Disabilities: responsiveness and habituation. Journal of Autism and Developmental Disorders, Volume 24(4), pp. 457 - 471
Baranek, G.T., Foster, L.G., & Berkson, G. (1997). Sensory Defensiveness in Persons With Developmental Disabilities. The Occupational Therapy Journal of Research, Volume 17(3), pp. 173 - 185
Baranek, G.T. (2002). Efficacy of Sensory and Motor Interventions for Children with Autism. Journal of Autism and Developmental Disorders, Volume (32(5), pp. 397 – 422
Barber, M. (1994). Contingency Awareness: putting research into the classroom. In - J. Coupe O’Kane & B. Smith (eds), Taking Control:enabling people with learning difficulties. London: David Fulton.
Barber, M. (2007). Imitation, interaction and dialogue using Intensive Interaction: tea party rules, Support for Learning, Volume 22 (3): pp.124 – 130.
Barksdale, A.L. (2003). Music therapy and leisure for persons with disabilities. Sagamore Publishing
Barnes, D. (1976). From Communication to Curriculum. Penguin
Baron-Cohen, S., Leslie, A., & Frith, U. (1985). Does the autistic child have a “theory of mind”? Cognition, Volume 21, pp. 37 - 46.
Baron-Cohen, S. (1989). The autistic child's theory of mind: A case of specific developmental delay. Journal of Psychology and Psychiatry, Volume 30, pp. 285 - 297.
Baron-Cohen, S. (2000). The cognitive neuroscience of autism: Evolutionary approaches. In The New Cognitive Neurosciences (2nd ed.), ed. M. Gazzaniga, pp. 1249 - 1257. Cambridge, MA: MIT press
Barrera, F.J., Violo, R.A., & Graver, E.E. (2007). On the form and function of severe self-injurious behavior. Behavioral Interventions, Volume 22(1), pp. 5 - 33
Bartheld, C.S., Bahney, J., & Herculano‐Houzel, S. (2016). The search for true numbers of neurons and glial cells in the human brain: a review of 150 years of cell counting. Journal of Comparative Neurology, Volume 524(18), pp. 3865 - 3895
Bartlo, P., & Klein, P.J. (2011). Physical activity benefits and needs in adults with intellectual disabilities: Systematic review of the literature. American Journal on Intellectual and Developmental Disabilities, Volume 116(3), pp. 220 – 232
Basil, C. (1986). Social interaction and learned helplessness in nonvocal severely handicapped children. Presentation at 4th Biennial Conference on AAC, Cardiff
Basil, C. (1992). Social interaction and learned helplessness in severely disabled children, AAC, Volume 8, pp. 188 - 199
Bass, M.M., Duchowny, C.A., & Liabra, M.M. (2009). The effect of therapeutic horseback riding on social functioning in children with autism. Journal of Autism and Developmental Disorders. Volume 39. pp.1261 – 1267
Battro, A.M., Fischer, K.W., & Lena, P.J. (Eds.)(2008). The Educated Brain: Essays in Neuroeducation. Cambridge University Press
Bauer, B. (1977a). Tactile sensitivity: development of a behavioral responses checklist. American Journal of Occupational Therapy, Volume 31(6), pp. 357 - 361
Bauer, B. (1977b). Tactile-sensitive behavior in hyperactive and non-hyperactive children. American Journal of Occupational Therapy, Volume 31(7), pp. 446 - 453
Baumeister, A.A., & MacLean, W.E. (1984). Deceleration of self-injurious and stereotypic responding by exercise. Applied Research in Mental Retardation, Volume 5, pp. 385 - 393
Baumeister, R.F. (1999). The nature and structure of the self: An overview. In R. Baumeister (Ed.), The self in social psychology (pp. 1–21). Philadelphia, PA: Psychology Press
Baumeister, R.F., & Vohs, K.D. (2007). Self-Regulation, Ego Depletion, and Motivation. Social and Personality. Psychology Compass, Volume 1(1). pp. 115 – 128
Beadle‐Brown, J., Hutchinson, A., & Whelton, B. (2012). Person‐Centred Active Support – Increasing Choice, Promoting Independence and Reducing Challenging Behaviour. Journal of Applied Research in Intellectual Disabilities, 2012, Volume 25(4), pp. 291 - 307
Beadle‐Brown, J., Leigh, J., Whelton, B., Richardson, L., Beecham, J., Baumker, T., & Bradshaw, J. (2016). Quality of life and quality of support for people with severe intellectual disability and complex needs. Journal of Applied Research in Intellectual Disabilities, Volume 29(5), pp. 409 - 421
Beange, H., Gale, L., & Stewart, L. (1995). Project renourish: a dietary intervention to improve nutritional status in people with multiple disabilities. Australia and New Zealand Journal of Developmental Disabilities, Volume 20(3), pp. 165 - 174
Beange, H., McElduff, A., & Baker, W. (1995). Medical disorders of adults with mental retardation: a population study. American Journal on Mental Retardation. Volume 99(6), pp. 595 - 604
Begley, A., & Lewis, A. (1998). Methodological issues in the assessment of the self-concept of children with Down syndrome. Child Psychology and Psychiatry Review, Volume 3, pp. 33 - 40
Begley, S. (2009). The Plastic Mind. Ballantine Books: New York
Belfiore, P.J., Browder, D.M., & Mace, F.C. (1993). Effects of community and center-based settings on the alertness of persons with profound mental retardation. Journal of Applied Behavior Analysis, Volume 26(3), pp. 401 - 402
Belfiore, P.J., Browder, D.M. & Mace, C.J. (1994). Assessing choice-making and preference in adults with profound mental retardation across community and center-based settings. Journal of Behavioral Education. Volume 4(2), pp. 217 – 226
Bellamy, G., Croot, L., Bush, A., Berry, H., & Smith, A. (2010). A study to define: profound and multiple learning disabilities (PMLD). Journal of Intellectual Disabilities, Volume 14, pp. 221 – 235
Belva, B.C., Matson, J.L., Sipes, M., & Bamburg, J.W. (2012). An examination of specific communication deficits in adults with profound intellectual disabilities. Research in Developmental Disabilities, Volume 33(2), pp. 525 - 529
Ben-Artzi, E., Mikulincer, M., & Glaubman, H. (1995) The multifaceted nature of self-consciousness: Conceptualization, measurement, and consequences, Imagination, Cognition and Personality, Volume 15(1), pp. 17 – 43
Benda, W., McGibbon, N.H., & Grant, K.L. (2003) Improvements in Muscle Symmetry in Children with Cerebral Palsy After Equine-Assisted Therapy (Hippotherapy). The Journal of Alternative and Complementary Medicine. Volume 9(6), pp. 817- 825.
Benson, G., Abbeduto, L., Short, K., Bibler-Nuccio, J., & Maas, F. (1993). Development of a theory of mind in individuals with mental retardation. American Journal on Mental Retardation, Volume 98, pp. 427 - 433
Benson, J.D., Beeman, E., Smitsky, D., & Provident , I. (2011). The Deep Pressure and Proprioceptive Technique (DPPT) Versus Nonspecific Child-Guided Brushing: A Case Study. Journal Of Occupational Therapy, Schools, & Early Intervention. Volume 4(3-4), pp. 204 - 214.
Benton, D., & Burgess, N. (2009) The effect of the consumption of water on the memory and attention of children. Appetite. Volume 53. pp. 143 - 146
Bergouignan, L., Nyberg, L., & Ehrsson, H.H. (2014). Out-of-body induced hippocampal amnesia. Proceedings of the National Academy of Sciences, Volume 111(12), pp. 4421 – 4426
Bergström, H., Hagströmer, M., Hagberg, J., & Elinder, L.S. (2013). A multi-component universal intervention to improve diet and physical activity among adults with intellectual disabilities in community residences: a cluster randomised controlled trial. Research in Developmental Disabilities, Volume 34(11), pp. 3847 - 3857
Berrol, C.F. (1981). A neurophysiologic approach to dance/movement therapy: Theory and practice. American Journal of Dance Therapy, Volume 4(1), pp. 72 - 84
Bersani, H.A., & Heifetz, I.J. (1985). Perceived stress and satisfaction of direct care staff members in community residences for mentally retarded adults. American Journal of Mental Deficiency, Volume 90, pp. 289 - 295
Bertolami, M.D., & Martino, L.A. (2002). Music therapy in a private school for visually impaired and multiply handicapped children. Voices: A World Forum for Music Therapy, Volume 2(1), Retrieved from https://normt.uib.no/index.php/voices/article/viewArticle/69/59.
Beveridge, M., & Berry, P. (1977). Observing interactions in severely mentally handicapped children. Research in Education. Volume 17, pp. 13 - 22
Beveridge, M., & Hurrell, P. (1979). Teachers' responses to severely mentally handicapped children. Journal of Child Psychiatry. Volume 21, pp. 175 - 181
Beveridge, M. (Ed.) (1982). Children thinking through language. London: Edward Arnold
Beveridge, M., & Conti- Ramsden, G. (1987). Children with language disabilities. Open University Press: ISBN 0-335-10279-4
Beveridge, M., Conti- Ramsden, G., & Leudar, I. (Eds.)(1988). Languages and communication in mentally handicapped people. London: Chapman and Hall
Bexkens, A., Ruzzano, L., Collot d'Escury‐Koenigs, A.M.L., Van der Molen, M.W., & Huizenga, H.M. (2014). Inhibition deficits in individuals with intellectual disability: a meta‐regression analysis. Journal of Intellectual Disability Research, Volume 58(1), pp. 3 - 16
Bhaumik, S., Watson, J.M., Thorp, C.F., Tyrer, F., & McGrother, C.W. (2008). Body mass index in adults with intellectual disability: distribution, associations and service implications: a population‐based prevalence study. Journal of Intellectual Disability Research, Volume 52(4), pp. 287 - 298
Bidabe, L., & Lollar, J.M. (1995). MOVE (Mobility Opportunities Via Education). 3rd edition. Kern Country Superintendent of Schools, Bakersfield.
Biddiss, E., Blain-Moraes, S., Chesser, S., Kingsnorth, S., & McKeever, P. (2013). Biomusic: A novel technology for revealing personhood of people with profound multiple disabilities. Augmentative and Alternative Communication, Volume 29(2), pp. 159 - 173
Bigby, C., Clement, T., Mansell, J., & Beadle-Brown, J. (2009). ‘It’s pretty hard with our ones, they can’t talk, the more able bodied can participate’: Staff attitudes about the applicability of disability policies to people with severe and profound intellectual disabilities. Journal of Intellectual Disability Research. Volume 53, pp. 363 – 376
Birch, T., Cross, A., Dumble, M., & Park, K. (2000): Switching on to Stories: AAC Use and Storytelling with Children with Severe and Profound Learning Disabilities. Communication Matters. Volume 14 (2), pp. 2 - 4
Birdi, K.S. (2005). No idea? Evaluating the effectiveness of creativity training. Journal of European Industrial Training, Volume 29(2), pp. 102 - 111
Biringer, F., & Anderson., J.R. (1993). Self-recognition in Alzheimer’s disease: Use of mirror and video techniques and enrichment. In Recent Advances in Aging Science (Volume 1), ed. I. Beregi, & K. Rajczi, pp. 697 - 705. Bologna: Monduzzi Editore.
Bizub, A.L., Ann, J., & Davidson, L. (2003). It’s like being in another world: Demonstrating the benefits of therapeutic horseback riding for individuals with psychiatric disability. Psychiatric Rehabilitation Journal, Volume 26(4), pp. 377 – 384
Blacher J., & McIntyre L.L. (2006). Syndrome specificity and behavioural disorders in young adults with intellectual disability: cultural differences in family impact. Journal of Intellectual Disability Research. Volume 50, pp. 184 – 98
Blades, M. (2000). Autism: an interesting dietary case history. Nutrition & Food Science, Volume 30(3), pp. 137 - 140
Blaich, C., Wise, K., Pascarella, E.T., & Roksa, J. (2016). Instructional Clarity and Organization: It's Not New or Fancy, But It Matters. Change: The Magazine of Higher Learning, Volume 48(4), pp. 6 - 13
Blakemore, S., & Frith, U. (2005). The Learning Brain: lessons for education. Blackwell Publishing
Blanchard, K., & Johnson, S. (1983). The One Minute Manager. Fontana
Blanchard, K., & Lorber, R. (1984). Putting the One Minute Manager to Work. Fontana
Blanchard, K., Zigarmi, P., & Zigarmi, D. (1987). Leadership and the One Minute Manager. Fontana
Blanchard, K. (1999). Catch People Doing Something Right. Executive Excellence Publications
Blank, M., & Marquis, M.S. (1987). Directing Discourse, (Communication Skill Builders) Winslow Press
Block, N. (1995). On a confusion about a function of consciousness. Behavioral and Brain Sciences, Volume 18, pp. 227 – 247
Bloomberg, K., West, D., & Iacono, T.A. (2003). Picture it: An evaluation of a training program for carers of adults with severe and multiple disabilities. Journal of Intellectual & Developmental Disability, Volume 28, pp. 260 – 282
BMJ (2015). Get up and stand up for at least 2 hours daily during working hours. British Journal of Sports Medicine. Press Release
Boat, B. (2006). Clinical approaches to assessing and utilising animal-related experiences in therapeutic interventions with children, adolescents and their caregivers. In - Fine A.H. (ed.), Handbook on Animal Assisted Therapy: Theoretical Foundations and Guidelines for Practice. (3rd ed.). Elsevier, London
Bobzien, J.L. (2011). A review of curricular approaches and quality of life indicators in the United States for individuals displaying profound multiple disabilities. Social Welfare: Interdisciplinary Approach, Volume 1(2), pp. 8 – 22
Bobzien, J.L. (2014). Academic or Functional Life Skills? Using Behaviors Associated with Happiness to Guide Instruction for Students with Profound/Multiple Disabilities. Education Research International. Volume 2014, Article ID 710816, 12 pages
Bodde A.E., & Dong-Chul S. (2009). A review of social and environmental barriers to physical activity for adults with intellectual disabilities. Disability and Health Journal, Volume 2, pp. 57 - 66
Boe, R.B. (1977). Economical procedures for the reduction of aggression in a residential setting. Mental Retardation, Volume 15, pp. 25 - 28
Bolte Taylor, J. (2008). My Stroke of Insight. Hodder and Stoughton
Booker, M. (2011). Developmental Drama: Dramatherapy Approaches for People with Profound or Severe Multiple Disabilities, Including Sensory Impairment. Jessica Kingsley Publishers
Booth, P., Taylor, B., & Edmonds, C.J. (2012) Water supplementation improves visual attention and fine motor skills in schoolchildren. Education and Health. Volume 30. pp. 75 - 79
Borthwick-Duffy, S.A., Eyman, R.K., & White, J.F. (1987). Client characteristics and residential placement patterns. American Journal of Mental Deficiency, Volume 92, pp. 24 - 30
Borthwick-Duffy, S.A. (1990). Quality of life of persons with severe or profound mental retardation. In R. L. Schalock (Ed.), Quality of life: Perspectives and issues (pp. 177 - 189). American Association on Mental Retardation.
Borthwick-Duffy, S.A. (1994).Prevalence of Destructive Behaviours. In T.Thompson & D.B. Gray (Eds.) Destructive Behaviour in Developmental Disabilities: Diagnoses and Treatment. pp. 3 - 23. Thousand Oaks: Sage.
Bosch, J.J., & Ringdahl, J. (2001). Functional Analysis of problem behaviour in children with mental retardation: what is it and why should pediatric nurses care?. The American Journal of Maternal/Child Nursing, Volume 26(6), pp. 307 - 311
Bott, C., Farmer, R., & Rhode, J. (1997). Behaviour problems associated with lack of speech in people with learning disabilities. Journal of Intellectual Disability Research. Volume 41, pp. 3 - 7
Bouhadiba, Z., Dacher, J., Monroe, M., Vanhulle, C., Menard, J., & Kalifa, G. (2000). MRI of the brain in the evaluation of children with developmental delay. European Journal of Radiology, Volume 81. pp. 870 – 873
Bower, T.G.R., & Wishart, J.G. (1972). The effects of motor skill on object permanence. Cognition, Volume 1(2-3), pp. 165 - 172
Bower, T.G.R., & Paterson, J.G. (1972). Stages in the development of the object concept. Cognition, Volume 1(1), pp. 47 - 55
Boxall, K., & Ralph, S. (2009) Research ethics and the use of visual images in research with people with intellectual disabilities. Journal of Intellectual and Developmental Disability, Volume 34(1), pp. 45 - 5.
Boxall, K. (2010). Involving people with profound and multiple learning difficulties in research: barriers and possibilities. Disability Studies Conference Proceedings, University of Lancaster, September
Boxhill, E.H. (1981). A continuum of awareness: Music therapy with the developmentally handicapped. Music Therapy, Volume 1(1), pp. 43 - 49
Boxhill, E.H. (1985). Music therapy for the developmentally disabled. Austin, TX: PRO-ED.
Bradley, A. & Ouvry, C. (1999). Unit Six: Planning for everyday good practice. In J. Harris (ed.), Better Choices: Fuller Lives. Working with people with profound learning disability and complex support needs. First Draft Publications. BILD
Bradley, H. (1998). Assessing and Developing Successful communication, in Lacey, P., & Ouvry, C. (1998). People with Profound and Multiple Learning Disabilities – A collaborative approach to meeting complex needs. London: David Fulton Publishers
Bradley, J. (2012). The effect of choice for people with learning disabilities: A systematic review, Journal of Applied Research in
Intellectual Disabilities
Bradshaw, J. (2001). Communication Partnerships with People with Profound and Multiple Learning Disabilities. Tizard Learning
Disability Review, Volume 6(2), pp. 6 – 15
Bradshaw, J. (2001b). Complexity of staff communication and reported level of understanding skills in adults with intellectual disability. Journal of Intellectual Disability Research, Volume 45, pp. 233 – 243
Braitenberg, V. (2001). Brain size and number of neurons: an exercise in synthetic neuroanatomy. Journal of Computational Neuroscience, Volume 10(1), pp. 71 - 77
Bray, N., & Turner, L. (1986):The rehearsal deficit hypothesis. in - International Review of Research in Mental Retardation, Volume 14, pp. 47 - 71, Ellis, N. & Bray N. (Eds.). New York: Academic Press
Bray, N., & Turner, L. (1987): Production anomalies (not strategic deficiencies) in mentally retarded individuals. Intelligence, Volume 11, pp. 49 - 60
Bray, N. (1990): A cognitive model for Minspeak, 5th Annual Minspeak conference proceedings. November 14th -15th, Seattle, Washington
Wooster, OH: PRC
Breau, L.M., Camfield, C.S., McGrath, P.J., & Finley, G.A. (2003). The incidence of pain in children with severe cognitive impairments. Archives of Pediatrics & Adolescent Medicine, Volume 157(12), pp. 1219 - 1226
Breau, L.M., Camfield, C.S., Symons, F.J., Bodfish, J. W., McKay, A., & Finley, G.A. (2003). Pain and self-injurious behaviour in neurologically impaired children. Journal of Pediatrics, Volume 142(5), pp. 498 - 503
Breau L.M., Camfield C.S., Symons F.J., Bodfish J.W., MacKay A., Finley G.A., & McGrath, P.J. (2003). Relation between pain and self-injurious behavior in nonverbal children with severe cognitive impairments. Journal of Pediatrics. Volume 142(5), pp. 498 – 503.
Breau, L.M., & Burkitt, C. (2009). Assessing pain in children with intellectual disabilities. Pain Research & Management: The Journal of the Canadian Pain Society, Volume 14(2), pp. 116 -120
Brett-Green, B.A., Miller, L.J., Schoen, S.M., & Nielson, D.M. (2010). An exploratory event-related potential study of multisensory integration in sensory over-responsive children. Brain Research, Volume 1321, pp. 67 – 77
Bright, T., Bittick, K., & Fleeman, B. (1981). Reduction of self injurious behavior using sensory integrative techniques. American Journal of Occupational Therapy, Volume 35, pp. 167 – 172
Briscoe, G. (2002). Language, inner speech, and consciousness. Paper presented at the Association for the Scientific Study of Consciousness. Barcelona, Spain
Brodin, J. (2005). Diversity of aspects on play in children with profound multiple disabilities. Early Child Development and Care, Volume 175, pp. 635 - 646
Brody, J.F., Thomas, J.A., Brody, D.M., & Kucherawy, D.A. (1977). Comparison of sensory integration and operant methods for production of vocalization in profoundly retarded adults. Perceptual and motor skills, Volume 44(3 supplement), pp. 1283 - 1296
Broesch, T., Callaghan, T., Henrich, J., Murphy, C., & Rochat, P. (2011). Cultural variations in children’s mirror self-recognition. Journal of Cross-Cultural Psychology, Volume 40(6), pp. 1019 - 1031
Brotherson, S.E. (2005). Understanding brain development in young children. Fargo, ND: NDSU Extension Service
Browder, D.M., Cooper, K.J., & Lim, L. (1998). Teaching adults with severe disabilities to express their choice of settings for leisure activities. Education and Training in Mental Retardation and Developmental Disabilities, Volume 33, pp. 228 - 238
Browder, D.M, Wakeman, S.Y., Spooner, F., Ahlgrim-Delzell, L., & Algozzine, B. (2006). Research on reading instruction for individuals with significant cognitive disabilities, Exceptional Children, Volume 72(4), pp. 392 – 408
Browder, D.M, Wakeman, S.Y., Flowers, C., Rickelman, R.J., Pugalee, D., & Karvonen, M. (2007). Creating access to the general curriculum with links to grade-level content for students with significant cognitive disabilities: an explication of the concept, Journal of Special Education, Volume 41(1), pp. 2 – 16
Browder, D.M., Gibbs, S., Ahlgrim-Delzell, L., Courtade, G.R.,. Mraz, M., & Flowers, C. (2009). Literacy for students with severe developmental disabilities: what should we teach and what should we hope to achieve? Remedial and Special Education, Volume 30(5), pp. 269 – 282
Browder, D.M., & Spooner, F. (2011). Teaching Students with Moderate and Severe Disabilities. Guilford Publications
Browder, D. M., Wood, L., Thompson, J., & Ribuffo, C. (2014). Evidence-based practices for students with severe disabilities (Document No. IC-3). Retrieved from University of Florida, Collaboration for Effective Educator, Development, Accountability, and Reform Center website: http://ceedar.education.ufl.edu/wp-content/uploads/2014/09/IC-3_FINAL_03-03-15.pdf
Brown, F. (1991). Creative daily scheduling: A nonintrusive approach to challenging behaviors in community residences. Journal of the Association for Persons with Severe Handicaps, Volume 16, pp. 75 - 84
Brown, F. Appel, C., Corsi, L. & Wenig, B. (1993). Choice diversity for people with severe disabilities. Education & Training in Mental Retardation, Volume 28, pp. 318 - 326.
Brown, F., Gothelf, C.R., Guess, D., & Lehr, D.H. (1998). Self-determination for individuals with the most severe disabilities: Moving beyond chimera. Journal of the Association for Person with Severe Handicaps, Volume 23, pp. 17 – 26
Brown, I., & Brown, R.I. (2003). Quality of Life and Disability.. Jessica Kingsley
Brown, I., & Brown, R.I. (2009). Choice as an aspect of quality of life for people with intellectual disabilities. Journal of Policy and Practice in Intellectual Disabilities, volume 6 (1), pp.11 - 18
Brown, J.D. (2009). The Self. Routledge
Brown, L., Falvey, M., Vincent, L., Kage, N., Johnson, F., Fettara-Pattish, P., & Gruenewald, L. (1980). Strategies for generating comprehensive, longitudinal and chronological age appropriate individual educational plans for adolescent and young severely handicapped students. In L. Brown, M. Falvey, D. Baumgart, I. Pumpian, J. Schroeder, & L. Gruenewald (Eds.), Strategies for teaching chronological age appropriate functional skills to adolescent and young adult severely handicapped students (pp. 10 - 34). Madison, WI: University of Wisconsin-Madison and Madison Metropolitan School District.
Brown, L.S., & Jellison, J.A. (2012). Music research with children and youth with disabilities and typically developing peers: A systematic review. Journal of Music Therapy, Volume 49(3), pp. 335 - 364
Brown, N., McLinden, M., & Porter, J. (1998). Sensory needs in P. Lacey & C. Ouvry (eds), People with Profound and Multiple Learning Disabilities: A collaborative approach to meeting complex needs. London: David Fulton, pp. 29 - 38
Brown, R.I., Bayer, M.B., & Brown, P.M. (1992). Empowerment and Developmental Handicaps: Choices and Quality of Life. Toronto: Captus Press
Brown, S. (1994). Autism and music therapy - is change possible and why music? Journal of British Music Therapy, Volume 8(1), pp. 15 - 25
Browning, M. (1983). Identifying the Needs of Profoundly Mentally Handicapped Children. Jordanhill Project. Glasgow
Brownson, T. (2012). Seventy amazing facts about your brain. Biak.us
Brouns, B., Tap, R., Waninge, A., & Van der Woude, L.H.V. (2015). Applicability of a measurement method to determine the degree of daily movement of children with intellectual disabilities. Dutch magazine for care for people with intellectual disabilities. Volume 2. pp.121 - 131
Bruce, D.J. (1958). The Effect of Listeners' Anticipations on the Intelligibility of Heard Speech. Language and Speech, Volume 1(2), pp. 79 - 97
Bruce, S.M., Trief, E., & Cascella, P.W. (2011). Teachers’ and Speech-Language Pathologists’ Perceptions about a Tangible Symbols
Intervention: Efficacy, Generalization, and Recommendations. Augmentative and Alternative Communication, Volume 27 (3) , Pages 172 - 182
Bruininks, R.H., Olsen, K.M., Larson, S.A., & Lakin, K.C. (1994). Challenging behavior among persons with mental retardation in residential settings. In T. Thompson & D.B. Gray (Eds.), Destructive Behavior in Developmenal Disabilties: Diagnosis and Treatment. pp. 24 - 48. Thousand Oaks: Sage
Brylewski J., & Wiggs, L. (1999). Sleep problems and daytime challenging behaviour in a community-based sample of adults with intellectual disability. Journal of Intellectual Disability Research. Volume 43, pp. 504 – 512
Bubic, A., Striem-Amit, E., & Amedi, A. (2010). Large-Scale Brain Plasticity Following Blindness and the Use of Sensory Substitution Devices, in M.J. Naumer, & J. Kaiser (eds.), Multisensory Object Perception in the Primate Brain, chapter 18, pp. 351 - 380, Springer Science+Business Media
Buie, T. (2013). The relationship of autism and gluten. Clinical Therapeutics, Volume 35(5), pp. 578 - 583
Bull, S., & O’Farrell, K. (Eds.). (2012). Art therapy and learning disability: ‘Don’t guess my happiness’. Hove, Routledge.
Bullivant, M. (2015). Self-injurious Behaviour in Cornelia de Lange Syndrome. PMLD Link. Volume 27(2), Issue 81, pp. 23 - 25
Bullivant, M., & Jones, A.P. (2016). Sensory Stories Webpage. TalkSense Website
Bundy, A.C., Lane, S.J., & Murray, E.A. (2002). Sensory Integration: Theory and Practice. Second Edition. Philadelphia: F.A. Davis
Bunnell, T. (2007). Music Makes a Difference: A Practical Guide to Developing Music Sessions with People with Learning Disabilities. Keswick: M&K Update.
Bunning, K. (1998). To engage or not to engage? Affecting the interactions of learning disabled adults. International Journal of Language and Communication Disorders, Volume 33(Supplement), pp. 386 - 391
Burton, M., Kagan, C. & Clements. P. (1995). Social Skills for People with Learning Disabilities. Therapy in Practice Volume 48. Chapman and Hall
Bustad, L.K., & Hines, L. (1984). Historical perspectives of the human-animal bond. In - Anderson. R.K., Hart, B.L., & Hart, L.A. (eds.). The Pet Connection: Its Influence on Our Health and Quality of Life. Minneapolis: Centre to Study Human-Animal Relationships and Environments. University of Minnesota, Minnesota. pp.15 - 29
Butté, C. (2007). An Inquiry into the Use of Interpersonal Touch in Dance Movement Therapy with Adults with Profound and Multiple Learning Difficulties/Disabilities. Unpublished Master's Thesis. Dissertation DMT045L407Y. Roehampton University, London
Butté, C., & Unkovich, G. (2009). Foundations of Dance Movement Psychotherapy Practice in Profound and Multiple Learning Difficulties. E-Motion, Volume 19(4), pp. 25 -33
Buultjens, M., & Aitken, S. (1987). Assessment of vision in multiply impaired children. British Journal of Special Education, Volume 14(3), pp. 112 - 114
Byers, R. (1996). Classroom Processes in B. Carpenter, R. Ashdown, & K. Bovair (eds), Enabling Access - effective teaching and learning for learners with learning difficulties. London: David Fulton.
Byers, R. (1998) Managing the learning environment. In: P. Lacey and C. Ouvry (eds.), People with Profound and Multiple Learning Disabilities: a collaborative approach to meeting complex needs. London: David Fulton Publishers.
Byers, R. (1999). Experience and achievement: initiatives in curriculum development for learners with severe and profound and multiple learning difficulties. British Journal of Special Education, Volume 26(4), pp. 184 - 188
Caldwell, P. (1991) Stimulating People with Profound Handicaps. How can we work together? British Journal of Mental Subnormality. Volume 37,(2), pp. 92 - 100
Caldwell, P. (1997). 'Getting in touch' with people with severe learning disabilities. British Journal of Nursing, Volume 6(13), pp. 751 - 756
Caldwell, P. (1998). Person to Person: Establishing Contact and Communication with People with Profound Disabilities. Pavilion Publishing (Brighton) Ltd
Caldwell, P. (2006a). Finding You Finding Me: Using Intensive Interaction to get in touch with people whose severe learning disabilities are combined with autistic spectrum disorder. London: Jessica Kingsley Publishers
Caldwell, P. (2006b). Speaking the other's language: Imitation as a gateway to relationship. Infant and Child Development, Volume 15, pp. 275 - 282
Cambridge, P., & Carnaby, S. (2000). A personal touch: managing the risks of abuse during intimate and personal care. The Journal of Adult Protection, Volume 2(4), pp. 4 - 16
Cameron, L. & Bell, D. (2001). Enhanced Interaction Training: A method of multi-disciplinary staff training in Intensive Interaction to reduce challenging behaviour in adults who have learning disabilities and who also have a severe communication disorder, Working with People who have a Learning Disability, Volume 18, (3), pp. 8 - 15
Cameron, L., & Murphy, J. (2002). Enabling young people with learning disability to make choices at a time of transition. British Journal of Learning Disabilities, Volume 30, pp. 105 – 112
Cammaerts, M.C., & Cammaerts, R. (2015). Are Ants (Hymenoptera, Formicidae) Capable of Self Recognition? Journal of Science. Volume 5(7), pp. 521 - 532
Campo, S.F., Sharpton, W.R., Thompson, B., & Sexton, D. (1997). Correlates of the quality of life of adults with severe or profound mental retardation. Mental Retardation, Volume 35(5), pp. 329 - 337
Cannella, H.I., O’Reilly, M.F., & Lancioni, G.F. (2005). Choice and preference assessment research with people with severe to profound developmental disabilities: a review of the literature. Research in Developmental Disabilities, Volume 26, pp.1 – 15
Carmeli, E., Orbach, I., Zinger-Vaknin, T., Morad, M., & Merrick, J. (2008) Physical training and well-being in older adults with mild intellectual disability: A residential care study, Journal of Applied Research in Intellectual Disabilities, Volume 21, pp. 457 – 465
Carnaby, S., & Cambridge, P. (2002). Getting personal: an exploratory study of intimate and personal care provision for people with profound and multiple intellectual disabilities. Journal of Intellectual Disability Research, Volume 46(2), 120 - 132
Carnaby, S., & Cambridge, P. (2006). Intimate and personal care with people with learning disabilities. Jessica Kingsley Publishers
Carnaby, S., & Pawlyn, J. (2009). Profound intellectual and multiple disabilities: meeting complex needs through complex means, in - J. Pawlyn & S. Carnaby (eds), Profound Intellectual and Multiple Disabilities: Nursing Complex Needs. Oxford: Wiley Blackwell
Carpenter, B., Egerton, J., Cockbill, B., Bloom, T., Fotheringham, J., Rawson, H., & Thistlewaite, J. (2015). Engaging Learners with Complex Learning Difficulties and Disabilities. Oxon: Routledge
Carpenter, B., Egerton, J., Cockbill, B., Bloom, T., Fotheringham, J., Rawson, H., & Thistlewaite, J. (2015). Mental health and children with Complex Learning Difficulties and Disabilities, in - Carpenter B. et al (Ed.), Engaging Learners with Complex Learning Difficulties and Disabilities. Oxon: Routledge
Carr, E.G., Newsom, C.D., & Binkoff, J.A. (1976). Stimulus control of self-destructive behavior in a psychotic child. Journal of Abnormal Child Psychology, Volume 4, pp. 139 - 153
Carr, E.G. (1977). The motivation of self-injurious behaviour: A review of some hypotheses. Psychological Bulletin, Volume 84 (4), pp. 800 –816
Carr, E.G., & McDowell, J.J. (1980). Social control of self-injurious behavior of organic etiology. Behavior Therapy, Volume 11, pp. 402 - 409
Carr, E.G., Newsom, C.D., & Binkoff, J.A. (1980). Escape as a factor in the aggressive behavior of two retarded children. Journal of Applied Behavior Analysis, Volume 13, 101 - 117
Carr, E.G., & Durand, V.M. (1985a). Reducing behavior problems through functional communication training. Journal of Applied Behavior Analysis, Volume 18(2), pp. 111 - 126
Carr, E.G., & Durand, V.M. (1985b). The social communicative basis of severe behaviour problems in children, in S. Reiss and R. Bootzin (Eds.), Theoretical Issues in Behaviour Therapy. Academic Press, New York, pp. 219 - 54
Carr, E.G., & Newsom, C.D. (1985). Demand-related tantrums: Conceptualisation and treatment. Behavior Modification, Volume 9, pp. 403 - 426
Carr, E.G., Robinson, S., & Palumbo, L.W. (1990). The wrong issue: Aversive versus nonaversive treatment. The right issue: Functional versus nonfunctional treatment. In A. Repp & N. Singh (Eds.), Perspectives on the use of nonaversive and aversive interventions for persons
with developmental disabilities, pp. 361-379. Sycamore, IL: Sycamore.
Carr, E.G., Robinson, S., Taylor, J.C., & Carlson, J.I. (1990). Positive approaches to the treatment of severe behavior problems in persons with developmental disabilities: A review and analysis of reinforcement and stimulus-based procedures. Monograph of the Association
for Persons with Severe Handicaps, Volume 4.
Carr, E.G., Taylor, J.C., & Robinson, S. (1991). The effects of severe behavior problems in children on the teaching behavior of adults. Journal of Applied Behavior Analysis, Volume 24, pp. 523 - 535
Carr, E.G., & Carlson, J.I. (1993). Reduction of severe behavior problems in the community using a multicomponent treatment approach. Journal of Applied Behavior Analysis, Volume 26, pp. 157 - 172
Carr, E.G. (1994). Emerging themes in the functional analysis of problem behavior. Journal of Applied Behavior Analysis. Volume 27(2), pp. 393 - 399
Carr, E.G., Levin, L., McConnachie, G., Carlson, J.I., Smith, C.E., & Kemp, D.C. (1994). Communication-based intervention for problem behavior. Baltimore: Paul H. Brookes.
Carr, E.G., Levin, L, McConnachie, G., Carlson, J.I., Kemp, D.C., & Smith, C.E. (1997). Communication-baased Intervention for Problem Behavior: A User's Guide for Producing Positive Change. Paul H. Brookes
Carr, E.G., Yarbrough, S.C., & Langdon, N.A. (1997). Effects of idiosyncratic stimulus variables on functional analysis outcomes. Journal of Applied Behavior Analysis. Volume 30(4), pp. 673 - 686
Carsrud, A.L., Carsrud, K.B., & Standifer, J.T. (1980). Social variables affecting mental health in the geriatric mentally retarded: An exploratory study. Mental Retardation, Volume 18, pp. 88 - 90
Carsrud, A.L. (1986). Effects of structured social interaction with geriatric mentally retarded clients: An exploratory study. Journal of Psychology and Aging, Volume 1(1), pp. 78 - 79
Carter, E.W., Lane, K.L., Pierson, M.R., & Glaeser, B. (2006). Self-determination skills and opportunities of transition-age youth with emotional disturbance and learning disabilities. Exceptional Children, Volume 72, pp. 333 – 346
Carter, S. (1982). Music Therapy for Handicapped Children: Mentally Retarded. Washington D.C.: National Association for Music Therapy.
Cartwright, C., & Wind-Cowie, S. (2005). Profound and Multiple Learning Difficulties. Continuum International Publishing
Case-Smith, J. (1991). The effects of tactile defensiveness and tactile discrimination on in-hand manipulation skills. American Journal of Occupational Therapy, Volume 45, pp. 811 – 825
Cataldo, M.F., & Harris, J. (1982). The biological basis for self-injury in the mentally retarded. Analysis and Intervention in Developmental Disabilities, Volume 2, pp. 21 - 39
Cavet, J.(1989). Occupational and Leisure Activities for People with Profound Retardation and Multiple Impairments: A study of Creative Activities to Facilitate Social Integration. Hester Adrian Research Centre. University of Manchester.
Cavet, J. (1995). Leisure provision in Europe. In - J. Hogg & J. Cavet (Eds), Making leisure provision for people with profound learning and multiple disabilities. London: Chapman & Hall, pp. 49 - 64
CDC (Centers for Disease Control and Prevention)(2003). Prevalence of physical activity, including lifestyle activities among adults – USA. Morbidity and Mortality Weekly Report, Volume 52(32). pp. 764 - 769
Cecchi, G.A., Petreanu, L.T., Alvarez-Buylla, A., & Magnasco, M.O. (2001). Unsupervised learning and adaptation in a model of adult neurogenesis. Journal of Computational Neuroscience, Volume 11(2), pp. 175 - 182
Çetrez İscan, G., Nurcin, E., & Fazlioglu, Y. (2016). Effect of most-to-least prompting procedure on dressing skill of students with Autism. Educational Research and Reviews, Volume 11(18), pp. 1766 - 1774
Chadwick, D.D., & Joliffe, J. (2009). A pilot investigation into the efficacy of a signing training strategy for staff working with adults with intellectual disabilities. British Journal of Learning Disabilities, Volume 37, pp. 34 - 42
Chadwick, O., Piroth, N., Walker, J., Bernard, S., & Taylor, E. (2000). Factors affecting the risk of behaviour problems in children with severe intellectual disability. Journal of Intellectual Disability Research, Volume 44, pp. 108 – 123
Chadwick, O., Kusel, Y., & Cuddy, M. (2008). Factors associated with the risk of behaviour problems in adolescents with severe intellectual disabilities. Journal of Intellectual Disability Research, Volume 52(10), pp. 864 – 876
Chambers, C.R., Wehmeyer, M.L., Saito, Y., Lida, K.M., Lee, Y., & Singh, V. (2007). Self-determination: What do we know? Where do we go? Exceptionality, Volume 15, pp. 3 – 15
Chan, J.S., & Yau, M.K. (2002). A study on the nature of interactions between direct care staff and persons with developmental disabilities in institutional care. The British Journal of Developmental Disabilities, Volume 48(94), pp. 39 - 51
Chan, J.S., & Chien, W.T. (2017). A randomised controlled trial on evaluation of the clinical efficacy of massage therapy in a multisensory environment for residents with severe and profound intellectual disabilities: a pilot study. Journal of Intellectual Disability Research, Volume 61(6), pp. 532 - 548
Chandler, C. (2005). Animal Assisted Therapy in Counselling. Routledge, Taylor and Francis Group, New York
Chao, W.L. (2007). Face Recognition. GICE, National Taiwan University
Chapman, J.W. (1988). Learning disabled children’s self-concepts. Review of Educational Research, Volume 58(3), pp. 347 - 371
Chase, K.M. (2004). Music therapy assessment for children with developmental disabilities: A survey study. Journal of Music Therapy, Volume 41(1), pp. 28 - 54
Chesebro, J.L. (2003). Effects of teaching clarity and nonverbal immediacy on student learning, receiver apprehension, and affect. Communication Education, Volume 52(2), pp. 135 - 147
Chesner, A. (1995). Dramatherapy for people with Learning Disabilities. Jessica Kingsley: London
Chiang, J.Y.K. (2008). Music therapy for young children who have special needs: The music Therapy experience from the perspectives of carers and professionals. Master's Degree Dissertation: New Zealand School of Music, Wellington
Cian, C., Koulmann, N., Barraud, P.A., Raphel, C., Jimenez, C., & Melin, B. (2000). Influences of variations in body hydration on cognitive function: Effect of hyper-hydration, heat stress, and exercise-induced dehydration. Journal of Psychophysiology. Volume 14. pp. 29 - 36
Cipani, E. (1981). Modifying food spillage behavior in an institutionalized retarded client. Journal of behavior therapy and experimental psychiatry, Volume 12(3), pp. 261 - 265
Clark, F.A., Miller, L.R., Thomas, J.A., Kucherway, O,A,, & Azin S.P. (1978). A comparison of operant and sensory integration methods on vocalizations and other developmental parameters in profoundly retarded adults. American Journal of Occupational Therapy, Volume 32, pp. 86 - 93
Clark, F.A., & Shuer, J. (1978). A clarification of sensory integrative therapy and its application to programming with retarded people. Mental Retardation, Volume 16, pp. 227 - 232
Clark, P. (1988). Adapting signs for deaf-blind children. Talking Sense, Volume 34(1), pp. 16 - 17
Clark, S. (1991). Children with Profound / Complex Physical and Learning Difficulties. NCSE (Reprint 1993 by NASEN)
Clayton, J., Burdge, M., Denham, A., Kleinert, H.L., & Kearns, J. (2006). A four-step process for accessing the general curriculum for students with significant cognitive disabilities, Teaching Exceptional Children, Volume 38(5), pp. 20 – 27
Clayton, K., Fleming, J.M., & Copley, J. (2003). Behavioral Responses to Tactile Stimuli in Children with Cerebral Palsy. Physical & Occupational Therapy In Pediatrics, Volume 23(1), pp. 43 - 62
Clement, T., & Bigby, C. (2009). Breaking out of a distinct social space: Reflections on supporting community participation for people with severe and profound intellectual disability. Journal of Applied Research in Intellectual Disability, Volume 22(3), pp. 264 - 275
Close, W., Carpenter, M., & Cibiri, S. (1986). An evaluation study of sensory motor therapy for profoundly retarded adults. Canadian Journal of Occupational Therapy, Volume 53(5), pp. 259 - 264
Cobb, B., Lehmann, J., Newman-Gonchar, R., & Alwell, M. (2009). Self-determination for students with disabilities: A narrative meta-synthesis. Career Development for Exceptional Individuals, Volume 32, pp. 108 – 114
Cobigo, V., Morin, D., & Lachapelle, Y. (2007). Assessing Work Task Preferences among Persons with Intellectual Disabilities: An Integrative Review of Literature. Education and Training in Developmental Disabilities, Volume 42(3), pp. 286 – 300
Codling, M., & MacDonald, N. (2009). Epilepsy: Implications for people with profound intellectual and multiple disabilities. In J. Pawlyn, & S. Carnaby (Eds.), Profound Intellectual and Multiple Disabilities Nursing Complex Needs. pp. 134 – 146. Oxford: Wiley-Blackwell,
Coffey, E. (2014). The Effect of Equine Assisted Therapy on the Social Functioning of Children with Autism. Dissertation psychology degree at Dublin Business School, School of Arts, Dublin.
Cole, C.L., & Levinson, T.R. (2002). Effects of within-activity choices on the challenging behavior of children with severe developmental disabilities. Journal of Positive Behavior Interventions, Volume 4(1), pp. 29 - 37
Coleman, M. (2002). Creating your own multisensory environment. Eye Contact, Volume 32, pp. 31 - 32
Collacott R.A., Cooper S.A., Branford D., & McGrother C. (1998). Epidemiology of self-injurious behaviour in adults with learning disabilities. British Journal of Psychiatry. Volume 173, pp. 428 – 432
Colley, A. (2013). Personalised Learning for Young People With Profound and Multiple Learning Difficulties. Jessica Kingsley
Conyers, C., Doole, A., Vause, T., Harapiak, S., Yu, C.T., & Martin, G.L. (2002). Predicting the relative efficacy of three presentation methods for assessing preferences of persons with developmental disabilities. Journal of Applied Behavior Analysis, Volume 35(1), pp. 49 – 58
Cook, J. (1996). Early sensory skills. Winslow Press
Cooke, J., & Williams, D.(1985). Working with children’s language. Winslow Press
Cooley, E.J., & Ayers, R.R. (1988). Self-concept and success-failure attributions of non-handicapped students and students with learning disabilities. Journal of Learning Disabilities, Volume 21(3), pp. 174 - 178
Coombes, K. (1986). Voice in cerebral palsied children. In - M. Fawcus (Ed.). Voice disorders and their management. Croom Helm
Cooper, S.A., Smiley, E., Jackson, A., Finlayson, J., Allan, L., Mantry, D., & Morrison, J. (2009). Adults with intellectual disabilities: prevalence, incidence and remission of aggressive behaviour and related factors. Journal of Intellectual Disability Research, Volume 53, pp. 217 - 232
Cornish, E. (2002). Gluten and casein free diets in autism: a study of the effects on food choice and nutrition. Journal of Human Nutrition and Dietetics, Volume 15(4), pp. 261 - 269
Corno, L, & Mandinach., E.B., (1983). The Role of Cognitive Engagement in Classroom Learning and Motivation, Educational Psychologist, Volume 18(2), pp. 88 - 108
Cortright, B. (2015). The Neurogenesis diet and lifestyle: Upgrade your brain, Upgrade your life. Psyche Media
Costandi, M. (2016). Neuroplasticity. MIT Press, Essential Knowledge Series
Coupe, J., Barton, L., Barber, M., Collins, L., Levy, D., & Murphy, D. (1985). Affective Communication Assessment. Manchester Education Committee
Coupe O'Kane, J., & Smith, B. (eds) (1994). Taking Control: Enabling People with Learning Difficulties. London: David Fulton.
Coupe O' Kane, J., & Goldbart, J. (1998). Communication Before Speech - Development and Assessment (2nd edition). London: David Fulton.
Courchesne, E., & Pierce, K. (2005). Why the frontal cortex in autism might be talking only to itself: local over-connectivity but long-distance disconnection. Current Opinion in Neurobiology, Volume 15(2), pp. 225 - 230
Courtemanche, A.B. (2010). Positive relationship development and the acquisition of communication and task compliance for individuals with profound intellectual developmental disabilities. Doctoral dissertation, University of Kansas
Crabbe, M. (2007). The Intensive Interaction research project… and beyond’, Royal College of Speech and Language Therapy Bulletin, August 2007, pp.12 - 13
Creber, P. (1972). Lost for words: Language and educational failure. Penguin Books
Creedon, M.P., & Baranek, G.T. (1988). Touch another way: Recognizing and managing tactile defensiveness at home and in the classroom. Proceedings of the Annual Conference of the Autism Society of America. pp. 49 – 54
Cripps, C., Tsiris, G., & Spiro, N. (Eds.). (2016). Research and resources for music therapy 2016: A compilation developed by the Nordoff Robbins research team. London: Nordoff Robbins
Croce, R., & Horvat, M. (1992). Effects of reinforcement based exercise on fitness and work productivity in adults with mental retardation. Adapted Physical Activity Quarterly, Volume 9(2), pp. 148 - 178
Crocker, A.G., Mercier, C., Lachapelle, Y., Brunet, A., Morin, D., & Roy, M.E. (2006). Prevalence and types of aggressive behaviour among adults with intellectual disabilities. Journal of Intellectual Disability, Volume 50, pp. 652 - 661
Crome, L. (1960). The brain and mental retardation. British Medical Journal, Volume 1(5177), pp. 897 - 904
Cromby, J.J., Standen, P.J., Newman, J., & Tasker, H. (1996). Successful transfer to the real world of skills practised in a virtual environment by students with severe learning difficulties. In - Proceedings 1st European Conference for Disability, Virtual Reality and Assoc. Tech., Maidenhead, UK.
