Communication and Loss: Ideas for Practice
"However, knowing that we cannot solve grief, nor prevent it, knowing that it is the price we pay for our attachment to others, we can still hope not to make it worse; especially not worse for people who are already vulnerable because they are lonely, or very young or very old, or sick, or handicapped in some way." (OSWIN M., 1991)
"A severely handicapped man, who is non-verbal, knelt before the open casket of his friend. He bowed his head as though in prayer, then reached in the casket to touch the corpse After rubbing the arm of the deceased, he stood and headed towards the pew. After taking four or five steps, he turned and waved goodbye. The staff and I had no idea that this man had an understanding of death." (Marquardt, 1989, page 347)
There are times in everyone's life when we are saddened by loss. This does not always have to be the death of someone close but can also involve the loss of:
- a lover (on the break up of a relationship);
- something special to us;
- position or employment;
- financial stability;
- home;
- other.
At such times, we experience a range of emotions ranging from denial, anger and grief to confusion and angst. If we feel such emotions then imagine, therefore, how much more problematic it must be for those individuals who are experiencing some form of learning difficulty. It might be assumed that those experiencing the most profound difficulties are 'shielded' from such emotions by their cognitive state but this would be erroneous: while the individual might have little or no concept of death (or other other forms of loss), s/he will 'understand' that a significant person who was there every day for them is now no longer there, that a favourite object or thing which has accompanied their journey to this point no longer is with them. This 'realisation' can lead to great anguish, confusion, and upset which may result in a change in behaviour. A lack of ability to communicate about such understandings and emotions only compounds the issue. To assume that a person's cognitive level will shield them from all emotions is, therefore, incorrect. Anyone in a conscious state can feel emotions unless there is significant damage to those areas of the brain in which such feelings are experienced. Even then, the individual might be 'asking' why is this person no longer around? Is it something to do with me? Has someone evil taken them away? Will they return and take me away too? Simply because we do not know how an individual is conceiving a particular loss does not mean that we should assume that there will be no response at all.
The concept of loss for individuals experiencing learning difficulties is often glossed over or not addressed at all in books on 'Mental Handicap', 'Retardation' (terms I generally do not use) or Learning Disabilities or Difficulties. If you have such reference works on your shelf, take them down and look in the index for 'loss, or 'bereavement' or 'death', it is likely that such terms will not be found there. Research has shown that there is much confusion about death amongst people who are experiencing Learning Difficulties (McEvoy 1989, Myreddi & Narayan 1993) and that such individuals can have rich and varied dreams about people who have died (Turner and Graffam 1987).
The price we all have to pay for becoming attached to another person or thing are the strong emotional reactions following the loss of the same for whatever reason. Such emotional reactions affect us ALL: rich or poor, strong or weak, able or ...
"When we work with a client with mental retardation, we must never assume that he 'doesn't know' about the loss and the experience
of grieving ... we must, in fact, proceed on the assumption that he knows about the loss, that he feels it emotionally, and that it affects
his physical body and his spiritual center." Howell, M.C. (1989)
This page therefore deals with issues of loss and presents a set of ideas for good practice which may be of help in such circumstances. It is for you to decide which of the ideas presented are of any worth and which to use. Where possible, links to other materials are provided.
"A severely handicapped man, who is non-verbal, knelt before the open casket of his friend. He bowed his head as though in prayer, then reached in the casket to touch the corpse After rubbing the arm of the deceased, he stood and headed towards the pew. After taking four or five steps, he turned and waved goodbye. The staff and I had no idea that this man had an understanding of death." (Marquardt, 1989, page 347)
There are times in everyone's life when we are saddened by loss. This does not always have to be the death of someone close but can also involve the loss of:
- a lover (on the break up of a relationship);
- something special to us;
- position or employment;
- financial stability;
- home;
- other.
At such times, we experience a range of emotions ranging from denial, anger and grief to confusion and angst. If we feel such emotions then imagine, therefore, how much more problematic it must be for those individuals who are experiencing some form of learning difficulty. It might be assumed that those experiencing the most profound difficulties are 'shielded' from such emotions by their cognitive state but this would be erroneous: while the individual might have little or no concept of death (or other other forms of loss), s/he will 'understand' that a significant person who was there every day for them is now no longer there, that a favourite object or thing which has accompanied their journey to this point no longer is with them. This 'realisation' can lead to great anguish, confusion, and upset which may result in a change in behaviour. A lack of ability to communicate about such understandings and emotions only compounds the issue. To assume that a person's cognitive level will shield them from all emotions is, therefore, incorrect. Anyone in a conscious state can feel emotions unless there is significant damage to those areas of the brain in which such feelings are experienced. Even then, the individual might be 'asking' why is this person no longer around? Is it something to do with me? Has someone evil taken them away? Will they return and take me away too? Simply because we do not know how an individual is conceiving a particular loss does not mean that we should assume that there will be no response at all.
The concept of loss for individuals experiencing learning difficulties is often glossed over or not addressed at all in books on 'Mental Handicap', 'Retardation' (terms I generally do not use) or Learning Disabilities or Difficulties. If you have such reference works on your shelf, take them down and look in the index for 'loss, or 'bereavement' or 'death', it is likely that such terms will not be found there. Research has shown that there is much confusion about death amongst people who are experiencing Learning Difficulties (McEvoy 1989, Myreddi & Narayan 1993) and that such individuals can have rich and varied dreams about people who have died (Turner and Graffam 1987).
The price we all have to pay for becoming attached to another person or thing are the strong emotional reactions following the loss of the same for whatever reason. Such emotional reactions affect us ALL: rich or poor, strong or weak, able or ...
"When we work with a client with mental retardation, we must never assume that he 'doesn't know' about the loss and the experience
of grieving ... we must, in fact, proceed on the assumption that he knows about the loss, that he feels it emotionally, and that it affects
his physical body and his spiritual center." Howell, M.C. (1989)
This page therefore deals with issues of loss and presents a set of ideas for good practice which may be of help in such circumstances. It is for you to decide which of the ideas presented are of any worth and which to use. Where possible, links to other materials are provided.
Death or Loss?
This webpage will use the term 'Loss' rather than 'Death' and not, as you may think, because loss is a 'nicer' term to use. It is because the page is about loss and death is just one form of loss that a person may experience. A close friend may move away, we may lose some special thing that we have cherished for a long period, a routine may change in which we found particular comfort. All these and many more can be experienced as a loss. Death is a particular form of loss and one with which we must all deal at varying points in our lives. The way in which we learn to cope with it may be different for each person but cope we must 'life goes on'. What other forms of loss that may affect the individual can we think? While some may seem trivial to us when we compare them to a great loss such as death, they may nevertheless be very significant to an individual experiencing a learning difficulty:
- Loss of friendship (Fall out, Person moves away, finds a new job, changes shifts ...);
- Loss of love (break up of a relationship);
- Loss of routine (changes in timetable, care procedure change, transition);
- Loss of home or placement (transition to a new establishment)(short-term residential care, long-term residential care);
- Loss of identity (person becomes a 'number' within a large group of people);
- Loss of stability/security (there is comfort in predictability. Such comfort may be lost when things are forced to change);
- Loss of financial stability;
- Loss of position (employment, part of a team, part of a group);
- Loss of independence (moving placement may involve going to a place with stricter rules and guidelines for example;
- Loss of a possession (Comforter, favourite cherished item, something of significance, treasured item);
- Loss of self-esteem / dignity (changes in placement, practice or staff create a situation in wich such loss occurs);
- Loss of life (death).