Crosby, K.G., & Blatt, B. (1968). Attention and mental retardation. The Journal of Education, Volume 150(3), pp. 67 - 81
Crosby, K. (2002). Communication through music for pupils with profound and multiple learning difficulties. The SLD Experience, Volume 32. pp. 19 – 21
Csorba, J., Radvanyi, K., Regenyi, E., & Dinya, E. (2011). A study of behaviour profiles among intellectually disabled people in residential care in Hungary. Research in Developmental Disabilities, Volume 32(5), pp. 1757 – 1763
Culham, A. (2004). Getting in Touch with our Feminine Sides? Men's Difficulties and Concerns with Doing Intensive Interaction, British Journal of Special Education, Volume 31 (2), pp.81 - 88
Cullen, C. (1992). Staff training and management for intellectual disability services. International review of research in mental retardation, Volume 18, pp. 225 - 245
Cummins, R.A. (1991). Sensory Integration and Learning Disabilities: Ayres' Factor Analyses Reappraised. Journal of Learning Disabilities, Volume 24(3), pp. 160 - 168
Cunningham, C., & Glenn, S. (2004). Self-awareness in young adults with Down syndrome: I. Awareness of Down syndrome and disability. International Journal of Disability, Development and Education, Volume 51(4), pp. 335 - 361
Cunningham, R.D. (1996). Neuroimaging studies in children with developmental delay. Journal of Pediatrics. Volume 128(2), pp. 302
Cuskelly, M., & de Jong, I. (1996). Self-concept in children with Down syndrome. Down Syndrome: Research and Practice, Volume 4, pp. 59 - 64
Cuvo, A.J., May, M.M., & Post, T.M. (2001). Effects of living room, Snoezelen room, and outdoor activities on stereotypic behavior and engagement by adults with profound mental retardation. Research in Developmental Disabilities, Volume 22(3), pp. 183 - 204
Dairo, Y.M., Collett, J., Dawes, H., & Oskrochi, G.R. (2016). Physical activity levels in adults with intellectual disabilities: A systematic review. Preventive Medicine Reports, Volume 4, pp. 209 - 219
Dale, F.J. (1990). Stimulation Guide for Multi-Sensory Impaired Children. Chapman and Hall: London
Dalrymple, A.J. (1989). Sensory extinction of stereotyped object-dropping: Identification of a reinforcer for skill training. Behavioral Interventions. Volume 4(2), pp. 99 – 111
Dalton, P. (1994). Counselling people with communication problems. London: Sage Publications. ISBN 0-8039-8895-8
D’anci, K.E., Vibhakar, A., Kanter, J.H., Mahoney, C.R., & Taylor, H.A. (2009). Voluntary dehydration and cognitive performance in
trained college athletes. Perceptual and Motor Skills. Volume 109:. pp. 251 - 269
Dattilo, J., & Rusch, F.R. (1985). Effects of choice on leisure participation for persons with severe handicaps. Journal of the Association for Persons with Severe Handicaps, Volume 10(4), pp. 194 - 199
Dattilo, J. (1986). Computerized assessment of preference for severely handicapped individuals. Journal of Applied Behavior Analysis, Volume 19, pp. 445 - 448
Daveson, B., & Edwards, J. (1998). A role for music therapy in special education. International Journal of Disability, Development and Education, Volume 45(4), pp. 449 - 457
David, N., Newen, A., & Vogeley, K. (2008). The ‘‘sense of agency” and its underlying cognitive and neural mechanisms. Consciousness and Cognition. Volume 17, pp. 523 – 534
Davidson, P.W., Cain, N.N., Sloane-Reeves, J.E., Van Speybroech, A., Segel, J., Gutkin, J., Quijano, L.E., Kramer, B.M., Porter, B., & Shoham, I. (1994). Characteristics of community-based individuals with mental retardation and aggressive behavioral disorders. American Journal of Mental Retardation. Volume 98(6). pp. 704 - 716
Davidson, P.W., Houser, K.D., Cain, N.N., Sloane-Reeves, J., Quijano, L., Matons, L., Giesow, V., & Ladrigan, P.M. (1999). Characteristics of older adults with intellectual disabilities referred for crisis intervention. Journal of Intellectual Disability Research. Volume 43(1). pp. 38 - 46
Davies, C.A., & Jenkins, R. (1997). She has different fits to me: How people with learning difficulties see themselves. Disability and Society, Volume 12, pp. 95 - 109
Davies, L., & Oliver, C. (2013). Age related prevalence of aggression and self-injury in persons with an intellectual disability. Research in Developmental Disabilities, Volume 34, pp. 764 – 775
Davis, J. (2001). A Sensory Approach to the Curriculum: For Pupils with Profound and Multiple Learning Difficulties. David Fulton Publishers
Davis, P.K., Young, A., Cherry, H., Dahman,D., & Rehfeldt, R.A. (2004). Increasing the happiness of individuals with profound multiple disabilities: replication and extension, Journal of Applied Behavior Analysis, Volume 37(4), pp. 531 – 534
Davis, S., & Wehmeyer, M.L. (1991). Ten steps to independence: Promoting self-determination in the home. Arlington, TX: The Arc of the United States.
De Bildt, A., Sytema, S., Kraijer, D., Sparrow, S., & Minderaa, R. (2005). Adaptive functioning and behaviour problems in relation to level of education in children and adolescents with intellectual disability. Journal of Intellectual Disability Research, Volume 49(9), pp. 672 - 681
De Bono, E. (1985). Six Thinking Hats: An Essential Approach to Business Management. Little, Brown, & Company.
De Oliveira, M.F., Pinto, F.C.G., Nishikuni, K., Botelho, R.V., Lima, A.M., & Rotta, J.M. (2011). Revisiting hydrocephalus as a model to study brain resilience. Frontiers in human neuroscience, Volume 5, Article 181, pp. 1 - 4
De Vries, C., Yu, C.T., Sakko, G., Wirth, K.M., Walters, K.L., Carole, Marion, C. & Martin, G. (2005). Predicting the relative efficacy of verbal, pictorial, and tangible stimuli for assessing preferences of leisure activities. American Journal on Mental Retardation, Volume 110, pp. 145 – 154
De Waele, I., & Van Hove, G. (2005). Modern times: An ethnographic study on the quality of life of people with a high support need in a Flemish residential facility. Disability & Society, Volume 20(6), pp. 625 – 639
De Winter, C.F., Jansen, A.A.C., & Evenhuis, H.M. (2011). Physical Conditions and Challenging Behaviour in People with Intellectual Disability: A Systematic Review. Journal of Intellectual Disability Research. Volume 55(7), pp. 675 - 698
Dean, E.C., & Aitken, S. (1986). Functional communication in blind multiply-impaired children: a case study. Insight, Volume 4(1), pp. 7 - 11
Deb, S., Thomas, M., & Bright C. (2001). Mental disorder in adults with intellectual disability. 2: The rate of behaviour disorders among a community-based population aged between 16 and 64 years. Journal of Intellectual Disability Research, Volume 45, pp. 506 - 514
Dee, L., Byers, R., Hayhoe, H., & Maudslay, L. (2002). Enhancing Quality of Life – facilitating transitions for people with profound and complex learning difficulties: a literature review. London: Skill/Cambridge: University of Cambridge.
DeLeon, I.G., & Iwata, B.A. (1996). Evaluation of a multiple-stimulus presentation format for assessing reinforcer preferences. Journal of Applied Behavior Analysis, Volume 29, pp. 519 - 533
Delfour, F., & Marten, K. (2001). Mirror image processing in three marine mammal species: killer whales (Orcinus orca), false killer whales (Pseudorca crassidens) and California sea lions (Zalophus californianus), Behavioral Processes, Volume 53(3), pp. 181 - 190
deLissovoy, V. (1963). Head banging in early childhood: A suggested cause. Journal of Genetic Psychology, Volume 102, pp. 109 - 114
DeLong, G.R., & Heinz, E.R. (1997). The clinical syndrome of early-life bilateral hippocampal sclerosis. Annals of Neurology. Volume 42. pp. 11 – 17
Deng, W., Aimone, J.B., & Gage, F.H. (2010). New neurons and new memories: how does adult hippocampal neurogenesis affect learning and memory? Nature Reviews Neuroscience, Volume 11(5), pp. 339 - 350
Dennis, R. (2002). Nonverbal narratives: Listening to people with severe intellectual disability. Research and Practice for Persons with Severe Disabilities, Volume 27(4), pp. 239 - 249
Densem, J. F., Nuthall, G. A., Bushnell, J., & Horn, J. (1989). Effectiveness of a sensory integrative therapy program for children with perceptual-motor deficits. Journal of Learning Disabilities, Volume 22, pp. 221 - 229
Denton, D.M. (1970). Remarks in support of total communication. Communication symposium. Maryland school for the deaf. Frederick, MD.
Diamond, M.C., Krech, D., & Rosenzweig, M.R. (1964). The Effects of an Enriched Environment on the Histology of the Rat Cerebral Cortex. Journal of Comparative Neurology and Psychology. Volume 123. pp. 111 - 120
Diamond, M.C., Law, F., Rhodes, H., Lindner, B., Rosenzweig, M.R., Krech, D., & Bennett, E. (1966). Increases in cortical depth and glia numbers in rats subjected to enriched environment. Journal of Comparative Neurology. Volume 128 (1). pp. 117 – 125
Diamond, M.C., Rosenzweig, M.R., Bennett, E.L., Lindner, B., & Lyon, L. (1972). Effects of environmental enrichment and impoverishment on rat cerebral cortex. Journal of Neurobiology, Volume 3(1). pp. 47 - 64
Dickerson, L. (1995). Techniques for the integration of people who use alternative communication devices in the workplace. 3rd Annual Pittsburgh Employment Conference Proceedings. pp. 27 - 34. Pittsburgh: Shout Press
Didden, R., Korzilius, H., van Aperlo, B., van overloop, C., & de Vries, M. (2002). Sleep problems and daytime problem behaviours in children with intellectual disability. Journal of Intellectual Disability Research. Volume 46, pp. 537 – 547
Diego, M.A., Jones, N.A., Field, T., Hernandez-Reif, M., Schanberg, S., Kuhn, C., Galamaga, M., McAdam, V., & Galamaga, R. (1998). Aromatherapy positively affects mood, EEG patterns of alertness and math computations. International Journal of Neuroscience, Volume 96(3-4), pp. 217 - 224
Dieringer, S.T., Gumm, E., & Porretta, D. (2013). Using music therapy principles to enhance physical activity participation in children and adolescents with disabilities. PALAESTRA: Forum of Sport, Physical Education, and Recreation for Those with Disabilities, Volume 27(3), pp. 42 - 46
Dimaggio, G., Lysaker, P.H., Carcione, A., Nicolo, G., & Semerari, A. (2008). Know yourself and you shall know the other...to a certain extent: multiple paths of influence of self-reflection on mind reading, Consciousness and Cognition, Volume 17, pp. 778 – 789
Diorio, M.S., & Konarski, E.A. (1984). Evaluation of a method for teaching dressing skills to profoundly mentally retarded persons. American Journal of Mental Deficiency. Volume 89(3), pp. 307 - 309
Dixon-Ibarra, A., Lee, M., & Dugala, A. (2013). Physical activity and sedentary behavior in older adults with intellectual disabilities: a comparative study. Adapted Physical Activity Quarterly, Volume 30(1), pp. 1 - 19
Dobson, S., Dodsworth, S., & Miller, M. (2000). Problem solving in small multidisciplinary teams: a means of improving the quality of the communication environment for people with profound learning disability. British Journal of Learning Disability, Volume 28(1), pp. 25 - 30
Dobson, S., Upadhyaya, S., & Stanley, B. (2002). Using an interdisciplinary approach to training to develop the quality of communication with adults with profound learning disabilities by care staff. International Journal of Language & Communication Disorders, Volume 37(1), pp. 41 – 57
Doidge, N. (2007). The brain that changes itself: Stories of personal triumph from the frontiers of brain science. Penguin
Došen, A. (2007). Integrative treatment in persons with intellectual disability and mental health problems. Journal of Intellectual Disability Research, Volume 51(1), pp. 66 – 74
Dosman, C., Adams, D., Wudel, B., Vogels, L., Turner, J., & Vohra, S. (2013). Complementary, holistic, and integrative medicine: autism spectrum disorder and gluten-and casein-free diet. Pediatrics in Review:American Academy of Pediatrics, Volume 34(10), e36 - 41
Dote-Kwan, J., & Chen. D. (1999). Developing meaningful interventions. In D. Chen (Ed.), Essential elements in early communication visual impairments and multiple disabilities (pp. 287-336). New York: American Foundation for the Blind Press
Dowey, A., Toogood, S., Hastings, R.P., & Nash, S. (2007). Can brief workshop interventions change care staff understanding of challenging behaviours? Journal of Applied Research in Intellectual Disabilities, Volume 20(1), pp. 52 – 55
Dowling, J. (2011): Therapeutic storytelling, PMLD Link, Volume 23 (3), Issue 70. pp. 28 - 29
Dowling, S., Hassan, D., McConkey, R., & Breslin, G. (2012). Examining the relationship between physical activity and the health and wellbeing of people with intellectual disabilities: A literature review. Special Olympics Ireland and the University of Ulster
Downing, J.E. (Ed.) (2002). Including students with severe and multiple disabilities in typical classrooms: Practical strategies for
teachers (2nd ed.). Baltimore: Paul H. Brookes.
Downing, J.E., & Chen, D. (2003). Using tactile strategies with students who are blind and have severe disabilities. Teaching Exceptional Children, Volume 36(2), pp. 56 - 61
Downs, C., Morgan, M., Ouvry, C. & Porter, J. (2001). Interpreting the communication of people with profound and multiple learning
difficulties. British Journal of Learning Disabilities, Volume 29, pp. 12 - 16
Draganski, B., Gaser, C., Busch, V., Schuierer, G., Bogdahn, U., & May, A. (2004). Neuroplasticity: changes in grey matter induced by training. Nature, Volume 427(6972). pp.311 - 312
Draheim, C.C., Williams, D.P., & McCubbin, J.A. (2002). Prevalence of physical inactivity and recommended physical activity in community-based adults with mental retardation. Mental Retardation, Volume 40(6), pp. 436 – 444
Dubois, A., Capdevila, X., Bringuier, S., & Pry, R. (2010). Pain expression in children with intellectual disability. European Journal of Pain. Volume 14, pp. 654 – 660
Duggan, D. (1978). Goals and methods in dance therapy with severely multiply-handicapped children. American Journal of Dance Therapy. Volume 2(1), pp. 31 - 34
Duggan, D. (1995). The 4’s: A Dance Therapy Program for Learning-Disabled Adolescents, in Levy, F. J. (ed.), Dance and Other Expressive Arts Therapies: When Words are not enough, London: Routledge
Duggan, D., Stratton-Gonzalez, S., & Gallant, C. (2009). Dance Education for Diverse Learners: A Special Education Supplement to the Blueprint for Teaching and Learning in Dance. NYC Department of Education
Duker, P.C., & Jutten, W. (1997). Establishing gestural yes-no responding with individuals with profound mental retardation. Education and Training in Developmental Disabilities, Volume 32(1), pp. 62 - 75
Dunbar, R. (1996). Grooming, gossip and the evolution of language. Faber and Faber. ISBN 0-571-17396-9
Duncan, D., Matson, J.L., Bamburg, J.W., Cherry, K.E., & Buckley, T. (1999). The relationship of self-injurious behavior and aggression to social skills in persons with severe and profund learning disability. Research in Developmental Disabilities, Volume 20, pp. 441 - 448
Dunlap, G., Kern-Dunlap, L., Clarke, S., & Robbins, F.R. (1991). Functional assessment, curricular revision, and severe behavior problems. Journal of Applied Behavior Analysis, Volume 24, pp. 387 - 397
Dunn, W. (2001). The sensations of everyday life: Empirical, theoretical, and pragmatic considerations. American Journal of Occupational
Therapy, Volume 55, pp. 608 - 620.
Durand, V.M., & Kishi, G. (1987). Reducing severe behavior problems among persons with dual sensory impairments: An evaluation of a technical assistance model. Journal of the Association for Persons with Severe Handicaps, Volume 12, pp. 2 - 10
Durand, V.M., & Crimmins, D.B. (1988). Identifying the variables maintaining self-injurious behaviour. Journal of Autism and Developmental Disorders, Volume 18, 99 - 117
Durand, V.M., & Crimmins, D.B. (1991). Teaching functionally equivalent responses as an intervention for challenging behaviour, in B. Remington (Ed.), The Challenge of Severe Mental Handicap: a behaviour analytic approach. London: Wiley.
Dutt, A.S.K. (2010). The effects of skill training on preference for individuals with severe to profound multiple disabilities. PhD (Doctor of Philosophy) thesis, University of Iowa
Duval, S., & Wicklund, R.A. (1972). A Theory of Objective Self Awareness. New York: Academic Press.
Dyer, K., Schwartz, I.S., & Luce, S.C. (1984). A supervision program for increasing functional activities for severely handicapped students in a residential setting. Journal of Applied Behavior Analysis, Volume 17(2), pp. 249 - 259
Dyer, K., Dunlap, G., & Winterling, V. (1990). Effects of choice making on the serious problem behaviors of students with severe handicaps. Journal of Applied Behavior Analysis, Volume 23(4), pp. 515 - 524
Dykens, E.M., Rosner, B.A., Ly, T., & Sagun, J. (2005). Music and anxiety in Williams syndrome: A harmonious or discordant relationship? American Journal on Mental Retardation, Volume 110(5), pp. 346 - 358
Edmonds, C.J., & Burford, D. (2009) Should children drink more water?: the effects of drinking water on cognition in children. Appetite. Volume 52. pp. 776 - 779
Edmonds, C.J., & Jeffes, B. (2009). Does having a drink help you think? 6-7-Year-old children show improvements in cognitive performance from baseline to test after having a drink of water. Appetite. Volume 53. pp. 469 - 472
Edmonds, C.J., Crombie, R., & Gardner, M.R. (2013). Subjective thirst moderates changes in speed of responding associated
with water consumption. Frontiers in Human Neuroscience. Volume 7. Article 363
Edmonds, C.J., Crombie, R., Ballieux, H., Gardner, M.R., & Dawkins, L. (2013). Water consumption, not expectancies about water consumption, affects cognitive performance in adults. Appetite. Volume 60. pp. 148 - 153
Ehrsson, H.H. (2007). The experimental induction of out-of-body experiences. Science, Volume 317, pp. 1048 – 1048
Eiland, L., & Romeo R.D. (2013). Stress and the developing adolescent brain. Neuroscience, Volume 249. pp. 162 – 171
Einarsson, I.O., Ólafsson, Á., Hinriksdóttir, G., Jóhannsson, E., Daly, D., & Arngrímsson, S.A. (2015). Differences in physical activity among youth with and without intellectual disability. Medicine and Science in Sports and Exercise, Volume 47(2), pp. 411 - 418
Elbaum, B., & Vaughn, S. (2001). School-Based Interventions to Enhance the Self Concept of Students with Learning Disabilities: A Meta-Analysis. The Elementary School Journal, Volume 101(3), Special Issue: Instructional Interventions for Students with Learning Disabilities, pp. 303 - 329
Elder, J.H., Shankar, M., Shuster, J., Theriaque, D., Burns, S., & Sherrill, L. (2006). The gluten-free, casein-free diet in autism: results of a preliminary double blind clinical trial. Journal of autism and developmental disorders, Volume 36(3), pp. 413 - 420
Elder, J.H. (2008). The gluten-free, casein-free diet in autism: an overview with clinical implications. Nutrition in Clinical Practice, Volume 23(6), pp. 583 - 588
Elder, J.H., Kreider, C.M., Schaefer, N.M., & de Laosa, M.B. (2015). A review of gluten-and casein-free diets for treatment of autism: 2005–2015. Nutrition and Dietary Supplements, Volume 7, pp. 87 - 101
Elgie, S. & Maguire, N. (2001). Intensive Interaction with a woman with multiple and profound disabilities: a case study’, Tizard Learning Disability Review, Volume 6(3), pp.18 - 24
Elgie, S., & Hastings, R.P. (2002). Staff definitions of challenging behavior. Education and Training in Mental Retardation and Developmental Disabilities, Volume 37(2), pp. 202 – 208
Ellingford, J., James, I., Mackenzie, L., & Marsland, L. (2007): Using dolls to alter behaviour in patients with dementia. Nursing Times, Volume 103 (38). pp.36 - 37
Ellis, D. (Ed.)(1986). Sensory impairments in mentally handicapped people. Taylor & Francis.
Emerson, E., Barrett, S., Bell, C., Cummings, R., Hughes, H., McCool, C., Toogood, A., & Mansell, J. (1987). The Special Development Team: Developing Services for People with Severe Learning Difficulties and Challenging Behaviours. University of Kent at Canterbury
Emerson, E., Toogood, A., Mansell, J., Barrett, S., Bell, C., Cummings, R., & McCool, C. (1987). Challenging behaviour and community services: 1 Introduction and Overview, Mental Handicap, Volume 15, pp. 166 - 169
Emerson, E., Cummings, R., Barrett, S., Hughes, H., & McCool, C., & Toogood, A. (1988). Challenging Behaviour and community services: 2. Who are the people who challenge services? Mental Handicap, Volume 16, pp. 16 - 19
Emerson, E., Cummings, R., Hughes, H., Toogood, A., McCool, C., & Barrett, S. (1989). Challenging behaviour and community services. 6. Evaluation and overview. Mental Handicap, Volume 17, pp. 104 - 108
Emerson, E., & McGill, P. (1989). Normalisation and applied behaviour analysis: Values and technology in services for people with learning difficulties. Behavioural Psychotherapy, Volume 17, pp. 101 - 117
Emerson, E. (1990). Designing individualised community-based placements as an alternative to institutions for people with severe mental handicap and severe problem behaviour, in W.I. Fraser (Ed.), Key Issues in Mental Retardation Research. Routledge, London, pp. 395 - 404.
Emerson, E. (1992). Self-injurious behaviour: an overview of recent developments in epidemiological and behavioural research. Mental handicap Research. Volume 4, pp. 49 - 81
Emerson, E., Beasley, F., Offord, G., & Mansell, J. (1992) Specialised housing for people with seriously challenging behaviours. Journal of Mental Deficiency Research, Volume 36, pp. 291 - 307
Emerson, E., & McGill, P. (1993). Developing services for people with severe learning disabilities and seriously challenging behaviours: South East Thames Regional Health Authority, 1985-1991. In I. Fleming & B. Stenfert Kroese (Eds.), People with Severe Learning Difficulties who also Display Challenging Behaviour. Manchester: Manchester University Press
Emerson, E., McGill, P. and Mansell, J. (Eds.)(1994). Severe Learning Disabilities and Challenging Behaviours. London: Chapman and Hall.
Emerson, E. (1995). Challenging Behaviour: Analysis and Intervention in People with Learning Disabilities. Cambridge: Cambridge University Press.
Emerson, E., Cullen, C., Hatton, C. & Cross, B. (1996). Residential Provision for People with Learning Disabilities: Summary Report. Manchester: Hester Adrian Research Centre, Manchester University.
Emerson, E., Forrest, J., Cambridge, P., & Mansell, J. (1996). Community support teams for people with learning disabilities and challenging behaviours: results of a national survey. Journal of Mental Health, 5(4), pp. 395 - 406
Emerson, E., Alborz, A., Kiernan, C., Mason, H., Reeves, D., Swarbrick, R., & Mason, L. (1997). The Treatment & Management of Challenging Behaviour: HARC Challenging Behaviour Project Report 5. Manchester: Hester Adrian Research Centre.
Emerson, E., Robertson, J., Gregory, N., Hatton, C., Kessissoglou, S., Hallam, A., & Hillery, J. (2000). Treatment and Management of Challenging Behaviours in Residential Settings. Journal of Applied Research in Intellectual Disabilities, Volume 13(4), pp. 197 - 215
Emerson, E., Robertson, J., Gregory, N., Hatton, C., Kessissoglou, S., Hallam, A., Knapp, M., Jarbrink, K., Walsh, P.N., & Netten, A. (2000). The quality and costs of community-based residential supports, village communities and residential campuses in the United Kingdom. American Journal of Mental Retardation, Volume 105(2), pp. 81 - 102
Emerson, E., Robertson, J., Gregory, N., Kessissoglou, S., Hatton, C., Hallam, A., Knapp, M., Jarbrink, K., Netten, A. & Linehan, C. (2000). The quality and costs of community-based residential supports and residential campuses for people with severe and complex disabilities. Journal of Intellectual and Developmental Disability, Volume 25(4), pp. 263 - 279
Emerson, E. (2001). Challenging Behaviour: Analysis and Intervention in People with Severe Intellectual Disabilites. Second Edition. Cambridge University Press
Emerson, E., Kiernan, C., Alborz, A., Reeves, D., Mason, H., Swarbrick, R., Mason, L., & Hatton, C. (2001). The prevalence of challenging behaviors: a total population study. Research In Developmental Disabilities. Volume 22(1). pp. 77 - 93
Emerson, E. (2005). Underweight, obesity and exercise among adults with intellectual disabilities in supported accommodation in Northern England. Journal of Intellectual Disability Research, Volume 49(2), pp. 134 – 143
Emerson, E., & Baines, S. (2011). Health inequalities and people with learning disabilities in the UK. Tizard Learning Disability Review, Volume 16(1), pp. 42 - 48
Emerson, E., & Einfeld, S. (2011). Challenging Behaviour. Cambridge: Cambridge University Press
Erikson, E.H. (1950). Childhood and society. WW Norton & Company
European Food Safety Authority (2011). Scientific Opinion on the substantiation of health claims related to water and maintenance of normal physical and cognitive functions, maintenance of normal thermoregulation and basic requirement of all living things. Download http://www.efsa.europa.eu/en/efsajournal/pub/2075.htm
Evans, L. (1982). Total Communication: Structure and Strategy. Washington, DC: Galludet College Press
Evenhuis, H.M., & Nagtzaam, L.M.D. (1999). Onderzoeksprogramma chronisch zieken. Wetenschap en geneeskunde voor mensen met een verstandelijke handicap: Een nieuw ontgonnen gebied in de Nederlandse gezondheidszorg. Den Haag: NOW-MW
Evenhuis, H.M., Theunissen, M., Denkers, I., Verschuure, H., & Kemme, H. (2001). Prevalence of visual and hearing impairment in a Dutch institutionalized population with intellectual disability. Journal of Intellectual Disability Research, Volume 45(5), pp. 457 - 464
Eyman, R.K., & Call, T. (1977). Maladaptive behavior and community placement of mentally retarded persons. American Journal of Mental Deficiency, Volume 82, pp. 137 -144
Fadda, R., Rapinett, G., Grathwohl, D., Parisi, M., Fanari, R., Calo, C.M., & Schmitt, J. (2012). Effects of drinking supplementary water
at school on cognitive performance in children. Appetite. Volume 59. pp. 730 - 737
Fahey, A., & Carr, A. (2002). Prevention of adjustment difficulties in children with sensory impairments. In: A. Carr (ed.) Prevention: What works with Children and Adolescents? A Critical Review of Psychological Prevention Programmes for Children, Adolescents and their Families. East Sussex: Brunner-Routledge.
Farlow, L.J., & Snell, M.E. (2003). Teaching Basic Self-Care Skills. In - M. Snell & F. Brown (Eds.), Instruction of Students with Severe Disabilities. pp. 331 - 377. Ohio: Merill Prentice Hall, Colombus.
Farrell, M. (2006). The Effective Teacher's Guide to Moderate, Severe and Profound Learning Difficulties: Practical Strategies. Taylor & Francis
Farrell, P. (1991). Behavioural and interactive teaching for children with severe learning difficulties: Match or mismatch? Educational and Child Psychology, Volume 8(2), pp. 61 - 68
Farrell, P. (1997). Teaching Pupils with Learning Difficulties: Strategies and Solutions. London: Cassell.
Farrer, C., & Frith, C.D. (2002). Experiencing oneself vs another person as being the cause of an action: the neural correlates of the experience of agency, Neuroimage, Volume 15(3), pp. 596 – 603
Favell, J.E., & Cannon, P.R. (1976). Evaluation of entertainment materials for severely retarded persons. American Journal of Mental Deficiency, Volume 81, pp. 357 – 361
Favell, J.E., McGimsey, J.F., & Schell, R.M. (1982). Treatment of self-injury by providing alternate sensory activities. Analysis and Intervention in Developmental Disabilities, Volume 2, pp. 83 - 104
Favell, J.E., Realon, R.E., & Sutton, K.A. (1996). Measuring and increasing the happiness of people with profound mental retardation and physical handicaps. Behavioral Interventions, Volume 11(1), pp. 47 - 58
Felce, D., de Kock, U., & Repp, A.C. (1986). An eco-behavioural comparison of small community-based houses and traditional large hospitals for severely and profoundly mentally handicapped adults. Applied Research in Mental Retardation, Volume 7, pp. 393 - 408.
Felce, D., Saxby, H., de Kock, U., Repp, A., Ager, A., & Blunden, R. (1987). To what behaviors do attending adults respond?: A replication. American Journal of Mental Deficiency, Volume 91, pp.496 - 504
Felce, D., & Repp, A. (1992). The behavioral and social ecology of community houses. Research in Developmental Disabilities, Volume 13, pp. 27 - 42
Felce, D., Bowley, C., Baxter, H., Jones, E., Lowe, K., & Emerson, E. (2000). The effectiveness of staff support: evaluating active support training using a conditional probability approach. Research in Developmental Disabilities, Volume 21(4), pp. 243 - 255
Felce, D., Lowe, K., Beecham, J., & Hallam, A. (2000). Exploring the relationships between costs and quality of services for adults with severe intellectual disabilities and the most severe challenging behaviours in Wales: A multivariate regression analysis. Journal of Intellectual and Developmental Disability, Volume 25(4), pp. 307 - 326
Felce, D., Jones, E., & Lowe, K. (2002). Active support: planning daily activities and support for people with severe mental retardation. In S. Holburn & P.M. Vietze (Eds.), Person centered planning. Research, practice and future directions (pp.247-269). Baltimore: P.H.Brookes
Fernandez-Jaen, A. (2006). Attention deficit hyperactivity disorder and mental retardation. Revista de Neurologia, Volume 42, Supplement 2, 25 - 27
FEU/Mencap (1994). Learning for Life. FEU/Mencap; London.
Feuerstein, R., Feuerstein, R.S., Falik, L.H., & Rand, Y. (2006). Creating and Enhancing Cognitive Modifiability: The Feuerstein Instrumental Enrichment Program. Jerusalem, Israel: ICELP Press
Feuerstein, R., Feuerstein, R.S., & Falik, L.H. (2010). Beyond Smarter: Mediated Learning and the Brain’s Capacity to Change. New York: Teacher’s College Press
Feuillet, L., Dufour, H., & Pelletier, J. (2007). Brain of a white-collar worker. The Lancet, Volume 370(9583), pp. 262
Field, S. (1996). Self-determination instructional strategies for youth with learning disabilities. Journal of Learning Disabilities, Volume 29, pp. 40 – 52
Field, S., Martin, J.E., Miller, R.J., Ward, M.J., & Wehmeyer, M.L. (1998). A practical guide for teaching self-determination. Reston, VA: Council for Exceptional Children.
Field, S., Sarver, M.D., & Shaw, S.F. (2003). Self-determination: A key to success in post secondary education for students with learning disabilities. Remedial and Special Education, Volume 24, pp. 339 – 349.
Filipek, P.A. (1999). Neuroimaging in the developmental disorders: the state of the science. The Journal of Child Psychology and Psychiatry and allied disciplines. Volume 40(1), pp. 113 – 128
Filippi, C.G., Uluğ, A.M., Deck, M.D., Zimmerman, R.D., & Heier, L.A. (2002). Developmental delay in children: assessment with proton MR spectroscopy. American Journal of Neuroradiology, Volume 23(5), pp. 882 - 888
Fine, A. (Ed) (2010). Handbook on Animal Assisted Therapy: Theoretical Foundations and Guidelines for Practice (3rd ed). Elsevier, London
Finlay, W.M.L., & Lyons, E. (1998). Social identity and people with learning difficulties: Implications for self-advocacy groups. Disability and Society, Volume 13, pp. 37 - 51
Finlay, W.M.L., & Lyons, E. (2000). Social categorisations, social comparisons and stigma:Presentations of self in people with learning difficulties. British Journal of Social Psychology, Volume 39, pp. 129 - 146
Finlay, W.M.L., Antaki, C., Walton, C., & Stribling, P. (2008). The dilemma for staff in "playing a game" with a person with profound intellectual disabilities: empowerment, inclusion and competence in interactional practice. Sociology of Health & Illness, Volume 30(4), pp. 531 - 549
Finlayson, J., Jackson, A., Cooper, S.A., Morrison, J., Melville, C., Smiley, E., Allan, L., & Mantry, D. (2009). Understanding predictors of low physical activity in adults with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 22(3), pp. 236 - 247
Firth, G. (2006). Intensive Interaction – a Research Review’, Mental Health and Learning Disabilities Research and Practice, Volume 3(1), pp. 53 - 58
Firth, G. (2008). A Dual Aspect Process Model of Intensive Interaction, British Journal of Learning Disabilities, Volume 37, pp. 43 – 49
Firth, G., Elford, H., Leeming, C., & Crabbe, M. (2008). Intensive Interaction as a Novel Approach in Social Care: Care Staff’s Views on the Practice Change Process, Journal of Applied Research in Intellectual Disabilities, Volume 21, pp. 58 - 69
Fisch, L. (1969). Hearing loss and cerebral palsy. In - Blencowe, S. (Ed.). Cerebral palsy and the young child. Livingstone
Fisher, A.F., & Dunn, W.D. (1983). Tactile Defensiveness: Historical Perspectives, new Research – A Theory Grows. Sensory Integration Special Interest Section Newsletter, Volume 6(2), pp. 1 - 2
Fisher, D., & Frey, N. (2014). Checking For Understanding: Formative Assessment Techniques for your Classroom. ASCD
Fisher, A.V., Godwin, K.E., & Seltman, H. (2014). Visual environment, attention allocation, and learning in young children: When too much of a good thing may be bad. Psychological Science, Volume 25(7), pp. 1362 - 1370
Fisher, W.W., Piazza, C.C., Bowman, L.G., Hagopian, L.P., Owens, J.C., & Slevin, I. (1992). A comparison of two approaches for identifying reinforcers for persons with severe and profound disabilities. Journal of Applied Behavior Analysis, Volume 25, pp. 491 – 498
Fisher, W.W., Piazza, C.C., Bowman, L.G., & Amari, A. (1996). Integrating caregiver report with a systematic choice assessment to enhance reinforcer identification. American Journal on Mental Retardation, Volume 101, pp. 15 - 25
Fisher, W.W., Thompson, R.H., Piazza, C.C., Crosland, K., & Gotjen, D. (1997). On the relative reinforcing effects of choice and differential consequence. Journal of Applied Behavior Analysis, Volume 30, pp. 423 - 438
Flaherty, A.W. (2003). Writing like crazy: a word on the brain. Chronicle of Higher Education, Volume 50(13), pp. 1 - 6
Flaherty, A.W. (2004). The Midnight Disease. Press Release. Houghton Mifflin Company
Flaherty, A.W. (2015). The midnight disease: The drive to write, writer's block, and the creative brain. Houghton Mifflin Harcourt.
Flora, S.R., & Polenick, C.A. (2013). Effects of Sugar Consumption on Human Behavior and Performance. The Psychological Record, Volume 63, pp. 1 – 12
Fodstad, J., & Matson, J. (2008). A comparison of feeding and mealtime problems in adults with intellectual disabilities with and without autism. Journal of Developmental and Physical Disabilities, Volume 20(6), pp. 541 - 550
Foote, A.L., & Crystal, J.D. (2007). Metacognition in the Rat. Current Biology. Volume 17(6), pp. 551 – 555
Foreman, P., & Arthur, M. (2002). Parental perspectives on educational programmes for students with high support needs. European Journal of Special Needs Education, Volume 17, pp. 175 – 184
Foreman, P., Arthur-Kelly, M., Pascoe, S., & Smyth King, B. (2004). Evaluating the Educational Experiences of Students with Profound and Multiple Disabilities in Inclusive and Segregated Classroom Settings: An Australian Perspective. Research and Practice for Persons with Severe Disabilities, Volume 29(3), pp. 183 - 193
Foreman, P., Arthur‐Kelly, M., Bennett, D., Neilands, J., & Colyvas, K. (2014). Observed changes in the alertness and communicative involvement of students with multiple and severe disability following in‐class mentor modelling for staff in segregated and general education classrooms. Journal of Intellectual Disability Research, Volume 58(8), pp. 704 - 720
Forster, S., & Iacono, T. (2008). Disability support workers’ experience of interaction with a person with profound intellectual disability. Journal of Intellectual and Developmental Disability, Volume 33(2), pp. 137 - 147
Forster, S. (2010). Age-appropriateness: Enabler or barrier to a good life for people with profound intellectual and multiple disabilities? Journal of Intellectual & Developmental Disability, Volume 35(2): pp. 129 – 131
Forster, S. (2011). An ethical dilemma of too much listening and responding. PMLD Link, Volume 23(1). pp. 5 - 6
Forster, S., Gray, K.M., Taffe, J., Einfeld, S.L., & Tonge, B.J. (2011). Behavioural and emotional problems in people with severe and profound intellectual disability, Journal of Intellectual Disability Research, Volume 55(2), pp. 190 – 198
Fowler, C.H., Konrad, M., Walker, A.R., Test, D.W., & Wood, W.M. (2007). Self-determination interventions’ effects on the academic performance of students with developmental disabilities. Education and Training in Developmental Disabilities, Volume 42, pp. 270 – 285
Fowler, S. (2007). Sensory Stimulation. Jessica Kingsley Publishers
Fowler, S. (2008). Multisensory Rooms and Environments: Controlled Sensory Experiences for People with Profound and Multiple Disabilities: A Guide to Controlled Sensory Experiences. Jessica Kingsley Publishers
Fox, R.A., & Rotatori, A.F. (1982). Prevalence of obesity among mentally retarded adults. American Journal of Mental Deficiency. Volume 87(2), pp. 228 - 230
Fox, R.A., & Wade, E. (1998). Attention deficit hyperactivity disorder among adults with severe and profound mental retardation. Research in Developmental Disabilities, Volume 19(3), pp. 275 - 280
Foxall, E.L. (2002). The use of horses as a means of improving communication abilities of those with autism spectrum disorders: an investigation into the use and effectiveness of the horse as a therapy tool for improving communication in those with autism. Unpublished
manuscript. Coventry, UK: Coventry University.
Fragala, M.S., Beyer, K.S., Jajtner, A.R., Townsend, J.R., Pruna, G.J., Boone, C.H., Bohner, J.D., Fukuda, D.H., Stout, J.R., & Hoffman, J.R. (2014). Resistance exercise may improve spatial awareness and visual reaction in older adults. The Journal of Strength & Conditioning Research, Volume 28(8), pp.2079 - 2087
Fragkouli, A. (2013). Music therapy in special schools: The assessment of the quality of relationship. Approaches: Music Therapy & Special Music Education, Volume 5(2), pp. 152 - 165. Retrieved from: http://approaches.gr/musictherapy-in-special-schools-the-assessment-of-the-quality-of-relationship-aspasia-fragkouli/.
Francis, D., Diorio, J., Plotsky, P.M., & Meaney, M.J. (2002). Environmental enrichment reverses the effects of maternal separation on stress reactivity. Journal of Neuroscience, Volume 22(18), pp. 7840 - 7843
Fraser, W.I., Leudar, I., Gray, J., & Campbell, I. (1986) Psychiatric and behaviour disturbance in mental handicap. Journal of Mental Deficiency Research, Volume 30, pp. 49 - 57
Frey, G.C. (2004). Comparison of physical activity levels between adults with and without mental retardation. Journal of Physical Activity and Health, Volume 1(3), pp. 235 - 245
Frey G.C., Buchanan A.M., & Rosser Sandt D.D. (2005). ‘‘I’d Rather Watch TV’’ an examination of physical activity in adults with mental retardation. Mental Retardation. Volume 43, pp. 241 - 254
Frey G.C., Stanish H., & Temple V.A. (2008). Physical activity of youth with intellectual disability. Review and research agenda. Adapted Physical Activity Quarterly. Volume 25, pp. 95 – 117
Frymier, A.B., & Mongeau, P.A. (1997). Communicating with Touch in the Teacher/Student Relationship. Paper presented at the Annual Meeting of the Eastern Communication Association (Baltimore, MD, April 10-13)
Fuglestad, A.J., Rao, R., & Georgieff, M.K. (2008). The Role of Nutrition in Cognitive Development . In - C. Nelson & M. Collin (Eds), Handbook of Developmental Cognitive Neuroscience. pp. 623 - 641. MIT Press; 2nd revised edition
Fulton, K., Woodley, K. & Sanderson, H. (2008). Supported Decision Making: A guide for supporters, Paradigm
Furniss, F., & Biswas, A.B. (2012). Recent research on aetiology, development and phenomenology of self-injurious behaviour in people with intellectual disabilities: a systematic review and implications for treatment. Journal of Intellectual Disability Research, Volume 56(5), pp. 453 - 475
Fyson, R., & Cromby, J. (2010). Memory, sexual abuse and the politics of learning disability. In - Haaken, J. & Reavey, P., Memory Matters: contexts for understanding sexual abuse recollections, (pp. 157 - 174) Hove, Routledge
Fyson, R., & Cromby, J. (2013). Human rights and intellectual disabilities in an era of ‘choice’. Journal of Intellectual Disability Research, Volume 57(12), pp. 1164 - 1172
Gabrielli, O., Salvolini, U., Bonifazi, V., Ciferri, L., Lanza, R., Rossi, R., Coppa, G.V., & Giorgi, P.L. (1993). Morphological studies of the corpus callosum by MRI in children with malformative syndromes. Neuroradiology, Volume 35(2), pp. 109 - 112
Gabrielli, O., Coppa, G.V., Manzoni, M., Carloni, I., Kantar, A., Maricotti, M., & Salvolini, U. (1998). Minor cerebral alterations observed by magnetic resonance imaging in syndromic children with mental retardation. European Journal of Radiology, Volume 27(2), pp. 139 - 144
Gabrielli, O., Bruni, S., Coppa, G.V., Carloni, I., Polonara, G., Regnicolo, L., Salvolini, S., & Salvolini, U. (2002). White-matter alterations and callosal abnormalities in syndromic patients with mental retardation. Journal of Child Neurology, Volume 17(3), pp.164 - 168
Gaddes, W.H. (1985). Learning Disabilities and Brain Function: A Neuropsychological Approach. Second Edition. New York: Springer Science and Business Media
Gal, E., Dyck, M., & Passmore, A. (2009). The relationship between stereotyped movements and self-injurious behavior in children with developmental or sensory disabilities. Research in Developmental Disabilities, Volume 30(2), pp. 342 – 352
Gallagher, S. (2000). Philosophical conceptions of the self: Implications for cognitive science. Trends in Cognitive Sciences, Volume 4(1), pp. 14 – 21
Gallup, G.G., Jr. (1970). Chimpanzees: self-recognition. Science, Volume 167: pp. 86 - 87
Gallup, G.G., Jr., McClure, M.K., Hill, S.D., and Bundy, R.A. (1971). Capacity for self-recognition in differentially reared chimpanzees. Psychological Record, Volume 21: pp. 69 - 74
Gallup, G.G., Jr. (1979). Self-recognition in chimpanzees and man: A developmental and comparative perspective. New York: Plenum Press.
Gallup, G.G., Jr. (1982). Self-awareness and the emergence of mind in primates. American Journal of Primatology, Volume 2, pp. 237 - 248
Gallup, G.G. Jr. (1985). Do minds exist in species other than our own? Neuroscience and Biobehavioral Reviews, Volume 9, pp. 631 - 641
Gallup, G.G., Jr., and Suarez, S.D. (1986). Self-awareness and the emergence of mind in humans and other primates. In - J. Suls and A. Greenwald (eds.), Psychological Perspectives on the Self (Vol. 3), pp. 3-26. Hillsdale, N.J.: Erlbaum.
Gallup, G.G., Jr. (1987). Self-awareness. In J.R. Mitchell (ed.) Comparative Primate Biology, Behavior, Cognition, and Motivation, Volume 2B, pp. 3 - 16. New York: Liss.
Gallup, G.G., Jr. (1994). Self-recognition: research strategies and experimental design. In S.T. Parker, R.W. Mitchell & M.L. Boccia (Eds.),
Self-awareness in animals and humans: developmental perspectives, pp. 35-50. New York: Cambridge University Press.
Gallup, G.G., Jr., Povinelli, D.J., Suarez, S.D., Anderson, J.R., Lethmate, J., and Menzel, E. (1995). Further reflections on self-recognition in primates. Animal Behaviour, Volume 50: pp. 1525 - 1532
Ganio, M.S., Armstrong, L.E., Casa, D.J., McDermott, B.P., Lee, E.C., Yamamoto, L.M., Marzano, S., Lopez, R.M., Jimenez, L., Le. B.L., Chevillotte, E., & Lieberman, H.R. (2011). Mild dehydration impairs cognitive performance and mood of men. British Journal of Nutrition. Volume 106. pp. 1535 - 1543
Gardner, A. & Rikberg Smyly, S. (1997). How do we stop doing and start listening: responding to the emotional needs of people with learning disabilities, British Journal of Learning Disabilities, Volume 25, pp. 26 - 30
Gardner, J.M. (1985). Using microcomputers to help staff reduce violent behavior. Computers in Human Services, Volume 1, pp. 53 - 61
Garretson, M.D. (1976). Total Communication, In - A bicentennial monograph on hearing impairment: Trends in the USA, Frizina, D.R. (Ed.), pp. 88 - 95, Washington, DC: Alexander Graham Bell Association for the Deaf
Gaskell, G., Dockrell, J., & Rehman, H. (1995) Community care for people with challenging behaviors and mild learning disability: An evaluation of an assessment and treatment unit. British Journal of Clinical Psychology, Volume 34(3), pp. 383 - 395
Gaylord-Ross, R.J. (1982). Curricular considerations in treating behavior problems of severely handicapped students. In K.D. Gadow and I. Bialer (Eds.), Advances in Learning and Behavioral Disabilities, Volume 1. JAI Press, Greenwich CT, pp.193 - 224
Geake, J. (2009). The Brain at School, Educational Neuroscience in the classroom. Open University Press.
Geary, D.C. (2000). From infancy to adulthood: The development of numerical abilities. European Child & Adolescent Psychiatry, Volume 9 (Supplement 2), S11 - S16
George, M.S., Costa, D.C., Kouris, K., Ring, H.A., & Ell, P.J. (1992). Cerebral blood flow abnormalities in adults with infantile autism. The Journal of Nervous and Mental Disease, Volume 180(7), pp. 413 - 417
Gergely, G. (2001). The obscure object of desire: ‘Nearly but clearly not, like me’: Contingency preference in normal children versus children with autism. Bulletin of the Menninger Clinic, Volume 65, pp. 411 - 426
Gergely, G., & Watson, J.S. (1999). Early social-emotional development: Contingency perception and the social-biofeedback model. In P. Rochat (Ed.). Early social cognition: Understanding others in the first months of life (pp. 101 - 136). Mahwah, NJ: Erlbaum.
Gerrity, Kevin W., Hourigan, Ryan M., & Horton, Patrick W. (2013). Conditions that facilitate music learning among students with special needs: A mixed-methods inquiry. Journal of Research in Music Education, Volume61(2), 144 - 159
Ghaem, O., Mellet, E., Crivello, F., Tzourio, N., Mazoyer, B., Bethoz, A., & Denis, M. (1997). Mental navigation along memorized routes activates the hippocampus, precuneus, and insula. NeuroReport, Volume 8. pp. 739 – 744
Gilbert, D. (2006). Stumbling on to happiness. New York: Alfed. A. Knopf
Gleason, J.J. (1993). The creation of meaning: what persons with severe or profound multiple developmental disabilities do in context. Australia and New Zealand Journal of Developmental Disabilities, Volume 18(3), pp. 157 - 167
Gledhill, K. (2009). Life experience packages (LEPs). Information Exchange, Volume 79, pp. 21 - 22
Glenn, S. (1987). Interactive approaches to working with children with profound and multiple learning difficulties, In Smith, B. (Ed), Interactive Approaches to the Education of Children with Severe Learning Difficulties. Birmingham: Westhill College
Glenn, S.M., & Cunningham, C.C. (2001). Evaluation of self by young people with Down syndrome. International Journal of Disability, Development and Education, Volume 48, pp. 163 - 177
Glenn, S.M, & Cunningham, C.C. (2004). Self-awareness in Young Adults with Down Syndrome: II. Self-understanding. International Journal of Disability, Development and Education, Volume 51(4), pp. 363 - 381
Godwin, K.E., Almeda, M.V., Seltman, H., Kai, S., Skerbetz, M.D., Baker, R.S., & Fisher, A.V. (2016). Off-task behavior in elementary school children. Learning and Instruction, Volume 44, pp. 128 - 143
Goldbart, J. (1994). Opening the communication curriculum to students with PMLDs. In - Jean Ware (Ed.), Educating Children with Profound and Multiple Learning Difficulties. pp. 15 - 62. David Fulton Publishers
Golden, J., & Reese, M. (1996). Focus on communication: Improving interaction between staff and residents who have severe or profound mental retardation. Research in Developmental Disabilities, Volume 17(5), pp. 363 - 382
Goldsmith, H.H., Van Hulle, C.A., Arneson, C.L., Schreiber, J.E., & Gernsbacher, M.A. (2006). A Population-Based Twin Study of Parentally Reported Tactile and Auditory Defensiveness in Young Children. Journal of Abnormal Child Psychology, Volume 34(3), pp. 378 – 392
Gomez-Pinilla, F. (2008). Brain foods: The effects of nutrients on brain function, Nature Reviews Neuroscience. Volume 9. pp. 568 -578
González, M.J., Miranda-Massari, J.R., Rodríguez Gómez, J., Ricart, C.M. & Rodriguez-Pagán, D. (2012). Energy Drinks and Health: A Brief Review of their Effects and Consequences. Ciencias de la Conducta. Volume 27(1). pp. 23 - 34
Goode, D. (2010). A world without words: The social construction of children born deaf and blind. Temple University Press.
Goodman, K. (2007). Music Therapy Group work with Special Needs Children. Springfield, IL: Charles C Thomas
Goodman, L. (1990). Time and learning in the special education classroom. Suny Press
Goodwin, D.L., Krohn, J., & Kuhnle, A. (2004). Beyond the wheelchair: The experience of dance. Adapted Physical Activity Quarterly, Volume 21(3), pp. 229 - 247
Goodwin, M., & Edwards, C. (2009). I’m Creative Too. PMLD Link, Volume
Goodwin, M., & Edwards, C. (2012). Playing or Playing Up? Behaviours and Schema with Young People with Severe Learning Disabilities. Bristol: Share – Short Breaks Network Magazine
Goodwin, M. (2013). Listening and responding to children with PMLD – towards a framework and possibilities. SLD Experience, Volume 65, pp. 21 - 27
Goodyer, I. (1995). Parents who don’t want peace and quiet. Article in - Times Educational Supplement. September 15, 1995, no 4133, page 13
Goold, L., & Hummell, J. (1993). Supporting the receptive communication of individuals with Significant Multiple Disabilities: selective use of touch to enhance comprehension. North Rocks, Australia: North Rocks Press
Gopinathan, P.M., Pichan, G., & Sharma, V.M. (1988). Role of dehydration in heat stress-induced variations in mental performance. Archives of Environmental Health, Volume 43. pp.15 - 17
Goss, P. (2006). Meaning-led learning for pupils with severe and profound and multiple learning difficulties. British Journal of Special Education. Volume 33 (4), pp. 210 - 219
Goswami, U. (2008). Cognitive Development: The Learning Brain. Hove: Psychology Press
Got, I.L.S., & Cheng, S.T. (2008). The effects of art facilitation on the social functioning of people with developmental disability. Art Therapy: Journal of the American Art Therapy Association, Volume 25(1), pp. 32 – 37
Gourgouvelis, J., Yielder, P., & Murphy, B. (2017). Exercise Promotes Neuroplasticity in Both Healthy and Depressed Brains: An fMRI Pilot Study. Neural Plasticity, Volume 2017, 13 pages
Grace, J. (2014). Sensory Stories for Children and Teens with Special Educational Needs. Jessica Kingsley Publishers
Grace, J. (2017). Sensory-Being for Sensory Beings: Creating Entrancing Sensory Experiences. Routledge
Graham, A., & Reid, G. (2000). Physical fitness of adults with an intellectual disability: A 13-year follow-up study. Research Quarterly for Exercise and Sport, Volume 71(2), pp. 152 - 161
Graham, J. (2004). Communicating with the uncommunicative: music therapy with pre-verbal adults. British Journal Learning Disability, Volume 32(1), pp. 24 - 29
Grandgeorge, M., Tordjman, S., Lazartigues, A., Lemonnier, E., Deleau, M., & Hausberger, M. (2012). Does pet arrival trigger prosocial behaviors in individuals with autism? PLoS ONE, Series 7: e41739
Grandin, T. (1992). An inside view of autism. In E. Schopler & G.B. Mesibov (Eds), High Functioning Individuals with Autism. Plenum Press, New York.
Grandin, T. (1992). My Experiences with Visual Thinking Sensory Problems and Communication Difficulties. Center for the Study of Autism
Grandin, T. (1996). Thinking in Pictures. New York: Vintage Books, Random House.
Grandjean, A.C. (2007). Dehydration and cognitive performance. Journal of the American College of Nutrition. Volume 26 (Supplement). pp. 549 - 554
Granlund, M., & Olsson, C. (1991). Investigating communicative functions in profoundly retarded persons: A comparison of two methods of obtaining information about communicative behaviours. Mental Handicap Research, Volume 6(2), pp. 112 - 119
Granlund, M., Steensson, A.L., Sundin, M., & Olsson, C. (1992). Inservice training in collaborative problem solving and goal setting for special education teacher consultants working with profoundly impaired persons. British Journal of Mental Subnormality, Volume 38(Part 2), pp. 94 - 113
Granlund, M., Terneby, J., & Olsson, C. (1992a). Creating communicative opportunities through a combined in-service training and supervision package. European Journal of Special Needs Education, Volume 7(3), pp. 229 - 252
Granlund, M., Terneby, J., & Olsson, C. (1992b). Subject characteristics and the communicative environment of profoundly retarded adults. Scandinavian Journal of Educational Research, Volume 36(4), pp. 323 - 338
Granlund, M., Björck-Åkesson, E., Brodin, J., & Olsson, C. (1995). Communication intervention for persons with profound disabilities: A Swedish perspective. Augmentative and Alternative Communication, Volume 11(1), pp. 49 - 59
Granlund, M., & Olsson, C. (1999). Efficacy of communication intervention for pre-symbolic communicators. Augmentative and Alternative Communication, Volume 15, pp. 25 - 37
Grant, A. (2013). Give and Take: A Revolutionary Approach to Success. Viking Books
Grant, G.W.B., & Moores, B. (1977). Resident characteristics and staff behavior in two hospitals for mentally retarded adults. American Journal of Mental Deficiency, Volume 82(3), pp. 259 - 265
Gray, B., & Ridden, G. (1999). Lifemaps of people with learning disabilities, Jessica Kingsley Publishers
Gray, R., & McAnespie, L. (2004) Consulted or excluded? Learning Disability Practice, Volume 7 (6), pp. 30 - 32
Greathead, S., Yates, R., Hill, V., Kenny, L., Croydon, A., & Pellicano, E. (2016). Supporting Children With Severe-to-Profound Learning Difficulties and Complex Communication Needs to Make Their Views Known: Observation Tools and Methods. Topics in Language Disorders. Volume 36(3), pp. 217 - 244
Green, C.W., Reid, D.H., White, L.K., Halford, R.C., Brittain, D.P., & Gardner, S M. (1988). Identifying reinforcers for persons with profound handicaps: Staff opinion versus systematic assessment of preferences. Journal of Applied Behavior Analysis, Volume 21(1), pp. 31 - 43
Green, C.W., Reid, D.H., Canipe, V.S., & Gardner, S.M. (1991). A comprehensive evaluation of reinforcer identification processes for persons with profound multiple handicaps. Journal of Applied Behavior Analysis, Volume 24, pp. 537 - 552
Green, C W., Reid, D.H., Perkins, L.I., & Gardner, S.M. (1991). Increasing habilitative services for persons with profound handicaps: An application of structural analysis to staff management. Journal of Applied Behavior Analysis, Volume 24, pp. 459 – 471
Green, C.W., Gardner, S.M., Canipe, V.S., & Reid, D.H. (1994). Analyzing alertness among people with profound multiple disabilities: implications for provision of training. Journal of Applied Behavior Analysis, Volume 27(3), pp. 519 - 531
Green, C.W., & Reid, D.H. (1996). Defining, validating, and increasing indices of happiness among people with profound multiple disabilities. Journal of Applied Behavior Analysis, Volume 29(1), pp. 67 – 78
Green, C.W., Gardner, C.M., & Reid, D.H. (1997). Increasing indices of happiness among people with profound multiple disabilities: a program replication and component analysis. Journal of Applied Behaviour Analysis, Volume 30 (2) pp. 217 - 228
Green, C.W., & Reid, D.H. (1999). A behavioral approach to identifying sources of happiness and unhappiness among individuals with profound multiple disabilities, Behavior Modification, Volume 23(2), pp. 280 – 293
Green, C.W., Middleton, S., & Reid, D.H. (2000). Embedded evaluation of preferences sampled from person-centered plans for people with profound multiple disabilities. Journal of Applied Behavior Analysis, Volume 33 (4), pp. 639 - 642
Green, C.W., Reid, D.H., Rollyson, J.H. & Passante, S.C. (2005). An enriched teaching program for reducing resistance and indices of unhappiness among individuals with profound multiple disabilities. Journal of Applied Behavior Analysis, Volume 38(2), pp. 221 – 233
Greenspan, S.I. (1996). The Challenging Child: Understanding, Raising, and Enjoying the Five 'Difficult' Types of Children. Da Capo Press
Griffin, J.C., Ricketts, R.W.,& Williams, D.E. (1986). Reaction to Richmond et al.: propriety of mechanical restrainst and protective devices as tertiary techniques. In K.D. Gadow (Ed.), Advances in Learning and Behavioural Disabilities.(Volume 5. London, JAI Press
Griffiths, C.R. (2010). Attuning: A Theory of Interaction of People with Severe and Profound Intellectual and Multiple Disability and Their Carers. Doctoral dissertation, Trinity College Dublin
Griffiths, M. (1994). Transition to Adulthood: The Role of Education for Young People with Severe Learning Difficulties. David Fulton; London.
Griffiths, M., & Tennyson, C. (1997). The Extended Curriculum: Meeting the Needs of Young People. David Fulton Publishers
Gron, G., Wunderlich, A.P., Spitzer, M., Tomczak, R., & Riepe, M.W. (2000). Brain activation during human navigation: gender-different neural networks. Nature Neuroscience, Volume 3. pp. 404 – 408
Gross, D.W., Li, L.M., & Andermann, F. (1998) Catastrophic deterioration and hippocampal atrophy after childhood status epilepticus. Annals of Neurology, Volume 43(5). pp. 687- 692
Grove, N., Porter, J., Bunning, K., & Olsson, C. (1999). See What I Mean: Interpreting the Meaning of Communication by People with Severe and Profound Learning Difficulties: Theoretical and Methodological Issues. Journal of Applied Research in Intellectual Disabilities, Volume 12 (3), pp. 190 - 203
Grove, N. (2001). See What I Mean: Guidelines to Aid Understanding of Communication by People with Severe and Profound Learning Disabilities. BILD Publications
Guenther, K. (2016). ‘It’s All Done With Mirrors’: V.S. Ramachandran and the Material Culture of Phantom Limb Research. Medical History. Volume 60(3). pp. 342 - 358
Guess, D., Benson, H. A., & Siegel-Causey, E. (1985). Concepts and issues related to choice-making and autonomy among persons with severe disabilities. Journal of The Association for Persons with Severe Handicaps, Volume 10 (2), pp. 79 - 86
Guess, D., Mulligan-Ault, M., Roberts, S., Struth, J., Siegel-Causey, E., Thompson, B., Bronicki, G.B., & Guy, B. (1988). Implications of biobehavioral states for the education and treatment of students with the most profoundly handicapping conditions. Journal of the Association for Persons with Severe Handicaps, Volume 13(3), pp. 163 - 174
Guess, D., & Carr, E.G. (1991). Emergence and Maintenance of of stereotypy and self-injury. American Journal on Mental Retardation. Volume 96, pp. 299 - 319
Guess, D., Roberts, S., Siegel-Causey, E., Ault, M., Guy, B., & Thompson, B. (1993). Analysis of behavior state conditions and associated environmental variables among students with profound handicaps. American Journal on Mental Retardation, Volume 97(6), pp. 634 - 653
Guess, D., Roberts, S., Siegel-Causey, E., & Rues, J. (1995). Replication and extended analysis of behavior state, environmental events, and related variables among individuals with profound disabilities. American Journal on Mental Retardation, Volume 100(1), pp. 36 – 50
Guess, D., & Siegel-Causey, D. (1995). Attractor dimensions of behavior state changes among individuals with profound disabilities. American Journal on Mental Retardation, Volume 99(6), pp. 642 - 663
Guess, D., Roberts, S., & Rues, J. (2002). Longitudinal analysis of state patterns and related variables among infants and children with significant disabilities. Research and Practice for Persons with Severe Disabilities, Volume 27(2), pp. 112 – 124
Gunnar, M.R., & Vazquez, D. (2006). Stress neurobiology and developmental psychopathology. In D. Cicchetti & D. Cohen, (Eds.), Developmental psychopathology, volume 2: Developmental neuroscience (2nd edition). New York: John Wiley & Sons, Inc
Gunnar, M.R., & Quevedo, K. (2007). The Neurobiology of Stress and Development. Annual Review of Psychology. Volume 58. pp. 145 - 173
Gunsett, R.P., Mulick, J.A., Fernald, W.B., & Martin, J.L. (1989). Brief report: Indications for medical screening prior to behavioral programming for severely and profoundly mentally retarded clients. Journal of Autism and Developmental Disorders, Volume 19, pp. 167 - 172
Gupta, S.K., & Ratnam, B.V. (2009). Cerebral Perfusion Abnormalities in Children with Autism and Mental Retardation: A Segmental Quantitative SPECT Study. Indian Pediatrics. Volume 46. pp. 161 -164
Gutowski, S.J. (1996). Response acquisition for music or beverages in adults with profound multiple handicap. Journal of Developmental and Physical Disabilities. Volume 8(3), pp. 221 – 231
Hackett, S.S., & Critchley, S. (2012). From art therapy to arts in health: Bridging the gap for people with learning disabilities. Newsbriefing, November, pp. 12 – 13.
Hackett, S., Rothwell, K., Lyle, C., Bourne, J., Downing, L., & Morison, C.J. (2016). Art, drama and music therapies, In - Nigel Beail, (Ed.), Psychological therapies and people who have intellectual disabilities, Chapter 10, pp. 93 -98. Commissioning Team for the Faculties for Intellectual Disabilities of the Royal College of Psychiatrists and the Division of Clinical Psychology of the British Psychological Society
Hagopian, L.P., Long, E.S., & Rush, K.S. (2004). Preference assessment procedures for individuals with developmental disabilities. Behavior Modification, Volume 28(5), pp. 668 – 677
Haith, M.M. (1972). The forgotten message of the infant smile. Merrill-Palmer Quarterly, Volume 18, pp. 321 - 322
Hall, S., Oliver, C., & Murphy, G. (2001). The early development of self-injurious behaviour: An empirical study. Americal Journal on Mental Retardation, Volume 106, pp.189 - 199
Halle, J.W., & Spradlin, J.E. (1993). Identifying stimulus control of challenging behavior. In J. Reichle & D.P. Wacker (Eds.), Communicative
alternatives to challenging behavior: Integrating functional assessment and intervention strategies, pp. 83–109. Baltimore: Paul H. Brookes.
Hamilton, M.T., Hamilton, D.G., & Zderic, T.W. (2007). Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes, Volume 56, pp. 2655 – 2667
Hamlin, J.K., Wynn, K., & Bloom, P. (2007). Social evaluation by preverbal infants. Nature, Volume 450(7169), pp. 557 - 559
Happe, F.G., Brownell, H., Winner, E. (1999). Acquired "theory of mind" impairments following stroke. Cognition, Volume 70, pp. 211 - 240
Haring, N., Liberty, K., & White, O. (1981). An Investigation of Phases of Learning and Facilitating Instructional Events for the Severely/Profoundly Handicapped (final project report). Seattle: University of Washington College of Education.
Harlow, H.F. (1959). The development of learning in the rhesus monkey. American Scientist.
Harlow, H.F. (1964). Early social deprivation and later behavior in the monkey. In - Abrams, A., Gurner, H.H., & Tomal, J.E.P. (Eds.), Unfinished tasks in the behavioral sciences, pp.154 - 173, Baltimore: Williams & Wilkins
Harlow, H.F., Dodsworth, R.O., & Harlow, M.K. (1965). Total social isolation in monkeys. Proceedings of the National Academy of Sciences, Volume 54(1), pp. 90 - 97
Harlow, H.F., & Harlow, M.K. (1969). Effects of various mother-infant relationships on rhesus monkey behaviors. Determinants of Infant Behavior, Volume 4, pp. 15 - 36
Harlow, H.F., Harlow, M.K., & Suomi, S.J. (1971). From thought to therapy: lessons from a primate laboratory. American Scientist. Volume 59(5), pp. 538 – 549
Harlow, H.F., & Suomi, S.J. (1971). Social recovery by isolation-reared monkeys. Proceedings of the National Academy of Sciences, Volume 68(7), pp. 1534 - 1538
Harlow, H.F., & Suomi, S.J. (1974). Induced depression in monkeys. Behavioral Biology, Volume 12(3), pp. 273 - 296
Harris, C., & Card, B. (2012). A pilot study to evaluate nutritional influences on gastrointestinal symptoms and behavior patterns in children with Autism Spectrum Disorder. Complementary Therapies in Medicine, Volume 20(6), pp. 437 - 440
Harris, J., Cook, M., & Upton, G. (1996). Pupils with Severe Learning Difficulties who Present Challenging Behaviour: a whole school approach to assessment and intervention. Kidderminster: BILD.
Harris, L.P. (1977). Self-recognition among institutionalized profoundly retarded males: A replication. Bulletin of the Psychonomic Society, Volume 9, pp. 43 - 44
Harris, P. (1993). The nature and extent of aggressive behaviour among people with learning difficulties (mental handicap) in a single health district. Journal of Intellectual Disability Research. Volume 37, pp. 221 - 242
Harris, S.L., & Wolchik, S.A. (1979). Suppression of self stimulation: Three alternative strategies. Journal of Applied Behavior Analysis, Volume 12, pp. 185 – 198
Hart, J., Bock, K.A., Cartaxo, A., Converse, J., & Ferro, P. (2015). Round table Discussion: The impact of GI and nutritional issues on autism. Alternative and Complementary Therapies, Volume 21(2), pp. 84 - 89
Hart, P. (2006). Using imitation with congenitally deafblind adults: Establishing meaningful communication partnerships. Infant and Child Development, Volume 15, pp. 263 - 274
Harter, S. (1990). Self and identity development. In S. Feldman & G. Elliott (Eds.), At the threshold: The developing adolescent (pp. 352 –387). Cambridge: Harvard University Press.
Hassiotis, A.A. & Hall, I. (2008). Behavioural and cognitive behavioural interventions for outwardly directed aggressive behaviour in people with learning disabilities. Cochrane Database of Systematic Reviews (3), Art. No. CD003406.
Hastings, R.P.,& Remington, P.B. (1994). Staff behaviour and its implications for people with learning disabilities and challenging behaviours, British Journal of Clinical Psychology, Volume 33(4), pp. 423 – 438
Hastings, R.P., Remington, P.B., & Hopper, G.M. (1995). Experienced and inexperienced health care workers’ beliefs about challenging behaviours. Journal of Intellectual Disability Research, Volume 39(6), pp. 474 – 483
Hastings, R.P. (1997). Measuring staff perceptions of challenging behaviour: The Challenging Behaviour Attributions Scale (CHABA),
Journal of Intellectual Disability Research, Volume 41(6), pp. 495 – 501
Hastings, R.P. (2002). Do challenging behaviors affect staff psychological well-being? Issues of causality and mechanism. American Journal on Mental Retardation, Volume 107(6), pp. 455 – 467
Hastings, R.P., & Brown, T. (2002) Behavioural knowledge, causal beliefs and self-efficacy as predictors of special educator’s emotional reactions to challenging behaviour. Research in Developmental Disabilities. Volume 24, pp. 323 – 332
Hastings, R.P. (2005). Staff in special education settings and behaviour problems: Toward a framework for research and practice.
Educational Psychology, Volume 25(2/3), pp. 207 – 221
Hatch-Rasmussen, C. (1995). Sensory integration. Center for the Study of Autism at www. autism. org/si. html.
Hatton, C., Brown, R., Caine, A., & Emerson, E. (1995) Stressors, coping strategies and stress-related outcomes among direct care staff in staffed houses for people with learning disabilities. Mental Handicap Research, Volume 8(4), pp. 252 - 271
Hatton, C., Emerson, E., Robertson, J., Henderson, D., & Cooper, J. (1996). Factors associated with staff support and resident lifestyle in services for people with multiple disabilities: a path analytic approach. Journal of Intellectual Disability Research, Volume 40(5), pp. 466 - 477
Hatton, C., Emerson, E., Rivers, M., Mason, H., Swarbrick, R., Mason, L., Kiernan, C., Reeves, D., & Alborz, A. (2001). Factors associated with intended staff turnover and job search behaviour in services for people with intellectual disability. Journal of Intellectual Disability Research, Volume 45(3), pp. 258 - 270
Hatton, C. (2004). Choice. In E. Emerson, C. Hatton, T. Thompson, & T.R. Parmenter (Eds.), The international handbook of applied research in intellectual disabilities (pp. 335 – 351). Chichester: John Wiley & Sons
Hayashida, N., Hiramatsu, K., Katayama, S., Koga, M., Kudo, T., Mori, S., Orita, M., Shinkawa, T., Takamura, N., & Togo, M. (2012). Monitoring the autonomic nervous activity as the objective evaluation of music therapy for severely and multiply disabled children. The Tohoku Journal of Experimental Medicine, Volume 227(3), pp. 185 - 189
Hayes, T. (2016). Music Therapy in the Context of the Special School. In - J. Edwards (Ed.), Oxford Handbook of Music Therapy, pp. 176 - 185. Oxford: Oxford University Press
Healy, D., & Noonan Walsh, P. (2007). Communication among nurses and adults with severe and profound intellectual disabilities: predicted and observed strategies. Journal of Intellectual Disabilities, Volume 11(2), pp. 127 - 141
Healy, J. (1994). Your Child's growing Mind: A Practical Guide ot Brain Development from Birth to Adolescence. New York: Doubleday
Heath, G.W., & Fenten, P.H. (1997). Physical activity among persons with disabilities – a public health perspective. Exercise and Sports Science Reviews. Volume 25, pp. 195 – 234
Heaton, P., & Wallace, G.L. (2004). Annotation: The savant syndrome. Journal of Child Psychology and Psychiatry, Volume 45(5), pp. 899 - 911
Heimlich, K. (2001). Animal-assisted therapy and the severely disabled child: A quantitative study. Journal of Rehabilitation. Volume 67(4). pp. 48 - 54
Heller, S. (2004). Too Loud Too Bright Too Fast Too Tight: What to Do If You are Sensory Defensive in an Overstimulating World. Harper Collins: Reprint edition
Heller, S. (2015). Uptight & Off Center: How Sensory Processing Disorder Throws Adults Off Balance & How to Create Stability. Symmetry
Heller, T., Miller, A.B., & Factor, A. (1999). Autonomy in residential facilities and community functioning of adults with mental retardation. Mental Retardation, Volume 37(6), pp. 449 - 457
Helm, D.T. (2000). The measurement of happiness. The American Journal on Mental Retardation, Volume 105(5), pp. 326 – 335
Hemmings, C.P., Gravestock, S., Pickard, M., & Bouras, N. (2006). Psychiatric symptoms and problem behaviours in people with intellectual disabilities. Journal of Intellectual Disability Research, Volume 50, pp. 269 - 276
Henderson, E. (2005). Journeys Toward Communication. PMLD Link. Volume 17(1), Issue 50, pp. 19 - 21
Henry, D.B., Duvdevany, I., Keys, C.B., & Balcazar, F.E. (2004). Attitudes of American and Israeli staff toward people with intellectual disabilities. Mental Retardation, Volume 42(1), pp. 26 - 36
Herbert, M.R., & Buckley, J.A. (2013). Autism and dietary therapy: case report and review of the literature. Journal of Child Neurology, Volume 28(8), pp. 975 - 982
Hermelin, B., O’Connor, N., & Lee, S. (1987). Musical inventiveness of five idiot-savants. Psychological Medicine, Volume17(3), pp. 695 - 694
Hermelin, B., & O’Connor N. (1991). Talents and preoccupations in idiot-savants. Psychological Medicine, Volume 21(4), pp. 959 - 964
Herzog, H. (2011). The impact of pets on human health and psychological well-being: fact, fiction or hypothesis? Current Directions in Psychological Science. Volume 20(4), pp. 236 - 239
Hewett, D. (2006). The most important and complicated learning: that’s what play is for! ICAN Talking Point, March. www.talkingpoint.org.uk
Hewett, D. (2007). Do touch: physical contact and people who have severe, profound and multiple learning difficulties, Support for Learning, Volume 22 (3), pp.116 -123
Hewett, D. & Nind, M. (1988). Developing an Interactive Curriculum for Pupils with Severe and Complex Learning Difficulties, in Smith, B. (Ed), Interactive Approaches to the Education of Children with Severe Learning Difficulties. Birmingham: Westhill College.
Hewett, D. (1989). The Most Severe Learning Difficulties: Does Your Curriculum Go Back Far Enough?’ in Ainscow, M. (Ed), Special Education in Change. London: David Fulton.
Hewett, D., & Nind, M. (1989). Interaction as Curriculum at Harperbury School, PMLD Link 5.
Hewett, D., & Nind, M. (1989). Developing an interactive curriculum for pupils with severe and complex learning difficulties: a classroom process. In Interactive approaches to the education of children with severe learning difficulties. Smith, B. (Ed.). Birmingham: Westhill College
Hewett, D., & Nind, M. (1992). Returning to the Basics: A Curriculum at Harperbury Hospital School’, in: Booth, T., Swann, W., Masterton, M., & Potts, P. (Eds.), Curricula for Diversity in Education. London: Open University Press/Routledge
Hewett, D., & Nind, M. (1993). Access to Communication. Intensive Interaction: an approach to helping learners who are still in the pre-speech stages of communication learning, Information Exchange 37, May 1993.
Hewett, D. (1994). Understanding and writing a methodology of Intensive Interaction – teaching pre-speech communication abilities to learners with severe learning difficulties: a naturalistic inquiry using qualitative evaluation methods. Ph.D Thesis, Cambridge Institute of Education.
Hewett, D. (1996). How to do Intensive Interaction, in Collis, M. & Lacey, P. 1996 (eds) Interactive Approaches to Teaching: A Framework for INSET, London: David Fulton.
Hewett, D. & Nind, M. (2003). Severe Learning Difficulties: Intensive Interaction, Five to Eleven, Volume 2(10) pp.30 - 32
Hewett, D. (2007): Do touch: physical contact and people who have severe, profound and multiple learning difficulties. Support for Learning, Volume 22 (3), pp. 116 - 123
Higgins, E.T. (1987). Self-Discrepancy: A Theory Relating Self and Affect. Psychological Review. Volume 94(3), pp. 319 - 340
Hile, M.G., & Walbran, B.B. (1991). Observing staff-resident interactions: What staff do, what residents receive. Mental Retardation, Volume 29(1), pp. 35 - 41
Hilgenkamp, T.I.M., Reis, D., van Wijck, R., & Evenhuis, H.M. (2012). Physical activity levels in older adults with intellectual disabilities are extremely low. Research in Developmental Disabilities, Volume 33(2), pp. 477 – 483
Hill, B.K., & Bruininks, R.H. (1984). Maladaptive behavior of mentally retarded individuals in residential facilities. American Journal of Mental Deficiency, Volume 88, pp. 380 - 387
Hill, J., Brantner, J., & Spreat, S. (1989). The effect of contingent music on the in-seat behavior of a blind young woman with profound mental retardation. Education and Treatment of Children, Volume 12(2), pp. 165 - 173
Hill, S.D., & Tomlin, C. (1981). Self-recognition in retarded children. Child Development, Volume 52, pp. 145 - 150
Hillery, J. & Mulcahy, M. (1997). Self-injurious behaviour in persons with a mental handicap: an epidemiological study in an Irish population. Irish Journal of Psychological Medicine, Volume 14, pp. 12 - 15
Hirabuki, N., Fujita, N., Fujii, K., Hashimoto, T., & Kozuka, T. (1994). MR appearance of Virchow-Robin spaces along lenticulostriate arteries: spin-echo and two-dimensional fast low-angle shot imaging. American Journal of Neuroradiology, Volume 15(2), pp. 277 - 281
Hirama, H. (1989). Self-injurious behavior: A somatosensory treatment approach. Bethesda, MD: Chess Publications.
Hirstwood, R. (1998). Communication in multi-sensory rooms. Focus, Volume 23, pp. 20 - 31
Hobbs, V., How, R., & Lloyd, J. (2006). An Alternative curriculum. Insight, Volume 6. pp. 31 - 33
Hobbs, V. (2009). Maximising the progress of learners with profound and multiple learning difficulties. The SLD Experience. Volume 55(1), pp. 10 - 16
Hobbs, V. (2012). Where are the pupils with profound and multiple learning difficulties? The SLD Experience. Volume 64(1), pp. 24 - 28
Hobbs, V. (2012). Assessing the achievements of learners with PMLD, Education Today, Volume 61(3)
Hobbs, V. (2014). What do practitioners believe are the elements, conditions, factors and considerations that contribute to the provision of an appropriate and relevant learning environment for pupils with Profound and Multiple Learning Difficulties? Unpublished report for Associateship, Institute of Education
Hodgson, C., & Berry, M. (Eds.)(2011). Adventure Education: An Introduction. Taylor & Francis
Hoefkens, A., & Allen, D. (1990). Evaluation of a special behaviour unit for people with mental handicaps and challenging behaviour. Journal of Mental Deficiency Research, Volume 34, pp. 213 - 228
Hoehn, T.P., & Baumeister, A.A. (1994). A critique of the application of sensory integration therapy to children with learning disabilities.
Journal of Learning Disabilities, Volume 27, pp. 338 - 350
Hoffman, M.B., & Rand, Y. (2014). Instrumental enrichment, an intervention program for structural cognitive modifiability: Theory and practice. Thinking and Learning Skills: Volume 1: Relating Instruction To Research, Volume 43.
Hoge, G., & Dattilo, J. (1995). Recreation participation patterns of adults with and without mental retardation. Education and Training in Mental Retardation and Developmental Disabilities, Volume 30(4), pp. 283 - 298
Hogg, J., & Sebba, J. (1986a). Profound Retardation and Multiple Impairment. Volume I, Croom Helm
Hogg, J., & Sebba, J. (1986b). Profound Retardation and Multiple Impairment. Volume II, Croom Helm
Hogg, J., Sebba, J., & Lambe, L. (1990). Profound Retardation and Multiple Impairment. Volume III, Medical and Physical care and Managment. Chapman and Hall: London
Hogg, J. (1992). The administration of psychotropic and anticonvulsant drugs to children with profound intellectual disability and multiple
impairments. Journal of Intellectual Disability Research, Volume 36(6), pp. 473 - 488
Hogg, J. (1995). The Ecology of Leisure Provision:Context and Engagement, in Hogg, J., & Cavet, J. (Eds.), Making Leisure Provision for People with Profound and Multiple Disabilities, Chapman & Hall
Hogg, J., & Cavet, J. (Eds.) (1995). Making Leisure Provision for People with Profound and Multiple Disabilities. London:Chapman & Hall
Hogg, J., Cavet, J., Lambe, L., & Smeddle, M. (2001). The use of 'Snoezelen' as multisensory stimulation with people with intellectual disabilities: a review of the research. Research in Developmental Disabilities, Volume 22(5), pp. 353 - 372
Hogg, J., Reeves, D., Roberts, J., & Mudford, O.C. (2001). Consistency, context and confidence in judgements of affective communication in adults with profound intellectual and multiple disabilities. Journal of Intellectual Disability Research, Volume 45(1), pp. 18 - 29
Holburn, S. (1997). A renaissance in residential behavior analysis? A historical perspective and a better way to help people with challenging behavior. The Behavior Analyst, Volume 20(2), pp. 61 - 85
Holburn, S., & Vietze, P. (Eds.). (2002). Person-centered planning: Research, practice, and future directions. Paul H Brookes Publishing Company.
Holburn, S., Nguyen, D., & Vietze, P.M. (2004). Computer‐assisted learning for adults with profound multiple disabilities. Behavioral Interventions, Volume 19(1), pp. 25 - 37
Holland, T., & Murphy, G. (1990). Behavioural and psychiatric disorder in adults with mild learning difficulties. International Review of Psychiatry, Volume 2, pp. 117 - 136
Holmes, J., Gathercole, S.E., & Dunning, D.L. (2009). Adaptive training leads to sustained enhancement of poor working memory in children. Developmental Science, Volume 12(4), pp. F1 - F7
Holmes, J., & Gathercole, S.E. (2014). Taking working memory training from the laboratory into schools. Educational Psychology, Volume 34(4), pp. 440 - 450
Hong, E. & Perkins, P.G. (1997). Children's Responses to Self-Concept Questionnaires Administered in Differential Contexts. Child Study Journal, Volume 27(2), pp. 111 - 127
Hooper, J, & Lindsay, B. (1990). Music and the Mentally Handicapped - the Effect of Music on Anxiety. Journal of British Music Therapy, Volume 4, pp. 19 - 26
Hooper, J., Lindsay, B., & Richardson, I. (1991). Recreation and music therapy: An experimental study. Journal of British Music Therapy, Volume 5(2), pp. 10-13
Hooper, J., & Lindsay, B. (1992). Improving the quality of life through music: A case study. Mental Handicap, Volume 20(1), pp. 27 - 30
Hooper, J., & Lindsay, B. (1997). The Use of the Somatron on the Treatment of Anxiety Problems with Clients who Have Learning Disabilities. In - C.D.T. Wigram (Ed.), Music, Vibration and Health. Cherry Hill, NJ: Jeffrey Books
Hooper, J. (2001). Overcoming the problems of deinstitutionalization: Using music activities to encourage interaction between four adults with a developmental disability. Music Therapy Perspectives, Volume 19(2), pp. 121 - 127
Hooper, J. (2002). Using music to develop peer interaction: An examination of the response of two subjects with a learning disability. British Journal of Learning Disabilities, Volume 30, pp. 166 – 170
Hooper, J., McManus, A., & McIntyre, A. (2004). Exploring the link between music therapy and sensory integration: An individual case study. British Journal of Music Therapy, Volume 18(1), pp. 15 - 23
Hooper, J., Wigram, T., Carson, D., & Lindsay, B. (2011). The practical implication of comparing how adults with and without intellectual disability respond to music. British Journal of Learning Disabilities, Volume 39(1), pp. 22 - 28
Hoppestad, B.S. (2007). Inadequacies in computer access using assistive technology devices in profoundly disabled individuals: An overview of the current literature. Disability and Rehabilitation: Assistive Technology, Volume 2(4), pp. 189 - 199
Horak, F.B., Shumway‐Cook, A., Crowe, T.K., & Black, F.O. (1988). Vestibular function and motor proficiency of children with impaired hearing, or with learning disability and motor impairments. Developmental Medicine & Child Neurology, Volume 30(1), pp. 64 - 79
Horner, R.D. (1980). The effects of an environmental “enrichment” program on the behaviour of institutionalized profoundly retarded children. Journal of Applied Behaviour Analysis, Volume 13, pp. 473 – 491
Horner, R.H., Day, H.M., Sprague, J.R., O'Brien, M., & Heathfield, L.T. (1991). Interspersed requests: A nonaversive procedure for decreasing aggression and self injury during instruction. Journal of Applied Behavior Analysis, Volume 24, pp. 265 - 278
Horner, R.H., & O'Neill, R. (1992). Oregon Community Support: A two year analysis of community support for 11 people with histories of severe problem behaviour. Paper presented at the Association for Behavior Analysis, 18th Annual Convention, 25-28 May, 1992, San Francisco.
Horner, R.H., Close, D.W., Fredericks, H.D.B., O'Neill, R.E., Albin, R.W., Sprague, J.R., Kennedy, C.H., Flannery, K.B., & Heathfield, L.T. (1996). Supported living for people with severe problem behaviors: A demonstration. In D. H. Lehr & F. Brown (Eds.), Persons with disabilities who challenge the system. Baltimore: Paul H Brookes.
Hostyn, I., & Maes, B. (2009). Interaction between persons with profound intellectual and multiple disabilities and their partners: A literature review. Journal of Intellectual and Developmental Disability, Volume 34(4), pp. 296 - 312
Hostyn, I., Daelman, M., Janssen, M.J., & Maes, B. (2010). Describing dialogue between persons with profound intellectual and multiple disabilities and direct support staff using the scale for dialogical meaning making. Journal of Intellectual Disability Research, Volume 54(8), pp. 679 - 690
Hostyn, I., Neerinckx, H., & Maes, B. (2011): Attentional processes in interactions between people with profound intellectual and multiple disabilities and direct support staff. Research in Developmental Disability. Volume 32 (2): pp. 491 - 503
Houghton, J., Bronicki, G.J.B., & Guess, D. (1987). Opportunities to express preferences and make choices among students with severe disabilities in classroom settings. Journal of The Association for Persons with Severe Handicaps, Volume 12(1), pp. 18 – 27
Houwen, S., van der Putten, A., & Vlaskamp, C. (2014). A systematic review of the effects of motor interventions to improve motor, cognitive, and/or social functioning in people with severe or profound intellectual disabilities. Research in Developmental Disabilities, Volume 35, pp. 2093 – 2116
Hove, O. (2004). Weight survey on adult persons with mental retardation living in the community. Research in Developmental Disabilities, 25(1), pp. 9 - 17
Howe, M.B., Brittain, L.A., & McCathren, R.B. (2004). Meeting the Sensory Needs of Young Children in Classrooms. Young Exceptional Children. Volume 8(1), pp. 11 - 19
Howlin, P., Goode, S., Hutton, J., & Rutter, M. (2009). Savant skills in autism: psychometric approaches and parental reports. Philosophical Transactions of the Royal Society of London B: Biological Sciences, Volume 364(1522), pp. 1359 - 1367
Hsu, C.L., Lin, C.Y., Chen, C.L., Wang, C.M., & Wong, M.K. (2009). The effects of a gluten and casein-free diet in children with autism: a case report. Chang Gung Medical Journal, Volume 32(4), pp. 459 - 465
Huff, D.M., & Harris, S.C. (1987). Using sensorimotor integrative treatment with mentally retarded adults. American Journal of Occupational Therapy, Volume 41, pp. 227 - 231
Hughes, C., Pitkin, S.E., & Lorden, S.W. (1998). Assessing preferences and choices of persons with severe and profound mental
retardation. Education and Training in Mental Retardation and Developmental Disabilities, Volume 33(4), pp. 299 - 316
Hughes, M.W., Schuster, J.W., Nelson, C.M. (1993). The acquisition of independent dressing skills by students with multiple disabilities. Journal of Developmental and Physical Disabilities, Volume 5(4), pp. 233 - 252
Hughes, R.N. (1996). Drugs which induce anxiety: caffeine. New Zealand Journal of Psychology. Volume 25(1), pp. 36 - 42
Hui-chuan, Chu (2002). Functional Analysis and Assessment-based Interventions for Aberrant Behavior of Children with Developmental Disabilities. Journal of National Taipei Teachers College. Volume 15, pp. 387 - 432
Hulme, C., & Mackenzie, S. (1992). Working Memory and Severe Learning Difficulties. Hove: Lawrence Erlbaum Associates
Hulsegge, J., & Verheul, A. (1987). Snoezelen, another world. A practical book of sensory experience environments for the mentally handicapped. Chesterfield: Rompa
Humphries, K., Traci, M.A., & Seekins, T. (2009). Nutrition and adults with intellectual or developmental disabilities: systematic literature review results. Intellectual and Developmental Disabilities, Volume 47(3), pp. 163 - 185
Humphries, T., Wright, M., McDougall, B., & Vertes, J. (1990). The efficacy of sensory integration therapy for children with learning
disability. Physical and Occupational Therapy in Pediatrics, Volume 10(3), pp.1 - 17
Humphries, T., Wright, M., Snider, L., & McDougall, B. (1992). A comparison of the effectiveness of sensory integrative therapy and
perceptual-motor training in treating children with learning disabilities. Developmental and Behavioral Pediatrics, Volume 13(I), pp. 31 - 40
Humphries, T.W., Snider, L., & McDougall, B. (1993). Clinical evaluation of the effectiveness of sensory integrative and perceptual
motor therapy in improving sensory integrative function in children with learning disabilities. Occupational Therapy Journal of Research, Volume 13, pp. 163 - 182
Humphreys, M., Churchill, R., & Kerr, E. (2014). The Multi-Sensory Project: Art for all the Senses. PMLD Link, Volume 26(3), Issue 79, pp. 2 - 4
Hurwitz, S. (2013). The gluten-free, casein-free diet and autism: limited return on family investment. Journal of Early Intervention, Volume 35(1), pp. 3 - 19
Hutchinson, L.M., Hastings, R.P., Hunt, P.H., Bowler, C.L., Banks, M.E., & Totsika, V. (2014). Who's Challenging Who? Changing attitudes towards those whose behaviour challenges. Journal of Intellectual Disability Research, Volume 58(2), pp. 99 - 109
Hydration For Health (2015). Hydration, mood state and cognitive function. Hydration For Health Initiative. Danone Nutricia Research
Hylkema, T., & Vlaskamp, C. (2009). Significant improvement in sleep in people with intellectual disabilities living in residential settings by
non-pharmaceutical interventions. Journal of Intellectual Disability Research, Volume 53(8), pp. 695 - 703
Hyman, P., Oliver, C., & Hall, S. (2002). Self-Injurious Behaviour, Self-Restraint, and Compulsive Behaviors in Cornelia de Lange Syndrome. American Journal on Mental Retardation, Volume 107(2), pp. 146 – 154
Hyman, S.L., Stewart, P.A., Smith, T., Foley, J., Cain, U., Peck, R., Morris, D.D., & Wang, H. (2010). The gluten free and casein free (GFCF) diet: A double blind, placebo controlled challenge study. Presented at International Meeting for Autism Research, Philadelphia, PA.
Hyman, S.L., Stewart, P.A., Foley, J., Cain, U., Peck, R., Morris, D.D., Wang, H., & Smith, T. (2016). The gluten-free/casein-free diet: a double-blind challenge trial in children with autism. Journal of Autism and Developmental Disorders, Volume 46(1), pp. 205 - 220
Imray, P. (2005). Moving towards simple, understandable and workable definitions of severe learning difficulties and profound and multiple learning difficulties. SLD Experience, Volume 42: pp. 33 - 37
Imray, P., & Hinchcliffe, V. (2012). Not fit for purpose: a call for separate and distinct pedagogies as part of a national framework for those with severe and profound learning difficulties, Support for Learning, Volume 27(4), pp. 150 - 157
Imray, P., & Hinchcliffe, V. (2013). Curricula for Teaching Children and Young People with Severe or Profound and Multiple Learning Difficulties. David Fulton / Nasen
Inal, S. (2014). Competitive dance for individuals with disabilities. PALAESTRA: Forum of Sport, Physical Education, and Recreation for Those with Disabilities, Volume 28(1), pp. 32 - 35
Ionatamishvili, N.I., Tsverava, D.M., Loriya, M.S., Sheshaberidze, E.G., & Rukhadze, M.M. (2004). Riding therapy as a method of rehabilitation of children with cerebral palsy. Human physiology, Volume 30(5), pp. 561 - 565
Intagliata, J., & Willer, B. (1982). Reinstitutionalization of mentally retarded persons successfully placed into family-care and group homes. American Journal of Mental Deficiency, Volume 87(1), pp. 34 - 39
Irvin, D.S. (2006). Using analog assessment procedures for determining the effects of a gluten‐free and casein‐free diet on rate of problem behaviors for an adolescent with autism. Behavioral Interventions, Volume 21(4), pp. 281 - 286
Irvine, C. (1998). Addressing the needs of adults with profound and multiple learning disabilities in social services provision, in Hewett, D and Nind, M. (Eds.), Interaction in Action. David Fulton. London
Irvine, C. (2001). On the floor and playing…, Royal College of Speech and Language Therapy Bulletin, November, pp. 9 - 11
Irvine, C. (2002). Preliminary findings of an informal longitudinal study into the research/practice interface: noting the influence of extra trees in the wood rather than throwing the baby out with the bathwater, Speech and Language Therapy in Practice
Isaacs, E., & Oates, J. (2008). Nutrition and cognition: assessing cognitive abilities in children and young people. European Journal of Nutrition. Volume 47(Supplement 3). pp. 4 – 24
Ivancic, M.T., & Bailey, J.S. (1996). Current limits to reinforcer identification for some persons with profound multiple disabilities. Research in Developmental Disabilities, Volume 17(1), pp. 77 - 92
Ivancic, M.T., Barrett, G.T., Simonow, A., & Kimberly, A. (1997). A replication to increase happiness indices among some people with profound multiple disabilities. Research in Developmental Disabilities, Volume 18(1), pp. 79 - 89
Iwasaki, K., & Holm, M.B. (1989). Sensory treatment for the reduction of stereotypic behaviors in persons with severe multiple disabilities. Occupational Therapy Journal of Research, Volume 9, pp. 170 – 183
Iwata, B.A., Dorsey, M.F., Slifer, K.J., Bauman, K.E., & Richman, G.S. (1982). Toward a functional analysis of self-injury. Analysis and Intervention in Developmental Disabilities, Volume 2, pp. 3 - 20
Iwata, B.A., Pace, G., Kalsher, M., Cowdery, G., & Cataldo, M. (1990). Experimental analysis and extinction of self-injurous escape behavior. Journal of Applied Behavior Analysis, Volume 23, pp. 11 - 27
Jacobson, J.W. (1982). Problem behaviour and psychiatric impairment within a developmentally disabled population I: behaviour frequency. Applied Research in Mental Retardation, Volume 3, pp. 121 - 139
Jackson, J. (2014). ‘Sit with me, talk to me’: How the use of multi-media advocacy supported a brighter future for a nineteen year old learner
coping with PMLD and presenting challenging verbal behaviour. PMLD Link. Volume 26(3), Issue 79, pp. 39 - 44
Jackson, E., & Jackson, N. (1999). Helping people with a learning disability explore choice. London: Jessica Kingsley Publishers
Jackson, N., & Jackson, E. (1998). Choice making for people with a learning disability. Learning Disability Practice; Volume 1(3), pp. 22 – 25
Jacobson, J.W., Foxx, R.M., & Mulick J.A. (2005). Controversial therapies for developmental disabilities. Fad, fashion, and science in professional practice. Mahwah, New Jersey: Lawrence Erlbaum Associates, Publishers
Jambaqué, I., Hertz-Pannier, L., Mikaeloff, Y., Martins, S., Peudenier, S., Dulac, O., & Chiron, C. (2003). Severe memory impairment in a child with bihippocampal injury after status epilepticus. Developmental Medicine and Child Neurology. Volume 48(3). pp 223 - 226
James, J. (1996a). Dramatherapy with people with learning disabilities. In - S. Mitchell (Ed.), Dramatherapy: Clinical Studies. Jessica Kingsley: London. pp. 15 - 32
James, J. (1996b). Poetry in motion: drama and movement therapy with people with learning disabilities. In - J. Pearson (Ed.), Discovering the Self through Drama and Movement. Jessica Kingsley: London. pp. 209 - 221
Janicki, M.P., & Dalton, A.J. (1998). Sensory impairments among older adults with intellectual disability. Journal of Intellectual and Developmental Disability, Volume 23(1), pp. 3 - 11
Jansen, D.E., Krol, B., Groothoff, J.W., & Post, D. (2004). People with intellectual disability and their health problems: a review of comparative studies. Journal of Intellectual Disability Research, Volume 48(2), pp. 93 - 102
Jansma, P., McCubbin, J., Combs, S., Decker, J., & Ersing, W. (1987). Fitness and hygiene programming for the severely handicapped: A curriculum-embedded assessment guide. Worthington, OH: Moody's.
Janssen, M.J., Riksen-Walraven, J.M., & van Dijk, J.P.M. (2006). Applying the diagnostic intervention model for fostering harmonious interactions between deaf-blind children and their educators: A case study. Journal of Visual Impairment & Blindness, Volume 100(2), pp. 91 - 105
Jeffree, D., & McConkey, R. (1976). Let me speak. London: Human Horizons Series: Souvenir Press
Jellison, J.A. (1979). The music therapist in the educational setting: Developing and implementing curriculum for the handicapped. Journal of Music Therapy, Volume 16(3), pp. 126 - 137
Jenkins, J.R., Fewell, R., & Harris, S.R. (1983). Comparison of sensory integrative therapy and motor programming. American Journal
of Mental Deficiency, Volume 88, pp. 221 - 224
Jenkins, R., Rose, J., & Lovell, C. (1995). Psychological well-being of staff working with people who have challenging behaviour. Journal of Intellectual Disability Research, Volume 41, pp. 502 - 511
Jenson, C.C., Watson, L.S., DeWulf, M., Johnson, S.P., Davis, N.S., & Sottolano, D.C. (1992). Normalization of mealtime for persons with developmental disabilities: Implementation by professional and direct-care staff. Behavioral Residential Treatment, Volume 7, pp. 355 - 371
Jobling, A. (2001). Beyond sex and cooking: Health education for individuals with intellectual disability. Mental Retardation, Volume 39(4), pp. 310 - 321
Jobling, A., Virji-Babul, N., & Nichols, D. (2006). Children with Down Syndrome: Discovering the Joy of Movement. Journal of Physical Education, Recreation and Dance. Volume 77(6), pp. 34 - 38
Jockers, D. (2012). Is your brain getting enough of this nutrient? Natural News.com
Johnson, C.R., Handen, B.L., Zimmer, M., Sacco, K., & Turner, K. (2011). Effects of gluten free/casein free diet in young children with autism: a pilot study. Journal of Developmental and Physical Disabilities, Volume 23(3), pp. 213 - 225
Johnson, C.R., Turner, K., Stewart, P.A., Schmidt, B., Shui, A., Macklin, E., Reynolds, A., James, J., Johnson, S.L., Courtney, P.M., & Hyman, S.L. (2014). Relationships between feeding problems, behavioral characteristics and nutritional quality in children with ASD. Journal of Autism and Developmental Disorders, Volume 44(9), pp. 2175 - 2184
Johnson, H., Douglas, J., Bigby, C., & Iacono, T. (2012). Social Interaction with Adults with Severe Intellectual Disability: Having Fun and Hanging Out. Journal of Applied Research in Intellectual Disabilities, Volume 25(4), pp. 329 - 341
Johnson, R.K., Appel, L., Brands, M., Howard, B., Lefevre, M., Lustig, R., Sacks, F., Steffen, L., & Wyllie-Rosett, J. (2009). Dietary sugars intake and cardiovascular health: a scientific statement from the American Heart Association. Circulation, Volume 120(11), pp. 1011 - 1120
Johnson, W.L., & Day, R.M. (1992). The incidence and prevalence of self-injurious behavior. In J.K. Luiselli, J.L. Matson, & N.N. Singh (eds.), Self-Injurious Behavior: Analysis, Assessment and Treatment, pp. 21 -58. New York: Springer-verlag
Jones, A.P. (2016). String switch sessions. TalkSense Website (this webpage)
Jones, C., & Hastings, R.P. (2003). Staff reactions to self-injurious behaviours in learning disability services: Attributions, emotional responses and helping. British Journal of Clinical Psychology, Volume 42(2), pp. 189 – 203
Jones, E., Perry, J., Lowe, K., Felce, D., Toogood, S., Dunstan, F., Allen, D., & Pagler, J. (1999). Opportunity and the promotion of activity among adults with severe intellectual disability living in community residences: the impact of training staff in active support. Journal of Intellectual Disability Research, Volume 43(3), pp. 164 - 178
Jones, E., Perry, J., Lowe, K., Allen, D., Toogood, S., & Felce, D. (2009). Active Support: A handbook for supporting people with
learning disabilities to lead full lives. Welsh Centre for Learning Disabilities Applied Research Unit. University of Wales, Cardiff
Jones, F., Pring, T., & Grove, N. (2002). Developing communication in adults with profound and multiple learning difficulties using objects of reference. International Journal of Language and Communication Disorders, Volume 37(2), pp. 173 - 184
Jones, M.C., Walley, R.M., Leech, A., Paterson, M., Common, S., & Metcalf, C. (2007). Behavioral and psychosocial outcomes of a 16-week rebound therapy-based exercise program for people with profound intellectual disabilities. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(2), pp. 111 – 119
Jones, O., O’Neil, N., Pavlicevic, M., Powell, H., & Sampathianaki, E. (2014). Making music, making friends: Long-term music therapy with young adults with severe learning disabilities. Journal of Intellectual Disabilities, Volume 18(1), pp. 5 - 19
Jones, P. (2004). 'They are not like us and neither should they be': issues of teacher identity for teachers of pupils with profound and multiple learning difficulties. Disability and Society, Volume 19(2), pp. 159 - 169.
Jones, P. (2005). Teachers' views of their pupils with profound and multiple learning difficulties. European Journal of Special Needs Education, Volume 20(4), pp. 375 - 385
Jones, R. & Williams, H. (1998). Reducing Stereotyped Behaviour: an experimental analysis of Intensive Interaction, International Journal of Practical Approaches to Disability, Volume 22 (2/3), pp. 21 - 25
Jones, R.S.P., & Eayrs, C.B. (1993). Challenging Behaviour and Intellectual Disability: A Psychological Perspective. BILD
Jones, S., Cooper, S.A., Smiley, E., Allan, L., Williamson, A., & Morrison, J. (2008). Prevalence of, and factors associated with, problem behaviors in adults with intellectual disabilities. The Journal of Nervous and Mental Disease. Volume 196, pp. 678 – 686
Joseph, D. (1986). The morning. Communication Outlook. Volume 8(2), pp. 8
Kahn, J.V. (1978). Applications of the Piagetian literature to severely and profoundly retarded persons. Mental Retardation, Volume 17, pp. 273 - 280
Kahng, S., Boscoe, J.H., & Byrne, S. (2003). The use of an escape contingency and a token economy to increase food acceptance. Journal of Applied Behavior Analysis, Volume 36(3), pp. 349 - 353
Kapell, D., Nightingale, B., Rodriguez, A., Lee, J.H., Zigman, W.B., & Schupf, N. (1998). Prevalence of chronic medical conditions in adults with mental retardation: Comparison with the general population. Mental Retardation, Volume 36(4), pp. 269 - 279
Kaplan, H., Clopton, M., Kaplan, M., Messbauer, L., & McPherson, K. (2006). Snoezelen multi-sensory environments: Task engagement and generalization. Research in Developmental Disabilities, Volume 27(4), pp. 443 - 455
Karkou, V., & Sanderson, P. (1997). Dance Movement Therapy Approaches and Particular References to Children with Special Needs, in E. Antilla (ed.) The Seventh Conference of Dance and the Child International (daCI): The Call of Forests and Lakes. Proceedings, pp. 159 – 166. Kuopio, Finland: Dance and the Child International.
Karlan, G.R. (1980). The effects of preference for objects and repeated measure upon the assessed level of object permanence in severely handicapped students. Journal of the Association for the Severely Handicapped, Volume 5, pp. 174 - 193
Kastner, T., Walsh, K.K., & Fraser, M. (2001). Undiagnosed medical conditions and medication side effects presenting as behavioral/psychiatric problems in people with mental retardation. Mental Health Aspects of Developmental Disabilities. Volume 4, pp. 101 – 107
Katcher, A.H. (1977). Physiologic and behavioural responses to companion animals. Psychosomatic Medicine. Volume 39(3), pp.188 - 192
Kaufman, J.C., & Sternberg, R.J. (Eds.). (2010). The Cambridge handbook of creativity. Cambridge University Press.
Kaufman, J.C. (2016). Creativity 101. Springer Publishing
Kearney, C.A., & McKnight, T.J. (1997). Preference, choice and persons with disabilities: a synopsis of assessments, interventions and future directions. Clinical Psychology Review, Volume 17, pp. 217 – 238
Kearney, C.A., Bergan, K.P., & McKnight, T.J. (1998). Choice availability and persons with mental retardation: A longitudinal and regression analysis. Journal of Developmental and Physical Disabilities, Volume 10(3), pp. 291 - 305
Kellett, M. (2000). Sam’s story: evaluating Intensive interaction in terms of its effect on the social and communicative ability of a young child with severe learning difficulties, Support for Learning, Volume 15 (4), pp.165 - 171
Kellett, M. (2001). Implementing Intensive Interaction: an evaluation of the efficacy of Intensive Interaction in promoting sociability and communication in young children who have severe learning difficulties and of factors affecting its implementation in community schools. Ph.D Thesis, Oxford Brookes University.
Kellet, M., & Nind, M. (2002). Responding to individuals with severe learning difficulties and stereotyped behaviour. European Journal of
Special Needs Education, Volume 17(3),pp. 265 – 282
Kellett, M. (2003). Jacob’s Journey: developing sociability and communication in a young boy with severe and complex learning difficulties using the Intensive interaction teaching approach, Journal of Research in Special Educational Needs, March.
Kellet, M., & Nind, M. (2003). Implementing Intensive Interaction in Schools. London: David Fulton Publishers.
Kellett M. (2004). Intensive Interaction in the inclusive classroom: using interactive pedagogy to connect with students who are hardest to reach, Westminster Studies in Education, Volume 27, pp.175 – 188
Kellett, M. (2005). Catherine’s Legacy: social communication development for individuals with profound learning difficulties and fragile life expectancies, British Journal of Special Education, Volume 32 (3), pp.116 - 121
Kelley, M.F., Sexton, D., Burdg, N.B., & Haynes, M.D. (1988). Assessment of Self-Recognition in Young Children with Handicaps. Assessment for Effective Intervention. Volume 13(2-4), pp. 86 - 97
Kelly, L.E., Rimmer, J.H., & Ness, R.A. (1986). Obesity levels in institutionalized mentally retarded adults. Adapted Physical Activity Quarterly, Volume 3(2), pp. 167 - 176
Kempermann, G., & Gage, F.H. (1999). New nerve cells for the adult brain. Scientific American, Volume 280(5), pp. 48 - 53
Kempton, M.J., Ettinger, U., Foster, R., Williams, S.C., Calvert, G.A., Hampshire, A., Zelaya, F.O., O’Gorman, R.L., McMorris, T., Owen, A.M., & Smith, M.S. (2011). Dehydration affects brain structure and function in healthy adolescents. Human Brain Mapping. Volume 32. pp. 71 - 79
Kennedy, A. (2001). Intensive Interaction, Learning Disability Practice, Volume 4(3), pp.14 - 15
Kennedy, C.H., & Haring, T.G. (1993). Teaching Choice Making During Social Interactions to Students with Profound Multiple Disabilities. Journal of Applied Behavior Analysis, Volume 26(1), pp. 63 - 76
Kennedy, C.H., & Itkonen, T. (1993). Effects of setting events on the problem behavior of students with severe disabilities. Journal of Applied Behavior Analysis, Volume 26, pp. 321 - 327
Kennedy, C.H., & Meyer, K.A. (1996). Sleep deprivation, allergy symptoms, and negatively reinforced problem behaviour. Journal of Applied Behavior Analysis. Volume 29, pp. 133 – 135
Kennedy, H. (2011). What is video interactive guidance (V.I.G.). In H. Kennedy, M. Landor & L. Todd (Eds), Video Interactive Guidance: A
Relationship-Based Intervention to Promote Attunement, Empathy and Wellbeing. London: Jessica Kingsley.
Kennedy, H., Landor, M., & Todd. L. (2011). Video Interactive Guidance: A Relationship-Based Intervention to Promote Attunement, Empathy and Wellbeing. London: Jessica Kingsley.
Kennedy, M., McCombie, L., Dawes, P., McConnell, K.N., & Dunnigan, M.G. (1997). Nutritional support for patients with intellectual disability and nutrition/dysphagia disorders in community care. Journal of Intellectual Disability Research, Volume 41(5), pp. 430 - 436
Kenny, C.B. (1982). The Mythic Artery: The Magic of Music Therapy, Atascadero, California: Ridgeview Publishing Company.
Kerdegari, H., Kim, Y., & Prescott, T.J. (2016). Head-mounted sensory augmentation device: designing a tactile language, IEEE transactions on haptics, Volume 9 (3), pp. 376 - 386
Kern, L., Koegel, R.L., Dyer, K., Blew, P.A., & Fenton, L.R. (1982). The effects of physical exercise on self stimulation and appropriate responding in autistic children. Journal of Autism and Developmental Disorders, Volume 12, pp. 399 - 419
Kern, P., Wolery, M., & Aldridge, D. (2007). Use of songs to promote independence in morning greeting routines for young children with autism. Journal of Autism & Developmental Disorders, Volume 37(7), pp. 1264 - 1271
Kiernan, C. (1991). Professional ethics: Behaviour analysis and normalisation. In B. Remington (Ed.), The Challenge of Severe Mental Handicap: A Behaviour Analytic Approach. John Wiley and Sons, Chichester, pp. 369 - 392
Kiernan, C. (1993). Future directions. In S. Jones & C. Eayres (Eds), Challenging Behaviour and Intellectual Disability: a psychological perspective. Kidderminster: BILD.
Kiernan, C., & Qureshi, H. (1993). Challenging behaviour. In C. Kiernan (Ed.), Research to Practice? Implications of Research on the Challenging Behaviour of People with Learning Disabilities. pp. 53 - 87. Kidderminster: British Institute of Learning Disabilities Publications.
Kiernan, C., & Kiernan, D. (1994). Challenging behaviour in schools for pupils with severe learning difficulties. Mental Handicap Research, Volume 7, pp. 117 - 201
Kiernan, C., Reeves, D., & Alborz, A. (1995). The use of anti-psychotic drugs with adults with learning disabilities and challenging behaviour. Journal of Intellectual Disability Research, Volume 39, pp. 263 - 274
Kiernan, C., & Alborz, A. (1996). Persistence and change in challenging and problem behaviours of young adults with intellectual disability living in the family home. Journal of Applied Research in Intellectual Disabilities, Volume 3, pp. 181 - 193
Kimball, J.G. (1988). The emphasis is on integration, not sensory. American Journal of Mental Retardation, Volume 92, pp. 423 - 424
King, B. (2007). Psychopharmacology in intellectual disabilities. In Bouras, N. & Holt, G. (Eds.) Psychiatric and Behavioural Disorders in Intellectual and Developmental Disabilities. Cambridge: Cambridge University Press.
King, G.A., Shultz, I.Z., Steel, K., Gilpin, M., & Cathers, T. (1993). Self-evaluation and self-concept of adolescents with physical disabilities, American Journal of Occupational Therapy, Volume 47(2), pp. 132 - 140
Kingsley, J. (2009). First steps in intervention with your child with autism: Framework for communication. Philadelphia, PA. Jessica Kingsley
Kinnealey M. (1973). Aversive and non-aversive responses to sensory stimulation in mentally retarded children. American Journal of Occupational Therapy, Volume 27, pp. 464 – 471
Kinnealey, M. (1976). Aversive and non-aversive Responses to Sensory Stimulation in Mentally Retarded Children, In A.Price, E. Gilfoyle & C, Myers (Eds.) Research in Sensory Integrative Development (pp. 33 - 40). Rockville, MD: American Occupational Therapy Association
Kinnealey M., Oliver B., & Wilbarger P. (1995). A phenomenological study of sensory defensiveness in adults. American Journal of Occupational Therapy, Volume 49, pp. 444 – 451
Kinnealey, M., & Fuiek, M. (1999). The relationship between sensory defensiveness, anxiety, depression, and perception of pain in adults.
Occupational Therapy International, Volume 6, pp. 195 - 206
Kishi, G., Teelucksingh, B., Zollers, N., Park-Lee, S., & Meyer, L. (1988). Daily decision-making in community residences: A social comparison of adults with and without mental retardation. American Journal on Mental Retardation, Volume 92, pp. 430 - 435
Kitch, R. (1995). Creating success in the land of Oz and earthquakes. 3rd Annual Pittsburgh Employment Conference Proceedings. pp. 3 - 8
Kivitie-Kallio, S., Autti, T., Salonen, O., & Norio, R. (1998). MRI of the brain in the Cohen syndrome: a relatively large corpus callosum in patients with mental retardation and microcephaly. Neuropediatrics, Volume 29(06), pp. 298 - 301
Kjos, B.O., Umansky, R., & Barkovich, A.J. (1990). Brain MR imaging in children with developmental retardation of unknown cause: results in 76 cases. American Journal of Neuroradiology, Volume 11(5), pp. 1035 - 1040
Kleim, J.A. & Jones, T.A. (2008). Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. Supplement: Journal of Speech, Language, and Hearing Research, Volume 51(1), S225 - S239
Knight, C. (1991). Developing Communication through Interaction, in Watson, J. (ed) Innovatory Practice and Severe Learning Difficulties. Edinburgh: Moray House.
Knight, C. (1992). Speech therapy on the run: Creating opportunities for effective communication. Eye Contact. Volume 3. Royal National Institute for the Blind
Knill, C. (1983) Body awareness, communication and development: a programme employing music with the profoundly handicapped. International Journal of Rehabilitation Research, Volume 6(4), pp. 489 - 492
Kobe, F.H., Mulick, J.A., Rash, T.A., & Martin, J. (1994). Non-ambulatory persons with profound mental retardation: physical, developmental, and behavioural characteristics. Research in Developmental Disabilities. Volume 15, pp. 413 – 423
Koller, H., Richardson, S.A., Katz, M., & McLaren, J. (1982). Behaviour disturbance in childhood and the early adults years in populations who were and were not mentally retarded. Journal of Preventive Psychiatry, Volume 1, pp. 453 - 468
Konarski, E.A., Sutton, K., & Huffman, A. (1997). Personal characteristics asociated with episodes of injury in a residential facilty. American Journal of Mental Retardation. Volume 102, pp. 37 - 44
Konrad, M., Fowler, C.H., Walker, A.R., Test, D.W., & Wood, W.M. (2007). Effects of self-determination interventions on the academic skills of students with learning disabilities. Learning Disabilities Quarterly, Volume 30, pp. 89 – 113
Koomar, J., Kranowitz, C., Szklut, S., & Balzer-Martin, L. (2001). Answers to Questions Teachers Ask About Sensory Integration: Forms, Checklists, and Practical Tools. Future Horizons
Koski, K., Martikainen, K., Burakoff, K., & Launonen, K. (2010). Staff members' understandings about communication with individuals who have multiple learning disabilities: A case of Finnish OIVA communication training. Journal of Intellectual and Developmental Disability, Volume 35(4), pp. 279 - 289
Koski, K. (2014). Indirect Speech and Language Therapy for Individuals with Profound and Multiple Learning Disabilities: An Ecological Perspective. The Finnish Association on Intellectual and Developmental Disabilities
Koziol, L.F. & Ely Budding, D., & Chidekel, D. (2011). Sensory Integration, Sensory Processing, and Sensory Modulation Disorders: Putative Functional Neuroanatomic Underpinnings. Cerebellum, Volume 10. pp. 770 – 792
Kozma, A., Mansell, J., & Beadle-Brown, J. (2009). Outcomes in different residential settings for people with intellectual disability: a systematic review. American Journal on Intellectual and Developmental Disabilities, Volume 114(3), pp. 193 - 222
Kranowitz, C.S. (1998). The Out-of-Sync Child: Recognizing and Coping with Sensory Integration Dysfunction. New York: Perigee
Kranowitz, C.S., Szklut, S., Balzer-Martin, L., Haber, E., & Sava, D.I. (2002). Answers to questions teachers ask about sensory integration. Las Vegas, NM: Sensory Resources.
Kranowitz, C.S. (2003). The out-of-sync child has fun. New York: Berkley Publishing.
Kranowitz, C.S. (2005). The Out of Sync Child: Recognizing and Coping with Sensory Processing Disorder. New York: Perigee.
Krech, D., Rosenzweig, M.R., & Bennett, E.L. (1960). Effects of environmental complexity and training on brain chemistry. Journal of Comparative Physiological Psychology. Volume 53. pp. 509 - 519
Kršková, L., Talarovièová, A., & Olexová, L. (2010). Guinea pigs-The “small great” therapist for autistic children, or: Do guinea pigs have positive effects on autistic child social behavior? Society & Animals, Volume 18, pp. 139 – 151
Kuder, S.J., & Bryen, D.N. (1993). Conversational topics of staff members and institutionalized individuals with mental retardation. Mental Retardation, volume 31(3), pp. 148 - 153
Kuder, S.J. (2003). Teaching students with language and communication difficulties. Boston, MA: Allyn and Bacon
Kuhn, H.G., Palmer, T.D., & Fuchs, E. (2001). Adult neurogenesis: a compensatory mechanism for neuronal damage. European Archives of Psychiatry and Clinical Neuroscience, Volume 251(4), pp. 152 - 158
Kurtz, P.F., Boetler, E.W., Jarmolowicz, D.P., Chin, M.D., & Hagopian, L.P. (2011). An analysis of functional communication training as an empirically supported treatment for problem behaviors displayed by individuals with intellectual disabilities. Research in Developmental Disabilities, Volume 32(6), pp. 2935 - 2942
Kyselo, M. (2014). The body social: an enactive approach to the self. Frontiers in Psychology, Volume 5, Article 986. pp. 1 - 16
Lacey, P. (1996). The inner life of children with profound and multiple learning difficulties. In - Varma, V. (ed), The Inner Life of Children with Special Needs. London: Whurr.
Lacey, P. (1998). Meeting complex needs through multidisciplinary teamwork. In P. Lacey & C. Ouvry (Eds), People with Profound and Multiple Learning Disabilities: A Collaborative Approach to Meeting Complex Needs. London: David Fulton
Lacey, P., & Ouvry, C. (1998). People with Profound & Multiple Learning Disabilities: Collaborative Approach to Meeting Complex Needs. David Fulton
Lacey, P., & Porter, J. (1998). Enabling Teachers: in-service education in learning difficulties and challenging behaviour, Journal of In-Service Education, Volume 24(3), pp. 475 - 491
Lacey, P. (2001). Music. In - Carpenter, B., Ashdown, R., & Bovair, K. (eds), Enabling Access: Effective Teaching and Learning for Pupils with Learning Difficulties. London: David Fulton. 2nd Edition
Lacey, P. (2001b). The role of learning support assistants in the inclusive learning of pupils with severe and profound learning difficulties. Educational Review, Volume 53(2), pp. 157 - 167
Lacey, P. (2007). Start Where The Learner Is: Coaching For a Better Quality Of Life. PMLD Link, Volume 19(2), Issue 57, pp. 10 - 16
Lacey, P., Layton, L., Miller, C., Goldbart, J., & Lawson, H. (2007) ‘Literacy for children with severe learning difficulties: exploring conventional and inclusive literacy. Journal of Research in Special Educational Needs. Volume 7(3), pp. 149 - 160
Lacey, P. (2009). Developing The Thinking of Learners With PMLD. PMLD Link. Volume 21(2), Issue 63, pp. 15 - 19
Lacey, P. (2010). SMART and SCRUFFY Targets, SLD Experience, Volume 57, pp. 16 - 21
Lacey, P. (2011). Listening to challenging behaviour. PMLD Link. Volume 23(1), Issue 68, pp. 7 - 9
Lacey, P. (2015). Developing The Thinking of Learners With PMLD. PMLD Link. Volume 27(2), Issue 81, pp. 43 - 47
Lacey, P. , Ashdown, R., Jones, P., Lawson, H., & Pipe, M. (Eds) (2015). The Routledge Companion to Severe, Profound and Multiple Learning Difficulties. Routledge
Lachapelle, Y., Wehmeyer, M.L., Haelewyck, M.C., Courbois, Y., Keith, K.D., Schalock, R., & Walsh, P.N. (2005). The relationship
between quality of life and self-determination: An international study. Journal of Intellectual Disability Research, Volume 49, pp. 740 – 744.
LaFay L. (1987). That smarts! Accident leaves man with unforgettable gift. Virgina Pilot. Volume 17, pp. 31 - 33
Lahtinen, U., Rintala, P., & Malin, A. (2007). Physical performance of individuals with intellectual disability: A 30-year follow-up. Adapted Physical Activity Quarterly, Volume 24, pp. 125 – 143
Lakin, K.C., Hill, B.K., Hauber, F.A., Bruininks, R.H. & Heal, L.W. (1983). New admissions and re-admissions to a national sample of public residental facilties. American Journal of Mental Deficiency, Volume 88, pp. 13 - 20
Lakin, K.C., & Stancliffe, R.J. (2007). Residential supports for persons with intellectual and developmental disabilities. Developmental Disabilities Research Reviews, Volume 13(2), pp. 151 - 159
Lakin, K.C., Doljanac, R., Byun, S.Y., Stancliffe, R.J., Taub, S., & Chiri, G. (2008). Factors associated with expenditures for Medicaid home and community based services (HCBS) and intermediate care facilities for persons with mental retardation (ICF/MR) services for persons with intellectual and developmental disabilities. Intellectual and Developmental Disabilities, Volume 46(3), pp. 200 - 214
Lakin, K.C., Doljanac, R., Byun, S.Y., Stancliffe, R.J., Taub, S., & Chiri, G. (2008b). Choice-making among Medicaid HCBS and ICF/MR recipients in six states. American Journal on Mental Retardation, Volume 113(5), pp. 325 - 342
Lalli, J.S., Browder, D.M., Mace, F.C., & Brown, D.K. (1993). Teacher use of descriptive analysis data to implement interventions to decrease students' problem behaviors. Journal of Applied Behavior Analysis, 26, pp. 227 - 238
Lambe, L. (1990). Leisure Resource training Pack for People with Profound and Multiple Disabilities. Mencap: London
Lambe, L., & Hogg, J. (2000). Creative Arts and People with Profound and Multiple Learning Disabilities: Education, Therapy and Leisure. Pavilion Publishing (Brighton) Ltd
Lambrechts, G. Kuppens, S. & Maes, B. (2009). Staff variables associated with the challenging behaviour of clients with severe or profound intellectual disabilities. Journal of Intellectual Disability Research, Volume 53(7), pp. 620 – 632
Lamond, I.R. (2006). Two steps forward and One step back (Being a reflection on the impact of incorporating dance into the curriculum of Profound and Multiple Learning Difficulties pupils at a Special School). Unpublished Master's Thesis, Leeds Beckett University
Lamonde, M. (2017). Sensory Processing: Techniques, Tactics & SPD Games To Help Your Child With Sensory Processing Disorder. Create Space Independent Publishing Platform
Lancioni, G.E., O’Reilly M.F., & Emerson E. (1996). A review of choice research with people with severe and profound developmental disabilities. Research in Developmental Disabilities, Volume 17(5), pp. 391 – 411
Lancioni, G.E., & O'Reilly, M.F. (1998). A review of research on physical exercise with people with severe and profound developmental disabilities. Research in Developmental Disabilities, Volume 19(6), pp. 477 - 492
Lancioni, G.E., O’Reilly, M.F., Campodonico, F., & Mantini, M. (1998a). Task variation versus task repetition for people with profound developmental disabilities: An assessment of preferences. Research in Developmental Disabilities, Volume 19, 189 – 199
Lancioni, G.E., O’Reilly, M.F., Campodonico, F., & Mantini, M. (1998b). Mobility versus sedentariness in task arrangements for people with multiple disabilities: An assessment of preferences. Research in Developmental Disabilities, Volume 19(6), pp. 465 – 475
Lancioni, G.E., O’Reilly, M.F., Van Dijk, J., & Klaase, M. (1998). An environmental enrichment program to promote adaptive responding in two children with multiple disabilities. Scandinavian Journal of Behaviour Therapy, Volume 27(3), pp. 130 - 134
Lancioni, G.E., O'Reilly, M.F., & Basili, G. (1999). Review of strategies for treating sleep problems in persons with severe or profound mental retardation or multiple handicaps. American Journal on Mental Retardation, Volume 104(2), pp.170 - 186
Lancioni, G.E., O’Reilly, M.F., & Mantini, M. (1999). Activity arrangements with or without mobility and performance of persons with multiple
disabilities over long sessions. Irish Journal of Psychology, Volume 20(2), pp. 124 - 135
Lancioni, G.E., Dijkstra, A.W., & O’Reilly, M.F. (2000). Frequent versus nonfrequent verbal prompts delivered unobtrusively: Their impact on the task performance of adults with intellectual disability. Education and Training in Mental Retardation and Developmental Disabilities, Volume 35(4), pp. 428 - 433
Lancioni, G.E., Cuvo, A.J., & O'Reilly, M.F. (2002). Snoezelen: An overview of research with people with disabilities and dementia. Disability and Rehabilitation: An International, Multidisciplinary Journal, Volume 24(4), pp. 175 - 184
Lancioni, G.E., Abels, J., Wilms, E.H., Singh, N.N., O’Reilly, M.F., & Groeneweg, J. (2003). Microswitch responding and awareness of contingency in persons with profound multiple disabilities. Perceptual and Motor Skills, Volume 96(3), pp. 835 – 838
Lancioni, G.E., Singh, N.N., O'Reilly, M.F., Oliva,D., & Basili, G.(2005). An overview of research on increasing indices of happiness of people with severe/profound intellectual and multiple disabilities,” Disability and Rehabilitation, Volume 27(3), pp. 83 – 93
Lancioni, G.E., Singh, N.N., O’Reilly, M.F., Oliva, D., & Severini, L. (2005). Assessing a micro switch-based stimulation procedure for eye-blinking responses in a young woman with profound multiple disabilities. Perceptual and Motor Skills, Volume 101(1), pp. 212 - 216
Lancioni, G.E., O'Reilly, M.F., Singh, N.N., Sigafoos, J., Oliva, D., Campodonico, F., & Piazzolla, G. (2006). Promoting fluency of performance during morning dressing by two persons with multiple disabilities. Perceptual and Motor Skills, Volume 103, pp. 771 - 777
Lancioni, G.E., O'Reilly, M.F., Singh, N.N., Sigafoos, J., Oliva, D., Campodonico, F., & Groeneweg, J. (2007). Helping Three Persons with Multiple Disabilities Acquire Independent Dressing Through Assistive Technology. Journal of Visual Impairment & Blindness, Volume 101(12), pp. 768 - 773
Lancioni, G.E., Singh, N.N., O'Reilly, M.F., Sigafoos, J., Didden, R., Oliva, D., et al. (2007). Effects of microswitch-based programs on indices of happiness of students with multiple disabilities: A new research evaluation. American Journal on Mental Retardation, Volume 112(3), pp. 167 - 176
Lancioni, G.E., Singh, N.N., O’Reilly, M.F., Sigafoos, J., D’Amico, F., Buonocunto, F., Navarro, J., Lanzilotti, C., Fiore, P., Megna, M., & Damiani, S. (2015). Assistive technology to help persons in a minimally conscious state develop responding and stimulation control: Performance assessment and social rating. NeuroRehabilitation, Volume 37(3), pp. 393 - 403
Land, G., Errington-Povalac, E., & Paul, S. (2001). The effects of therapeutic horseback riding on sitting posture in individuals with disabilities. Occupational Therapy in Care, Volume 14(1), pp. 1 - 12
Lange, K.W., Hauser, J., & Reissmann, A. (2015). Gluten-free and casein-free diets in the therapy of autism. Current Opinion in Clinical Nutrition & Metabolic Care, Volume 18(6), 572 - 575
Langer, E.J., & Rodin, J. (1976). The Effect of Choice and Enhanced Personal Responsibility for the Aged: A Field Experiment in an
Institutional Setting. Journal of Personality and Social Psychology, Volume 34, pp.191 – 98
Langley, B., & Dubose, R.F. (1976). Functional Vision Screening for Severely Handicapped Children. Journal of Visual Impairment & Blindness. Volume 70(8), pp. 346 - 350
Larkey, S. (2007). Practical Sensory Programmes for Students with Autism Spectrum Disorder and Other Special Needs. London: Jessica Kingsley Publishers.
Larson, K.A. (1982). The Sensory History of developmentally Delayed Children With and Without Tactile Defensiveness. American Journal of Occupational Therapy, Volume 36, pp. 590 - 596
LaVigna, G.W., & Donellan, A.M. (1986). Alternatives to Punishment: Solving Behavior Problems with Non-Aversive Strategies. New York: Irvington
Lawes, C., & Woodcock, J. (2000). Music therapy and people with severe learning disabilities who exhibit self injurious behaviour. In - Wigram T, Saperston B, & West R (Eds), The art and science of music therapy. A handbook. Harwood Academic Publishers, Netherlands
Lawrence, M., & Wigram, T. (2005). Music therapy as a tool for assessing hand use and communicativeness in children with Rett Syndrome. Brain & Development, Volume 27, S95 - S96
L’Ecuyer, R. (1978). Le concept de soi [The self-concept], Paris: Presses de l’Universite de France.
Leaning, B., & Watson T. (2006). From the inside looking out – an Intensive Interaction group for people with profound and multiple learning disabilities, British Journal of Learning Disabilities, Volume 34, pp.103 - 109
Leary, M.R. (2004). The curse of the self: Self-awareness, egotism, and the quality of human life. Oxford University Press.
Lecavalier, L. (2006). Behavioral and emotional problems in young people with pervasive developmental disorders: Relative prevalence,
effects of subject characteristics, and empirical classification. Journal of Autism and Developmental Disorders, Volume 36(8), pp. 1101 – 1114
Lee, J., & McFerran, K. (2012). The improvement of non-verbal communication skills of five females with profound and multiple disabilities using song-choices in music therapy. Voices: A World Forum for Music Therapy, Volume 12(3), Retrieved from https://normt.uib.no/index.php/voices/article/viewArticle/644.
Lee, S.H., Wehmeyer, M.L., Soukup, J.H., & Palmer, S.B. (2010). Impact of curriculum modifications on access to the general education curriculum for students with disabilities. Exceptional Children, Volume 76, pp. 213 – 233
Lee, V., & Das Gupta, P. (Eds.)(1995). Children’s cognitive and language development. The Open University. Oxford: Blackwell Publishers
ISBN 0-631-19428-2
Legault, J.R. (1992) A study of the relationship of community living situation to independence and satisfaction on the lives of mentally retarded adults. Journal of Intellectual Disability Research. Volume 36, pp. 129 - 141
Lehtonen, K. (1993). Music Therapy in Finland. In Maranto, C.D., (Ed.), Music Therapy: International Perspectives, Pipersville, Pennsylvania: Jeffrey Books.
Lemke, H. (1974). Self-abusive behavior in the mentally retarded. American Journal of Occupational Therapy, Volume 28, pp. 94 – 98
Lenggenhager, B., Tadi, T., Metzinger, T., & Blanke, O. (2007). Video ergo sum: Manipulating bodily self-consciousness. Science, Volume 317, pp. 1096 – 1099
Lerer, R.J. (1981). An open letter to an occupational therapist. Journal of Learning Disability, Volume 14, pp. 3 - 4
Lerman, D.C., & Iwata, B.A. (1993). Descriptive and experimental analyses of variables maintaining self-injurious behavior. Journal of Applied Behavior Analysis, Volume 26, pp. 293 - 319
Levinger, B. (1992). Nutrition, health, and learning. School nutrition and health network monograph series, Number 1
Lewis, A., & Norwich, B. (2000). Mapping a pedagogy for special educational needs. Exeter : School of Education, University of Exeter.
Lewis, A., & Norwich, B. (2001). A critical review of systematic evidence concerning distinctive pedagogies for pupils with difficulties in learning. Journal of Research in Special Educational Needs, Volume 1(1), pp. 1 - 13
Lewis, A. ( 2002 June). The development of children’s ideas about others’ difficulties in learning, British Journal of Special Education, Volume 29(2), pp. 59 - 65
Lewis, A. ( 2002 August). Accessing, through research interviews, the views of children with difficulties in learning. Support for Learning, Volume 17(3), pp. 111 - 116
Lewis, A., & Norwich, B. (eds)(2005). Special Teaching for Special Children. Berkshire: Open University Press.
Lieberman, H.R. (2007). Hydration and cognition: a critical review and recommendations for future research. Journal of the American
College of Nutrition, Volume 26(5), Supplement, pp. 555 - 561
Lieberman, H.R. (2012). Methods for assessing the effects of dehydration on cognitive function. Nutrition Reviews. Volume 70(2), Supplement. pp.143 - 146
Light, J., McNaughton, D., & Parnes, P. (1986). A protocol for the assessment of the communicative interaction skills of nonspeaking severely handicapped adults and their facilitators. Toronto: Hugh Macmillan Medical Centre
Linderman, T.M., & Stewart, K.B. (1999). Sensory integrative based occupational therapy and functional outcomes in young children with pervasive developmental disorders: A single subject study. American Journal of Occupational Therapy, Volume 53, pp. 207 – 213
Lindsay, W.R., Pitcaithly, D., Geelen, N., Buntin, L., Broxholme, S., & Ashby, M. (1997). A comparison of the effects of four therapy procedures on concentration and responsiveness in people with profound learning disabilities. Journal of Intellectual Disability Research, Volume 41(3), pp. 201 - 207
Lindsay, W.R., Black, E., Broxholme, S., Pitcaithly, D., & Hornsby, N. (2001). Effects of four therapy procedures on communication in people with profound intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 14(2), pp. 110 - 119
Lindsey, J.P. (1996). The right to choose: Informed consent in the lives of adults with mental retardation and developmental disabilities. Education and Training in Mental Retardation and Developmental Disabilities. Volume 31, pp. 171 – 176
Little, T.D., Hawley, P.H., Henrich, C.C., & Marsland, K. (2002). Three views of the agentic self: A developmental synthesis. In E.
L.Deci & R.M.Ryan(Eds.), Handbook of self-determination research (pp. 389 – 404). Rochester, NY: University of Rochester Press.
Little, T.D., Snyder, C.R., & Wehmeyer, M.L. (2006). The agentic self: On the nature and origins of personal agency across the life span. In D. K. Mroczek & T. D. Little (Eds.), Handbook of personality development (pp. 61 – 80). Mahwah, NJ: Lawrence Erlbaum Associates.
Liutsko, L.N. (2013). Proprioception as a basis for individual differences. Psychology in Russia: State of the Art. Volume 6(3), pp. 107 -119
Lloyd, P. (2007). Let's All Listen: Songs for Group Work in Settings that Include Students with Learning Difficulties and Autism. London: Jessica Kingsley.
Logan, K.R., Jacobs, H.A., Gast, D.L., Murray, A.S., Daino, K. & Skala, C. (1998). The impact of typical peers on the perceived happiness of students with profound multiple disabilities. Journal of the Association for Persons with Severe Handicaps, Volume 23(4), pp. 309 – 318
Logan, K.R., & Gast, D.L. (2001). Conducting preference assessments and reinforcer testing for individuals with profound multiple disabilities: Issues and procedures. Exceptionality, Volume 9(3), pp. 123 - 134
Logan, K.R., Jacobs, H.A., Gast, D.L., Smith, P.D., Daniel, J., & Rawls, J. (2001). Preferences and reinforcers for students with profound multiple disabilities: can we identify them? Journal of Developmental and Physical Disabilities, Volume 13(2), pp. 97 - 122
Lohrmann-O'Rourke, S., & Browder, D.M. (1998). Empirically based methods to assess the preferences of individuals with severe disabilities. American Journal of Mental Retardation, Volume 103(2), pp. 146 - 161
Lohrmann-O'Rourke, S., & Yurman, B. (2001). Naturalistic assessment of and intervention for mouthing behaviors influenced by establishing operations. Journal of Positive Behavior Interventions, Volume 3(1), pp. 19 - 27
Lomas, H., & Hallas, P. (1998). It’s a mystery: Accounts of an art therapy group for people with learning disabilities. In - M. Rees (Ed.) Drawing on difference: Art Therapy with people who have learning difficulties, pp. 31–58. London: Routledge.
Longhorn, F. (1988). A Sensory Curriculum for Very Special People. Souvenir Press
Longhorn, F. (2009). Parachute play from Flo Longhorn. Information Exchange, Volume 79, pp. 9 - 10
Longley, S., & Collins, G.J. (1994). The development of a non-verbal satisfaction measure for use with people who have severe or profound learning disabilities. British Journal of Developmental Disabilities, Volume XL(79), pp. 143 - 149
Longo, M., Schüür, F., Kammers, M.P.M., Tsakiris, M., & Haggard, P. (2008). What is embodiment? A psychometric approach. Cognition, Volume 107, pp. 978 – 998
Longo, M.R., Schüür, F., Kammers, M.P., Tsakiris, M., & Haggard, P. (2009). Self awareness and the body image. Acta Psychologica,
Volume 132(2), pp. 166 – 172
Loots, G., & Malschaert, E. (1999). The use in Belgium of developmental movement according to the work of Veronica Sherborne: a developmental psychology view. European Journal of Special Needs Education, Volume 14(3), pp. 221 - 230
Lovaas, I., Freitag, G., Gold, V.J., & Kassorla, I.C. (1965). Experimental studies in childhood schitzophrenia: analysis of self-destructive behavior. Journal of Experimental Child Psychology. Volume 2, pp. 67 - 84
Lovaas, I., Newsom, C., & Hickman, C. (1987). Self-stimulatory behavior and perceptual reinforcement, Journal of Applied Behavior Analysis, Volume 20 (1), pp. 45 - 68
Lovell, D.M., Jones, R.S.P., & Ephraim, G. (1998). The effect of Intensive Interaction on the sociability of a man with severe intellectual disabilities,International Journal of Practical Approaches to Disability. Volume 22(2/3), pp. 3 - 9
Lowe, K., De Paiva, S., & Felce, D. (1993). Effects of a community-based service on adaptive and maladaptive behaviours: A longitudinal study. Journal of Intellectual Disability Research, Volume 37, pp. 3 - 22.
Lowe, K., Felce, D., & Orlowska, D. (1993). Evaluating services for people with challenging behaviour. In I. Fleming & B. Stenfert Kroese (Eds), People with Learning Disability and Severe Challenging Behaviour. Manchester: Manchester University Press.
Lowe, K. Felce, D., & Blackman, D. (1995). People with learning disabilities and challenging behaviour: The characteristics of those referred and not referred to specialist teams. Psychological Medicine, Volume 25(03), pp. 595 – 603
Lowe, K., Allen, D., Jones, E., Brophy, S., Moore, K., & James, W. (2007). Challenging behaviours: prevalence and topographies. Journal of Intellectual Disability Research, Volume 51(8), pp. 625 - 636
Lowe, K., Jones, E., Allen, D., Davies, D., James, W., Doyle, T., Andrew, J., Kaye, N., Jones, S., Brophy, S., & Moore K.(2007). Staff training in positive behaviour support: Impact on attitudes and knowledge. Journal of Applied Research in Intellectual Disabilities, Volume 20(1), pp. 30 – 40
Luijkx, J., van der Putten, A.A., & Vlaskamp, C. (2017). A valuable burden? The impact of children with profound intellectual and multiple disabilities on family life. Journal of Intellectual & Developmental Disability, pp. 1 - 6
Luiselli, J.K. (1992). Protective equipment. In J.K. Luiselli,J.L. Matson, N.N. Singh (Eds.), Self-Injurious behaviour: Analysis, assessment and Treatment. New York: Springer-Verlag
Lundqvist, L. (2013). Prevalence and risk markers of behaviour problems among adults with intellectual disabilities: A total population study in Örebro County. Sweden. Research in Developmental Disabilities, Volume 34(4), pp. 1346 – 1356
Lupien, S.J., McEwen, B.S., Gunnar, M.R., & Heim, C. (2009). Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nature Reviews Neuroscience, Volume 10, pp. 434 - 445
Lustig, R.H., Schmidt, L.A., & Brindis, C.D. (2012). The toxic truth about sugar. Nature. Volume 482. pp. 27 - 29
Lustig, R.H. (2013). Fat Chance: The Bitter Truth about Sugar. Hudson Street Press
Lustig, R.H. (2013b). Fructose: It’s 'Alcohol Without the Buzz'. Advances in Nutrition. Volume 4. pp. 226 - 235
Lyons, G. (2003). Life satisfaction for children with profound and multiple disabilities. (Doctoral dissertation). Newcastle: University of Newcastle, Faculty of Education and Arts.
Lyons, G. (2005). The Life Satisfaction Matrix: an instrument and procedure for assessing the subjective quality of life of individuals with profound multiple disabilities. Journal of Intellectual Disability Research, Volume 49(10), pp. 766 - 769
Lyons, G., & Cassebohm, M. (2012). The education of Australian school students with the most severe intellectual disabilities: where have we been and where could we go? a discussion primer, Australasian Journal of Special Education, Volume 34 (1). pp. 79 - 96
Maag, J.W., Wolchik, S.A., Rutherford, R.B., & Parks, B.T. (1986). Response covariation on self-stimulatory behaviors during sensory extinction procedures. Journal of Autism and Developmental Disorders, Volume 16(2), pp. 119 - 132
Maber-Aleksandrowicz, S., Avent,C., & Hassiotis, A. (2016). A Systematic Review of Animal-Assisted Therapy on Psychosocial Outcomes in People with Intellectual Disability. Research in Developmental Disabilities. Volume 49–50, pp. 322 – 338
Macauley, B.L., & Guiterrez, K.M. (2004). The effectiveness of hippotherapy for children with language-learning disabilities. Communication Disorders Quarterly, Volume 25(4), pp. 205 – 217
MacDonald, J. (1992). Dance? Of Course I can! Dance movement therapy for people with learning disabilities, in Payne, H. (Ed.), Dance Movement Therapy: Theory and Practice, London: Routledge, pp. 202 - 217 (First edition)
MacDonald, R., O’Donnell, P., & Davies, J. (1999). An empirical investigation into the effects of structured music workshops for individuals with intellectuals disabilities. Journal of Applied Research in Intellectual Disabilities. Volume 12, pp. 225 – 240
MacFarland, S. (1995). Teaching strategies of the van Dijk curricular approach. Journal of Visual Impairment & Blindness, Volume 89, pp. 222 - 228
Mackie, R.T., McCulloch, D.L., Saunders, K.J., Ballantyne, J., Day, R.E., Bradnam, M.S., & Dutton, G.N. (1995). Comparison of visual assessment tests in multiply handicapped children. Eye, Volume 9(1), pp. 136 - 141
MacKinnon, J.R., Noh, S., Lariviere, J., MacPhail, A., Allan, D.E., & Labiberte, D. (1995a). A study of therapeutic effects of horseback riding for children with cerebral palsy. Physical & Occupational Therapy in Pediatrics, Volume 15(1), pp. 17 - 34
MacKinnon, J.R., Noh, S., Lariviere, J., MacPhail, A., Allan, D.E., & Labiberte, D. (1995b). Therapeutic horse riding: A review of the literature. Physical & Occupational Therapy in Pediatrics, Volume 15(1), pp. 1 - 15
MacPhail, A.H.E., Edwards, J., Golding, J., Miller, K., Mosier, C., & Zwiers, T. (1998). Trunk postural reactions in children with and without cerebral palsy during therapeutic horseback riding. Pediatric Physical Therapy, Volume 10, pp.143 – 147
Madge, N. & Fassam, M. (1982): Ask the children. London: Batsford
Maes, B., Lambrechts, G., Hostyn, I., & Petry, K. (2007). Quality-enhancing interventions for people with profound intellectual and multiple disabilities: A review of the empirical research literature. Journal of Intellectual and Developmental Disability, Volume 32(3), pp. 163 – 178
Maestú, F., Arrazola, J., Fernández, A., Simos, P.G., Amo, C., Gil-Gregorio, P., Fernandez, S., Papanicolaou, A., & Ortiz, T. (2003). Do cognitive patterns of brain magnetic activity correlate with hippocampal atrophy in Alzheimer’s disease? The Journal of Neurology, Neurosurgery, and Psychiatry. Volume 74. pp. 208 – 212
Magee, W., & Bowen, C. (2008). Using music in leisure to enhance social relationships with patients with complex disabilities. NeuroRehabilitation, Volume 23(4), pp. 305 - 311
Mageshwari, U.S., & Minitha, S.J. (2006). Impact of dietary exclusion of casein and gluten on selected autistic children. Indian Journal of Nutrition and Dietetics, Volume 43, pp. 183 – 191
Maglieri, K.A., DeLeon, I.G., Rodriguez-Catter, V., & Sevin, B.M. (2000). Treatment of covert food stealing in an individual with Prader-Willi syndrome. Journal of Applied Behavior Analysis, Volume 33(4), pp. 615 - 618
Magne Tellevik, J., & Elmerskog, B. (2009). Activity-based intervention for multiple-disabled visually impaired people. The British Journal of Visual Impairment, Volume 27(3), pp. 204 - 220
Maguire, E.A., Frackowiak, R.S.J., & Frith, C.D. (1997). Recalling routes around London: activation of the right hippocampus in taxi drivers. Journal of Neuroscience, Volume 17, pp. 7103 – 7110
Maguire, E.A., Burgess, N., Donnett, J.G., Frackowiak, R.S.J., Frith, C.D., & O’Keefe, J. (1998). Knowing where and getting there: a human navigation network. Science, Volume 280. pp. 921 – 924
Maguire, E.A., Gadian, D.G., Johnsrude, I.S., Good, C.D., Ashburner, J., Frackowiak, R.S.J., & Frith, C.D. (2000). Navigation-related structural change in the hippocampi of taxi drivers. Proceedings of the National Academy of Sciences of the United States of America, Volume 97(8), pp. 4398 – 4403
Maguire, E.A., Spiers, H.J., Good, C.D., Hartley, T., Frackowiak,R.S.J., & Burgess, N. (2003). Navigation Expertise and the Human Hippocampus: A Structural Brain Imaging Analysis. Hippocampus. Volume 13. pp. 208 – 217
Maguire, E.A., Woollett, K., & Spiers, H.J. (2006). London taxi drivers and bus drivers: a structural MRI and neuropsychological analysis. Hippocampus. Volume 16(12). pp. 1091 - 1101
Maier, S.F., & Seligman, M. (1976). Learned helplessness: Theory and evidence. Journal of Experimental Psychology, Volume 105, pp. 3 - 46
Maisto, C.R., Baumeister, A.A., & Maisto, A.A. (1978). An analysis of variable related to self-injurious behavior among institutionalised retarded persons. Journal of Mental Deficiency Research. Volume 22, pp. 27 - 36
Mailloux, Z. (1992). Tactile Defensiveness: Some People are More Sensitive. Sensory Integration Quarterly, Vol 20(3), pp. 10 - 11
Mailloux, Z., Mulligan, S., Smith Roley, S., Blanche, E., Cermak, S., Geppert Coleman, G., Bodison, S., & Lane, C.J. (2011). Verification and Clarification of Patterns of Sensory Integrative Dysfunction, American Journal of Occupational Therapy, Volume 65, pp. 143 - 151
Manly, T., Dobler, V.B., Dodds, C.M., & George, M.A. (2005). Rightward shift in spatial awareness with declining alertness. Neuropsychologia, Volume 43(12), pp. 1721 - 1728
Mans, L., Cicchetti, D., & Sroufe, L.A. (1978). Mirror reactions of Down syndrome infants and toddlers: Cognitive underpinnings of self-recognition. Child Development, Volume 49, pp. 1247 - 1250
Mansell, J., Felce, D., de Kock, U., & Jenkins, J. (1982). Increasing purposeful activity of severely and profoundly mentally- handicapped adults. Behaviour Research and Therapy, Volume 20, 593 - 604
Mansell, J. (1984). The operation of regional special support services for people with mental handicap and behavioural problems. Croydon: South East Thames Regional Health Authority.
Mansell, J., Jenkins, J., Felce, D., & de Kock, U. (1984). Measuring the activity of severely and profoundly mentally handicapped adults in ordinary housing. Behaviour Research and Therapy, Volume 22(1), pp. 23 - 29
Mansell, J. (1985). Special services for people with severe mental handicap and severe behaviour problems. Croydon: South East Thames Regional Health Authority
Mansell, J., Felce, D., Jenkins, J., de Kock, U., & Toogood, A. (1987). Developing staffed housing for people with mental handicaps. Tunbridge Wells: Costello.
Mansell, J., & Beasley, F. (1990). Severe mental handicap and problem behaviour: Evaluating transfer from institutions to community care. In W. Fraser (Ed.), Key Issues in Mental Retardation Research. Routledge, London, pp. pp. 405 - 414
Mansell, J. (1994) Specialized group homes for persons with severe or profound mental retardation and serious problem behaviour in England. Research in Developmental Disabilities, Volume 15, pp. 371 - 388
Mansell, J., Hughes, H., & McGill, P. (1994) Maintaining local residential placements. In E. Emerson, P. McGill, & J. Mansell (Eds.), Severe Learning Disabilities and Challenging Behaviour: Designing High-Quality Services (pp. 260 - 281). London: Chapman and Hall.
Mansell, J. (1995). Staffing and staff performance in services for people with severe or profound learning disability and serious challenging behaviour. Journal of Intellectual Disability Research, Volume 39, pp. 3 - 14
Mansell, J., & Elliott, T. (2001). Staff members' prediction of consequences for their work in residential settings. American Journal on Mental Retardation, Volume 106(5), pp. 434 - 447
Mansell, J., McGill, P., & Emerson, E. (2001). Development and evaluation of innovative residential services for people with severe intellectual disability and serious challenging behaviour. In L.M. Glidden (Ed.), International Review of Research in Mental Retardation (pp.245-298). San Diego, CA: Academic Press.
Mansell, J., Elliott, T., Beadle-Brown, J., Ashman, B., & Macdonald, S. (2002). Engagement in meaningful activity and ‘active support’ of people with intellectual disabilities in residential care. Research in Developmental Disabilities, Volume 23(5), pp. 342 – 352
Mansell, J., Beadle-Brown, J., Macdonald, S., & Ashman, B. (2003). Resident involvement in activity in small community homes for people with learning disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 16(1), pp. 63 - 74
Mansell, J., & Beadle‐Brown, J. (2004). Person‐centred planning or person‐centred action? Policy and practice in intellectual disability services. Journal of Applied Research in Intellectual Disabilities, Volume 17(1), pp. 1 - 9
Mansell, J. (2010). Raising our Sights. How-to-Guide . What people do in the day. Mencap
Marcason, W. (2009). What is the current status of research concerning use of a gluten-free, casein-free diet for children diagnosed with autism? Journal of the American Dietetic Association, Volume 109(3), pp. 572
March, J. (1990). The use of peer students to facilitate Words Strategy training. 11th Southeast Annual Augmentative Communication Conference Proceedings, pp. 94 - 98, Birmingham, Alabama: SEAC
Margetts, L. (2010). ‘Hansel and Gretel’. Meaning and relevance in a therapeutic journey: An exploration of the relevance of fairy tales to work with older learning disabled clients who have been institutionalised. British Journal of Music Therapy, Volume 24, pp. 12 – 21
Marí-Bauset, S., Zazpe, I., Mari-Sanchis, A., Llopis-González, A., & Morales-Suárez-Varela, M. (2014). Evidence of the gluten-free and casein-free diet in autism spectrum disorders: a systematic review. Journal of Child Neurology, Volume 29(12), pp. 1718 - 1727
Markowitsch, H.J., & Staniloiu, A. (2011). Memory, autonoetic consciousness, and the self, Consciousness and Cognition, Volume 20(1), pp. 16 - 39
Marsh, H.W. (1994). Using the National Longitudinal Study of 1988 to evaluate theoretical models of self-concept: The Self-Description Questionnaire. Journal of Educational Psychology, Volume 86(3), pp. 439 - 456
Martell, K.A. (2012). Increasing Positive Interactions Between Staff and Individuals with Disabilities: The Impact of Training on
Acquisition and Maintenance. Dissertations. 660.
Martin, F., & Farnum, J. (2002). Animal assisted therapy for children with pervasive developmental disorders. Western Journal of Nursing Research, Volume 24, pp. 657 – 670
Martin, J.E., Marshall, L., Maxson, L.L., & Jerman, P. (1993). Self-Directed IEP. Longmont, CO: Sopris West.
Martin, J.E., Van Dycke, J.L., Christensen, W.R., Greene, B.A., Gardner, J.E., & Lovett, D.L. (2006). Increasing student participation in IEP meetings: Establishing the self-directed IEP as an evidenced-based practice. Exceptional Children, Volume 72, pp. 299 – 316
Martin, P.L., & Foxx, R.M. (1973). Victim control of the aggression of an institutionalized retardate. Journal of Behavior Therapy and Experimental Psychiatry, Volume 4, pp. 161 - 165
Martin, T.L., Martin, G.L., Spevack, S., Verbeke, A., & Yu, D.C.T. (2002). Does choice, independent of preference, improve behavior for persons with developmental disabilities? A review. Developmental Disabilities Bulletin, Volume 30, pp. 1 – 15
Martorell, A., Gutierrez-Recacha, P., Pereda, A., & Ayuso-Mateos, J.L. (2008). Identification of personal factors that determine work outcome for adults with intellectual disability. Journal of Intellectual Disability Research, Volume 52, pp. 1091 – 1101
Masento, N.A., Golightly, M., Field, D.T., Butler, L.T., & van Reekum, C.M. (2014). Effects of hydration status on cognitive performance and mood. British Journal of Nutrition. Volume 111. pp. 1841 - 1852
Mason, C., Field, S., & Sawilowsky, S. (2004). Implementation of self-determination activities and student participation in IEPs. Exceptional Children, Volume 70, pp. 441 – 451
Mason, S.A., & Iwata, B.A. (1990). Artifactual effects of sensory-integrative therapy on self-injurious behavior. Journal of Applied Behavior Analysis, Volume 23, pp. 361 – 370
Matson, J.L., Smiroldo, B.B., Hamilton, M., & Baglio, C.S. (1997). Do anxiety disorders exist in persons with severe and profound mental retardation? Research in Developmental Disabilities, Volume 18(1), pp. 39 - 44
Matson, J.L., Bielecki, J., Mayville, E.A., Smalls, Y., Bamburg, J.W., & Baglio, C.S. (1999). The Development of a Reinforcer Choice Assessment Scale for Persons with Severe and Profound Mental Retardation. Research in Developmental Disabilities, Volume 20(5). pp. 379 – 384
Matson, J.L., Bamburg, J.W., & Smalls, Y. (2004). An analysis of Snoezelen equipment to reinforce persons with severe or profound mental retardation. Research in Developmental Disabilities, Volume 25(1), pp. 89 - 95
Matson, J.L., & Boisjoli, J.A. (2007). Multiple versus maintaining factors of challenging behaviours as assessed by the QABF for adults with intellectual disabilities. Journal of Intellectual Disability Research. Volume 32, pp. 39 – 44
Matson, J.L., Neal, D., Hess, J.A., & Kozlowski, A.M. (2011). Assessment of toileting difficulties in adults with intellectual disabilities: An examination using the profile of toileting issues (POTI). Research in Developmental Disabilities, Volume 32(1), pp. 176 - 179
Matthews, T., Weston, N., Baxter, H., Felce, D., & Kerr, M. (2008). A general practice-based prevalence study of epilepsy among adults with intellectual disabilities and of its association with psychiatric disorder, behaviour disturbance and carer stress. Journal of Intellectual Disability Research. Volume 52, pp. 163 – 173
Mauer, D.A. (1999). Issues and Applications of Sensory Integration Theory and Treatment With Children With Language Disorders. Language, Speech, and Hearing Services in Schools. Volume 30, pp. 383 - 392
Maurice, P., & Trudel, G. (1982). Self-injurious behavior: prevalence and relationship to environmental events. In J.H. Hollis & C.E. Meyers, (Eds.), Life-Threatening Behavior: Analysis and Intervention. Washington, D.C.: American Association on Mental Deficiency.
May-Benson, T. (2011). Understanding the Occupational Therapy Needs of Adults With Sensory Processing Disorder. OT practice, Volume 16(10), pp.13 - 14,16 - 18
McAfee,J.K. (1987). Classroom density and the aggressive behavior of handicapped children. Education and Treatment of Children, Volume 10, pp. 134 - 145
McBride, K. (2003). Identifying Person Preference in Individuals With a Profound Learning Disability and High Support Needs. University of Hull
McBride, S.D., Perentos, N., & Morton, A.J. (2015). Understanding the concept of a reflective surface: Can sheep improve navigational ability through the use of a mirror? Animal Cognition, Volume 18, pp. 361 – 371
McBrien, J., & Weightman, J. (1980). The effect of room management procedures on engagement of profoundly handicapped children. British Journal of Mental Subnormality, Volume 26, pp. 38 - 53
McCall, R.B. (1972). Smiling and vocalization in infants as indices of perceptual-cognitive processes. Merrill-Palmer Quarterly, Volume 18, pp. 341 - 347
McCarty, B.C., McElfresh, C.T., Rice, S.V., & Wilson, S.J. (1978). The effect of contingent background music on inappropriate bus behaviour. Journal of Music Therapy, Volume 15(3), pp. 150 - 156
McClelland, J.L. (1996). Role of the Hippocampus In Learning and Memory: A Computational Analysis. In - Ono, T., McNaughton, B.L., Molotchnikoff, S., Rolls, E.T., & Nichijo, H. (Eds. ), Perception, Memory, and Emotion. pp. 601- 613. Frontier in Neuroscience. Oxford: Elsevier Science, Ltd.
McClintock, K., Hall, S., & Oliver, C. (2003). Risk markers associated with challenging behaviours in people with intellectual disabilities: A meta-analytic study. Journal of Intellectual Disability Research, Volume 47(6), pp. 405 - 416
McConkey, R., Morris, I., & Purcell, M. (1999). Communications between staff and adults with intellectual disabilities in naturally occurring settings. Journal of Intellectual Disability Research, Volume 43(3), pp. 194 - 205
McConkey, R., & Collins, S. (2010a). Using personal goal setting to promote the social inclusion of people with intellectual disability living in supported accommodation. Journal of Intellectual Disability Research, Volume 54(2), pp. 135 - 143
McConkey, R., & Collins, S. (2010b). The role of support staff in promoting the social inclusion of persons with an intellectual disability. Journal of Intellectual Disability Research, Volume 54(8), pp. 691 - 700
McCool, C., Barrett, S., Emerson, E., Toogood, A., Hughes, H., & Cummings, R. (1989). Challenging behaviour and community services. 5. Structuring staff and client activity. Mental Handicap, Volume 17, pp. 60 - 64
McDonnell, A., & Sturmey, P. (1993). Managing violent and aggressive behaviour: towards better practice. In S. Jones & C. Eayres (Eds), Challenging Behaviour and Intellectual Disability: psychological perspectives. Kidderminster: BILD
McEwen, B.S. (2012). Brain on stress: How the social environment gets under the skin. Proceedings of the National Academy of Sciences. Volume 109(2). pp. 17180 – 17185
McEwen, I.R. (1992). Assistive positioning as a control parameter of social-communicative interactions between students with profound multiple disabilities and classroom staff. Physical Therapy, Volume 72(9), pp. 634 - 644
McFerran, K., & Rickson, D. (2007). Music therapy in special education: Where are we now? The New Zealand Journal of Education, Volume 8(1), pp. 40 - 47
McFerran, K., & Shanahan, E. (2011). Music therapy practice in special education and children's hospice: A systematic comparison of two music therapists' strategies with three pre-adolescent boys. Music Therapy Perspectives, Volume 29(2), pp. 103 - 111
McFerran, K., & Elefant, C. (2012). A Fresh Look at Music Therapy in Special Education. In - G. McPherson & G. Velch (Eds.), The Oxford Handbook of Music Education, Vol. 2, pp. 51 - 64. Oxford: Oxford University Press.
McFerran, K., & Shoemark, H. (2013). How musical engagement promotes well-being in education contexts: The case of a young man with profound and multiple disabilities. International Journal of Qualitative Studies on Health & Well-Being, Volume 8, pp. 1 - 14
McGill, P., Emerson, E., & Mansell, J. (1994). Individually designed residential provision for people with seriously challenging behaviours. In E. Emerson, P. McGill, & J. Mansell (Eds.), Severe Learning Disabilities and Challenging Behaviour: Designing High-Quality Services. London: Chapman and Hall.
McGill, P., & Mansell, P. (1995). Community placements for people with severe and profound learning disabilities and serious challenging behaviour: Individual illustrations of issues and problems. Journal of Mental Health, Volume 4, pp. 183 - 198.
McGill, P., Bradshaw, J., & Hughes, A. (2007). Impact of extended education/training in positive behaviour support on staff knowledge, causal attributions and emotional responses. Journal of Applied Research in Intellectual Disabilities, Volume 20(1), pp. 41 – 51
McGimsey, J.F., & Favell, J.E. (1988). The effects of increased physical exercise on disruptive behavior in retarded persons. Journal of Autism and Developmental Disorders, Volume 18, pp. 167 - 179
McGuire, B.E. Daly, P., & Smyth, F. (2007). Lifestyle and health behaviours of adults with an intellectual disability. Journal of Intellectual Disability Research, Volume 51(7). pp. 497 - 510
McGuire, J., & McDonnell, J. (2008). Relationships between recreation and levels of self-determination for adolescents and young adults with disabilities. Career Development for Exceptional Individuals, Volume 31, pp. 154 – 163
McIntyre, L.L. Blacher, J., & Baker, B.L. (2002). Behaviour/mental health problems in young adults with intellectual disability: The impact on families. Journal of Intellectual Disability Research, Volume 46, pp. 239 – 249
McIntyre, L.L., Kraemer, B.R., & Blacher, J. Simmerman., S. (2004). Quality of life for young adults with severe intellectual disability: Mothers' thoughts and reflections. Journal of Intellectual and Developmental Disability, Volume 29, pp. 131 - 146
McKendrick, O. (1991). Assessment of Multi-handicapped Visually Impaired Children. Royal National Institute for the Blind.
McKenzie, K. (2011). Providing services in the United Kingdom to people with an intellectual disability who present behaviour which challenges: A review of the literature. Research in Developmental Disabilities, Volume 32(2). pp. 395 - 403
McKnight, T.J., & Kearney, C.A. (2001). Staff Training Regarding Choice Availability for Persons with Mental Retardation: A Preliminary Analysis. Journal of Developmental and Physical Disabilities, Volume 13(1), pp. 1 - 10
McLarty, M. (1991). Learning through real experience. Deafblind Education, Volume 7, pp. 10 - 13
McLean, J. E., McLean, L. K., Brady, N. C., & Etter, R. (1991). Communication profiles of two types of gesture using nonverbal persons with severe to profound mental retardation. Journal of Speech, Language, and Hearing Research, Volume 34(2), pp. 294 - 308
McLinden, M.. & McCall, S. (2002). Learning through Touch. Supporting Children with Visual Impairment and Additional Difficulties. London: David Fulton.
McNairn, P. (1995). Freedom and success. 3rd Annual Pittsburgh Employment Conference Proceedings. pp. 73 - 77
McNaughton, D., & Light, J. (1989). Teaching facilitators to support the communication skills of an adult with severe cognitive disabilities: A case study. Augmentative and Alternative Communication, Volume 5(1), pp. 35 - 41
McNicholas, J., Collis, G.M., & Morley, I.E. (1993). Psychological and physical effects of enforced pet loss on older people entering residential care. Journal of Companion Animal Studies. Volume 5(4)
McNicholas, J., Gilbey, A., Rennie, A., Ahmedzai, S., Dono, J., & Ormerod, E. (2005). Pet ownership and human health: a brief review of evidence and issues. British Medical Journal, Volume 7527, pp. 1252 - 1254
McNicholas. J., & Collis, G.M. (2006). Animals as social supports: insights for understanding animal assisted therapy. In - Fine, A. (ed.), Handbook on Animal-Assisted Therapy. Elsevier, San Diego:pp. 49 - 71
McVilly, K.R., Burton-Smith, R.M., & Davidson, J.A. (2000). Concurrence between subject and proxy ratings of quality of life for people with and without intellectual disabilities. Journal of Intellectual and Developmental Disability, Volume 25(1), pp. 19 - 39
Meador, D.M., & Osborn, R.G. (1992). Prevalence of severe behavior disorders in persons with mental retardation and treatment procedures used in community and institutional settings. Behavioral Residentiall Treatment. Volume 4, pp. 299 - 314
Medeiros, K., Rojahn, J., Moore, L.L., & Ingen, D.J. (2014). Functional properties of behaviour problems depending on level of intellectual disability. Journal of Intellectual Disability Research, Volume 58(2), pp. 151 - 161
Mednick, M. (2002). Supporting children with multiple disabilities. Birmingham: Questions Publishing.
Mehigan, P. (2004). Teaching contingency awareness in the classroom to pupils with very profound general learning disabilities, Unpublished Master's Thesis, St. Patrick's College, Dublin City University.
Mehigan, P. & Ware, J. (2004). Teaching Contingency-Awareness in the Classroom, Presentation at IASSID 12th World Congress, Montpellier, France.
Mehler, M.F. (2000). Brain dystrophin, neurogenetics and mental retardation. Brain Research Reviews, Volume 32(1), pp. 277 - 307
Mehrabian, A., & Ferris, S.R. (1967). Inference of attitudes from nonverbal communication in two channels. The Journal of Counselling Psychology. Volume 31(3), pp. 248 - 252
Mellstrom, B.P., Saunders, M.D., Saunders, R.R., & Olswang, L.B. (2005). Interaction of behavioural state and microswitch use in individuals with profound multiple impairments. Journal of Developmental and Physical Disabilities, Volume 17(1), pp. 35 – 53
Melville, C.A., Hamilton, S., Hankey, C.R., Miller, S., & Boyle, S. (2007). The prevalence and determinants of obesity in adults with intellectual disabilities. Obesity Reviews, Volume 8(3), 223 - 230
Melville, C.A., Cooper, S.A., Morrison, J., Allan, L., Smiley, E., & Williamson, A. (2008). The prevalence and determinants of obesity in adults with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 21(5), pp. 425 - 437
Melville, C.A., Oppewal, A., Elinder, L.S., Freiberger, E., Guerra-Balic, M., Hilgenkamp, T.I., Einarsson, I., Izquierdo-Gómez, R., Sansano-Nadal, O., Rintala, P., & Cuesta-Vargas, A. (2017). Definitions, measurement and prevalence of sedentary behaviour in adults with intellectual disabilities - A systematic review. Preventive Medicine. Volume 97. pp. 62 - 71
Melville, H. (1853). Bartleby, The Scrivener: A Story Of Wall-street. Putnam's Monthly Magazine, two parts in November and December 1853
Mencap (2008). About Profound and Multiple Learning Disabilities, Mencap Publications
Mercer, C.D., & Snell, M.E. (1977). Learning theory research in mental retardation: Implications for teaching. Columbus, OH: Merrill.
Mercieca, D.P. (2012). Living Otherwise: Students with Profound and Multiple Learning Disabilities as Agents in Educational Contexts. Sense Publishers
Merino, J., Kones, R., Ferré, R., Plana, N., Girona, J., Aragonés, G., Ibarretxe, D., Heras, M., & Masana, L. (2013). Negative effect of a low-carbohydrate, high-protein, high-fat diet on small peripheral artery reactivity in patients with increased cardiovascular risk. British Journal of Nutrition. Volume 109(7). pp. 1241 - 1247
Messent, P.R., Cooke, C.B., & Long, J. (1998). Physical activity, exercise and health of adults with mild and moderate learning disabilities. British Journal of Learning Disabilities, Volume 26(1), pp. 17 – 22
Messent, P.R., Cooke, C.B., & Long, J. (1999). Primary and secondary barriers to physically active healthy lifestyles for adults with learning disabilities. Disability and Rehabilitation, Volume 21(9), pp. 409 - 419
Metell, M. (2014). Dis/Abling musicking: Reflections on a disability studies perspective in music therapy. Voices: A World Forum for Music Therapy, Volume 14(3), Retrieved from: https://voices.no/index.php/voices/article/view/786/657.
Milgram, N. (1973). Cognition and language in mental retardates: Distinctions and implications In - The experimental psychology of mental
retardation, Routh, D. (Ed.), pp. 157 - 230, London: Crosby Lockwood Staples (1974)
Miller, K. (2008) Wired: Energy drinks, jock identity, masculine norms, and risk taking. Journal American College Health, Volume 56(5), pp.
481 - 490
Miller, L.J. (2007). Sensational Kids: Hope and Help for Children with Sensory Processing Disorder. New York: Perigee.
Miller, L.K. (1999). The savant syndrome: intellectual impairment and exceptional skill. Psychological Bulletin, volume 125(1), pp. 31 - 46
Miller, S., & Aitken, S. (2003). Personal Communication Passports, Guidelines for Good Practice. Call Centre, Scotland
Millward, C., Ferriter, M., Calver, S.J., & Connell‐Jones, G.G. (2008). Gluten‐and casein‐free diets for autistic spectrum disorder. The Cochrane Library.
Ming Lee Yeh, A. (2008). Canine AAT model for autistic children. Tokyo Japan: At Taiwan International Association of Human-Animal Interaction International Conference.
Mirenda, P. (1993a). AAC: Bonding the uncertain mosaic. AAC, Volume 9(1), pp. 3 - 9
Mirenda, P. (1993b). Communication approaches for persons with severe intellectual disabilities. 14th Southeast Annual Augmentative
Communication Conference Proceedings, pp. 67 - 83, Birmingham, Alabama: SEAC
Misso, N. (2001). Guide to orientation and mobility for young children with vision impairments. RNIB
Mitchell, J., & van der Gaag, A. (2002). Through the eye of the Cyclops: Evaluating a multi-sensory intervention programme for people with complex disabilities. British Journal of Learning Disabilities, Volume 30(4), pp. 159 – 165
Mitchell, R.W. (2002). Subjectivity and self-recognition in animals, in M.R. Leary & J.P. Tangney (Eds.), Handbook of Self and Identity. pp. 567 - 595. New York: Guilford Press.
Mitchell, S.W. (1871). Phantom limbs, Lippincott’s Magazine of Popular Literature and Science. Volume 8, pp. 563 – 569
Mithaug, D.E., & Hanawalt, D.A. (1978). The validation of procedures to assess prevocational task preferences in retarded adults. Journal of Applied Behavior Analysis, Volume 11, pp. 153 - 162
Mithaug, D.E., & Mar, D. (1980). The relation between choosing and working prevocational tasks in two severely retarded young adults. Journal of Applied Behavior Analysis, Volume 13, pp. 177 – 182
Mithaug, D.E., Campeau, P.L., & Wolman, J.M. (2003). Assessing self-determination prospects among students with and without disabilities. In D.E. Mithaug, D.K. Mithaug, M. Agran, J.E. Martin, & M.L. Wehmeyer (Eds.), Self determined learning theory: Construction, verification, and evaluation (pp. 61 – 76). Mahwah, NJ: Lawrence Erlbaum.
Mithaug, D.K., & Mithaug, D.E. (2003). The effects of choice opportunities and self-regulation training on the self-engagement and learning of young children with disabilities, in: Self-Determined Learning Theory: Construction, Verification, and Evaluation, D.E. Mithaug, D.K. Mithaug, M. Agran, J.E. Martin, and M. Wehmeyer, eds pp. 141–157. Mahwah, NJ: Lawrence Erlbaum Associates, Inc, Publishers
Moffat V. (1996). Life Without Jargon: How to Help People with Learning Difficulties Understand What You Are Saying. Choice Press
Montello, L., & Coons, E.E. (1999). Effects of active versus passive group music therapy on pre-adolescents with emotional, learning, and behavioral disorders. Journal of Music Therapy, Volume 35(1), pp. 49 - 67
Montgomery, P., & Richer, E. (1977). Effect of sensory integrative therapy on the neuromotor development of retarded children. Physical
Therapy, Volume 57, pp. 799 - 807
Morin, A., & DeBlois, S. (1989). Gallup's mirrors: more than an operationalization of self-awareness in primates? Psychological Reports, Volume 65, pp. 287 - 291
Morin, A., & Everett, J. (1990). Inner speech as a mediator of self-awareness, self-consciousness, and self-knowledge: an hypothesis, New Ideas in Psychology, Volume 8(3), pp. 337 - 356
Morin, A. (2002). Right hemispheric self-awareness: A critical assessment. Consciousness and Cognition, Volume 11, pp. 396 – 401
Morin, A. (2003). Let’s face it. A review of Keenan, Gallup, & Falk’s book ‘‘The Face in the Mirror”. Evolutionary Psychology, Volume 1, pp. 161 – 171
Morin, A. (2004). A neurocognitive and socioecological model of self-awareness. Genetic, Social, and General Psychology Monographs, Volume 130, pp. 197 – 222
Morin, A. (2005). Possible links between self-awareness and inner speech: Theoretical background, underlying mechanisms, and empirical evidence. Journal of Consciousness Studies, Volume 12(4-5), pp.115 - 134
Morin, A. (2006). Levels of consciousness and self-awareness: A comparison and integration of various views. Consciousness and Cognition. Volume 15, pp. 358 – 371
Morin, A. (2007). Self-awareness and the left hemisphere: The dark side of selectively reviewing the literature (Commentary on Keenan et al., Cortex, 2005). Cortex, Volume 8, pp. 1068 – 1073
Morin, A., & Michaud, J. (2007). Self-awareness and the left inferior frontal gyrus: Inner speech use during in self-related processing. Brain Research Bulletin, Volume 74(6), pp. 387 – 396
Morin, A. (2009). Self-awareness deficits following loss of inner speech: Dr. Jill Bolte Taylor's case study. Consciousness and Cognition. Volume 18(2), pp. 524 - 529
Morin, A. (2010). Self-recognition, Theory-of-Mind, and self-awareness: what side are you on? Laterality, Volume 16(3), pp. 367 - 383
Morin, A. (2011). Self‐Awareness Part 1: Definition, Measures, Effects, Functions, and Antecedents. Social and Personality Psychology Compass. Volume 5(10). pp. 807 – 823
Morin, A., Uttl, B., & Hamper, B. (2011). Self-reported frequency, content, and functions of inner speech, Procedia-Social and Behavioral Journal, Volume 30, pp. 1714 - 1718
Morin, A. (2012). Inner speech, in W. Hirstein (ed), Encyclopedia of human behavior (2nd edition), pp. 436 - 443, Elsevier.
Morin, A. (2017). The self-reflective function of inner speech: Twelve years later. ResearchGate.Net
Morley, R. & Lucas, A. (1997). Nutrition and cognitive development. British Medical Bulletin. Volume 53(1). pp.123 - 134
Morningstar, M., & Wehmeyer, M.L. (2008). The role of families in enhancing transition outcomes for youth with learning disabilities. In G. Blalock, J. Patton, P. Kohler, & D. Bassett (Eds.), Transition and students with learning disabilities: Facilitating the movement from school to adult life (2nd ed., pp. 79 – 104). Austin, TX: ProEd Publishers.
Morris, R. & Fillenz, M. (eds) (2003). Neuroscience: the Science of the Brain. The British Neuroscience Association
Morrison, M.L. (2007). Health benefits of animal assisted interventions. Complementary Health Practice Review. Volume 12(1). pp. 51 - 62
Mortenson, B.P., & Witt, J.C. (1998). The use of weekly performance feedback to increase teacher implementation of prereferral intervention. School Psychology Review, Volume 27(4), pp. 613 - 627
Moss, C.V. (1972). Recovery with Aphasia. Illinois: University of Illinois Press.
Moss, J., Oliver, C., Hall, S., Arron, K., Sloneem, J., & Petty, J. (2005). The association between environmental events and self-injurious behaviour in Cornelia de Lange syndrome. Journal of Intellectual Disability Research, Volume 49, pp. 269 – 277
Mottron, L., Belleville, S., Stip,E., & Morasse, K. (1998). Atypical memory performance in an autistic savant. Memory, Volume 6(6), pp. 593 - 607
Mount, H., & Cavet, J. (1995). Multi‐sensory environments: an exploration of their potential for young people with profound and multiple learning difficulties. British Journal of Special Education, Volume 22(2), pp. 52 - 55
Mulford, H. (2001). A review of the curriculum for pupils with profound and multiple learning disabilities. Tizard Learning Disability Review, Volume 6(2), pp. 30 - 31
Mulick, J.A., Hoyt, P., Rojahn, J., & Schroeder, S.R. (1978). Reduction of a “nervous habit” in a profoundly retarded youth by increasing toy play. Journal of Behavior Therapy and Experimental Psychiatry, Volume 9, pp. 381 – 385
Mulligan, S. (1998). Patterns of sensory integration dysfunction: A confirmatory factor analyses. American Journal of Occupational Therapy, Volume 52, pp. 819 – 828.
Mulligan, S. (2002). Advances in sensory integration research. In A.C. Bundy, S. Lane, & E.A. Murray, (Eds.). Sensory integration: Theory and practice (2nd ed., pp. 397 – 411). Philadelphia: F. A. Davis.
Mulloy, A., Lang, R., O’Reilly, M., Sigafoos, J., Lancioni, G., & Rispoli, M. (2010). Gluten-free and casein-free diets in the treatment of autism spectrum disorders: A systematic review. Research in Autism Spectrum Disorders, Volume 4(3), pp. 328 – 339
Mulloy, A., Lang, R., O’Reilly, M., Sigafoos, J., Lancioni, G., & Rispoli, M. (2011). Addendum to “gluten-free and casein-free diets in treatment of autism spectrum disorders: A systematic review”. Research in Autism Spectrum Disorders, Volume 5(1), pp. 86 - 88
Munde, V.S., & Vlaskamp, C. (2010). Alertness observations in children with profound intellectual and multiple disabilities. International Journal of Child Health and Human Development, Volume 3(1), pp. 115 - 124
Munde, V.S., Vlaskamp, C., Ruijssenaars, A.J.J.M., & Nakken, H. (2009a). Alertness in individuals with profound intellectual and multiple disabilities: A literature review. Research in Developmental Disabilities, Volume 30(3), pp. 462 - 480
Munde, V.S., Vlaskamp, C., Ruijssenaars, A.J.J.M., & Nakken, H. (2009b). Experts discussing “alertness in individuals with PIMD”: A Concept Mapping procedure. Journal of Developmental and Physical Disabilities, Volume 21(4), pp. 263 - 277
Munde, V.S., Vlaskamp, C., Ruijssenaars, A., Maes, B., & Nakken, H. (2010). Alertness and Snoezelen in individuals with PIMD. Journal of Applied Research in Intellectual Disabilities. Vol. 23(5), pp. 499
Munde, V.S. (2011). Attention please!. Alertness in individuals with profound intellectual and multiple disabilities. Doctoral dissertation. Rijksuniversiteit Groningen, Groningen.
Munde, V.S., Vlaskamp, C., Ruijssenaars, A.J.J.M., & Nakken, H. (2011). Determining alertness in individuals with profound intellectual and multiple disabilities: The reliability of an observation list. Education and Training in Autism and Developmental Disabilities, Volume 46(1), pp. 116 - 123
Munde, V.S., Vlaskamp, C., Post, W.J., Ruijssenaars, A.J.J.M., Maes, B., & Nakken, H. (2012). Observing and influencing alertness in individuals with profound intellectual and multiple disabilities in multisensory environments. Journal of Cognitive Education and Psychology, Volume 11(1), pp. 5 - 19
Munde, V.S, Vlaskamp, C., Vos, P., Maes, B., & Ruijssenaars, W. (2012). Physiological measurements as validation of alertness observations: An exploratory case study of three individuals with profound intellectual and multiple disabilities. Intellectual & Developmental Disabilities, Volume 50(4), pp. 300 - 310
Munde, V.S., Vlaskamp, C., Maes, B., & Ruijssenaars, A.J.J.M. (2014). Catch the wave! Time‐window sequential analysis of alertness stimulation in individuals with profound intellectual and multiple disabilities. Child: Care, Health and Development, Volume 40(1), pp. 95 - 105
Munde, V.S, & Vlaskamp, C. (2015). Initiation of activities and alertness in individuals with profound intellectual and multiple disabilities. Journal of Intellectual Disability Research, Volume 59(3), pp. 284 - 292
Munde, V.S., & Vlaskamp, C. (2015b). Vestibular stimulation and alertness in individuals with profound intellectual and multiple disabilities. European Journal of Intellectual Disability. Volume 9
Murdoch, H. (1994). "He can hear when he wants to!" Assessment of Hearing Function for People with Learning Difficulties'. Volume 22. pp. 85 - 89
Murdoch, H. (1997). Stereotyped behaviours: how should we think about them? British Journal of Special Education, Volume 24(2), pp. 71 - 75
Murdoch, H., McMinn, R., Gopsill, S., McLinden, A., & Smith, G. (2009): A curriculum for multi-sensory impaired children, MSI Unit
Victoria School Birmingham, Sense Publications
Murphy, G.H., & Oliver, C. (1987). Decreasing undesirable behaviours. In W. Yule and J. Carr (Eds.), Behaviour Modification for People with Mental Handicaps, 2nd Edn. Croom Helm, London, pp. 102 - 142
Murphy, G.H., Oliver, C., Corbett, J., Crayton, L., Hales, J., Head, D., & Hall, S. (1993). Epidemiology of self-injury, characteristics of people with severe self-injury and initial treatment outcome. In C. Kiernan (ed.), Research to Practice? Implications of Research on the Challenging Behaviour of People with Learning Difficulties. pp. 1 - 35. Kidderminster. BILD
Murphy, G.H., Hall, S., Oliver, C., & Kissi-Debra, R. (1999). Identification of early self-injurious behaviour in young children with intellectual disability. Journal of Intellectual Disability Research. Volume 43, pp. 149 - 163
Murphy, G.H., Beadle-Brown, J., Wing, L., Gould, J., Shah, A., & Holmes, N. (2005). Chronicity of challenging behaviours in people with severe intellectual disabilities and/or autism: a total population sample. Journal of Intellectual Disability Research. Volume 35, pp. 405 – 418
Murphy, J., & Cameron, L. (2008). The effectiveness of Talking Mats with people with intellectual disability. British Journal of Learning Disabilities, Volume 36(4), pp. 232 - 241
Murphy, K.M., Saunders, M.D., Saunders, R.R., & Olswang, L.B. (2004). Effects of ambient stimuli on measures of bio-behavioral state and microswitch use in adults with profound multiple impairments, Research in Developmental Disabilities, Volume 25(4), pp. 355 - 370
Musselwhite, C.R., & St. Louis, K.W. (1988). Communication programming for persons with severe handicaps: Vocal and augmentative
strategies. San Diego: College-Hill Press
Nackley, V.L. (2001). Sensory diet applications and environmental modifications: A winning combination. Sensory Integration Special Interest Section Quarterly, Volume 24(1), pp. 1 - 4
Nafstad, A., & Rødbroe, I. (1999). Co-creating communication: Perspectives on diagnostic education for individuals who are congenitally deafblind and individuals whose impairments may have similar effects. Nord-Press.
Naish, L., Bell, J., & Clunies-Ross, L. (2004). Exploring access: how to audit your school environment, focusing on the needs of pupils who have multiple disabilities and visual impairment. RNIB
Nakken, H., & Vlaskamp, C. (2002). Joining forces: Supporting individuals with profound multiple learning disabilities. Tizard Learning Disability Review, Volume 7(3), pp. 10 - 15
Nakken, H., & Vlaskamp, C. (2007). A need for a taxonomy for profound intellectual and multiple disabilities. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(2), pp. 83 - 87
Narayan, J., Madhavan, T., Suryaprakasham, B. (1993). Self-awareness of people with mental handicap. International Journal of Rehabilitation Research. Volume 16(1), pp. 59 - 63
National Scientific Council on the Developing Child. (2005/2014). Excessive Stress Disrupts the Architecture of the Developing Brain: Working Paper 3. Center on the Developing Child at Harvard University
Nazni, P., Wesely, E., & Nishadevi, V. (2008). Impact of casein and gluten free dietary intervention on selected autistic children. Iranian Journal of Pediatrics, Volume 18(3), pp. 244 - 250
NCAC (2011). Making sense of it all – young children and sensory processing. Putting Children First. The magazine of the National Childcare Accreditation Council (NCAC). Volume 38. pp. 18 - 20
Neely-Barnes, S., Marcenko, M., & Weber, L. (2008). Does choice influence quality of life for people with mild intellectual disabilities? Intellectual and Developmental Disabilities, Volume 46, pp.12 – 26
Neerinckx, H., Vos, P., Van Den Noortgate, W., & Maes, B. (2014). Temporal analysis of attentional processes in spontaneous interactions between people with profound intellectual and multiple disabilities and their support workers. Journal of Intellectual Disability Research, Volume 58(8), pp. 721 - 733
Neerinckx, H., & Maes, B. (2016). Joint attention behaviours in people with profound intellectual and multiple disabilities: the influence of the context. Journal of Applied Research in Intellectual Disabilities, Volume 29(6), pp. 574 - 584
Nelson, C., van Dijk, J., & McDonnell, A. (2001). Child-guided Strategies for Understanding Children who are Deaf-blind or have Severe Multiple Disabilities: The van Dijk Approach to Assessment on Child-guided Strategies for Assessing Children who are Deaf-blind or have
Multiple Disabilities, C. Nelson & J. van Dijk. CD-ROM from Aap Noot Muis Productions/Instituut voor Doven/Cidv, Netherlands.
Nelson, C., van Dijk, J., McDonnell, A.P., & Thompson, K. (2002). A framework for understanding young children with severe and multiple disabilities: The van Dijk approach to assessment. Research and Practice for Persons with Severe Disabilities, Volume 27(2), pp. 97 - 111
Nelson, D., Anderson, V., & Gonzales, A. (1984). Music activities as therapy for children with autism and other pervasive developmental disorders. Journal of Music Therapy, Volume 21(3), pp. 100 - 116
Nelson, K. (2005). Emerging levels of consciousness in early human development. In H.S. Terrace & J. Metcalfe (Eds.), The missing link in cognition: Origins of self-reflective consciousness. Oxford: Oxford University Press, pp. 116–141
Neuman, C.J., & Hill, S.D. (1978). Self-recognition and stimulus preference in autistic children. Developmental Psychobiology, Volume 11, pp. 571 - 578
Newman, I., & Emerson, E. (1991). Specialised treatment units for people with challenging behaviours. Mental Handicap, Volume 19(3), pp. 113 - 119
Newton, J.S., Horner, R.H., & Lund, L. (1991). Honoring activity preferences in individualized plan development: A descriptive analysis. Journal of The Association for Persons with Severe Handicaps, Volume 16, pp. 207 - 212
Nguyen, T. (2010). Total number of synapses in the adult human neocortex. Undergraduate Journal of Mathematical Modeling: One+ Two, Volume 3(1), pp. 1 -13
Nicholls, T. (2002). Could I Play a Different Role?: Group Music Therapy with Severely Learning Disabled Adolescents. In - A. Davies & E. Richards (Eds.), Music Therapy and Group Work: Sound Company, pp. 231 - 246. London: Jessica Kingsley
Nielsen, L. (1979). The Comprehending Hand. Copenhagen: Socialstyrelsen.
Nielsen, L. (1990). Are you Blind? Promotion of the Development of Children who are Especially Developmentally Threatened. Copenhagen: Sikon.
Nielsen, L. (1991). Spatial relations in congenitally blind infants: a study. Journal of Visual Impairment and Blindness, Volume 85, pp. 11 - 16
Nielsen, L. (1992). Space and Self-Active learning by means of the Little Room. Copenhagen: Sikon.
Nielsen, L. (1993). Early Learning Step by Step. Copenhagen: Sikon.
Nijs, S., Penne, A., Vlaskamp, C., & Maes, B. (2016). Peer Interactions among Children with Profound Intellectual and Multiple Disabilities during Group Activities. Journal of Applied Research in Intellectual Disabilities, Volume 29(4), pp. 366 - 377
Nijs, S., Vlaskamp, C., & Maes, B. (2016). Children with PIMD in interaction with peers with PIMD or siblings. Journal of Intellectual Disability Research, Volume 60(1), pp. 28 - 42
Nijs, S., Vlaskamp, C., & Maes, B. (2016b). The nature of peer‐directed behaviours in children with profound intellectual and multiple disabilities and its relationship with social scaffolding behaviours of the direct support worker. Child: Care, Health and Development, Volume 42(1), pp. 98 - 108
Nind, M., & Hewett, D. (1988). Interaction as Curriculum, British Journal of Special Education, Volume 15(2), pp. 55 - 57
Nind, M., & Hewett, D. (1989). Teaching pupils with very severe learning difficulties by means of Intensive Interaction: some typical questions and answers, Portage Into the Nineties Papers from the 1989 National Portage Association Conference. The National Portage Association.
Nind, M. (1993). Access to Communication: Efficacy of Intensive Interaction Teaching for people with severe developmental disabilities who demonstrate ritualistic behaviours. Ph.D Thesis, Cambridge Institute of Education.
Nind, M., & Hewett, D. (1994). Access to communication - developing the basics of communication with people with severe learning
difficulties. David Fulton
Nind, M. (1996). Efficacy of Intensive Interaction: developing sociability and communication in people with severe and complex learning difficulties using an approach based on caregiver-infant interaction’, European Journal of Special Needs Education, Volume 11(1), pp.48 - 66
Nind, M., & Hewett, D. (1996). When age-appropriateness isn't appropriate, in Coupe-O'Kane, J & Goldbart, J. (eds) Whose choice? London: David Fulton.
Nind, M. (2000). Teachers understanding of interactive approaches in special education, International Journal of Disability, Development and Education, Volume 47(2), pp.184 - 199
Nind, M. (2000). Intensive Interaction and children with autism, in Powell, S. (ed) Helping Children with Autism to Learn. London: David Fulton.
Nind, M. & Powell, S. (2000). Intensive Interaction and autism: some theoretical concerns, Children and Society, Volume 14(2), pp.98 - 109
Nind, M. & Kellett, M. (2002). Responding to learners with severe learning difficulties and stereotyped behaviour: challenges for an inclusive era, European Journal of Special Needs Education, Volume 17(3), pp.265 - 282
Nind, M., Kellett, M. & Hopkins, V. (2001). Teachers’ talk styles: communication with learners with severe learning difficulties, Child Language, Teaching and Therapy, Volume 17(2), pp.143 - 159
Nind, M. & Kellett, M. (2002). Response to James Hogg, Juliet Goldbart and John Harris re 'Responding to individuals with severe learning difficulties and stereotyped behaviour: challenges for an inclusive era’, European Journal of Special Needs Education, Volume 17(3), pp. 299 - 300
Nind, M. & Cochrane, S. (2002). Inclusive curricula? Pupils on the margins of special schools, International Journal of Inclusive Education, Volume 6(2), pp.185 - 198
Nind, M. (2003). Enhancing the communication learning environment of an early years unit through action research, Educational Action Research, Volume 11(3), pp.347 - 363
Nissen, J.M.J.F., & Haveman, M.J. (1997). Mortality and avoidable death in people with severe self-injurious behaviour: Results of a Dutch study. Journal of Intellectual Disability Research, Volume 41, pp. 252 - 257
Nordoff, P., & Robbins, C. (1965). Music Therapy for Handicapped Children: Investigations and Experiences. New York: Rudolf Steiner Publications.
Nordoff, P., & Robbins, C. (1971). Therapy in Music for Handicapped Children. London: Gollancz.
Nordoff, P., & Robbins, C. (1977). Creative Music Therapy: Individualized Treatment for the Handicapped Child. New York: John Day & Co.
Northern Ireland Curriculum (2012). Quest For Learning
Norton, Y. (1975). Neuro-development and sensory integration for the profoundly retarded multiply handicapped child. American Journal of Occupational Therapy, Volume 29, pp. 93 - 100
Nota, L., Ferrari, L., Soresi, S., & Wehmeyer, M.L. (2007). Self determination, social abilities, and the quality of life of people with intellectual disabilities. Journal of Intellectual Disability Research, Volume 51, pp. 850 – 865
Nozaki, K., & Mochizuki, A. (1995). Assessing Choice Making of a Person With Profound Disabilities: A Preliminary Analysis. Journal of The Association for Persons with Severe Handicaps. Volume 20(3), pp. 196 - 201
Nunez, M. (2014). Joint attention in deafblind children: a multisensory path towards a shared sense of the world. Sense Research.
O’Brien, J. (2000). Self-determination—with strings attached. Mouth, Volume 10(5), pp. 36
O’Brien, Y., Glenn, S., & Cunningham, C. (1994). Contingency Awareness in Infants and Children with Severe and Profound Learning Disabilities, International Journal of Disability, Development and Education, Volume 41(3), pp. 231 - 243
O'Haire, M.E. (2010). Companion animals and human health: Benefits, challenges, and the road ahead. Journal of Veterinary Behavior: Clinical Applications and Research. Volume 5, pp. 226 – 234
O'Haire, M.E. (2012). Animal-assisted intervention for autism spectrum disorder: A systematic literature review. Journal of Autism and Developmental Disorders, Volume 43(7), pp. 1606 - 1622
O’Haire, M.E., McKenzie, S.J., Beck, A.M., & Slaughter, V. (2013). Social behaviors increase in children with autism in the presence of animals compared to toys. PLoS ONE, Volume 8(2), pp. N/A
O’Haire, M.E., McKenzie, S.J., McCune, S., & Slaughter, V. (2013). Effects of animal-assisted activities with guinea pigs in the primary school classroom. Anthrozoös: A Multidisciplinary Journal of the Interactions of People and Animals, Volume 26(3), pp. 445 - 458
O’Haire, M.E., McKenzie, S.J., Beck, A.M., & Slaughter, V. (2015). Animals may act as social buffers: Skin conductance arousal in children with autism spectrum disorder in a social context. Developmental Psychobiology, Volume 57(5), pp. 584 - 595
O’Reilly, M.F., & Lancioni, G. (2000). Response covariation of escape-maintained aberrant behaviour correlated with sleep deprivation. Research in Developmental Disabilities. Volume 21, pp. 125 – 136
Oakley, M. (1991). Quoted in ‘The Hidden Handicap’ by Darby S. Times Educational Supplement (No.3930), October 25 1991, page 38
Ockelford, A. (2000). Music in the Education of Children with Severe or Profound Learning Difficulties: Issues in Current UK Provision, a New Conceptual Framework, and Proposals for Research. Psychology of Music, Volume 28, pp.197 - 217
Ockelford, A., Welch, G., & Zimmermann, S. (2002). Music education for pupils with severe or profound and multiple difficulties - current provision and future need. British Journal of Special Education, Volume 29(4), pp. 178 - 192
Ockelford, A. (2008). Music for Children and Young People with Complex Needs. Oxford: Oxford University Press.
Ockelford, A. (2009). Sounds of intent. Information Exchange, Volume 79, pp. 6 - 7
Ockelford, A. (2012). Songs Without Words: Exploring How Music Can Serve as a Proxy Language in Social Interaction with Autistic Children. In - R. MacDonald, G. Kreutz, & L. Mitchell (Eds.), Music, Health, and Well-being, pp. 289 - 323. Oxford: Oxford University Press.
Ockelford, A., & Markou, K. (2012). Music Education and Therapy for Children and Young People with Cognitive Impairments: Reporting on a Decade of Research. In R. MacDonald, G. Kreutz & L. Mitchell (Eds.), Music, Health, and Well-being, pp. 383 - 404. Oxford: Oxford University Press.
Ockelford, A., & Welch, G. (2012). Mapping Musical Development in Learners with the Most Complex Needs: The Sounds of Intent Project. In - G. McPherson & G. Welch (Eds.), The Oxford Handbook of Music Education, Volume 2, pp. 11 - 30. Oxford: Oxford University Press.
Ojemann, G. (1986). Brain mechanisms for consciousness and conscious experience. Canadian Psychology, Volume 27, pp. 158 – 168
Oldfield, A, & Adams, M. (1990). The Effects of Music Therapy on a Group of Profoundly Mentally Handicapped Adults. Journal of Mental Deficiency Research, Volume 34, pp. 107 - 124
Oliver, C., Murphy, G.H., & Corbett, J.A. (1987). Self injurious behaviour in people with mental handicap: a total population survey. Journal of Mental Deficiency Research. Volume 31. pp. 147 - 162
Oliver, C., & Head, D. (1990). Self-injurious behaviour in people with learning difficulties: Determinants and interventions. International Review of Psychiatry, Volume 2, 101 - 116
Oliver, C. (1991a). The application of analogue methodology to the functional analysis of challenging behaviour. In B. Remington (Ed.), The Challenge of Severe Mental Handicap: A Behaviour Analytic Approach. John Wiley and Sons, Chichester, pp. 97 - 118
Oliver, C. (1991b). Self-injurious Behaviour in People with Mental Handicap: Prevalence, Individual Characteristics and Functional Analysis, unpublished Ph.D. Thesis, University of London.
Oliver, C. (1993). Self-injurious behaviour: from response to strategy. In C. Kiernan (Ed.), Research to Practice? Implications of Research on the Challenging Behavour of People with Learning Disabilities. pp. 135 - 188. Kidderminster; British Institute of Learning Disabilities
Oliver C., McClintock K., Hall S., Smith M., Dagnan D. & Stenfert-Kroese B. (2002). Assessing the severity of challenging behaviour: psychometric properties of the challenging behaviour interview. Journal of Applied Research in Intellectual Disabilities, Volume 16, pp. 53 – 61
Oliver, C., Moss, J., Petty, J., Arron, K., Sloneem, J., & Hall, S. (2003). Self-injurious behaviour in Cornelia de Lange Syndrome A Guide for Parents and Carers. Coventry: Trident Communication Ltd.
Oliver, C. (2004). The neglect of psychological disorder in people with severe and profound intellectual disability. Journal of Intellectual Disability Research, Volume 48(4-5), pp. 360
Oliver, C., Sloneem, J., Hall, S., & Arron, K. (2009). Self‐injurious behaviour in Cornelia de Lange syndrome: 1. Prevalence and phenomenology. Journal of Intellectual Disability Research, Volume 53(7), pp. 575 - 589
Oliver, C., & Richards, C. (2010). Self-injurious behaviour in people with intellectual disability. Current Opinion in Psychiatry, Volume 23(5), pp. 412 – 416
Oliveros, P., Miller, L., Heyen, J., Siddall, G., & Hazard, S. (2011). A musical improvisation interface for people with severe physical disabilities. Music and Medicine, Volume 3(3), pp. 172 - 181
Olney, M.F. (2001). Communication strategies of adults with severe disabilities: Supporting self-determination. Rehabilitation Counseling Bulletin. Volume 44 (2), pp. 88 - 91
Olsson, C. (2004). Dyadic interaction with a child with multiple disabilities: A system theory perspective on communication. Augmentative and Alternative Communication, Volume 20(4), pp. 228 - 242
Orita, M., Hayashida, N., Shinkawa, T., Kudo, T., Koga, M., Togo, M., Katayama S, Hiramatsu K, Mori S, & Takamura, N. (2012). Monitoring the autonomic nervous activity as the objective evaluation of music therapy for severely and multiply disabled children. The Tohoku Journal of Experimental Medicine, Volume 227(3), pp. 185 - 189
Orelove, F.P., & Sobsey, D. (1987). Educating children with multiple disabilities: A transdisciplinary approach. Baltimore: Paul H. Brookes
Ottenbacher, K. (1982). Sensory Integration Therapy: Affect or Effect? American Journal of Occupational Therapy, Volume 36(9), pp. 571 - 578
Ottenbacher, K., & Short, M.A. (1985). Sensory integrative dysfunction in children: A review of theory and treatment. Advances in Developmental and Behavioral Pediatrics, Volume 6, pp. 287 – 329
Ouvry, C. (1987). Educating Children with Profound Handicaps. British Institute of Mental Handicap, Kidderminster
Oviedo, G.R., Travier, N., & Guerra-Balic, M. (2017). Sedentary and physical activity patterns in adults with intellectual disability. International Journal of Environmental Research and Public Health, Volume 14(9), 14 pages
Owen, M.T., Ware, A.M., & Barfoot, B. (2000). Caregiver-mother partnership behavior and quality of caregiver-child and mother-child interactions. Early Childhood Research Quarterly, Volume 15, pp. 413 – 428
Owens, T.J., Mortimer, J.T & Finch, M.D. (1996) Self determination as a source of self esteem in adolescence. Social Forces, Volume 74 (4) pp. 1377 - 1404
Pace, G.M., Ivancic, M.T., Edwards, G.L., Iwata, B.A., & Page, T.J. (1985). Assessment of stimulus preference and reinforcer value with profoundly retarded individuals. Journal of Applied Behavior Analysis, Volume 18, pp. 249 – 255
Pagliano, P. (1998). Multi-sensory environment: an open-minded space. British Journal of Visual Impairment. Volume 16(3), pp. 105 - 109
Pagliano, P. (2001). Using a Multisensory Environment: A Practical Guide for Teachers. David Fulton
Pagliano, P. (2007). Where next for multisensory environments? Insight. Volume 10, pp. 36 - 38
Pagliano, P., & Cook, J. (2007). Understanding and using multisensory environments. Insight, Volume 11, pp. 30 - 31
Pagliano, P. (2007). Pleasure, happiness and learning in the multisensory environment. Insight. Volume 12, pp. 32 - 33
Pagliano, P. (2012). The Multisensory Handbook: A guide for children and adults with sensory learning disabilities. Routledge
Palmer, S.B. (2010). Self-determination: A life-span perspective. Focus on Exceptional Children, Volume 42 (6), pp. 1 – 16
Palmer, S.B., Wehmeyer, M.L., Shogren, K.A., Williams-Diehm, K., & Soukup, J. (2012). An evaluation of the Beyond High School model on the self-determination of students with intellectual disability. Career Development for Exceptional Individuals, Volume 35(2), pp. 76 – 84
Para-Cremer, J.A. (2008). The effects of staff training on the level of engagement with individuals with developmental disabilities within two day-habilitation settings. Masters thesis, University of Kansas
Paradiso, S., Andreasen, N.C., O'leary, D.S., Arndt, S., & Robinson, R.G. (1997). Cerebellar size and cognition: correlations with IQ, verbal memory and motor dexterity. Cognitive and Behavioral Neurology, Volume 10(1), pp. 1 - 8
Parham, L.D., & Mailloux, Z. (2005). Sensory integration. In J. Case-Smith, A.S. Allen, & P.N. Pratt (Eds.), Occupational Therapy for Children (5th ed., pp. 356 – 411). St. Louis, MO: Mosby.
Parham, L.D., Cohn, E.S., Spitzer, S., Koomar, J.A., Miller, L.J., Burke, J.P., Brett-Green, B., Mailloux, Z., May-Benson, T.A., Smith Roley, S., Schaaf, R.C., Schoen, S.A., & Summerset, C.A. (2007). Fidelity in sensory integration intervention research. American Journal of Occupational Therapy, Volume 61, pp. 216 – 227
Parsons, M.B., & Reid, D.H. (1990). Assessing food preferences among persons with profound mental retardation: Providing opportunities to make choices. Journal of Applied Behavior Analysis, Volume 23, pp. 183 - 195
Parsons, M.B., & Reid, D.H. (1993). Evaluating and improving residential treatment during group leisure situations: A program replication and refinement. Research in Developmental Disabilities, Volume 14(1), pp. 67 - 85
Parsons, M.B., Reid, D.H., & Green, C.W. (1993). Preparing direct service staff to teach people with severe disabilities: A comprehensive evaluation of an effective and acceptable training program. Behavioral Residential Treatment, Volume 8(3), pp. 163 - 185
Parsons, M.B., & Reid, D.H. (1995). Training residential supervisors to provide feedback for maintaining staff teaching skills with people who have severe disabilities. Journal of Applied Behavior Analysis, Volume 28(3), pp. 317 - 322
Parsons, M.B., Harper, V.N., Jensen, J.M., & Reid, D.H. (1997). Assisting older adults with severe disabilities in expressing leisure preferences: A protocol for determining choice-making skills. Research in Developmental Disabilities, Volume 18, pp. 113 – 126
Parsons, M.B., Reid, D.H., & Green, C.W. (1998). Identifying work preferences prior to supported work for an individual with multiple severe disabilities including deaf-blindness. Journal of the Association for Persons with Severe Handicaps, Volume 23, pp. 329 – 333
Parsons, M.B., Rollyson, J.H., & Reid, D.H. (2004). Improving day-treatment services for adults with severe disabilities: a norm-referenced application of outcome management. Journal of Applied Behavior Analysis, Volume 37(3), pp. 365 - 377
Parsons, M.B., Reid, D.H., Towery, D., & Darden, M. (2008). Remediating minimal progress on teaching programs by adults with severe disabilities in a congregate day setting. Behavior Analysis in Practice, Volume 1(2), pp. 59 - 67
Parsons, M.B., Rollyson, J.H., & Reid, D.H. (2012). Evidence-based staff training: A guide for practitioners. Behavior Analysis in Practice, Volume 5(2), pp. 2 - 11
Parsons, R., Reid, D., Reynolds, J., & Bumgarner, M. (1990). Effects of chosen versus assigned jobs on the work performance of persons with severe handicaps. Journal of Applied Behavior Analysis, Volume 23, pp. 253 – 258
Parush, S., Kaitz, M., Sohmer, H., & Steinberg, A. (1991).Electrophysiological and behavioral correlates of tactile defensiveness. Paper presented at the national conference of the American Occupational Therapy Association, Cincinnati, OH.
Parush, S., Sohmer, H., Steinberg, A. & Kaitz, M. (2007). Somatosensory function in boys with ADHD and tactile defensiveness. Physiology & Behavior, Volume 90(4), pp. 553 - 558
Pase, M.P., Himali, J.J., Beiser, A.S., Aparicio, H.J., Satizabal, C.L., Vasan, R.S., Seshadri, S., & Jacques, P.F. (2017). Sugar and Artificially Sweetened Beverages and the Risks of Incident Stroke and Dementia: A Prospective Cohort Study. Stroke. Volume 48(5). pp. 1139 - 1146
Pase, M.P., Himali, J.J., Jacques, P.F., DeCarli, C., Satizabal, C.L., Aparicio, H., Vasan, R.S., Beiser, A.S., & Seshadri, S. (2017). Sugary beverage intake and preclinical Alzheimer's disease in the community. Alzheimer's & Dementia. Volume 13(9). pp. 955 – 964
Patterson, F.G. (1978a). The gestures of a gorilla: language acquisition in another pongid. Brain and Language, Volume 5, pp. 72 - 97
Patterson, F.G. (1978b). Conversations with a gorilla. National Geographic. Volume 154(4), pp. 438 - 465
Patterson, F.G. (1978c). Human communication with gorillas. In - The spirit of enterprise, Stone, G. (Ed.), pp. 182 - 186. San Francisco: Freeman
Patterson, F.G. (1979a). Linguistic capabilities of a lowland gorilla. Unpublished doctoral dissertation
Patterson, F.G. (1979b). Linguistic capabilities of a lowland gorilla. In - Language intervention from ape to child. Schiefelbusch, R. & Hollis, J. (Eds.), pp. 325 - 356. Baltimore: University Park Press
Patterson, F.G. (1980a). Innovative uses of language by a gorilla: A case study. In - Children's Language, Volume 2. Nelson, K. (Ed.), pp. 497 - 561. New York: Gardner Press
Patterson, F.G. (1980b). In search of man: Experiments in primate communication. Michigan Quarterly Review. Volume 19, pp. 94 - 114
Patterson, F.G. (1981a). Can an ape create a sentence? Some affirmative evidence. Science, Volume 211, pp. 86 - 87
Patterson, F.G. (1981b). Ape language. Science, Volume 211: pp. 86 - 87
Patterson, F.G., & Linden, E. (1981). The education of Koko. New York: Holt, Reinhart and Winston
Patterson, F.G. (1985a). Direct-mail funding solicitation letter. Washington: The Gorilla Foundation
Patterson, F.G. (1985b). Koko's kitten. New York: Scholastic
Patterson, F.G. (1987). Koko's story. New York: Scholastic
Pavlides, M. (2008). Animal-assisted Interventions for Individuals with Autism. London: Jessica Kingsley Publishers.
Pawson, C., Gardner, M.R, Doherty, S., Martin, L., Soares, R., Edmonds, C.J. (2013). Drink Availability is Associated with Enhanced Examination Performance in Adults. Psychology Teaching Review. Volume 19. pp. 57 - 66
Pease, L. (2008). Curriculum success for learners with complex needs. Insight. Volume 13, pp. 10 - 13
Pechacek, T.F., Bell, K.F., Cleland, C.C., Baum, C., & Boyle, M. (1973). Self-recognition in profoundly retarded males, Bulletin of the Psychonomic Society. Volume 1, pp. 328 - 330
Pedersen, L., Parlar, S., Kvist, K., Whiteley, P., & Shattock, P. (2014). Data mining the ScanBrit study of a gluten-and casein-free dietary intervention for children with autism spectrum disorders: behavioural and psychometric measures of dietary response. Nutritional Neuroscience, Volume 17(5), pp. 207 - 213
Pellitteri, J. (2000). Music therapy in the special education setting. Journal of Educational and Psychological Consultation, Volume 11(3&4), pp. 379 - 391
Pennesi, C.M., & Klein, L.C. (2012). Effectiveness of the gluten-free, casein-free diet for children diagnosed with autism spectrum disorder: based on parental report. Nutritional Neuroscience, Volume 15(2), pp. 85 - 91
Perkins, E.A. (2007). Self- and proxy reports across three populations: Older adults, persons with Alzheimer’s disease, and persons with intellectual disabilities. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(1), pp. 1 - 10
Perretta, L. (2001). Brain Food. Hamlyn Publishers
Perrig, W.J., Hollenstein, M., & Oelhafen, S. (2009). Can we improve fluid intelligence with training on working memory in persons with intellectual disabilities. Journal of Cognitive Education and Psychology, Volume 8(2), pp. 148 - 164
Perry, M. (2003). Relating improvisational music therapy with severely and multiply disabled children to communication development. Journal of Music Therapy, Volume 40(3), pp. 227 - 246
Peterson, J.J., Janz, K.F., & Lowe, J.B. (2008). Physical activity among adults with intellectual disabilities living in community settings. Preventive Medicine, Volume 47, pp. 101 – 106
Petkova, V.I., & Ehrsson, H.H. (2008). If I were you: Perceptual illusion of body swapping. PloS one, Volume 3(12), e3832
Petri, N.M., Dropulić, N., & Kardum, G. (2006). Effects of Voluntary Fluid Intake Deprivation on Mental and Psychomotor Performance. Croatian Medical Journal. Volume 47(6). pp. 855 – 861
Petry, K., Maes, B., & Vlaskamp, C. (2001). Developing a procedure for evaluating quality of life for people with profound and multiple disabilities. Tizard Learning Disability Review, Volume 6(2), pp. 45 - 48
Petry, K., Maes, B., & Vlaskamp, C. (2005). Domains of quality of life of people with profound multiple disabilities: the perspective of parents and direct support staff, Journal of Applied Research in Intellectual Disabilities, Volume 18(1), pp. 35 – 46
Petry, K., & Maes, B. (2006). Identifying expressions of pleasure and displeasure by persons with profound and multiple learning disabilities Journal of Intellectual & Developmental Learning Disability, Volume 31(1), pp. 28 – 38
Petry, K., Maes, B., & Vlaskamp, C. (2007a). Operationalizing quality of life for people with profound multiple disabilities: a Delphi study. Journal of Intellectual Disability Research, Volume 51(5), pp. 334 - 349
Petry, K., Maes, B., & Vlaskamp, C. (2007b). Support characteristics associated with the quality of life of people with profound intellectual and multiple disabilities: The perspective of parents and direct support staff. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(2), pp. 104 - 110
Petry, K., & Maes, B., & Vlaskamp, C. (2007c). Description of the support needs of people with profound multiple disabilities using the 2002 AAMR system: An overview of literature. Education and Training in developmental Disabilities, pp. 130 - 143
Petry, K., Maes, B., & Vlaskamp, C. (2007d). Service features associated with quality of support for people with profound intellectual disability and complex health care needs: The perspective of parents and direct support staff. Journal of Policy and Practice in Intellectual Disabilities, Volume 4, pp. 104 - 110
Petry, K., Maes, B., & Vlaskamp, C. (2009). Measuring the quality of life of people with profound multiple disabilities using the QOL-PMD: First results. Research in Developmental Disabilities, Volume 30(6), pp. 1394 - 1405
Pfeiffer, B., & Kinnealey, M. (2003). Treatment of sensory defensiveness in adults. Occupational Therapy International, Volume 10, pp. 175 – 184
Philippi, C.L., Feinstein, J.S., Khalsa, S.S., Damasio, A., Tranel, D., Landini, G., Williford, K., & Rudrauf, D. (2012) Preserved Self-Awareness following Extensive Bilateral Brain Damage to the Insula, Anterior Cingulate, and Medial Prefrontal Cortices. PLoS ONE, Volume7(8): e38413.
Piaget, J. (1952). The origins of intelligence in children. New York: Norton
Piazza, C.C., Fisher, W.W., & Kahng, S.W. (1996). Sleep patterns in children and young adults with mental retardation and severe behaviour disorders. Developmental Medicine and Child Neurology. Volume 38, pp. 335 – 344
Pierson, M.R., Carter, E.W., Lane, K.L., & Glaeser, B.C. (2008). Factors influencing the self-determination of transition-age youth with
high-incidence disabilities. Career Development for Exceptional Individuals, Volume 31(2), pp. 115 – 125
Pinkney, L. (2001). Multisensory environments. Eye Contact, Volume 31, pp. 24 - 26
Place, K., & Hodge, S.R. (2001): Social Inclusion of Students With Physical Disabilities in General Physical Education: A Behavioral Analysis. Adapted Physical Activity Quarterly, Volume 18; pp, 389 - 404
Plotnik, J.M., de Waal, F.B.M., Moore, D., & Reiss, D. (2010). Self-recognition in the Asian elephant and future directions for cognitive research with elephants in zoological settings. Zoo Biology, Volume 29, pp. 179 – 191
Podboy, J.W., & Mallory, W.A. (1977). Caffeine reduction and behavior change in the severely retarded. Mental Retardation, Volume 15(6), pp. 40
Polatajko, H. J., Law, M., Miller, J., Schaffer, R., & Macnab, J. (1991). The effect of a sensory integration program on academic
achievement, motor performance, and self-esteem in children identified as learning disabled: Results of a clinical trial. Occupational Therapy
Journal of Research, Volume 11, pp. 155 - 176
Polatajko, H.J., Kaplan, B., & Wilson, B. (1992). Sensory integration treatment for children with learning disabilities: Its status 20 years
later. Occupational Therapy Journal of Research, Volume 12, pp. 323 - 341
Polednak, A. (1977). Post-mortem neuropathology in a mentally retarded population. The Lancet, Volume 309(8009), pp. 492 - 493
Poppes, P., van der Putten, A.A., & Vlaskamp, C. (2010). Frequency and severity of challenging behaviour in people with profound intellectual and multiple disabilities. Research in Developmental Disabilities, Volume 31(6), pp. 1269 - 1275
Poppes, P., van der Putten, A.A., & Vlaskamp, C. (2014). Addressing challenging behaviour in people with profound intellectual and multiple disabilities: Analyzing the effects of daily practice. Journal of Policy and Practice in Intellectual Disabilities, Volume 11(2), pp. 128 – 136
Porter, J., & Lacey, P. (1999). What Provision for Pupils with Challenging Behavior? A Report of a Survey of Provision and Curriculum Provided for Pupils with Learning Difficulties and Challenging Behaviour. British Journal of Special Education. Volume 26(1), pp. 23 - 28
Porter, J., Ouvry, C., Morgan, M., & Downs, C. (2001). Interpreting the communication of people with profound and multiple learning difficulties. British Journal of Learning Disability, Volume 29(1), pp. 12 - 16
Postman, N. (1969). Teaching as a Subversive Activity. Delacorte Press
Powers, L.E., Geenen, S., Powers, J., Pommier-Satya, S., Turner, A., Dalton, L., & Swand, P. (2012). My life: Effects of a longitudinal, randomized study of self-determination enhancement on the transition outcomes of youth in foster care and special education. Children and Youth Services Review, Volume 34, pp. 2179 – 2187
Price, A. (1977). Nationally Speaking - Sensory integration in occupational therapy. American Journal of Occupational Therapy. Volume 31, pp. 287 - 289
Prior, H., Schwarz, A., & Guentuerkuen, O. (2008). Mirror-induced behavior in the magpie (Pica pica): evidence of self-recognition. PLoS
Biology, Volume 6, pp. 1642 – 1650
Prior, M., Minnes, P., Coyne, T., Golding, B., Hendy, J., & McGillivary, J. (1979). Verbal interactions between staff and residents in an institution for the young mentally retarded. Mental Retardation. Volume 17, pp. 65 – 69
Pross, N., Demazieres, A., Girard, N., Barnouin, R., Santoro, F., Chevillotte, E., Klein, A, & Le, B.L. (2013) Influence of progressive
fluid restriction on mood and physiological markers of dehydration in women. British Journal of Nutrition. Volume 109. pp. 313 - 321
Pross, N., Demazieres, A., Girard, N., Barnouin, R., Metzger, D., Klein, A., Perrier, E., & Guelinckx, I. (2014). Effects of changes in
water intake on mood of high and low drinkers. PLoS One. Volume 9: e94754
Psaltopoulou, D., Micheli, M., & Kavardinas, N. (2012). Music Therapy Enhances Perceptive and Cognitive Development in People with
Disabilities. A Quantitative Research. Proceedings of the 12th International Conference on Music Perception and Cognition and the 8th Triennial Conference of the European Society for the Cognitive Sciences of Music, July 23 - 28, 2012, Thessaloniki, Greece. pp. 824 - 833
Pugh, D. (2011a). Water and Educating Your Child. http://braincompatibleeducation.com/
Pugh, D. (2011b). The Owner's Guide to the Teenage Brain. BookPal
Pulsifer, M.B. (1996). The neuropsychology of mental retardation. Journal of the International Neuropsychological Society, Volume 2(2), pp. 159 - 176
Quest For Learning (2007). Guidance Booklet. The Council for Curriculum, Examinations & Assessment
Quest For Learning (2009): Guidance and Assessment Materials: Profound and Multiple Learning Difficulties. Northern Ireland Curriculum
Questad, K. & Cullinen, T. (1987). A reinforcer driven, data base rehabilitation program for severely brain injured adults. Archives of Physical Medicine and Rehabilitation, Volume 68, pp. 674
Quigley, S.P., & Kretchmer, R.E. (1982). The education of deaf children: Issues, Theory, and Practice. London: Edward Arnold
Quine, L. (1991). Sleep problems in children with mental handicap. Journal of Mental Deficiency Research. Volume 35(4), pp. 269 – 290
Quine, L. & Wade, K. (1991). Sleep Problems In Children with Severe Learning Difficulties: An Examination and An Intervention Trial. Final Report to Rowntree Foundation, University of Kent, Canterbury
Quine, L. (1992). Severity of sleep problems in children with severe learning difficulties: description and correlates. Journal of Community & Applied Social Psychology, Volume 2(4), pp. 247 - 268
Quine, L. (2001). Sleep problems in primary school children: comparison between mainstream and special school children. Child: Care, Health and Development, Volume 27(3), pp. 201 - 221
Quine, N., & Pahl, J. (1985). Examining the causes of stress in families with mentally handicapped children. British Journal of Social Work, Volume 15, pp. 501 - 517
Quine, N., & Pahl, J. (1991). Stress and coping in mothers caring for a child with severe learning difficulties: A test of Lazarus's transactional model of coping. Journal of Communityand Applied Psychology, Volume 1, pp. 57 - 70
Qureshi, H. (1992). Young adults with learning difficulties and challenging behaviour: parents' views of services in the community. Social Work and Social Services Review, Volume 3, pp. 104 - 123
Qureshi, H., & Alborz, A. (1992). The epidemiology of challenging behaviour. Mental Handicap Research, Volume 5, pp. 130 - 145
Qureshi, H. (1993). Prevalence of challenging behaviour in adults. In I. Fleming & B. Stenfert Kroese (eds.), People with Learnign Disability and Severe Challenging Behaviour: New Developments in Services and Therapy. Manchester University Press
Qureshi, H. (1994). The size of the problem. In E. Emerson, P. McGill, & J. Mansell (Eds.), Severe Learning Disabilities and Challenging Behaviour: Designing HighQuality Services. London: Chapman and Hall.
Raab, M., & Dunst, C.J. (1997). Extended benefits of active learning for young children with severe disabilities. Presentation at the International Conference on Children with Special Needs, New Orleans, LA. November 1997
Raab, M., Dunst, C.J., Wilson, L.L., & Parkey, C. (2009). Early Contingency Learning and Child and Teacher Concomitant Social–Emotional Behavior, International Journal of Early Childhood Special Education, Volume 1 (1), pp. 1 -14
Rainey P.M.M. (2003). Relating improvisational music therapy with severely and multiply disabled children to communication development. Journal of Music Therapy, Volume 40(3), pp. 227 - 246
Rainforth, B., Giangreco, M.F., & Dennis, R. (1989). Motor skills. In - A. Ford, R. Schnorr, L. Meyer, L. Davern, J. Black, & P. Dempsey (Eds.), Syracuse community-referenced curriculum guide for students with moderate and severe disabilities (pp. 211 - 230). Baltimore, MD: Paul H. Brookes.
Rajagopalan, S.S., Dhall, A., & Goecke, R. (2013). Self-stimulatory behaviours in the wild for autism diagnosis, IEEE International Conference on Computer Vision. Australian National University, 1-8 December. New York: Institute of Electrical and Electronics Engineers.
Rajala, A.Z., Reininger, K.R., Lancaster, K.M., & Populin, L.C. (2010). Rhesus monkeys (Macaca mulatta) do recognize themselves in the mirror: implications for the evolution of self-recognition. PLoS 2 ONE. Volume 5: e12865
Ramachandran, V.S. (1994). Phantom limbs, neglect syndromes, repressed memories, and Freudian psychology. International Review of Neurobiology, Volume 37, pp. 291 - 333
Ramachandran, V.S. (1996). The Brain's Potential for Growth and Change. UCSD Decade of the Brain Symposium, October 21, 1996
Ramachandran, V.S., & Blakeslee, S. (1998). Phantoms in the Brain: Probing the Mysteries of the Human Mind. William Morrow publishers
Ramachandran, V.S., & Hirstein, W. (1998). The Perception of Phantom Limbs: The D.O. Hebb Lecture, Brain, Volume 121 (1998), pp. 1603 – 1630
Ramachandran, V.S. (2002). Encyclopedia of the Human Brain. Academic Press, San Diego.
Ramachandran, V.S. (2003). The Emerging Mind. BBC/Profile Books, London
Ramachandran, V.S. (2004). A Brief Tour of Human Consciousness: From Impostor Poodles to Purple Numbers. New York: Pi Press.
Ramachandran, V.S. (2005). Plasticity and functional recovery in neurology. Clinical medicine, Volume 5(4), pp. 368 - 373
Ramachandran, V.S., & Oberman, L.M. (2006). Broken mirrors: a theory of autism. Scientific American, Volume 295(5), 62 - 69
Ramachandran, V.S., & Rogers-Ramachandran, D. (2007). It’s All Done with Mirrors. Scientific American Mind, Volume 18(4), pp. 16 - 18
Ramachandran, V.S., & Altschuler, E. (2009). The Use of Visual Feedback, in particular Mirror Visual Feedback, in Restoring Brain Function, Brain, Volume 132(7), pp. 1693 – 1710
Ramachandran, V.S. (2011). The Tell-Tale Brain: A Neuroscientist's Quest for What Makes Us Human. New York: W. W. Norton & Company
Rapoff, M.A., Altman, K., & Christophersen, E.R. (1980). Suppression of self-injurious behaviour: Determining the least restrictive alternative. Journal of Mental Deficiency Research, Volume 24, pp. 37 - 46
Reader, M. (2011). Setting Students up for Success Through Self-Awareness and Self-Advocacy. Foothills academy
Realon, R.E., Bligen, R.A., La Force, A., Helsel, W.J., & Goldman, V. (2002). The effects of the positive environment program (PEP) on the behaviors of adults with profound cognitive and physical disabilities. Behavioral Intervention, Volume 17(1), pp. 1 - 13
Redding, H. (1999). Stimulate the senses. Special! Summer 1999, pp. 16 - 19
Redefer, L.A., & Goodman, J.F. (1989). Brief Report: Pet Facilitated Therapy With Autistic Children. Journal of Autism and Developmental Disorders. Volume 19(3), pp. 461 - 467
Reed, L. (1991). Games with a New Look for All Ability Levels. The Spastics Society, Meldreth, Herts.
Rees, K. (2014). Using Innovative Approaches to Addressing Challenging Behaviours. PMLD Link, Volume 26(3), Issue 79, pp. 21 - 23
Rees, M. (1995). Making sense of marking space: Researching art therapy with people who have severe learning difficulties. In C. Lee & A. Gilroy (Eds.) Art and music therapy research. London: Routledge.
Rees, M. (1998). Drawing on difference: Art therapy with people who have learning difficulties. London: Routledge.
Reese, G.M., & Snell, M.E. (1991). Putting on and Removing Coats and Jackets: The Acquisition and Maintenance of Skills by Children with Severe Multiple Disabilities. Education and Training in Mental Retardation. Volume 26(4), pp. 398 - 410
Reese, R.M. (1997). Biobehavioral analysis of self-injurious behavior in a person with profound handicaps. Focus on Autism and Other Developmental Disabilities, Volume 12(2), pp. 87 - 94
Reichelt, K.L., & Knivsberg, A.M. (2009). The possibility and probability of a gut-to-brain connection in autism. Annals of Clinical Psychiatry, Volume 21(4), pp. 205 - 211
Reichle, J., Sigafoos, J., & Piche, L. (1989). Teaching an adolescent with blindness and severe disabilities: A correspondence between requesting and selecting preferred objects. Journal of the Association for Persons with Severe Handicaps, Volume 14, pp. 75 – 80
Reichle, J. (1991a). Defining Decisions, In - Reichle, J., York, J., & Sigafoos, J. (Eds.), Implementing Augmentative and Alternative Communication: Strategies for Learners with Severe Disabilities. Paul H. Brookes Publishing
Reichle, J. (1991b). Developing communicative exchanges, In - Reichle, J., York, J., & Sigafoos, J. (Eds.), Implementing Augmentative and Alternative Communication: Strategies for Learners with Severe Disabilities. Paul H. Brookes Publishing
Reichle, J., & Sigafoos, J. (1991a). Establishing an initial repertoire of requesting In - Reichle, J., York,J., & Sigafoos,J. (Eds.), Implementing Augmentative and Alternative Communication: Strategies for Learners with Severe Disabilities. Paul H. Brookes Publishing
Reichle, J., & Sigafoos, J. (1991b). Establishing spontaneity and generalization In - Reichle, J., York,J., & Sigafoos,J. (Eds.), Implementing AAC: Strategies for learners with severe disabilities, pp. 157 - 171, Paul H. Brookes Publishing Co.
Reichle, J., & Sigafoos, J. (1991c). Bringing communicative behavior under the control of the appropriate stimuli In - Reichle, J., York,J., & Sigafoos,J. (Eds.), Implementing AAC: Strategies for learners with severe disabilities, pp. 193 - 213, Paul H. Brookes Publishing Co.
Reichle, J., York,J., & Sigafoos,J. (Eds.) (1991). Implementing Augmentative and Alternative Communication: Strategies for Learners with Severe Disabilities. Paul H. Brookes Publishing
Reid, D.H., & Parsons, M.B. (1991). Making choice a routine part of mealtimes for persons with profound mental retardation. Behavioral Residential Treatment, Volume 6, pp. 249 - 261
Reid, D.H., Phillips, J.F., & Green, C.W. (1991). Teaching persons with profound multiple handicaps: A review of the effects of behavioral research. Journal of Applied Behavior Analysis, Volume 24(2), pp. 319 - 336
Reid, D.H., Everson. J.M., & Green, C.W. (1999). A systematic evaluation of preferences identified through person-centred planning for people with profound multiple disabilities. Journal of Applied Behavior Analysis, Volume 32(4), pp. 467 – 477
Reid, D.H., Parsons, M.B., & Green, C.W. (2001). Evaluating the functional utility of congregate day treatment activities for adults with severe disabilities. American Journal on Mental Retardation, Volume 106(5), pp. 460 - 469
Reid, D.H., Green, C.W., & Parsons, M.B. (2003). An outcome management program for extending advances in choice research into choice opportunities for supported workers with severe multiple disabilities. Journal of Applied Behavior Analysis, Volume 36(4), pp. 575 – 578
Reimer, A., & Siemonsma-Boom, M. (2013). Motoriek en visuele beperkingen [Motoric and visual impairments]. In - R. van Empelen, R. Nijhuis-van der Sanden, & A. Hartman (Eds.), Kinderfysiotherapie . pp. 639 – 659. Amsterdam, the Netherlands: Reed Business Education.
Reisman, J. (1993). Using a sensory integrative approach to treat self-injurious behavior in an adult with profound mental retardation. American Journal of Occupational Therapy, Volume 47, pp. 403 – 411
Reiss, D., & Marino, L. (2001). Mirror self-recognition in the bottle-nose dolphin: a case of cognitive convergence. Proceedings of the National Academy of Sciences of the United States of America, Volume 98, pp. 5937 – 5942
Reiss S. & Rojahn J. (1993). Joint occurrence of depression and aggression in children and adults with mental retardation. Journal of Intellectual Disability Research, Volume 37, pp. 287 – 294
Remington, B. (1996). Assessing the occurrence of learning in children with profound intellectual disability: A conditioning approach. International Journal of Disability, Development and Education, Volume 43(2), pp. 101 - 118
Repp, A.C., Felce, D., & de Kock, U. (1987). Observational studies of staff working with mentally retarded persons: a review. Research in Developmental Disabilities, Volume 8(2), pp. 331 - 350
Repp, A.C., Felce, D., & Barton, L.E. (1988). Basing the treatment of stereotypic and self-injurious behaviors on hypotheses of their causes. Journal of Applied Behavior Analysis, Volume 21, pp. 281 - 289
Resman, M.H. (1981). Effect of sensory stimulation on eye contact in a profoundly retarded adult. American Journal of Occupational Therapy, Volume 35, pp. 31 - 35
Reynolds, A. (2012). Pets as therapy: where is the evidence? Nursing & Residential Care, Volume 14(9), pp. 478 - 481
Reynolds, F. (2002). A survey of opportunities and barriers to creative leisure activity for people with learning disabilities. British Journal of Learning Disabilities, Volume 30 (2), pp. 63 - 67
Rhodes, J., & Hewett, D. (2010). The Human Touch: physical contact and making a social world available for the most profoundly disabled. PMLD Link. Volume 22(2), pp. 11 - 14
Richmond, G., Schroder, S.R., & Bickel, W. (1986). Tertiary prevention of attrition related to self-injurious behaviours. In K.D. Gadow (Ed.), Advances in Learning and Behavioural Disabilities, Volume 5. London: JAI Press
Rickson, D.J. (1997). The music therapist working in New Zealand schools with children who have disabilities. Annual Journal of the New Zealand Society for Music Therapy, 1997 edition, pp. 44 - 53
Rickson, D.J. (2001). A Music Therapy Practice in Special Education Settings in New Zealand. New Zealand Society for Music Therapy, 2001 edition, pp. 26 - 47
Rickson, D.J. (2006). Reflections on the nature of relationship in brief music therapy encounters with children who have developmental difficulties. New Zealand Journal of Music Therapy, Volume 4, pp. 23 - 45
Rickson, D.J. (2007). Music Therapy in Special Education: Do We Need More Evidence? A response to K. McFerran & J. Stephenson. British Journal of Music Therapy, Volume 21(1), pp. 28 - 29
Rickson, D.J., & McFerran K. (2007). Music Therapy in Special Education: Where are we now? New Zealand Journal of Educational Practice, Volume 8(1), pp. 40 - 47
Rickson, D.J. (2008). The potential role of music in special education (The Promise) - New Zealand music therapists consider collaborative consultation. New Zealand Journal of Music Therapy, Volume 6, pp. 76 - 97
Rickson, D.J. (2010). The development of a music therapy school consultation protocol for students with high or very high special educational needs. Thesis: Doctor of Philosophy in Music. New Zealand School of Music, Wellington,
Rimmer, J.H., Braddock, D., & Fujiura, G. (1993). Prevalence of obesity in adults with mental retardation: implications for health promotion and disease prevention. Mental Retardation, Volume 31(2), pp. 105 - 110
Rimmer, J.H. (1994). Fitness and rehabilitation programs for special populations. McGraw-Hill Humanities, Social Sciences & World Languages.
Rimmer, J.H., Braddock, D., & Marks, B. (1995). Health characteristics and behaviors of adults with mental retardation residing in three living arrangements. Research in Developmental Disabilities, Volume16(6), pp. 489 - 499
Rimmer, J.H., & Wang, E. (2005). Obesity prevalence among a group of Chicago residents with disabilities. Archives of Physical Medicine and Rehabilitation, Volume 86(7), pp. 1461 - 1464
Rimmer, J.H., & Yamaki, K. (2006). Obesity and intellectual disability. Developmental Disabilities Research Reviews, Volume 12(1), pp. 22 - 27
Rimmer, J.H., Yamaki, K., Lowry, B.M., Wang, E., & Vogel, L.C. (2010). Obesity and obesity‐related secondary conditions in adolescents with intellectual/developmental disabilities. Journal of Intellectual Disability Research, Volume 54(9), pp. 787 - 794
Rincover, A., Newsom, C.D., Lovaas, 0.I., & Koegel, R.L. (1977). Some motivational properties of sensory reinforcement in psychotic children. Journal of Experimental Child Psychology, Volume 24, pp. 312 - 323
Rincover, A. (1978). Sensory extinction: a procedure for eliminating self-stimulatory behavior in developmentally disabled children. Journal of Abnormal Child Psychology, Volume 6(3), pp. 229 - 310
Rincover, A., Cook, R., Peoples, A., & Packard, D. (1979). Sensory extinction and sensory reinforcement principles for programming multiple adaptive behavior change. Journal of Applied Behavior Analysis, Volume 12(2), pp. 221 - 233
Rincover, A., Newsom, C.D., & Carr, E.G. (1979). Using sensory extinction procedures in the treatment of compulsive like behavior of developmentally disabled children. Journal of Consulting and Clinical Psychology, Volume 47(4), pp. 695 - 701
Rincover, A. (1981). How to Use Sensory Extinction. Pro Ed
Rincover, A., & Devaney, J. (1982). The application of sensory extinction procedures to self-injury. Analysis and Intervention in Developmental Disabilities, Volume 2, pp. 67 - 81
Risley, T.R. (1996). Get a life! Positive behavioral intervention for challenging behaviour through life arrangement and life coaching. In L.K. Koegel, R.L. Koegel, & G. Dunlap (Eds.), Positive behavioral support : including people with difficult behavior in the community. Baltimore: Brookes
Ritchie, F. (1993). Opening Doors: The Effects of Music Therapy with People who have Severe Learning Difficulties and Display Challenging Behaviour. In Heal, M., & Wigram, T., (Eds.) Music Therapy in Health and Education, London: Jessica Kingsley.
Roberts, M. (2001). Off-task behavior in the classroom: Applying FBA and CBM. National Association of School Psychologists and The Guidance Channel (www.guidancechannel.com)
Roberts, S., & Rues, J. (1999). Using cueing strategies and behavior state analysis to increase alertness and responsiveness among infants with severe cognitive and multiple disabilities. (Model Demonstration Project, H324M990015) Washington, DC: U.S. Department of Education.
Roberts, S., Arthur-Kelly, M., Foreman, P., & Pascoe, S. (2005). Educational approaches for maximizing arousal in children with multiple and severe disability: New directions for research and practice in early childhood contexts. Pediatric Rehabilitation, Volume 8(2), pp. 88 - 91
Robertson, J., Emerson, E., Gregory, N., Hatton, C., Turner, S., Kessissoglou, S., & Hallam, A. (2000). Lifestyle related risk factors for poor health in residential settings for people with intellectual disabilities. Research in Developmental Disabilities, Volume 21(6), pp. 469 – 486
Rochat, P. (2003). Five levels of self-awareness as they unfold early in life. Consciousness and Cognition, Volume 12, pp. 717 – 731
Rochat, P., Broesch, T., & Jayne, K. (2012). Social awareness and early self-recognition. Consciousness and Cognition, Volume 21, pp. 1491 - 1497
Rochefort, C., Gheusi, G., Vincent, J.D., & Lledo, P.M. (2002). Enriched Odor Exposure Increases the Number of Newborn Neurons in the Adult Olfactory Bulb and Improves Odor Memory. The Journal of Neuroscience, Volume 22(7). pp. 2679 – 2689
Rodin, J. & Langer, E.J. (1977). Long-Term Effects of a Control-Relevant Intervention with the Institutional Aged. Journal of Personality and Social Psychology, Volume 35, pp. 897 – 902
Rogers, B., Stratton, P., Victor, J., Kennedy, B., & Andres, M. (1992). Chronic regurgitation among persons with mental retardation: a need for combined medical and interdisciplinary strategies. American Journal of Mental Retardation. Volume 96, pp. 522 – 527
Rogers P.J., Kainth, A., & Smit, H.J. (2001). A drink of water can improve or impair mental performance depending on small differences in thirst. Appetite. Volume 36. pp. 57 - 58
Rojahn, J., & Sisson, L. (1990). Stereotyped behaviour. In Matson, J (Ed.), Handbook of Behaviour Modification with the Mentally Retarded. pp. 181 - 223. New York: Springer US
Rojahn, J. (1994). Epidemiology and topographic taxonomy of self-injurious behavior. In T. Thompson & D.B. Gray (eds.), Destructive Behavior in Developmental Disabilities: Diagnosis and Treatment, pp. 49 - 67. Thousand oaks: Sage
Rojahn, J., Matson, J.L., Lott, D., Esbensen, A.J., & Smalls, Y. (2001). The behaviour problems inventory: An instrument for the assessment of self-injury, stereotyped behavior, and aggression/destruction in individuals with developmental disabilities. Journal of Autism and Developmental Disorders, Volume 31(6), pp. 577 – 588
Rojahn, J., Schroeder, S., & Hoch, T. (2008). Self-Injurious Behaviour in Intellectual Disabilities. Oxford: Elsevier.
Rojahn, J., Rowe, E.W., Kasdan, S., Moore, L.,& van Ingen, D.J. (2011). Psychometric properties of the Aberrant Behaviour Checklist, the Anxiety, Depression and Mood Scale, the Assessment of Dual Diagnosis and the Social Performance Survey Schedule in adults with intellectual disabilities. Research in Developmental Disabilities, Volume 32, pp. 2309 - 2320
Rojahn, J., Barnard-Brak, L., Richman, D., Dotson, W., Medeiros, K., Wei, T., & Abby, L. (2012). Behavior Problems in Individuals with Cornelia de Lange Syndrome: Population-Specific Validation of the Behavior Problem Inventory-01. Journal of Developmental and Physical Disabilities, Volume 25, pp. 505 – 515
Rowland, C., & Schweigert, P. (1989). Tangible symbols: Symbolic communication for individuals with multisensory impairments. Augmentative and Alternative Communication, Volume 5(4), pp. 226 - 234
Rolandelli, P.S., & Dunst, C.J. (2003). Influences of hippotherapy on the motor and social-emotional behavior of young children with disabilities. Bridges, Volume 2(1), pp. 1 - 5
Rose, S., & Massey, P. (1993). Adventurous Outdoor Activities: An Investigation into the benefits of Adventure for Seven People with Severe Learning Difficulties. Mental Handicap Research. Volume 6. pp. 287 - 301
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton, NJ: Princeton University Press.
Ross E. & Oliver C. (2002). The relationship between levels of mood, interest and pleasure and challenging behaviour in adults with severe and profound intellectual disability. Journal of Intellectual Disability Research, Volume 42, pp. 191 – 197
Rokvic, V. (2007). The Meaning and Role of Touch with an Adult with Profound Learning Disability in Dance Movement Therapy, Unpublished MA dissertation, Goldsmith University
Rosenzweig, M.R., Krech, D., Bennett, E.L., & Diamond, M.C. (1962). Effects of environmental complexity and training on brain chemistry and anatomy: A replication and extension. Journal of Comparative and Physiological Psychology, Volume 55(4), pp. 429 - 437
Rosenzweig, M.R., & Bennett, E.L. (1972). Cerebral changes in rats exposed individually to an enriched environment. Journal of Comparative and Physiological Psychology, Volume 80(2), pp. 304 - 313
Rowland, C.M., & Schweigert, P. (1989). Tangible symbols: symbolic communication for individuals with multisensory impairments. Augmentative and Alternative Communication, Volume 6(4), pp. 226 - 234
Rowland, C.M., & Schweigert, P. (2000). Tangible symbols, tangible outcomes. Augmentative and Alternative Communication, Volume 16, pp. 61 - 78
Royeen, C.B. (1985). Domain specification of the construct tactile defensiveness. American Journal of Occupational Therapy, Volume 39, pp. 596 – 599
Royeen, C.B. (1986). The development of a touch scale for measuring tactile defensiveness in children. American Journal of Occupational Therapy, Volume 40, pp. 414 – 418
Royeen, C.B. (1987a). Redefining tactile defensiveness. Paper presented at the Tactile Defensiveness Treatment, Research and Theory Workshop, Boston.
Royeen, C.B. (1987b). TIP-Touch inventory for preschoolers: A pilot study. Physical & Occupational Therapy in Pediatrics, Volume 7, pp. 29 – 40
Royeen, C.B., Miller, L.J., & Fortune, J. (1987). An analysis of tactile defensiveness and measures of development in elementary school aged children. Paper presented at the research forum of the annual meeting of the American Occupational Therapy Association, Indianapolis.
Royeen, C.B., & Lane, S.J. (1991). Tactile processing and sensory defensiveness. In A.G. Fisher, E.A. Murray, & A.C. Bundy. (Eds.), Sensory Integration: Theory and Practice (pp. 108-136). Philadelphia: F. A. Davis.
Rues, J. (1986). Developing basic motor skills in infants and children with severe handicaps: An experimental analysis with implications for education and treatment. Final report. Kansas: Kansas University
Rusalova, M.N. (2005). Characteristics of inter-hemisphere interactions at different levels of consciousness. Neuroscience and Behavioral Physiology, Volume 35, pp. 821 – 827
Rusch, R.G., Hall, J.C., & Griffin, H.C. (1986). Abuse provoking characteristics of institutionalized mentally retarded individuals. American Journal of Mental Deficiency. Volume 90(6). pp. 618 - 624
Sacks, O. (1989). Seeing Voices. University of California press. Picador Edition (1991). ISBN 0-330-31716-4
Salmento, M., & Bambara, L.M. (2000). Teaching staff members to provide choice opportunities for adults with multiple disabilities. Journal of Positive Behavior Interventions, Voulme 2(1), pp. 12 - 21
Saloviita, T. (2000). The structure and correlates of self-injurious behavior in an institutional setting. Research in Developmental Disabilities, Volume 21, pp. 501 - 511
Salzen, E.A. (1998). Emotion and self-awareness, Applied Animal Behaviour Science, Volume 57, pp. 299 - 313
Sams, M.J., Fortney, E.V., & Willenbring, S. (2006). Occupational therapy incorporating animals for children with autism: A pilot investigation. The American Journal of Occupational Therapy, Volume 60(3), pp. 268 – 274
Samuel, J. (2001a). Intensive Interaction, Clinical Psychology Forum, Volume 148, pp. 22 - 25
Samuel, J. (2001b). Intensive Interaction in context, Tizard Learning Disability Review, Volume 6(3), pp. 25 - 30
Samuel, J., & Pritchard, M. (2001). The ignored minority: Meeting the needs of people with profound learning disability. Tizard Learning Disability Review, Volume 6(2), pp. 34 - 44
Samuel, J. (2003). An Evaluation of Intensive Interaction in Community Living Settings for Adults with Profound Learning Disability, DclinPsychol thesis, Open University/BPS.
Samuel, J., Nind, M., Volans, A. & Scriven, I. (2008) ‘An evaluation of Intensive Interaction in community living settings for adults with profound intellectual disabilities’, Journal of Intellectual Disabilities, Volume 12(2), pp.111 - 126
Sandiford, P.J. (1997). A positive Outlook on Challenging Behaviour. National Children's Bureau
Sandler, A.G., & Voogt, K. (2001). Vestibular stimulation: Effects on visual and auditory alertness in children with multiple disabilities. Journal of Developmental and Physical Disabilities, Volume 13(4), pp. 333 - 341
Sasso, G.M., Reimers, T.M., Cooper, L.J., Wacker, D., Berg, W., Steege, M., Kelly, L., & Allaire, A. (1992). Use of descriptive and experimental analyses to identify the functional properties of aberrant behavior in school settings. Journal of Applied Behavior Analysis, Volume 25, pp. 809 - 821
Saunders, M.D., Questad, K.A., Kedziorski, T.L., Boase, B.C., Patterson, E.A., & Cullinan, T.B. (2001). Unprompted mechanical switch use in individuals with severe multiple disabilities: An evaluation of the effects of body position. Journal of Developmental and Physical Disabilities, Volume 13(1), pp. 27 - 39
Saunders, M.D., Smagner, J.P., & Saunders, R.R. (2003). Improving methodological and technological analyses of adaptive switch use of individuals with profound multiple impairments. Behavioral Interventions, Volume 18, pp. 227 - 243
Saunders, M.D., Timler, G.R., Cullinan, T.B., Pilkey, S., Questad, K.A., & Saunders, R.R. (2003). Evidence of contingency awareness in people with profound multiple impairments: response duration versus response rate indicators. Research in Developmental Disabilities, Volume 24(4), pp. 231 - 245
Saunders, M.D., Saunders, R.R., Mulugeta, A., Henderson, K., Kedziorski, T., Hekker, B., & Wilson, S. (2005). A novel method for testing learning and preferences in people with minimal motor movement. Research in Developmental Disabilities, Volume 26(3), pp. 255 - 266
Saunders, R.R., McEntee, J.E., & Saunders, M.D. (2005). Interaction of reinforcement schedules, a behavioral prosthesis, and work-related behavior in adult with mental retardation. Journal of Applied Behavior Analysis, Volume 38(2), pp. 163 - 176
Savage, L.M., Buzzetti, R.A., & Ramirez, D.R. (2004). The effects of hippocampal lesions on learning, memory, and reward expectancies.
Neurobiology of Learning and Memory. Volume 82(2), pp. 109 - 119
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1977). Initial acquisition of symbolic skills via the Yerkes computerized language analogue system, Presentation at Nonspeech Language Intervention Conference, Gulf Shores, Al, March 1977
Savage-Rumbaugh, E.S., Wilkerson, B., & Bakeman, R. (1977). Spontaneous gestural communication among conspecifics in the pygmy chimpanzee. In - Progress in ape research, Bourne, G. (Ed.) , pp. 97 - 116. New York: Academic Press
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1978). Symbolization, language, and chimpanzees: A theoretical reevaluation based on initial language acquisition processes in four young pan troglodytes. Brain and Language, Volume 6, pp. 265 - 300
Savage-Rumbaugh, E.S., Rumbaugh, D., & Boysen, S. (1978a). Linguistically mediated tool use and exchange by chimpanzees. Behavioral and Brain Sciences. Volume 1, pp. 539 - 554
Savage-Rumbaugh, E.S., Rumbaugh, D., & Boysen, S. (1978b). Symbolic communication between two chimpanzees. Science, Volume 201: pp. 641 - 644
Savage-Rumbaugh, E.S. (1979). Symbolic communication - its origins and early development in the chimpanzee. New Directions for Child Development. Volume 3, pp. 1 - 15
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1980a). Language analogue project, phase II: Theory and tactics. In - Children's language, Nelson, K. (Ed.), pp. 267 - 307. New York: Gardner Press
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1980b). Requisites of symbolic communication - Or, are words for birds? The Psychological Record, Volume 30, pp. 305 - 315
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1980c). A response to Herbert Terrace's paper, "Linguistic apes". The Psychological Record.
Volume 30, pp. 315 - 318
Savage-Rumbaugh, E.S., Rumbaugh, D., & Boysen, S. (1980). Do apes use language? American Scientist, Volume 68, pp. 49 - 61
Savage-Rumbaugh, E.S., Rumbaugh, D., Smith, S.T., & Lawson, J. (1980). Reference: The linguistic essential. Science. Volume 210, pp. 922 - 924
Savage-Rumbaugh, E.S. (1981). Can apes use symbols to represent their world? In - The Clever Hans Phenomenon: Communication with horses, whales, apes, and people, Sebeok, T. & Rosenthal, R. (Eds.). pp. 35 - 59. Annals of the New York Academy of Sciences, Volume 364
Savage-Rumbaugh, E.S., & Rumbaugh, D. (1982). Ape language research is alive and well: A reply. Anthropos, Volume 77: pp. 568 - 573
Savage-Rumbaugh, E.S., Pate, J., Lawson, J., Smith, S.T., & Rosenbaum, S. (1983). Can a chimpanzee make a statement? Journal of Experimental Psychology: General. Volume 112. pp. 457 - 492
Savage-Rumbaugh, E.S., Romski, M.A., Sevcik, R.A., & Pate, J. (1983). Assessing symbol usage versus symbol competency. Journal of Experimental Psychology: General. Volume 112, pp. 508 - 512
Savage-Rumbaugh, E.S. (1984a). Verbal behaviour at a procedural level in the chimpanzee. Journal of Experimental Analysis of Behaviour
Volume 41, pp. 223 - 250
Savage-Rumbaugh, E.S. (1984b). Pan paniscus and Pan troglodytes: Contrasts in preverbal communicative competence. In - The pygmy chimpanzee: Evolutionary biology and behavior, Susman, R. (Ed.). pp. 395 - 413. New York: Plenum
Savage-Rumbaugh, E.S. (1986). Ape language: From conditioned response to symbol. Oxford: Oxford University Press. New York: Columbia University Press
Savage-Rumbaugh, E.S., McDonald, K., Sevcik, R.A., Hopkins, W., & Rubert, E. (1986). Spontaneous symbol acquisition and
communicative use by pygmy chimpanzees. Journal of Experimental Psychology: General. Volume 115, pp. 211 - 235
Savage-Rumbaugh, E.S. (1987). Communication, symbolic communication, and Language: Reply to Seidenberg and Petitto. Journal of Experimental Psychology: General. Volume 116, pp. 288 - 292
Savage-Rumbaugh, E.S. (1998). A new look at ape language: Comprehension of vocal speech and syntax. In - Comparative perspectives in modern psychology. Nebraska Symposium on Motivation. Leger, D.W. (Ed.) . pp. 201 - 255. Lincoln, Nebraska: University of Nebraska Press
Savage-Rumbaugh, E.S., Sevcik, R., Brakke, K., Rumbaugh, D. & Greenfield, P. (1990). Symbols: Their communicative use, combination, and comprehension by Bobobos (pan paniscus). In - Advances in infancy research (Volume 6, pp. 221-278). Lipsett, L. & Rovee-Collier, C. (Eds). Norwood, NJ: Ablex
Savage-Rumbaugh, E.S. (1992). Pan to man: The language link. Presentation at the American Association for the Advancement of Science, February 8, 1992, Chicago
Savage-Rumbaugh, E.S., & Lewin, R. (1994). Kanzi: The ape at the brink of the human mind. London: Doubleday
Savarimuthu, D., & Bunnell, T. (2002). The effects of music on clients with learning disabilities: a literature review. Complementary Therapies in Nursing & Midwifery. Volume 8, pp. 160 -165
Saxby, H., Thomas, M., Felce, D., & De Kock, U. (1986). The use of shops, cafes and public houses by severely and profoundly mentally handicapped adults. British Journal of Mental Subnormality, Volume 32, pp. 69 - 81
Saxby, H, & Morgan, H. (1993). Behaviour Problems in Children with Learning Disabilities: to what extent do they exist and are they a problem? Child Care, Health and Development, Volume 19, pp. 149 - 157
Scarborough, D.R., Boyce, S., McCain, G., Oppenheimer, S., August, A., & Strinjas, J.N. (2006). Abnormal physiological responses to touch among children with persistent feeding difficulties. Developmental Medicine & Child Neurology. Volume 48, pp. 460 464
Scarth, S.B. (2001). Dance Movement therapy with adults with severe learning difficulties and behaviours that challenge. ADMT quarterly,
Volume 12(3), pp. 9 - 17
Schaaf, R.C., & Miller, L.J. (2005). Occupational therapy using a sensory integrative approach for children with developmental disabilities. Mental Retardation and Developmental Disabilities Research Reviews, Volume 11, pp. 143 – 148
Schaffer, R. (1984). Sensory integration therapy with learning disabled children: A critical review. Canadian Journal of Occupational
Therapy, Volume 51, pp. 73 - 77.
Schalock, R.L., Harper, R.S., & Genung, T. (1981). Community integration of mentally retarded adults: Community placement and program success. American Journal of Mental Deficiency, Volume 85(5), pp. 478 - 488.
Schalock, R.L., Brown, I., Brown, R., Cummins, R.A., Felce, D., Matikka, L., Keith K.D., & Parmenter, T. (2002). Conceptualization, measurement, and application of quality of life for people with intellectual disabilities: Report of an international panel of experts. Mental Retardation, Volume 40(6), pp. 457 – 470
Schalock, R.L., & Verdugo, M.A. (2002). Handbook on quality of life for human service practitioners. Washington, DC: American Association on Mental Retardation.
Schalock, R.L. (2004). The concept of quality of life: what we know and do not know. Journal of Intellectual Disability Research, Volume 48(3), pp. 203 – 216
Schalock, R.L., Verdugo, M.A., Jenaro, C., Wang, M., Wehmeyer, M., Xu, J., & Lachapelle, Y. (2005). A cross-cultural study of quality of life indicators. American Journal on Mental Retardation, Volume 110(4), pp. 298 – 311
Schalock, R.L. (2010). The measurement and use of quality of life-related personal outcomes, in - Enhancing the Quality of Life of People with Intellectual Disabilities, R. Kober, Ed., pp. 3 – 17, Springer, Dordrecht, The Netherlands
Schalock, R.L. & Verdugo, M.A. (2012). A leadership guide for today’s disabilities organizations. Baltimore, MD: Paul H. Brookes.
Schellingerhout, R., Smitsman, A.W., & Cox, R.F.A. (2005). Evolving patterns of haptic exploration in visually impaired infants. Infant Behavior & Development, Volume 28, pp. 360 – 388
Schepis, M.M., & Reid, D.H. (1994). Training direct service staff in congregate settings to interact with people with severe disabilities: A quick, effective and acceptable program. Behavioral Interventions, Volume 9(1), pp. 13 – 26
Schepis, M.M., & Reid, D.H. (1995). Effects of a voice output communication aid on interactions between support personnel and an individual with multiple disabilities. Journal of Applied Behavior Analysis, Volume 28(1), pp. 73 – 77
Schmitt, J.A.J., Benton, D., & Wolfgang Kallus, K. (2005). General methodological considerations for the assessment of nutritional influences on human cognitive functions. European Journal of Nutrition. Volume 44. pp. 459 – 464
Schneider, M.J., Bijam-Schulte, A.M., Janssen, C.G.C., & Stolk, J. (1995). The origin of self-injurious behaviour of children with mental retardation. British Journal of Developmental Disabilities. Volume 42, pp. 136 - 148
Schneider, R.S. (2016). Making Sense: A Guide to Sensory Issues. Future Horizons
Schroeder, S.R., Schroeder, C.S., Smith, B., & Dalldorf, J. (1978). Prevalence of self-injurious behaviors in a large state facility for the retarded: a three year follow-up. Journal of Autism and Childhood Schizophrenia, Volume 8, pp, 261 - 269
Schrojenstein Lantman‐de Valk, H.V., Akker, M.V.D., Maaskant, M.A., Haveman, M.J., Urlings, H.F.J., Kessels, A., & Crebolder, H.F.J. (1997). Prevalence and incidence of health problems in people with intellectual disability. Journal of Intellectual Disability Research, Volume 41(1), pp. 42 - 51
Schulz, R., & Hanusa, B.H. (1978). Long-Term Effects of Control and Predictability-Enhancing Interventions: Findings and Ethical
Issues. Journal of Personality and Social Psychology, Volume 36. pp. 1202 – 1012
Schwartz, B. (2005). The Paradox of Choice: Why More Is Less. Harper Perennial; New edition edition.
Schwartzman, L., Yu, C.T., & Martin, G.L. (2003). Choice responding as a function of choice presentation method and level of preference in persons with developmental disabilities. International Journal of Disability, Community & Rehabilitation, Volume 1, pp. 1 - 7
Schwartzman, L., Martin, G.L., Yu, C.T., & Whiteley, J. (2004). Choice, Degree of Preference, and Happiness Indices with Persons with Intellectual Disabilities: A Surprising Finding. Education and Training in Developmental Disabilities, Volume 39(3), pp 265 - 269
Scott, N. (2005). Special needs, special horses. A guide to the benefits of therapeutic riding. University of North Texas Press
Scott, R.C., King, M.D., Gadian, D.G., Neville, B.G., & Connelly, A. (2003). Hippocampal abnormalities after prolonged febrile convulsion: a longitudinal MRI study. Brain. Volume 126. pp. 2551 – 2557
Scoggins, A. (2016). The Effects of Positive-Interactions Staff Training on the Behavior of Staff and Clients during Small Groups in a Center-Based Program of Adult Day Services. (Doctoral dissertation, University of Kansas).
Sears, C.J. (1981). The Tactilely Defensive Child. Academic Therapy, Volume 16(5), pp. 563 - 569
Sears, C.J. (1994). Recognizing and coping with tactile defensiveness in young children. Infants & Young Children. Volume 6(4). pp. 46 - 53
Seay, B., & Harlow, H.F. (1965). Maternal separation in the rhesus monkey. The Journal of Nervous and Mental Disease, Volume 140(6), pp. 434 - 441
Sebba, J. (1988). The Education of People with Profound and Multiple Handicaps. Resource Material for Staff Training. Manchester University Press
Sebba, J., Byers, R., & Rose, R. (1995). Redefining the Whole Curriculum for Pupils with Learning Difficulties (revised edition). London: David Fulton Publishers
Seifert, M. (2002). Menschen mit schwerer Behinderung in Heimen. Ergebnisse der Ko¨lner Lebensqualita¨t-Studie [Humans with severe handicap in homes. Results of the Cologne quality of life study]. Geistige Behinderung, Volume 3, pp. 203 - 222
Seltzer, M.M., & Krauss, M.W. (2001). Quality of life of adults with mental retardation / developmental disabilities who live with family.
Mental Retardation and Developmental Disabilities Research Reviews, Volume 7, pp. 105 – 114
Serpell, J. (1991). Beneficial effects of pet ownership on some aspects of human health and behaviour. Journal of the Royal Society of Medicine. Volume 84(12). pp. 717 - 720
Seung, H., Rogalski, Y., Shankar, M., & Elder, J. (2007). The gluten-and casein-free diet and autism: Communication outcomes from a preliminary double-blind clinical trial. Journal of Medical Speech Language Pathology, Volume 15(4), pp. 337 - 345
Seys, D., Duker, P., Salemink, W., & Franken-Wijnhoven, J. (1998). Resident behaviors and characteristics as determinants of quality of residential care: An observational study. Research in Developmental Disabilities, Volume 19(3), pp. 261 – 273
Shapiro, M., Parush, S., Green, M., & Roth, D. (1997). The efficacy of the "Snoezelen" in the management of children with mental retardation who exhibit maladaptive behaviours. British Journal of Developmental Disabilities, Volume 43(2), pp. 140 - 155
Sharma, V.M., Sridharan, K., Pichan, G., & Panwar, M.R. (1986). Influence of heat-stress induced dehydration on mental functions. Ergonomics. Volume 29, pp. 791 - 799
Sheehy, K., & Nind, M. (2005). Emotional well-being for all: mental health and people with profound and multiple learning disabilities. British Journal of Learning Disabilities, Volume 33, pp. 34 - 38
Shenk, D. (2003). Concept of Information Overload, Encyclopedia of International Media and Communications, Volume 2, pp. 395 - 405
Shentoub, S.A., Soulairac, A., & Rustin, E. (1955). Compartement de l'enfant arriere devant Ie mirior. Enfance. Volume 7, pp. 333 - 340
Shere, B., & Kastenbaum, R. (1966). Mother child interaction in cerebral palsy: Environment and psychosocial obstacles to cognitive development, Genetic Psychology Monographs, Volume 73, pp. 255 - 335
Sheridan, M.D. (1964). Development of auditory attention and language symbols in young children. In - Renfrew, C. & Murphy, K.(Eds.), The child who does not talk. Clinics in developmental medicine. Spastics Society Medical Educational & Information Unit. William Heinemann medical books Ltd.
Shevin, M., & Klein, N.K. (1984). The importance of choice-making skills for students with severe disabilities. Journal of The Association for Persons with Severe Handicaps, Volume 9, pp. 159 - 166
Shirreffs, S.M., Merson, S.J., Fraser, S.M., & Archer, D.T. (2004). The effects of fluid restriction on hydration status and subjective
feelings in man. British Journal of Nutrition. Volume 91. pp. 951 - 958
Shogren, K.A., Lopez, S.J., Wehmeyer, M.L., Little, T.D., & Pressgrove, C.L. (2006). The role of positive psychology constructs in
predicting life satisfaction in adolescents with and without cognitive disabilities: An exploratory study. Journal of Positive Psychology, Volume 1, pp. 37 – 52
Shogren, K.A., Wehmeyer, M.L., Palmer, S.B., Soukup, J.H., Little, T.D., Garner, N., & Lawrence, M. (2007). Examining individual
and ecological predictors of the self-determination of students with disabilities. Exceptional Children, Volume 73, pp. 488 – 509
Shogren, K.A., Wehmeyer, M.L., Palmer, S.B., Soukup, J.H., Little, T., Garner, N., & Lawrence, M. (2008). Understanding the
construct of self-determination: Examining the relationship between the arc’s self-determination scale and the American Institute for
Research self-determination scale. Assessment for Effective Instruction, Volume 33, pp. 94 – 107
Shogren, K.A., Palmer, S.B., Bovaird, J., & Wehmeyer, M.L. (2010). Locus of control orientations in students with Intellectual Disability, Learning Disabilities, and no disabilities: A latent growth curve analysis. Research and Practice for Persons with Severe Disabilities, Volume 35(3-4), pp. 80 - 92
Shogren, K.A., Palmer, S.B., Wehmeyer, M.L., Williams-Diehm, K., & Little, T.D. (2012). Effect of intervention with the self-determined learning model of instruction on access and goal attainment. Remedial and Special Education, Volume 33, pp. 320 – 330
Shogren, K.A., Wehmeyer, M.L., Palmer, S.B., Rifenbark, G.G., & Little, T.D. (2015). Relationships between self-determination and post-school outcomes for youth with disabilities. Journal of Special Education. Volume 48(4), pp. 256 – 267
Shonkoff, J.P. (2011). Protecting brains, not simply stimulating minds. Science, Volume 333(6045), pp. 982 - 983
Shurtleff, T.L., Standeven, J.W., & Engsberg, J.R. (2009). Changes in Dynamic Trunk/Head Stability and Functional Reach After Hippotherapy. Archives of Physical Medical Rehabilitation, Volume 90, pp. 1185 - 1195
Siegel-Causey, E., Guy, B., & Guess, D. (1995). Severe and Multiple Disabilities. In - E.L. Meyen and T.M. Skrtic (Eds.), Special Education and Student Disability: an Introduction. Traditional, Emerging and Alternative Perspectives (4th ed.). Denver: Love Publishing.
Siegel-Causey, E., & Bashinski, S.M. (1997). Enhancing initial communication and responsiveness of learners with multiple disabilities: A tri-focus framework for partners. Focus on Autism and Other Developmental Disabilities, Volume 12(2), pp. 105 - 120
Siewertsen, C., French, E., & Teramoto, M. (2015). Autism Spectrum Disorder and Pet Therapy. Advances in Mind - Body Medicine, Volume 29(2), pp. 22 - 25
Sigafoos, J., & Dempsey, R. (1992). Assessing choice making among children with multiple disabilities. Journal of Applied Behavior Analysis, Volume 25, pp. 747 – 756
Sigafoos, J., Roberts, D., Couzens, D., & Caycho, L. (1992). Improving instruction for adults with developmental disabilities: Evaluation of a staff training package. Behavioral Interventions, Volume 7(4), pp. 283 - 297
Sigafoos, J., Roberts, D., Couzens, D., & Kerr, M. (1993). Providing opportunities for choice-making and turn-taking to adults with multiple disabilities. Journal of Developmental and Physical Disabilities, Volume 5, pp. 297 - 310
Sigelman, C.K., Schoenrock, C.J., Spanhel, C.L., Hromas, S.G., Winer, J.L., Budd, E.C., & Martin, P.W. (1980). Surveying Mentally Retarded Persons: Responsiveness and Response Validity in Three Samples. American Journal of Mental Deficiency, Volume 84 (5), pp. 479 - 486
Sigelman, C.K., Budd, E.C., Spanhel, C.L. & Schoenrock, C.J. (1981a) When in doubt say yes: acquiescence in interviews with mentally retarded persons. Mental Retardation. Volume 19, pp. 53 - 58
Sigelman, C.K., Budd, E.C., Spanhel, C.L. & Schoenrock, C.J. (1981b). Asking questions of mentally retarded persons: a comparison of yes-no and either-or formats, Applied Research in Mental Retardation, Volume 2, pp. 347 - 357
Sigelman, C.K., Schoenrock, C.J.,Winer, J.L., Spanhel, C.L., Hromas, S.G., Martin, P.W., Budd, E.C., & Bensberg, G.J. (1981). Issues in interviewing mentally retarded persons: An empirical study. In R.H. Bruininks, C.E. Meyers, B.B. Sigford, & K.C. Lakin (Eds.), Deinstitutionalization and community adjustment of mentally retarded people (Monograph No. 4). Washington, D.C.: American Association on Mental Deficiency.
Sigelman, C.K., Budd, E.C., Winer, J.L., Schoenrock, C.J., & Martin, P.W. (1982). Evaluating Alternative Techniques of Questioning Mentally Retarded Persons. American Journal of Mental Deficiency, Volume 86(5), 1982, pp. 511 - 518
Sigelman, C.K., Winer, J.L. & Schoenrock, C.J. (1982). The responsiveness of mentally retarded persons to questions. Education and Training of the Mentally Retarded, Volume 17, pp. 120 - 124
Sigelman, C.K., Schoenrock, C.J., Budd, E.C., Winer, J.L., Spanhel, C.L., Martin, P.W., Hromas, S.G., & Bensberg, G.J. (1983). Communicating with Mentally Retarded Persons: Asking Questions and Getting Answers, Research and Training Center in Mental Retardation, Texas Tech University
Sigelman, C.K., & Budd, E.C. (1986). Pictures as an aid in questioning mentally retarded persons, Rehabilitation Counselling Bulletin, Volume 29, pp. 173 - 181
Silva, K., Correia, R., Lima, M., Magalhães, A., & de Sousa, L. (2011). Can dogs prime autistic children for therapy? Evidence from a single case study. Journal of Alternative and Complementary Medicine, Volume 17, pp. 1 – 5
Simeon, D.T., & Grantham-McGregor, S,M. (1990). Nutritional deficiencies and children's behaviour and mental development. Nutrition Research Reviews. Volume 3. pp. 1 - 24
Simmons, B, & Watson, D. (2014). Challenging the Developmental Reductionism of ‘Profound and Multiple Learning Disabilities’ Through
Academic Innovation. PMLD Link, Volume 26(3), Issue 79, pp. 25 - 27
Simon, T.J., Hespos, S.J., & Rochat, P. (1995). Do infants understand simple arithmetic? A replication of Wynn (1992). Cognitive Development, Volume 10(2), pp. 253 - 269
Singer, W. (2008). Epigenesis and brain plasticity in education. In - A. Battro, K. Fischer, & P. Léna (Eds.), The Educated Brain: Essays in Neuroeducation (pp. 97-109). Cambridge: Cambridge University Press.
Singh, N.N., Lancioni, G.E., O’Reilly, M.F., Molina, E.J., Adkins, A.D., & Oliva, D. (2003). Self-determination during mealtimes through microswitch choice-making by an individual with complex multiple disabilities and profound mental retardation. Journal of Positive Behavior Interventions, Volume 5(4).
Singh, N.N., Lancioni, G.E., Winton, A.S.W., Wahler, R.G., Singh, J., & Sage, M. (2003). Mindful caregiving increases happiness among individuals with profound multiple disabilities. Research in Developmental Disabilities, Volume 25(2), pp. 207 – 218
Singh, N.N., Lancioni, G.E., Winton, A.S.W., Molina, E.J., Sage, M., Brown, S., et al. (2004). Effects of Snoezelen room, activities of daily living skills training, and vocational skills training on aggression and self-injury by adults with mental retardation and mental illness. Research in Developmental Disabilities, Volume 25(3), pp. 285 - 293
Singh, N.N., Lancioni, G.E., Winton, A.S.W., Wahler, R.G., Singh, J., & Sage, M. (2004). Mindful care-giving increases happiness among individuals with profound multiple disabilities. Research in Developmental Disabilities, Volume 25(2), pp. 207 - 218
Singh, V., & Ghai, A. (2009). Notions of self: Lived realities of children with disabilities. Disability and Society, Volume 24(2), pp.129 - 145
Sisson, L.A., Kilwein, M.L., & Van Hasselt, V.B. (1988). A graduated guidance procedure for teaching self-dressing skills to multi-handicapped children. Research in Developmental Disabilities. Volume 9(4), pp. 419 - 432
Skeja, E. (2014). The impact of cognitive intervention program and music therapy in learning disabilities. Procedia Social and Behavioral Sciences, Volume 159, pp. 605 - 609
Skinner, B.F. (1938). The Behavior of Organisms:An Experimental Analysis, New York: Appleton-Century-Crofts
Slater, A., Mattock, A., & Brown, E. (1990). Size constancy at birth: Newborn infants' responses to retinal and real size. Journal of Experimental Child Psychology, Volume 49(2), pp. 314 - 322
Slater, A., Morison, V., Somers, M., Mattock, A., Brown, E., & Taylor, D. (1990). Newborn and older infants' perception of partly occluded objects. Infant Behavior and Development, Volume 13(1), pp. 33 - 49
Slater, A., Mattock, A., Brown, E., & Bremner, J.G. (1991). Form perception at birth: Revisited. Journal of Experimental Child Psychology, Volume 51(3), pp. 395 - 406
Sloneem, J., Arron, K., Hall, S.S., & Oliver, C. (2009). Self-injurious behaviour in Cornelia de Lange syndrome: 2. association with environmental events’. Journal of Intellectual Disability Research, Volume 53, pp. 590 – 603
Sloper, P., Knussen, C.,Turner, S., & Cunningham, C. (1991). Factors relating to stress and satisfaction with life in families of children with Down's syndrome. Journal of Child Psychology and Psychiatry, Volume 32, pp. 655 - 676
Smidt, A., Balandin, S., Reed, V., & Sigafoos, J. (2007). A communication training programme for residential staff working with adults with challenging behaviour: Pilot data on intervention effects. Journal of Applied Research in Intellectual Disabilities, Volume 20 (1), pp. 16 – 29
Smith, A.M., Roux, S., Naidoo, N.T., & Venter, D.J.L. (2005). Food choices of tactile defensive children. Nutrition. Volume 21(1), pp. 14 – 19
Smith, B., Moore, Y., & Phillips, C.J. (1983). Education with understanding? Special Education; Forward Trends, Volume 10(2): pp. 21 - 24
Smith, B. (1994). Handing over control to people with learning difficulties. In J. Coupe-O'Kane and B. Smith - Taking Control: Enabling people with learning difficulties. David Fulton Publishers
Smith, B. (1996). Discussion: Age-appropriate or Developmentally appropriate Activities? In - Coupe O’Kane, J. & Goldbart, J. (eds)
Whose Choice? - Contentious Issues For Those Working With People With Learning Difficulties. London: David Fulton.
Smith, K.A., & Gouze, K.R. (2004). The Sensory-Sensitive Child. Collins
Smith, L.J. (1996). A behavioural approach to the treatment of non‐retentive encopresis in adults with learning disabilities. Journal of Intellectual Disability Research, Volume 40(2), pp. 130 - 139
Smith, L. (2001). Communication Partnerships with People with Profound and Multiple Learning Disabilities. Tizard Learning Disability
Review, Volume 6(2), pp.16 - 21
Smith, M.D. (1985). Managing the aggressive and self-injurious behavior of adults disabled by autism. Journal of the Association for Persons with Severe Handicaps, Volume 10, pp. 228 - 232
Smith, P. (2006). Choice and control: What families want from school and community supports. Paper presented at the Annual conference of TASH, Baltimore, MD.
Smith, P., & Routel, C.R. (2010). Transition failure: The cultural bias of self-determination and the journey to adulthood for people with disabilities. Disability Studies Quarterly, Volume 30(1), pp. 1 – 22
Smith, R.B., Morgan, M., & Davidson, J. (2005). Does the daily choice making of adults with intellectual disability meet the normalisation
principle? Journal of Intellectual & Developmental Disability. Volume 30(4), pp. 226 – 235
Smith, S.A., Press, B., Koenig, K.P., & Kinnealey, M. (2005). Effects of sensory integration intervention on self-stimulating
and self-injurious behaviors. American Journal of Occupational Therapy, Volume 59, pp. 418 – 425
Smith Roley, S., Mailloux, Z., Miller-Kuhaneck, H., & Glennon, T. (2007). Understanding Ayres' Sensory Integration. OT Practice. Volume 12(7)
Snell, M., & Brown, F. (eds.) (2000). Instruction of Students with Severe Disabilities. (5th edition). Upper Saddle River, NJ: Merril.
Snow, E. Langdon, P., & Reynolds, E.S. (2007). Care staff attributions toward self-injurious behaviour exhibited by adults with intellectual disabilities. Journal of Intellectual Disabilities, Volume 11(1), pp. 47 – 63
Snyder A.W., & Thomas M. (1997). Autistic artists give clues to cognition, Perception, Volume 26, pp. 93 - 96
Snyder A.W., & Mitchell D.J. (1999). Is integer arithmetic fundamental to mental processing? The mind’s secret arithmetic. Proceedings of the Royal Society of London B: Biological Sciences, Volume 266(1419), pp. 587 - 592
Snyder A.W. (2001). Paradox of the savant mind, Nature, Volume 413, pp. 251 - 252
Snyder, A.W., Mulcahy, E., Taylor, J.L., Mitchell, D.J., Sachdev, P., & Gandevia, S.C. (2003). Savant-like skills exposed in normal people by suppressing the left fronto-temporal lobe. Journal of Integrative Neuroscience, Volume 2(02), pp. 149 - 158
Snyder, A.W., Bossomaier, T., & Mitchell, D.J. (2004). Concept formation: 'object' attributes dynamically inhibited from conscious awareness. Journal of Integrative Neuroscience, Volume 3(01), pp. 31 - 46
Snyder, A.W. (2009). Explaining and inducing savant skills: privileged access to lower level, less-processed information. Philosophical Transactions of the Royal Society of London B: Biological Sciences, Volume 364(1522), pp. 1399 - 1405
Soto-Ares, G., Joyes, B., Lemaître, M.P., Vallée, L., & Pruvo, J.P. (2003). MRI in children with mental retardation. Pediatric Radiology, Volume 33(5), pp. 334 - 345
Sousa, D. (2007). How the Special Needs Brain Learns. Crown Press/Sage, CA USA.
Sowers, J., & Powers, L. (1995). Enhancing the participation and independence of students with severe physical and multiple disabilities in
performing community activities. Mental Retardation, Volume 33, pp. 209 – 220
Spevack, S., Martin, T.L., Hiebert, R., Yu, C.T., & Martin, G.L. (2004). Effects of choice of work tasks on on-task, aberrant, happiness and unhappiness behaviors of persons with developmental disabilities. Journal on Developmental Disabilities, Volume 11, pp. 79 – 98
Spiker, D., & Ricks, M. (1984). Visual Self-recognition in autistic children: Developmental relationships. Child Development, Volume 55: pp. 214 - 225
Spooner, F., Dymond, S.K.., Smith, A., & Kennedy, C.H. (2006). What we know and need to know about accessing the general curriculum for students with significant cognitive disabilities. Research and Practice for Persons with Severe Disabilities, Volume 31(4), pp. 277 – 283
Spragg, M. (2015). Music Therapy within a Multidisciplinary Special Education Team. In - C. Miller (Ed.), Arts Therapists in Multidisciplinary Settings: Working Together for Better Outcomes, pp. 83-95. Jessica Kingsley Publishers
Spreat, S., Lipinski, D. Hill, J., & Halpin, M.E. (1986). Safety indices associated with the use of contingent restraint procedures. Applied Research in Mental Retardation. Volume 1000, pp. 528 - 532
Spreat, S., Lamina, J., Jefferys, J., Axelrod, S., Murphy, B.J., & McGuffin, P. (1990). The impact of environmental noise on mealtime social interactions in a residential facility for persons with mental retardations. Behavioral Residential Treatment, Volume 5(1), pp. 1 - 13
Srinivasan, P. (2009). A review of dietary interventions in autism. Annals of Clinical Psychiatry: Official Journal of the American Academy of Clinical Psychiatrists, Volume 21(4), pp. 237 - 247
Stafford, A.M. (2005). Choice Making: A Strategy for Students With Severe Disabilities. Teaching Exceptional Children. Volume 37(6), pp. 12 - 17
Stagnitti, K., Raison, P., & Ryan, P. (1999). Sensory defensiveness syndrome: A paediatric perspective and case study. Australian Occupational Therapy Journal. Volume 46(4), pp. 175 – 187
Stalker, K., & Harris, P. (1998). The Exercise of Choice by Adults with Intellectual Disabilities: A Literature Review. Journal of Applied Intellectual Disabilities, Volume 11, pp. 60 - 76
Stamatis, P.J. (2011). Non verbal communication in classroom interactions: A pedagogical perspective of touch. Electronic Journal of Research in Educational Psychology, Volume 9(3), pp. 1427 - 1442
Stamenovic, M. (2009). Engagement in Music Therapy: a detailed study of communication between the therapist and client presenting with severe and multiple handicaps. Master of Music Therapy Thesis: New Zealand School of Music, Wellington
Stancliffe, R.J. (1995). Assessing opportunities for choice-making: A comparison of self- and staff reports. American Journal on Mental Retardation, Volume 99, pp. 418 – 429
Stancliffe, R.J., & Wehmeyer, M.L. (1995). Variability in the availability of choice to adults with mental retardation. The Journal of Vocational Rehabilitation, Volume 5, pp. 319 – 328
Stancliffe, R.J. (1997). Community living-unit size, staff presence and resident’s choice making. Mental Retardation, Volume 35, pp. 1 – 9
Stancliffe, R.J., & Abery, B.H. (1997). Longitudinal study of deinstitutionalization and the exercise of choice. Mental Retardation, Volume 35, pp. 159 – 169
Stancliffe, R.J., & Lakin, K.C. (1998). Analysis of expenditures and outcomes of residential alternatives for persons with developmental disabilities. American Journal on Mental Retardation, Volume 102(6), pp. 552 – 568
Stancliffe, R.J., Abery, B.H., & Smith, J. (2000). Personal control and the ecology of community living settings: Beyond living-unit size and
type. American Journal on Mental Retardation, Volume 105, pp. 431 – 454
Stancliffe, R.J., Abery, B.H., Springborg, H., & Elkin, S. (2000). Substitute decision making and personal control: Implications for self determination. Mental Retardation. Volume 38(5), pp. 407 - 421
Stancliffe, R.J. (2001). Living with support in the community: Predictors of choice and self determination. Mental Retardation and Developmental Disabilities Research Reviews, Volume 7, pp. 91 – 98
Stancliffe, R.J., & Lakin, K.C. (2005). Costs and outcomes of community services for people with intellectual disabilities. Paul H Brookes Publishing.
Stancliffe, R.J., Lakin, K.C., Larson, S., Engler, J., Bershadsky, J., Taub, S., Fortune, J., & Ticha, R. (2011). Overweight and obesity among adults with intellectual disabilities who use intellectual disability/developmental disability services in 20 US States. American Journal on Intellectual and Developmental Disabilities, Volume 116(6), pp. 401 - 418
Stanish, H.I., & Draheim, C.C. (2005). Assessment of walking activity using a pedometer and survey in adults with mental retardation. Adapted Physical Activity Quarterly, Volume 22(2), pp. 136 - 145
Stanton, D., Wilson, P., Foreman, N., & Duffy, H. (2000). Virtual environments as spatial training aids for children and adults with physical disabilities. 3rd International Conference on Disability, Virtual Reality and Associated Technologies.
Steege, M.W., Wacker, D.P., Cigrand, K.C., Berg, W.K., Novak, C.G., Reimers, T.M., Sasso, G.M. and DeRaad, A. (1990). Use of negative reinforcement in the treatment of self-injurious behavior. Journal of Applied Behavior Analysis, Volume 23, pp. 459 - 467
Stein, Z., & Susser, M. (1985). Effects of early nutrition on neurological and mental competence in human beings. Psychological Medicine. Volume 15. pp. 717 - 726
Steiner, H. (2012). Sensational Journeys: 48 Personal Stories of Sensory Processing Disorder. Future Horizons
Stenfert Kroese, B., & Fleming, I. (1992). Staff attitudes and working conditions in community-based group homes of people with learning difficulties, Mental Handicap Research, Volume 5, pp. 82 - 91
Stephenson, J. (2006). Music therapy and the education of students with severe disabilities. Education and Training in Developmental Disabilities (formerly Education and Training in Mental Retardation and Developmental Disabilities), Volume 41(3), pp. 290 - 299
Sterba, J.A., Rogers, B.T., France, A.P., & Vokes, D.A. (2002). Horseback riding in children with cerebral palsy: Effect on gross
motor function. Developmental Medicine and Child Neurology, Volume 44, pp. 301 – 308
Stern, D.N. (1985). The Interpersonal World of the Infant: A View from Psychoanalysis and Developmental Psychology: A View from Psychoanalysis and Development Psychology. Karnac Books
Sternberg, L. (1994). Individuals with Profound Disabilities: Instructional and Assistive Strategies (3rd edition), PRO-ED Inc., Austin, Texas
Stevenson, K. (2003). Music therapy assisted communication with children with severe disabilities. The New Zealand Journal of Music Therapy, Volume 1, pp. 82 - 92
Stewart, L., Beange, H., & Mackerras, D. (1994). A survey of dietary problems of adults with learning disabilities in the community. Journal of Applied Research in Intellectual Disabilities, Volume 7(1), pp. 41 - 50
Stock, S.E., Davies, D.K., Secor, R.R., & Wehmeyer, M.L. (2003). Self-directed career preference selection for individuals with intellectual disabilities: using computer technology to enhance self determination. Journal of Vocational Rehabilitation, Volume 19, pp. 95 – 103
Stolker, J.J., Scheifes, A., Egberts, A.C., & Heerdink, E.R. (2008). Inappropriate prescribing of antipsychotics to people with a mental disability and aggressive behavioural disorders. Nederlands Tijdschrift voor Geneeskunde, Volume 152, pp. 1501 – 1502
Stone, V.E., Baron-Cohen, S., & Knight, R.T. (1998). Frontal lobe contributions to theory of mind. Journal of Cognitive Neuroscience, Volume 10, pp. 640 - 656
Stonefelt, L.L., & Stein, F. (1998). Sensory integrative techniques applied to children with learning disabilities: An outcome study. Occupational Therapy International, Volume 5, pp. 252 – 272
Stores, R, Stores, G., Fellows, B.& Buckley, S. (1998). Daytime behaviour problems and maternal stress in children with Down's syndrome, their siblings, and non-intellectually disabled and other intellectually disabled peers. Journal of Intellectual Disability Research, Volume 42, pp. 228 - 237
Storey, K., Bates, P., McGhee, N., & Dycus, S. (1984). Reducing the self-stimulatory behavior of a profoundly retarded female through sensory awareness training. American Journal of Occupational Therapy, Volume 38, pp. 510 – 516
Strange, J. (2013). Improvised music to support interaction between profoundly learning-disabled teenagers and their learning support assistants. Doctoral dissertation, Anglia Ruskin University
Strnadova, I., & Evans, D. (2012). Subjective Quality of Life of Women with Intellectual Disabilities: The Role of Perceived Control over Their Own Life in Self-Determined Behaviour. Journal of Applied Research in Intellectual Disabilities, Volume 25(1), pp.71 - 79
Strupp, M., Arbusow, V., Dieterich, M., Sautier, W., & Brandt, T. (1998). Perceptual and oculomotor effects of neck muscle vibration in vestibular neuritis. Ipsilateral somatosensory substitution of vestibular function. Brain: a Journal of Neurology, Volume 121(4), pp. 677 - 685
Stuss, D.T., Gallup, G.G., Jr., & Alexander, M.P. (2001). The frontal lobes are necessary for theory of mind. Brain, Volume 124, pp. 279 - 286
Sugden, D. (1989). Cognitive Approaches in Special Education. Lewes: Falmer Press.
Suhr, J.A., Hall, J., Patterson, S.M., & Niinisto, R.T. (2004). The relation of hydration status to cognitive performance in healthy older adults. International Journal of Psychophysiology. Volume 53. pp. 121 - 125
Suhr, J.A., Patterson, S.M., Austin, A.W., & Heffner, K.L. (2010). The relation of hydration status to declarative memory and working memory in older adults. Journal of Nutrition, Health & Aging. Volume 14. pp. 840 - 843
Sullivan, M., & Lewis, M. (2000). Assistive technology for the very young: Creating responsive environments. Infants and Young Children, Volume 12 (4), pp. 34 - 52
Sullivan, M. W., & Lewis, M. (1990). Contingency intervention: A program portrait. Journal of Early Intervention, Volume 14, pp. 367 - 375
Sun, J., Chen, Q., Zhang, Q., Li, Y., Li, H., Wei, D., Yang, W., & Qiu, J. (2016). Training your brain to be more creative: brain functional and structural changes induced by divergent thinking training. Human Brain Mapping, Volume 37(10), pp. 3375 - 3387
Sutcliffe, J. (1990). Adults with learning difficulties: Education for choice and empowerment. National Institute for Adult Continuing Education (NIACE) in association with the Open University Press
Sutherland, G., Couch, M.A., & Iacono, T. (2002). Health issues for adults with developmental disability. Research in Developmental Disabilities, Volume 23(6), 422 - 445
Suzuki, W.A. (2015). Healthy Brain, Happpy Life. Dey Street Books
Suzuki, W.A. (2016). How Body Affects Brain. Cell Metabolism, Volume 24, pp. 192 - 193
Swanson, H.L. (2000). What Instruction Works for Students with Learning Disabilities? Summarizing the Results from a Meta-Analysis of Intervention Studies. In: R. Gersten, E.P. Schille, & S. Vaughn (eds). Contemporary Special Education Research: Syntheses of the
Knowledge Base on Critical Instructional Issues, pp. 1-30, Mahwah, NJ: Lawrence Erlbaum.
Sweeney, L.A. (1989). Reducing learned dependency in potential and early augmentative communication users. Southeast Augmentative Communication Conference Proceedings
Sweeney, L.A. (1991). Learned dependency and co-dependency among potential users of augmentative communication, American Speech Language Hearing Association Miniseminar, Atlanta, Georgia
Sweeney, L.A. (1993). Helplessness, Dependency, an explanatory style as variables of employment potential among Augmented Communicators, First Annual Pittsburgh Employment Conference for Augmented Communicators Proceedings, August 20-22: Shout Press: Pittsburgh
Sylwester, R. (1986). Synthesis of Research on Brain Plasticity: The Classroom Environment and Curriculum Enrichment. Educational Leadership, Volume 44(1), pp. 90 - 93
Symons, F.J., Davis M.L., & Thompson, T. (2000). Self-injurious behaviour and sleep disturbance in adults with developmental disabilities. Research in Developmental Disabilities. Volume 21, pp. 115 – 23
Symons, F.J., Sperry, L.A., Dropik, P.L., & Bodfish, J.W. (2005). The early development of stereotypy and self-injury: a review of research methods. Journal of Intellectual Disability Research, Volume 49(2), pp. 144 - 158
Symons, F.J., Harper, V.N., McGrath, P.J., Breau L.M., & Bodfish, J.W. (2009). Evidence of increased non-verbal behavioural signs of pain in adults with neurodevelopmental disorders and chronic self-injury. Research in Developmental Disabilities. Volume 30, pp. 521 – 528
Synofzik, M., Vosgerau, G., & Newen, A. (2008). I move, therefore I am: A new theoretical framework to investigate agency and ownership. Consciousness and Cognition, Volume 17, pp. 411 – 424
Szinnai, G., Schachinger, H., Arnaud, M.J., Linder, L., & Keller, U. (2005). Effect of water deprivation on cognitive-motor performance in healthy men and women. American Journal of Physiology. Regulatory, Integrative and Comparative Physiology. Volume 289. pp. 275 - 280
Szpunar, K.K. (2010). Episodic future thought: an emerging concept, Perspective in Psychological Science, Volume 5, pp. 142 – 162
Tadema, A.C., & Vlaskamp, C. (2010). The time and effort in taking care for children with profound intellectual and multiple disabilities: A study on care load and support. British Journal of Learning Disabilities, Volume 38(1), pp. 41 - 48
Takeuchi, E. (1994). Incidence of obesity among school children with mental retardation in Japan. American Journal on Mental Retardation.
Volume 99(3), pp. 283 - 288
Tammet, D. (2007). Born on a blue day: Inside the extraordinary mind of an autistic savant. Simon and Schuster.
Tammet, D. (2009). Embracing the wide sky: a tour across the horizons of the mind. Simon and Schuster.
Tanabe, H., Hashikawa, K., Nakagawa, Y., Ikeda, M., Yamamoto, H., Harada, K., Tsumoto, T., Nishimura, T., Shiraishi, J., & Kimura, K. (1991). Memory loss due to transient hypoperfusion in the medial temporal lobes including hippocampus. Acta Neurologica Scandinavica. Volume 84. pp. 22 - 27
Tang, Y., Nyengaard, J.R., De Groot, D.M., & Gundersen, H.J.G. (2001). Total regional and global number of synapses in the human brain neocortex. Synapse, Volume 41(3), pp. 258 - 273
Tate, B.G., & Baroff, G.S. (1966). Aversive control of self-injurious behavior in a psichotic boy. Behavior Research and Therapy. Volume 4, pp. 281 - 287
Taylor, J.C., & Carr, E.G. (1992a). Severe behavior problems related to social interaction. I: Attention seeking and social avoidance. Behavior Modification, Volume 16, pp. 305 - 335.
Taylor, J.C., & Carr, E.G. (1992b). Severe behavior problems related to social interaction. II: A systems analysis. Behavior Modification, Volume 16, pp. 336 - 371
Taylor, J.C., Sisson, L.A., McKelvey, J.L., & Trefelner, M.F. (1993). Situation specificity in attention-seeking problem behavior. Behavior Modification, Volume 17, pp. 474 - 497
Temple, V.A., & Walkley, J.W. (2003). Physical activity of adults with intellectual disability. Journal of Intellectual & Developmental Disability, Volume 28, pp. 342 – 352
Temple, V.A., Frey, G.C., & Stanish, H.I. (2006). Physical activity of adults with mental retardation: Review and research needs. American Journal of Health Promotion, Volume 21(1), pp. 2 – 12
Ten Brug, A., Van der Putten, A.A., & Vlaskamp, C. (2013). Learn and apply: Using multi-sensory storytelling to gather knowledge about preferences and abilities of children with profound intellectual and multiple disabilities – three case studies. Journal of Intellectual Disabilities, Volume 17(4), pp. 339 - 360
Ten Brug, A., Munde, V.S., van der Putten, A.A., & Vlaskamp, C. (2015). Look closer: the alertness of people with profound intellectual and multiple disabilities during multi-sensory storytelling, a time sequential analysis. European Journal of Special Needs Education, Volume 30(4), pp. 535 - 550
Ten Brug, A., Van der Putten, A.A., Penne, A., Maes, B., & Vlaskamp, C. (2015). Factors Influencing Attentiveness of People With Profound Intellectual and Multiple Disabilities to Multisensory Storytelling. Journal of Policy and Practice in Intellectual Disabilities, Volume 12(3), pp. 190 - 198
Ten Brug, A., Van der Putten, A.A., Penne, A., Maes, B., & Vlaskamp, C. (2016). Making a difference? A comparison between multi‐sensory and regular storytelling for persons with profound intellectual and multiple disabilities. Journal of Intellectual Disability Research, Volume 60(11), pp. 1043 - 1053
Tenneij, N.H., & Koot, H.M. (2008). Incidence, types and characteristics of aggressive behaviour in treatment facilities for adults with mild intellectual disability and severe challenging behaviour. Journal of Intellectual Disability Research. Volume 52, pp.114 – 124
Test, D.W., Karvonen, M., Wood, W.M., Browder, D., & Algozzine, B. (2000). Choosing a self-determination curriculum: Plan for the future. Teaching Exceptional Children, Volume 33(2), pp. 48 – 54
Test, D.W., Mason, C., Hughes, C., Konrad, M., Neale, M., & Wood, W.M. (2004). Student involvement in individualized education program meetings. Exceptional Children, Volume 70, pp. 391 – 412
Thoma, C.A., Pannozzo, G.M., Fritton, S.C., & Bartholomew, C.C. (2008). A qualitative study of pre-service teachers’ understanding of self-determination for students with significant disabilities. Career Development for Exceptional Individuals, Volume 31, pp. 94 – 105
Thompson, B., & Guess, D. (1989). Students who experience the most profound disabilities: Teacher perspectives. In Brown, F., Lehr, D. (Eds.), Persons with profound disabilities: Issues and practices, pp. 3 - 41, Baltimore: Paul H. Brookes
Thompson, J.R., Bradley, V.J., Buntinx, W.H., Schalock, R.L., Shogren, K.A., Snell, M.E., Wehmeyer, M.L., Borthwick-Duffy, S., Coulter, D.L., Craig, E.M., Gomez, S.C., Lachapelle, Y., Luckasson, R.A., Reeve, A., Spreat, S., Tassé, M. J., Verdugo, M.A., & Yeager, M.H. (2009). Conceptualizing supports and the support needs of people with intellectual disability. Intellectual and Developmental Disabilities, Volume 47(2), pp. 135 – 146
Thye, M.D., Bednarz, H.M., Herringshaw, A.J., Sartin, E.B. & Kana, R.K. (2017). The impact of atypical sensory processing on social impairments in autism spectrum disorder. Developmental Cognitive Neuroscience, In Press
Tierney, E., Quinlan, D., & Hastings, R.P. (2007). Impact of a 3 day training course on challenging behaviour on staff cognitive and emotional responses. Journal of Applied Research in Intellectual Disabilities, Volume 20(1), pp. 58 – 63
Tilstone, C. (ed)(1991). Teaching Pupils with Severe Learning Difficulties. London: David Fulton Publishers.
Timmeren, E.A., Putten, A.A.J., Schrojenstein Lantman‐de Valk, H.M.J., Schans, C.P., & Waninge, A. (2016). Prevalence of reported physical health problems in people with severe or profound intellectual and motor disabilities: a cross‐sectional study of medical records and care plans. Journal of Intellectual Disability Research, Volume 60(11), pp. 1109 - 1118
Tipple, R. (1992). Art therapy with people who have severe learning difficulties. In - D. Waller & A. Gilroy (Eds.), Art therapy: A handbook, pp.105 – 124. Buckingham: Open University Press
Tipple, R. (1993). Challenging assumptions: The importance of transference processes in work with people with learning difficulties. Inscape: Journal of the British Association of Art Therapists, Volume 2, pp. 2 – 9.
Tohill, C., & Laverty, A. (2001). Sunshine, diet and mobility for healthy bones: an intervention study designed to implement these standards into the daily routine in an at risk population of adults with intellectual disability. Journal of Intellectual & Developmental Disability, Volume 26, pp. 217 - 231.
Tomlinson, J., Derrington, P., & Oldfield, A. (Eds.). (2012). Music Therapy in Schools: Working with Children of All Ages in Mainstream and Special Education. London: Jessica Kingsley.
Tomporowski, P.D., Beasman, K., Ganio, M.S., & Cureton, K. (2007). Effects of dehydration and fluid ingestion on cognition.
International Journal of Sports Medicine. Volume 28. pp. 891 - 896
Toolan, P., & Coleman, S. (1994). Music therapy, a description of process: Engagement and avoidance in five people with learning disabilities. Journal of Intellectual Disability Research, Volume 38, pp. 433 - 444.
Toolan, P., & Coleman, S. (1995). Music therapy, adscription of process: Engagement and avoidance in five people
with learning disabilities. British Journal of Music Therapy, Volume 9(1), pp. 17 - 24
Tota, A., Lancioni, G.E., Singh, N.N., O'reilly, M.F., Sigafoos, J., & Oliva, D. (2006). Evaluating the applicability of optic microswitches for eyelid responses in students with profound multiple disabilities. Disability and Rehabilitation: Assistive Technology, Volume 1(4), pp. 217 - 223
Totsika, V., Toogood, S., Hastings, R.P., & Lewis, S. (2008). Persistence of challenging behaviours in adults with intellectual disability over a period of 11 years. Journal of Intellectual Disability Research. Volume 52, pp. 446 – 457
Totsika, V., Felce, D., Kerr, M., & Hastings, R.P. (2010). Behavior problems, psychiatric symptoms, and quality of life for older adults with intellectual disability with and without autism. Journal of Autism and Developmental Disorders, 40(10), pp. 1171 – 1178
Touchette, P.E., MacDonald, R.F., & Langer, S.N. (1985). A scatter plot for identifying stimulus control of problem behavior. Journal of Applied Behavior Analysis, Volume 18, pp. 343 – 351
Trachtenberg, J.T., Chen, B.E., Knott, G.W., Feng, G., Sanes, J.R., Welker, E., & Svoboda, K. (2002). Long term in vivo imaging of experience-dependent synaptic plasticity in adult cortex. Nature, Volume 420(6917), pp. 788 – 795
Treffert, D.A. (1988). The idiot savant: A review of the syndrome. American Journal of Psychiatry, Volume 145(5), pp. 563 - 572
Treffert, D.A. (1989). Extraordinary people. Bantam Press
Trief, E. (2007). Research report: the use of tangible cues for children with multiple disabilities and visual impairments. Journal of Visual Impairment and Blindness, Volume 10 (10), pp. 613 – 619
Trief, E., Bruce, S.M., Cascella, P.W., & Ivy S. (2009). The development of a universal tangible symbol system. Journal of visual impairment & blindness. July 2009. pp. 425 - 431
Trief, E., Bruce, S.M., & Cascella, P.W. (2010). The selection of tangible symbols by educators of students with visual impairments and additional disabilities. Journal of Visual Impairment & Blindness. Volume 104 (8): pp. 499 - 504
Trief, E. (2013). STACS: Standardized tactual augmentative communication system. Louisville: American Printing House for the Blind.
Trief, E., Cascella, P.W., & Bruce, S.M. (2013). A Field Study of a Standardized Tangible Symbol System for Learners Who Are Visually Impaired and Have Multiple Disabilities, Journal of Visual Impairment & Blindness, May-June 2013. pp. 180 - 191
Trott, M., Laurel, M. K., & Windeck, S.L. (1993). SenseAbilities: Understanding Sensory Integration. Tucson: Therapy Skill Builders
Tsakiris, M. (2017). The multisensory basis of the self: From body to identity to others. The Quarterly Journal of Experimental Psychology, Volume 70(4), pp. 597 - 609
Tsiouris J.A., Mann R., Patti P.J. & Sturmey P. (2003). Challenging behaviours should not be considered as depressive equivalents in individuals with intellectual disability. Journal of Intellectual Disability Research, Volume 47, pp. 14 – 21
Turnbull, A.P., Turnbull, H.R., Erwin, E.J.,Soodak, L.C., & Shogren, K.A. (2010).Families, professionals, and exceptionality: A special partnership (3rd ed.). Upper Saddle River,NJ: Merrill/Prentice Hall.
Turner, F., & Shepherd, M. (2014). Doll Therapy in Dementia Care: A review of current literature. Communicare. Volume 1 (1)
Tyler, H. (2002). Working, Playing and Relating - Issues in Group Music Therapy for Children with Special Needs. In - A. Davies & E. Richards (Eds.), Music Therapy and Group Work: Sound Company, pp. 216 - 230. London: Jessica Kingsley.
Tynan, H., & Allen, D. (2002). The impact of service user cognitive level on carer attributions for aggressive behaviour. Journal of Applied Research in Intellectual Disabilities, Volume 15(3), pp. 213 – 223
Tyrer, F., McGrother, C. W., Thorp, C. F., Donaldson, M., Bhaumik, S., Watson, J. M., & Hollin, C. (2006). Physical aggression towards others in adults with learning disabilities: Prevalence and associated factors. Journal of Intellectual Disability Research, Volume 50, pp. 295 -
304
Tzu-Wei, Lin, & Yu-Min, Kuo (2013). Exercise Benefits Brain Function: The Monoamine Connection. Brain Sciences. Volume 3, pp. 39 - 53
Ullman, L., & Krasner, L. (Eds.) (1965). Case Studies in Behaviour Modification. New York: Holt, Rinehart and Winston
United Cerebral Palsy Associations, Inc. (1992). UCPA policy on communication access and free speech rights of Americans with disabilities. United Cerebral Palsy Associations, Inc. Policy manual. Washington, DC: UCPA
Utley Adelizzi, J., & Goss, D.B. (2001). Parenting Children with Learning Disabilities, Bergin and Garvey
Uyanik, M., Bumin, G., & Kayihan, H. (2003). Comparison of different therapy approaches in children with Down syndrome. Pediatrics International, Volume 45, pp. 68 – 73
Valdovinos M.G., Caruso M., Roberts C., Kim G., & Kennedy C.H. (2005). Medical and behavioural symptoms as potential side effects in adults with developmental disabilities. American Journal of Mental Retardation, Volume 110, pp. 164 – 70
Van De Sande, M.M., van Buul, V.J., & Brouns, F.J. (2014). Autism and nutrition: the role of the gut–brain axis. Nutrition Research Reviews, Volume 27(2), pp. 199 - 214
Van Delden, R., Reidsma, D., van Oorsouw, W., Poppe, R., van der Vos, P., Lohmeijer, A., Embregts, P., Evers, V., & Heylen, D. (2014). Towards an interactive leisure activity for people with PIMD. In - International Conference on Computers for Handicapped Persons, pp. 276 - 282. Springer, Cham.
Van den Broek, E.G.C., Janssen, C.G.C., van Ramhorst, T., & Deen, L. (2004). Mensen met een (zeer) ernstige meervoudige beperking en slechtziendheid. Een inventariserend onderzoek naar het visueel functioneren (People with a (very) multiple severe limitation and poor eyesight. A survey of visual functioning). Nederlands Tijdschrift voor de Zorg aan personen met verstandelijke beperkingen, Volume 30, pp. 254 – 266
Van der Gaag, A. (1988). The development of a communication assessment procedure for use with adults with a mental handicap - an interim report. The British Journal of Mental Subnormality, Volume 34(66), pp. 62 - 68
Van der Gaag, A. (1988). CASP: The Communication Assessment Profile for Adults with a Mental Handicap. Speech Profiles Limited
Van der Putten, A., Reynders, K., Vlaskamp, C., & Nakken, H. (2004). A functionally focused curriculum for children with profound multiple disabilities: A goal analysis. Journal Applied Research in Intellectual Disabilities, Volume 17(2), pp. 71 - 75
Van der Putten, A. (2005). Moving Toward Independence?: Evaluation of the" Mobility Opportunities Via Education" Curriculum with Children with Profound Intellectual and Multiple Disabilities. Rijksuniversiteit Groningen.
Van der Putten, A., Vlaskamp, C., Reynders, K., & Nakken, H. (2005). Children with profound intellectual and multiple disabilities: The effects of functional movement activities. Clinical Rehabilitation, Volume 19(6), pp. 613 – 620
Van der Putten, A., Vlaskamp, C., Reynders, K., & Nakken, H. (2005b). Movement skill assessment in children with profound multiple disabilities: a psychometric analysis of the Top Down Motor Milestone Test. Clinical Rehabilitation, Volume 19(6), pp. 635 - 643
Van der Putten, A., Vlaskamp, C., & Poppes, P. (2009). The content of support of persons with profound intellectual and multiple disabilities: An analysis of the number and content of goals in the educational programmes. Journal of Applied Research in Intellectual Disabilities, Volume 22, pp. 391 – 394.
Van der Putten, A., & Vlaskamp, C. (2011). Pain assessment in people with profound intellectual and multiple disabilities; a pilot study into the use of the pain behaviour checklist in everyday practice. Research in Developmental Disabilities, Volume 32(5), pp. 1677 – 1684
Van der Putten, A., & Vlaskamp, C. (2011b). Day services for people with profound intellectual and multiple disabilities: An analysis of thematically organized activities. Journal of Policy and Practice in Intellectual Disabilities, Volume 8(1), pp. 10 - 17
Van der Putten, A., Bossink, L.W.M., Frans, N., Houwen, S., & Vlaskamp, C. (2017). Motor activation in people with profound intellectual and multiple disabilities in daily practice, Journal of Intellectual & Developmental Disability, Volume 42(1), pp. 1 - 11
Van Dijk, J. (1965). Motor development in the education of deaf-blind children. Proceedings of the Conference on the deaf-blind, Refsnes, Denmark (pp. 41–47). Boston: Perkins School for the Blind.
Van Dijk, J. (1967). The non-verbal deaf-blind child and his world: His outgrowth towards the world of symbols. Proceedings of the Jaaverslag Institute voor Doven, 1964–1967 (pp. 73–110). Sint-Michielsgestel: Holland.
Van Dijk, J. (1986). An educational curriculum for deaf-blind multi-handicapped persons. In - D. Ellis (Ed.). Sensory Impairments in Mentally Handicapped People. London: Croom Helm
Van Hanegem, E., Enkelaar, L., Smulders, E., & Weerdesteyn, V. (2014). Obstacle course training can improve mobility and prevent falls in people with intellectual disabilities. Journal of Intellectual Disability Research, Volume 58(5), pp. 485 - 492
Van Oorsouw, W.M., Embregts, P.J., Bosman, A.M., & Jahoda, A. (2009). Training staff serving clients with intellectual disabilities: A meta-analysis of aspects determining effectiveness. Research in Developmental Disabilities, Volume 30, pp. 503 - 511
Van Timmeren, E.A., Van der Putten, A.A.J., Schrojenstein Lantman-de Valk, H.M.J., Schans, C. P., & Waninge, A. (2016). Prevalence of reported physical health problems in people with severe or profound intellectual and motor disabilities: A cross-sectional study of medical records and care plans. Journal of Intellectual Disability Research, Volume 60(11), pp. 1109 – 1118
Vargas, S., & Camilli, G. (1999). A meta-analysis of research on sensory integration treatment. American Journal of Occupational
Therapy, Volume 53, pp. 189 - 198
Veit, S.W., Allen, G.J., & Chinsky, J.M. (1976). Interpersonal interactions between institutionalized retarded children and their attendants. American Journal of Mental Deficiency, Volume 80(5), pp. 535 - 542
Vernon, M. (1972). Mind over mouth: A rationale for 'total communication'. Volta Review, Volume 74, pp. 529 - 540
Vernon, M. (1987). Sensory Impairments in Mentally Handicapped People. American Annals of the Deaf, Volume 132(1), pp. 4 - 4
Vinter, A., Mounoud, P., & Husain, O. (1983). Accuracy and Stability of Self-Image of Mentally Retarded Adults. American Journal of Mental Deficiency, Volume 87(6), pp. 583 - 590
Vlaskamp, C. (1999). Een eigen perspectief. Een programma voor mensen met ernstige meervoudige beperkingen (Your own perspective. A program for people with severe multiple disabilities). Assen: Van Gorcum.
Vlaskamp, C., & Nakken, H. (1999). Missing in execution therapies and activities for individuals with profound multiple disabilities. British Journal of Developmental Disabilities, Volume 45(2), pp. 99 - 109
Vlaskamp, C., & Verkerk, M.A. (2000). Zorg als proces – over zorgpraktijken en zorgvocabulaires (Care as a process - about care practices and care vocabularies). Dutch Journal of Care for persons with intellectual disabilities, Volume 26, pp. 4 – 16
Vlaskamp, C., & Oxener, G. (2002). Communicatie bij mensen met ernstige meervoudige beperkingen: Een overzicht van assessment en interventie methoden (Communication in people with severe multiple disabilities: An overview of assessment and intervention methods). Dutch Journal of Care for persons with intellectual disabilities, Volume 28, pp. 226 - 237
Vlaskamp, C., de Geeter, K.I., Huijsmans, L.M., & Smit, I.H. (2003). Passive activities: the effectiveness of multisensory environments on the level of activity of individuals with profound multiple disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 16(2), pp. 135 - 143
Vlaskamp, C. (2005). Assessing people with profound intellectual and multiple disabilities. In J. Hogg & A. Langa (Eds.), Assessing adults with intellectual disability: A service provider’s guide (pp. 152 - 163). Blackwell Publishers: Oxford.
Vlaskamp, C., Fonteine, H., & Tadema, A. (2005). Handleiding bij de lijst 'Alertheid van kinderen met zeer ernstige verstandelijke en meervoudige beperkingen. [Manual of the list 'Alertness in children with profound intellectual and multiple disabilities']. Groningen: Stichting Kinderstudies.
Vlaskamp, C., & Cuppen-Fonteine, H. (2007). Reliability of assessing the sensory perception of children with profound intellectual and multiple disabilities: A case study. Child Care, Health and Development, Volume 33(5), pp. 547 - 551
Vlaskamp, C., Hiemstra, S.J., & Wiersma, L.A. (2007). Becoming aware of what you know or need to know: Gathering client and context characteristics in day services for persons with profound intellectual and multiple disabilities. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(2), pp. 97 - 103
Vlaskamp, C., Hiemstra, S.J., Wiersma, L.A., & Zijlstra, B.J.H. (2007). Extent, duration, and content of day services' activities for persons with profound intellectual and multiple disabilities. Journal of Policy and Practice in Intellectual Disabilities, Volume 4(2), pp. 152 - 159
Vlaskamp, C., & Nakken, H. (2008). Therapeutic interventions in the Netherlands and Belgium in support of people with profound intellectual and multiple disabilities. Education and Training in Developmental Disabilities, Volume 43(3), pp. 334 - 341
Vlaskamp, C., & Van der Putten, A. (2009). Focus on interaction: The use of an Individualized Support Program for persons with profound intellectual and multiple disabilities. Research in Developmental Disabilities, Volume 30(5), pp. 873 – 883
Vlaskamp, C., Fonteine, H., Tadema, A., & Munde, V.S. (2010). Manual for the “Alertness in people with profound intellectual and multiple disabilities” checklist. Groningen: Stichting Kinderstudies.
Vogeley, K., & Fink, G. R. (2003). Neural correlates for first-person perspective. Trends in Cognitive Sciences, Volume 7(1), pp. 38 – 42
Vogiatzoglou, A., Ockelford, A., Welch, G., & Himonides, E. (2011). Sounds of intent: Interactive software to assess the musical development of children and young people with complex needs. Music and Medicine, Volume 3(3), pp. 189 - 195
Von Tetzchner, S., & Martinsen, H. (1992). Introduction to Sign Teaching and the Use of Communication Aids. Whurr Publishers
Vos, P. de Cock, P., Petry, K., van den Noortgate, W., & Maes, B. (2010). What makes them feel like they do? Investigating the subjective well-being in people with severe and profound disabilities, Research in Developmental Disabilities, Volume 31(6), pp. 1623 – 1632
Vos, P., De Cock, P., Petry, K., Van den Noortgate, W., & Maes, B. (2010b). Do you know what I feel? A first step towards a physiological measure of the subjective well-being of persons with profound intellectual and multiple disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 23(4), pp. 366 - 378
Vos, P., de Cock, P., Munde, V., Neerinckx, H., Petry, K., Van Den Noortgate, W., & Maes, B. (2013). The role of attention in the affective life of people with severe or profound intellectual disabilities. Research in Developmental Disabilities, Volume 34(3), pp. 902 - 909
Vos, P. de Cock, P., Petry, K., van den Noortgate, W., & Maes, B. (2013). Investigating the relationship between observed mood and emotions in people with severe and profound intellectual disabilities, Journal of Intellectual Disability Research, Volume 57(5), pp. 440 – 451
Voss, M.W., Nagamatsu, L.S., Liu-Ambrose, T., & Kramer, A.F. (2011). Exercise, brain, and cognition across the life span. Journal of Applied Physiology, Volume 111, pp. 1505 – 1513
Vygotsky, L.S. (1993). The fundamentals of defectology. Translated by J.E. Knox & C.B. Stevens. In - Rieber, R.W. & Cartov, A.S. (Eds.).
The collected works of L.S. Vygotsky. New York and London: Plenum
Wachs, T.D., Moussa, W., Bishry, Z., Yunis, F., Sobhy, A.; McCabe, G., Jerome, N., Galal, O., Harrison, G, & Kirksey A. (1993). Relations between nutrition and cognitive performance in Egyptian toddlers. Intelligence. Volume 17(2). pp. 151 - 172
Walsh, R. (1997). When having means losing: Music therapy with a young adolescent with a learning disability and emotional and behavioural difficulties. British Journal of Music Therapy, Volume 11(1), pp. 13 - 19
Wang, J. (2014). Consumption of added sugars and development of metabolic syndrome components among a sample of youth at risk of obesity. Applied Physiology, Nutrition, and Metabolism, Volume 39(4), page 512
Waninge, A. (2011). Measuring physical fitness in persons with severe or profound intellectual and multiple disabilities. University of Groningen
Waninge, A., Evenhuis I.J., van Wijck, R., & Van der Schans, C.P. (2011). Feasibility and reliability of two different walking tests in people with severe intellectual and sensory disabilities. Journal of Applied Research in Intellectual Disabilities. Volume 24(6). pp. 518 - 527
Waninge, A., van der Putten, A.A., Stewart, R.E., Steenbergen, B., van Wijck, R., & van der Schans, C.P. (2013). Heart rate and physical activity patterns in persons with profound intellectual and multiple disabilities. Journal of Strength and Conditioning Research. Volume 27(11), pp. 3150 - 3158
Warburg, M. (1975). Blindness in mentally retarded children. Documenta Ophthalmologica, Volume 39(2), pp. 343 - 349
Warburg, M. (2001). Visual impairment in adult people with intellectual disability: literature review. Journal of Intellectual Disability Research, Volume 45(5), pp. 424 - 438
Ward, L., & Townsley, R. (2005). ‘It’s about a dialogue’: working with people with learning difficulties to develop accessible information. British Journal of Learning Disabilities, Volume 33 (2), pp. 59 - 64
Ward, M.J. (1988). The many facets of self-determination. National Information Center for Handicapped Children and Youth with handicaps:
Transition Issues, Volume 5, pp. 2 - 3
Ward, M.J. (1991). Self-determination revisited: Going beyond expectations. National Information Center for Handicapped Children and Youth with Handicaps: Transition Summary, Volume 7, pp. 3 - 5
Ward, M.J. (1996). Coming of age in the age of self-determination: A historical and personal perspective. In D. J. Sands & M. L. Wehmeyer (Eds.), Self-determination across the life span: Independence and choice for people with disabilities (pp. 1-14). Baltimore: Paul H. Brookes.
Ward, M.J., & Kohler, P. (1996). Promoting self-determination for individuals with disabilities: Content and process. In L. E. Powers, G. H. S. Singer, & J. Sowers (Eds.), Making our way: Building self-competence among children and youth with disabilities (pp. 275-290). Baltimore: Paul H. Brookes.
Ward, M.J., & Meyer, R.N. (1999). Self-determination for people with developmental disabilities and autism. Focus on Autism and Other Developmental Disabilities, Volume 14(3), pp. 133 – 139
Ware, J. (Ed.)(1994). Educating of Children With Profound and Multiple Learning Difficulties. London: David Fulton
Ware, J. (2003). Creating a responsive environment (second edition), David Fulton Publishers
Ware, J. (2004). Ascertaining the views of people with profound and multiple learning disabilities. British Journal of Learning Disabilities, Volume 32 (4), pp. 175 - 179
Ware, J., & Donnelly, V. (2004). Assessment for Learning for Pupils with PMLD – the ACCAC Insight Project, PMLD Link, Volume 16(3), Issue 49, pp. 12 - 17
Ware, J. (2005). Profound and Multiple Learning Difficulties. In: Lewis, A. and Norwich, B. (eds). Special Teaching for Special Children. Berkshire: Open University Press, pp. 67 - 80
Ware, J., Julian, G., & McGee, P. (2005). Education for children with severe and profound general learning disabilities in Ireland: factors influencing teachers’ decisions about teaching these pupils. European Journal of Special Needs Education. Volume 20(2), pp. 179 - 194
Ware, J. (2010). Understanding and promoting access for people with learning difficulties: seeing the opportunities and challenges of risk, European Journal of Special Needs Education. Volume 25(1), pp. 107 - 109
Warner, C. (2005). Music therapy with adults with learning difficulties and severe challenging behaviour. PhD, University of the West of
England. Available from: http://eprints.uwe.ac.uk/24593
Warren, S.A., & Mondy, L.W. (1971). To what behaviors do attending adults respond? American Journal of Mental Deficiency, Volume 75(4), pp. 419 - 455
Watson Genna, C. (2001). Tactile Defensiveness and Other Sensory Modulation Difficulties. Leaven, Volume 37(3), pp. 51 - 55
Watson, J., & Knight, C. (1991). An evaluation of intensive interaction teaching with pupils with severe learning difficulties, Child language, Teaching and Therapy, Volume 7(3) pp.10 - 25
Watson, J. (1994). Using Intensive Interaction in the education of pupils with PMLDs (ii) Intensive Interaction: two case studies, in Ware, J. (Ed.) Educating Children with Profound and Multiple Learning Difficulties. London: David Fulton.
Watson, J., & Fisher, A. (1997). Evaluating the effectiveness of Intensive Interactive teaching with pupils with profound and complex learning difficulties, British Journal of Special Education, Volume 24(2), pp. 80 - 87
Watson, J.S. (1972). Smiling, cooing, and 'The Game.' Merrill-Palmer Quarterly, Volume 18, pp. 323 - 339
Watson, T. (2002). Music Therapy with Adults with Learning Disabilities. In Bunt, L., & Hoskyns, S., (Eds.). The Handbook of Music Therapy, London: Routledge.
Watson, T., & Vickers, L. (2002). A Music and Art Therapy Group for People with Learning Disabilities. In Davies, A., & Richards, E., (Eds.) Music Therapy and Group Work: Sound Company, London: Jessica Kingsley.
Watson, T. (Ed.). (2007). Music Therapy with Adults with Learning Disabilities. Hove: Routledge.
Watson, T. (2007b). Working with people with profound and multiple learning disabilities in music therapy. In - Watson, T. (Ed.). Music Therapy with Adults with Learning Disabilities. Chapter 8, pp. 98 - 111. Hove: Routledge.
Weber, Y., & Westmoquette, K. (2010). Equine-Assisted Therapy as a Treatment Method for Children with Autism Spectrum Disorders
- a qualitative study. Department of Neurobiology, Care Sciences and Society, Karolinska Institute
Webster, M. (2008). Scientist finds fish are as clever as mammals - In Sarah Knapton article, Daily Telegraph, 29 Aug 2008
Wehman, P. (2013). Life beyond the classroom:Transition strategies for young people with disabilities (5th ed.). Baltimore, MD: Paul H. Brookes.
Wehmeyer, M.L., & Berkobien, R. (1991). Self-determination and self-advocacy: A case of mistaken identity. The Association for Persons with Severe Handicaps Newsletter, Volume 7(4)
Wehmeyer, M.L. (1992a). Self-determination and the education of students with mental retardation. Education and Training in Mental Retardation, Volume 27, pp. 302 - 314
Wehmeyer, M.L. (1992b). Self-determination: Critical skills for outcome oriented transition services. The Journal for Vocational Special Needs Education, Volume 15, pp. 3 - 9
Wehmeyer, M.L. (1993). Perceptual and psychological factors in career decision making of adolescents with and without cognitive disabilities. Career Development for Exceptional Individuals, Volume16, pp. 135 - 146
Wehmeyer, M.L. (1994). Perceptions of self-determination and psychological empowerment of adolescents with mental retardation. Education & Training in Mental Retardation & Developmental Disability, Volume 29 (1), pp. 9 - 21
Wehmeyer, M.L., & Kelchner, K. (1994). Interpersonal cognitive problem-solving skills of individuals with mental retardation. Education Training in Mental Retardation, Volume 29, pp. 265 - 278
Wehmeyer, M.L. (1995). A career education approach: Self-determination for youth with mild cognitive disabilities. Intervention in School and Clinic, Volume 30 (3), pp. 157 - 163
Wehmeyer, M.L., & Kelchner, K. (1995). The Arc's self-determination scale. Arlington, TX: The Arc National Headquarters.
Wehmeyer, M.L., & Kelchner, K. (1995). Interpersonal cognitive problem solving skills of individuals with mental retardation. Education and Training in Mental Retardation and Developmental Disabilities, Volume 29, pp. 265 - 278
Wehmeyer, M.L., & Metzler, C.A. (1995). How self-determined are people with mental retardation? The national consumer survey. Mental
Retardation, Volume 33 (2), pp. 111 - 119
Wehmeyer, M.L., Kelchner, K., & Richards, S. (1995). Individual and environmental factors related to the self-determination of adults with mental retardation. Journal of Vocational Rehabilitation, Volume 5, pp. 291 - 305
Wehmeyer, M.L., & Ward, M.J. (1995). The spirit of the IDEA mandate: Student involvement in transition planning. Journal of Vocational Special Needs Education, Volume 17, pp. 108 - 111
Wehmeyer, M.L. (1996a). Self-determination as an educational outcome: Why is it important to children, youth and adults with disabilities? In D.J. Sands & M.L. Wehmeyer (Eds.), Self determination across the life span: Independence and choice for people with disabilities (pp. 15 – 34). Baltimore, MD: Brookes.
Wehmeyer, M.L. (1996b). Student self-report measure of self-determination for students with cognitive disabilities. Education and Training in Mental Retardation and Developmental Disabilities, Volume 31, pp. 282 – 293
Wehmeyer, M.L., & Kelchner, K. (1996). Perceptions of classroom environment, locus of control and academic attributions of adolescents with and without cognitive disabilities. Career Development for Exceptional Individuals, Volume 19(1), pp. 15 - 29
Wehmeyer, M.L., Kelchner, K., & Richards, S. (1996). Essential characteristics of self-determined behaviors of adults with mental retardation and developmental disabilities. American Journal on Mental Retardation, Volume 100, pp. 632 - 642
Wehmeyer, M.L., & Schwartz, M. (1997). Self-determination and positive adult outcomes: A follow-up study of youth with mental retardation or learning disabilities. Exceptional Children, Volume 63, pp. 245 – 255
Wehmeyer, M.L. (1998). Self-determination and individuals with significant disabilities: Examining meanings and misinterpretations. Journal of The Association for Persons with Severe Handicaps, Volume 23 (1), pp. 5 - 16
Wehmeyer, M.L., & Sands, D.J. (1998). Making it happen: Student involvement in education planning, decision making, and instruction. Baltimore: Paul H. Brookes.
Wehmeyer, M.L., & Schwartz, M. (1998). The relationship between self-determination and quality of life for adults with mental retardation. Education and Training in Mental Retardation and Developmental Disabilities, Volume 33(1), pp. 3 – 12
Wehmeyer, M.L. (1999). A functional model of self-determination: Describing development and implementing instruction. Focus on Autism and Other Developmental Disabilities, Volume 14 (1), pp. 53 - 61
Wehmeyer, M.L., & Bolding, N. (1999). Self-determination across living and working environments: A matched-samples study of adults with mental retardation. Mental Retardation, Volume 37, pp. 353 – 363
Wehmeyer, M.L., Agran, M., & Hughes, C. (2000). A national survey of teacher's promotion of self-determination and student-directed learning. Journal of Special Education, Volume 34, pp. 58 - 68
Wehmeyer, M.L., Palmer, S.B., Agran, M., Mithaug, D.E., & Martin, J.E. (2000). Promoting causal agency: The self determined learning model of instruction. Exceptional Children, Volume 66, pp. 439 – 453
Wehmeyer, M.L., & Bolding, N. (2001). Enhanced self-determination of adults with intellectual disabilities as an outcome of moving to community-based work or living environments. Journal of Intellectual Disabilities Research, Volume 45, pp. 371 – 383
Wehmeyer, M.L, & Schalock, R.L. (2001). Self-Determination and Quality of Life: Implications for Special Education Services and Supports, Focus on Exceptional Children.
Wehmeyer, M.L., Abery, B., Mithaug, D.E., & Stancliffe, R.J.(2003). Theory in self-determination: Foundations for educational practice. Springfield, IL: Charles C Thomas.
Wehmeyer, M.L., & Garner, N.W. (2003). The impact of personal characteristics of people with intellectual and developmental disability on self-determination and autonomous functioning. Journal of Applied Research in Intellectual Disabilities, Volume 16, pp. 255 – 265
Wehmeyer, M.L., & Palmer, S.B. (2003). Adult outcomes from students with cognitive disabilities three years after high school: The impact of self-determination. Education and Training in Developmental Disabilities, Volume 38, pp. 131 – 144
Wehmeyer, M.L., Field, S.I., Doren, B., Jones, B., & Mason, C. (2004). Self-determination and student involvement in standards-based reform. Exceptional Children, Volume 70, pp. 413 - 425
Wehmeyer, M.L., Lawrence, M., Kelchner, K., Palmer, S., Garner, N., & Soukup, J. (2004). Whose Future Is It Anyway? A student directed transition planning process (2nd ed.). Lawrence, KS: Beach Center on Disability.
Wehmeyer, M.L. (2005). Self-determination and individuals with severe disabilities: Reexamining meanings and interpretations. Research and Practice for Persons with Severe Disabilities, Volume 30, pp. 113 – 120
Wehmeyer, M.L., Agran, M., Hughes, C., Martin, J., Mithaug, D.E., & Palmer, S.B. (2007). Promoting self-determination in students with intellectual and developmental disabilities. New York: Guilford.
Wehmeyer, M.L., & Field, S. (2007). Self-determination: Instructional and assessment strategies. Thousand Oaks, CA: Corwin Press.
Wehmeyer, M.L. (2008). The impact of disability on adolescent identity. In M. Sadowski (Ed.), Adolescents at school: Perspectives on youth, identity, and education (2nd ed., pp. 167 – 184). Cambridge: Harvard Education Press.
Wehmeyer, M.L., & Shogren, K.A. (2008). Self-determination and learners with autism spectrum disorders. In R. Simpson & B. Myles (Eds.), Educating children and youth with autism: Strategies for effective practice (2nd ed., pp. 433 – 476). Austin, TX: Pro-Ed.
Wehmeyer, M.L., Palmer, S.B., Lee, Y, Williams-Diehm, K.L., & Shogren, K.A. (2011). A randomized-trial evaluation of the effects of Whose Future is it Anyway? on self-determination. Career Development for Exceptional Individuals, Volume 34, pp. 45 - 56
Wehmeyer, M.L., Fields, S., & Thoma, C. (2012). Self-determination in adolescent transition education. In M. L. Wehmeyer & K. A. Webb (Eds.), Handbook of Adolescent Transition for Youth with Disabilities (pp. 171 - 190). New York: Routledge.
Wehmeyer, M.L., & Shogren, K.A. (2012). Self-determination: Getting students involved in leadership. In P. Wehman (Ed.), Life beyond the classroom: Transition strategies for young people with disabilities (5th ed., pp. 39 - 66). Baltimore: Paul H. Brookes.
Wehmeyer, M.L., Shogren, K.A., Palmer, S.B., Williams-Diehm, K.L., Little, T.D., & Boulton, A.(2012). The impact of the self-determined learning model of instruction on student self-determination. Exceptional Children, Volume 78, pp. 135 – 153
Wehmeyer, M.L., & Smith, T.E.C. (2012). Promoting self-determination and social inclusion: A review of research-based practices. In D. Zagar, M. L. Wehmeyer, & R. Simpson (Eds.), Educating students with autism spectrum disorders: Research-based principles and practices (pp. 227 - 246). New York: Taylor & Francis.
Wehmeyer, M.L., Tasse, M., Davies, D., & Stock, S. (2012). Support needs of adults with intellectual disability across domains: The role of technology. Journal of Special Education Technology, Volume 27 (2), pp.11 - 22
Wehmeyer, M.L. (2013). Self-determination: The most natural support. In M. L. Heward (Ed.), Exceptional children: An introductory survey of special education (10th ed., pp. 132 - 133). Upper Saddle River, NJ: Merrill/Prentice Hall.
Wehmeyer, M.L., & Abery, B.H. (2013). Self-Determination and Choice. Intellectual and Developmental Disabilities. Volume 51 (5), pp. 399 – 411
Wehmeyer, M.L., & Shogren, K.A. (2013). Self-determination and student involvement. In P. Wehman (Ed.), Life beyond the classroom: Transition strategies for young people with disabilities (5th ed., pp. 41 - 68). Baltimore: Paul H. Brookes.
Wehmeyer, M.L., & Little, T.D. (2013). Self-determination, positive psychology, and disability. In M.L. Wehmeyer (Ed.), Handbook of positive psychology and disability (pp. 116 - 136). Oxford, UK: Oxford University Press.
Wehmeyer, M.L., Palmer, S.B., Shogren, K.A., Williams-Diehm, K., & Soukup, J. (2013). Establishing a causal relationship between interventions to promote self-determination and enhanced student self-determination. Journal of Special Education, Volume 46(4), pp. 195 –210
Wehmeyer, M.L. (2014). Self-Determination: A Family Affair. Family Relations, Volume 63 (February): pp. 178 – 184
Wells, M.E., & Smith, D.W. (1983). Reduction of self-injurious behavior of mentally retarded persons using sensory integrative techniques. American Journal of Mental Deficiency, Volume 87, pp. 664 – 666
Welsh Assembly Government (2006). Routes for Learning: Assessment Materials for Learners with Profound Learning Difficulties and Additional Disabilities. Cardiff: Welsh Assembly Government
Werner, E.E., & Smith, R.S. (1980). An epidemiologic perspective on some antecedents and consequences of childhood mental health problems and learning disabilities. In S. Chess and A. Thomas (Eds.), Annual Progress in Child Psychiatry and Development. Brunner/Mazel, New York, pp.133 - 147
Werner, S. (2012). Individuals with Intellectual Disabilities: A Review of the Literature on Decision-Making since the Convention on the Rights of People with Disabilities (CRPD), Public Health Reviews,Volume 34 (2), pp. 1 - 27
Wertheimer, A. (ed.) (2000) Everyday Lives; Everyday Choices. London: The Foundation for People with Learning Disabilities.
Westergaard, G.C., & Hyatt, C.W. (1994). The responses of bonobos (Pan paniscus) to their mirror images: Evidence of self recognition.
Human Evolution, Volume 9(4), pp. 273 – 27
Wheeler, B.L. (1999). Experiencing Pleasure in Working with Severely Disabled Children. Journal of Music Therapy, Volume 36(1), pp. 56 - 80
Whitaker, S. (1989). Quality of life and people with a very profound handicap. British Journal of Mental Subnormality, Volume 35, pp. 3 - 7
White, B. (2015). ‘What sound can you make?’ A case study of a music therapy group for children with autism, learning disabilities and challenging behaviours. Approaches: An Interdisciplinary Journal of Music Therapy, Volume 7(2), pp. 197 - 206
Whiteley, P., Rodgers, J., Savery, D., & Shattock, P. (1999). A gluten-free diet as an intervention for autism and associated spectrum disorders: preliminary findings. Autism, Volume 3(1), pp. 45 - 65
Whiteley, P., Haracopos, D., Knivsberg, A.M., Reichelt, K.L., Parlar, S., Jacobsen, J., Seim, A., Pedersen, L., Schondel, M.. & Shattock, P. (2010). The ScanBrit randomised, controlled, single-blind study of a gluten-and casein-free dietary intervention for children with autism spectrum disorders. Nutritional Neuroscience, Volume 13(2), pp. 87 - 100
Whiteley, P., Shattock, P., Knivsberg, A.M., Seim, A., Reichelt, K.L., Todd, L., Carr, K., & Hooper, M. (2013). Gluten-and casein-free dietary intervention for autism spectrum conditions. Frontiers in Human Neuroscience. Volume 6, article 344, pp. 1 - 8
Whiteley, P. (2015). Nutritional management of (some) autism: a case for gluten-and casein-free diets? Proceedings of the Nutrition Society, Volume 74(3), pp. 202 - 207
Whitman, T.L. (1990). Self-regulation and mental retardation. American Journal on Mental Retardation, Volume 94 (4), pp. 347 - 362
Whittle, H., & Townend, S. (1995). Communication and technology for students with profound and multiple learning disabilities (PMLD) within the classroom setting. Communication Matters, Volume 9(2), pp. 15 - 16
Wier, K., Cooney, M., Walter, M., Moss, C., & Carter, E.W. (2011). Fostering self-determination among children with disabilities: Ideas
from parents for parents. Madison, WI: Natural Supports Project, Waisman Center, University of Wisconsin-Madison
Wiggs, L., & Stores, G. (1996) Severe sleep disturbance and daytime challenging behaviour in children with severe learning disabilities. Journal of Intellectual Disability Research. Volume 40(6), pp. 518 – 528
Wiggs, L., & Stores, G. (1998). Behavioural treatment for sleep problems in children with severe learning disabilities and challenging daytime behaviour: effect on sleep patterns of mother and child. Journal of Sleep Research, Volume 7(2), pp. 119 - 126
Wiggs, L., & Stores, G. (2004). Sleep patterns and sleep disorders in children with autistic spectrum disorders: insights using parent report and actigraphy. Developmental Medicine and Child Neurology, Volume 46(6), pp. 372 - 380
Wigram, A.L. (1988). Music therapy: Developments in mental handicap. Psychology of Music, Volume 16, pp. 42 – 51
Wigram, T., & DeBacker, J. (Eds.). (1999). Clinical Applications of Music Therapy in Developmental Disability, Pediatrics and Neurology. London: Jessica Kingsley.
Wigram, T., Pederson, I. N. & Bonde, L.O. (2002). A Comprehensive Guide to Music Therapy: Theory, Clinical Practice, Research and Training. London: Jessica Kingsley Publishers.
Wigram, T., & Lawrence, M. (2005). Music therapy as a tool for assessing hand use and communicativeness in children with Rett Syndrome. Brain & Development, Volume 27, pp. 95 - 96
Wilbarger P., & Wilbarger J. (1991). Sensory defensiveness in children. Santa Barbara, CA: Avanti Educational Programs.
Wilder, J., & Granlund, M. (2003). Behaviour style and interaction between seven children with multiple disabilities and their caregivers. Child: care, health and development, Volume 29(6), pp. 559 - 567
Wilkens, J. (2017). Photographic Memory: Photographic Memory Training, Advanced Techniques to Improve Your Memory & Strategies to Learn Faster. Create Space Independent Publishing Platform
Wilkinson, C. (1994). Teaching pupils with profound and multiple learning difficulties to exert control, in J. Coupe O’Kane & B. Smith (eds) Taking Control: enabling people with learning difficulties, London: David Fulton
Williams, C.A., Peters, S.U., & Calculator, S.N. (2009). Facts About Angelman Syndrome, 7th Edition, January 1, 2009. Angelman Syndrome Foundation
Williams, M. (2010). Meaningful participation for people with PMLD. PMLD Link. Volume 22(2), Issue 66, pp. 23
Williams, R.K. (1991). Choices, communication, and control: A call for expanding them in the lives of people with severe disabilities. In L. Meyer, C. Peck, L. Brown (Eds.), Critical Issues In The Lives Of People With Severe Disabilities (pp. 543 - 544). Baltimore: Paul H. Brookes.
Williams, S. Dagnan, D. Rodgers, J., & McDowell, K. (2012). Changes in attributions as a consequence of training for challenging and complex behaviour for carers of people with learning disabilities: A systematic review. Journal of Applied Research in Intellectual Disabilities, Volume 25(3), pp. 203 – 216
Williams-Diehm, K., Wehmeyer, M.L., Palmer, S., Soukup, J.H., & Garner, N. (2008). Self-determination and student involvement in
transition planning: A multivariate analysis. Journal on Developmental Disabilities, Volume 14(1), pp. 25 – 36
Willink, M., Widdershoven, G., van Schrojenstein Lantman-de Valk, H., Metsemakers, J. & Dinant, G. (2009). Autonomy in relation to health among people with intellectual disability: a literature review. Journal of Intellectual Disability Research, Volume 53(9), pp. 816 - 826
Willis, D., Grace, P.J., & Roy, C. (2008). A central unifying focus for the discipline: Facilitating humanization, meaning, choice, quality of life, and healing in living and dying. Advances in Nursing Science, Volume 31(1), pp. 28 - 40
Willner, P., Bailey, R., Parry, R., & Dymond, S. (2010). Performance in temporal discounting tasks by people with intellectual disabilities reveals difficulties in decision-making and impulse control. American Journal on Intellectual and Developmental Disabilities. Volume 115, pp. 157 - 171
Willoughby-Booth, S. & Pearce, J. (1998). On the edge: Art therapy for people with learning difficulties and disordered personalities. In M. Rees (Ed.), Drawing on difference: Art therapy with people who have learning difficulties, pp.63 – 78. London: Routledge.
Wilson, E.B. (1975). Sensory integration therapy for children with learning disorders. Rehabilitation in Australia, Volume 12, 27 – 29
Wilson, M.M., & Morley, J.E. (2003). Impaired cognitive function and mental performance in mild dehydration. European Journal of Clinical Nutrition. Volume 57(2), Supplement. pp. 24 - 29
Wilson, P.G., Reid, D.H., Phillips, J.F., & Burgio, L.D. (1984). Normalization of institutional mealtimes for profoundly retarded persons: Effects and non-effects of teaching family-style dining. Journal of Applied Behavior Analysis, Volume 17, pp. 189 - 201
Wilson, P.G., Reid, D.H., & Green, C.W. (2006). Evaluating and increasing in-home leisure activity among adults with severe disabilities in supported independent living. Research in Developmental Disabilities, Volume 27(1), pp. 93 - 107
Wilson, T.D. (2009). Know thyself, Perspectives in Psychological Science, Volume 4, pp. 384 – 389
Winchel, R.M., & Stanley, M. (1991). Self-injurious behaviour: a review of the behaviour and biology of self-mutilation. The American Journal of Psychiatry, Volume 148(3), pp. 306 - 317
Windsor, J., Piche, L.M. & Locke, P.A. (1994). Preference testing: a comparison of two presentation methods. Research in Developmental Disabilities, 15, pp. 439 - 455
Winefield, A.H. (1983). Cognitive performance deficits induced by exposure to response-independent positive outcomes. Motivation and Emotion, Volume 7, pp. 145 - 155
Wise, J. (2011). Shared decision making must move from rhetoric to reality, says King’s Fund. BMJ, 2011; 343: d4734
Wolf, J., & Joannou, K. (2012), Choice Making and Individuals with Significant Disabilities, University of Kansas
Wolf-Schein, E. (1998). Considerations in Assessment of Children with Severe Disabilities including Deaf-blindness and Autism. International Journal of Disability, Development and Education, Volume 45(1). pp. 35 - 55
Wong, J.G., Clare, I.C.H., Holland, A.J., Watson, P.C., & Gunn, M. (2000). The capacity of people with a ‘mental disability’ to make a health care decision. Psychological Medicine, Volume 30, pp. 295 - 306
Wood, D., Wood, H., Griffiths, A., & Howarth, A. (1986). Teaching and talking with deaf children. J. Wiley and Sons
Wood, W.M., Fowler, C.H., Uphold, N., & Test, D.W. (2005). A review of self- determination interventions with individuals with severe disabilities. Research & Practice for Persons with Severe Disabilities, Volume 30 (3), pp. 121 - 146
Woodcock, J., & Lawes, C. (1995). Music Therapy and People with Severe Learning Difficulties who Exhibit Self-injurious Behaviour. In: Wigram, T., Saperston, B., & West, R., (Eds.),The Art and Science of Music Therapy: a Handbook, London: Harwood Academic Press.
Woollett, K. & Macguire, E.A. (2011). Acquiring “the Knowledge” of London's Layout Drives Structural Brain Changes. Current Biology. Volume 21(24-2). pp. 2109 – 2114
Wragg, T. (1996). Year of the twerp and big chief I-spy. Last Word. Times Educational Supplement. No. 4138, Friday January 5th, page 64
Wyatt, M. (2001). The Disabled Enclave: Issues in the Dance Movement Therapist’s Counter transference with Severely Handicapped Adolescents. Master of Arts in Dance Movement Therapy, Unpublished Dissertation presented to the faculty of Laban Centre, London. Goldsmith, University of London
Wylie, M.E. (1983). Eliciting Vocal Responses in Severely and Profoundly Mentally Handicapped Subjects. Journal of Music Therapy, Volume 20(4), pp. 190 - 200
Wyman, R. (1986). Multiply handicapped children. Souvenir Press
Wyman, R. (2000). Making Sense Together: Practical approaches to supporting children who have multisensory impairments. Second Edition. Human Horizons Series
Wynn, K. (1992). Addition and subtraction by human infants. Nature, Volume 358(6389), pp. 749 - 750
Yack, E., Sutton, S., & Aquilla, P. (1998). Building bridges through sensory integration. Willowdale, Ontario: Special Needs Project.
Yamaki, K. (2005). Body weight status among adults with intellectual disability in the community. Mental Retardation, Volume 43(1), pp. 1 - 10
Yang, L.J. (2003). Combination of extinction and protective measures in the treatment of severely self-injurious behaviour. Behavioural Interventions, Volume 18, pp. 109 - 121
Yang, Q., Zhang, Z., Gregg, E., Flanders, D., Merritt, R., & Hu, F. (2014). Added Sugar Intake and Cardiovascular Diseases Mortality Among US Adults. JAMA Internal Medicine, Volume 174 (4), pp. 516 - 524
Yasuhara, A., & Sugiyama, Y. (2001). Music therapy for children with Rett syndrome. Brain & Development, Volume 23, pp. 82 - 84.
York, J., Nietupski, J., & Hamre-Nietupski, S. (1985). A decision making process for using microswitches. Journal of the Association for the Severely Handicapped, Volume 10, pp. 214 - 223
Yu, C.T., Spevack, S., Hiebert, R., Martin, T.L., Goodman, R., Martin, T.G., Harapiak, S. & Martin, G.L. (2002). Happiness indices among persons with profound and severe disabilities during leisure and work activities. Education and Training in Mental Retardation and Developmental Disabilities. Volume 37(4), pp. 421 – 426
Yu, C.T., & Martin, G.L. (2003). Tangibles, Pictures, and Verbal Descriptions: Which Should Be Used in Choice Presentations? Journal on Developmental Disabilities. Volume 10(1), pp. 137 -140
Yudkin, J. (1972). Pure, White and Deadly: The Problem of Sugar. London: Davis-Poynte
Yudkin, J. (2012). Pure, White and Deadly: The Problem of Sugar (revised edition). Penguin
Zainuddin, M.S.A., & Thuret, S. (2012). Nutrition, adult hippocampal neurogenesis and mental health. British Medical Bulletin. Volume 103(1). pp. 89 -114
Zangari, C., Lloyd, L., & Vicker, B. (1994). AAC: An historic perspective, AAC, March 1994, Volume 10 (1), pp. 27 - 59
Zeedyk, M.S., Davies, C.E., Parry, S., & Caldwell, P. (2009).Fostering social engagement in Romanian children with communicative impairments: The experiences of newly trained practitioners of Intensive Interaction, British Journal of Learning Disabilities, Volume 37(3), pp.186 - 196
Zeedyk, M.S., Caldwell, P., & Davies, C.E. (2009). How rapidly does Intensive Interaction promote social engagement for adults with profound learning disabilities and communicative impairments? European Journal of Special Needs Education, Volume 24(2), pp.119 – 137
Zeng Y., Zhao Y., & Bai J. (2016). Towards Robot Self-consciousness (I): Brain-Inspired Robot Mirror Neuron System Model and Its Application in Mirror Self-recognition. In - Liu CL., Hussain A., Luo B., Tan K., Zeng Y., Zhang Z. (Eds.). Advances in Brain Inspired Cognitive Systems. Lecture Notes in Computer Science, Volume 10023. Springer, Cham
Zhang, D., Wehmeyer, M.L, & Chen, L. (2005). Parent and teacher engagement in fostering the self-determination of students with disabilities: A comparison between the United States and the Republic of China. Remedial and Special Education, Volume 26, pp. 55 - 64
Zhang, J., Mayton, M. R., & Wheeler, J.J. (2013). Effectiveness of gluten-free and casein-free diets for individuals with autism spectrum disorders: An evidence-based research synthesis. Education and Training in Autism and Developmental Disabilities, Volume 48(2), pp. 276 - 287
Zhou, L., Iwata, B.A., Goff, G.A., & Shore, B.A. (2001). Longitudinal analysis of leisure-item preferences. Journal of Applied Behavior Analysis, Volume 34, pp. 179 – 184
Zijlstra, H.P., Vlaskamp, C., & Buntinx, W.H. (2001). Direct-care staff turnover: An indicator of the quality of life of individuals with profound multiple disabilities. European Journal on Mental Disability, Volume 22, pp. 39 – 56
Zijlstra, R. (2003). Dancing with elephants. A study of the implementation of the education program in the care for people with severe multiple disabilities. Groningen: Stichting Kinderstudies.
Zijlstra, R., & Penning, C. (2004). People with severe intellectual and multiple disabilities. In - M. Kersten & D. Flikweert (Eds.), Onderzoek over grenzen thematische rapportages en beschouwingen naar aanleiding van het 12de IASSID, Montpellier 2004 (pp. 49 – 63). Utrecht: NGBZ en LKNG/NIZW
Zijlstra, H.P., & Vlaskamp, C. (2005). Leisure provision for persons with profound intellectual and multiple disabilities: quality time or killing time? Journal of Intellectual Disability Research, Volume 49(6), pp. 434 - 448
Zijlstra, H.P., & Vlaskamp, C. (2005b). The impact of medical conditions on the support of children with profound intellectual and multiple disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 18(2), pp. 151 - 161
Zilbovicius, M., Garreau, B., Tzourio, N., Mazoyer, B., Bruck, B., Martinot, J.L., Raynaud, C., Samson, Y., Syrota, A., & Lelord, G. (1992). Regional cerebral blood flow in childhood autism: a SPECT study. American Journal of Psychiatry, Volume 149(7), pp. 924 - 930
Zissermann, L. (1992). The effects of deep pressure on self stimulating behaviors in a child with autism and other disabilities. American Journal of Occupational Therapy, Volume 46, pp. 547 – 551
Ziviani, J., Poulsen, A., & O'Brien, A. (1982). Effect of a sensory integrative/neurodevelopmental programme on motor and academic
performance of children with learning disabilities. Australian Occupational Therapy Journal, Volume 29, pp. 27 - 33
Zuckerman, M., Porac, J., Lathin, D., & Deci, E.L. (1978). On the Importance of Self‐Determination for Intrinsically‐Motivated Behavior. Personality and Social Psychology Bulletin, Volume 4 (3), pp. 443 ‐ 446
Zull, J.E. (2004). The art of changing the brain. Educational Leadership, Volume 62(1), 68 - 72
Return to Top of Page

To return to the top of this page click on the up arrow key symbol to the left.