I doubt if there is a single person reading this page who has not experienced at least one of the above forms of loss with all the subsequent emotions that it brings. We know what it feels like; even if we consider ourselves to be strong and have found ways to cope with the loss. For some the grief felt is overwhelming and goes on and on. Individuals experiencing learning difficulties (at all levels) will also feel loss; to be human is to feel loss. It is for all significant others to do what they can to help the individual understand and cope with their loss with empathy and sensitivity. Loss can be even greater for the individual as one loss can lead to further losses: for example, if an individual was living with a parent as a primary carer in the family home for all his/her life and then the parent dies, not only does the individual lose the much loved parent but now faces the possibility of having to move out from the home into a residential facility with new routines and new faces. In this instance, the loss is not just the person but also the home, the routine, the forms of meals, the ... We know how hard it is to cope with one loss, imagine how much harder then is it to cope with compound losses when you have a learning difficulty. Loss of a parent and a home ... that is a trauma that none of us would cope with easily.
In all the above list of losses there is a commonly element: change. The ideas below are therefore suggestions for coping with a change in our lives that may affect us emotionally.
- Loss of friendship (Fall out, Person moves away, finds a new job, changes shifts ...);
- Loss of love (break up of a relationship);
- Loss of routine (changes in timetable, care procedure change, transition);
- Loss of home or placement (transition to a new establishment)(short-term residential care, long-term residential care);
- Loss of identity (person becomes a 'number' within a large group of people);
- Loss of stability/security (there is comfort in predictability. Such comfort may be lost when things are forced to change);
- Loss of financial stability;
- Loss of position (employment, part of a team, part of a group);
- Loss of independence (moving placement may involve going to a place with stricter rules and guidelines for example;
- Loss of a possession (Comforter, favourite cherished item, something of significance, treasured item);
- Loss of self-esteem / dignity (changes in placement, practice or staff create a situation in wich such loss occurs);
- Loss of life (death).
I doubt if there is a single person reading this page who has not experienced at least one of the above forms of loss with all the subsequent emotions that it brings. We know what it feels like; even if we consider ourselves to be strong and have found ways to cope with the loss. For some the grief felt is overwhelming and goes on and on. Individuals experiencing learning difficulties (at all levels) will also feel loss; to be human is to feel loss. It is for all significant others to do what they can to help the individual understand and cope with their loss with empathy and sensitivity. Loss can be even greater for the individual as one loss can lead to further losses: for example, if an individual was living with a parent as a primary carer in the family home for all his/her life and then the parent dies, not only does the individual lose the much loved parent but now faces the possibility of having to move out from the home into a residential facility with new routines and new faces. In this instance, the loss is not just the person but also the home, the routine, the forms of meals, the ... We know how hard it is to cope with one loss, imagine how much harder then is it to cope with compound losses when you have a learning difficulty. Loss of a parent and a home ... that is a trauma that none of us would cope with easily.
In all the above list of losses there is a commonly element: change. The ideas below are therefore suggestions for coping with a change in our lives that may affect us emotionally.
Straight Talking
"Some people with learning difficulties may be given all sorts of peculiar ideas about what has happened,perhaps being told that the dead person has 'gone away' or 'gone to sleep'. Such explanations will be very frightening and terrible ..." (OSWIN M. 1991)
We all find talking about death difficult. It is probably one of the reasons that there are so many euphemisms for the term: for example such things as 'passed on', 'gone away', gone to a better place, suffering ended ... However, while we might comprehend just substitutions Individuals experiencing difficulties will not and they will only be further confused by them. While we might have good intentions and believe that we are shielding the individual from the harsh realities of life we are actually not helping the individual to come to terms with the loss. What is required is a clear and simple use of language and not substitutions within indirect references.
The most extreme form of shielding is not to inform the individual at all, after all, 'out of sight is out of mind', isn't it? Actually, it isn't! If there is a loss, the individual is likely to be aware of it at some level. We cannot judge at what level that may be and assumptions of a lack of understanding on the part of the individual are not helpful.
Thus, it is not 'Lenny has passed away' it is 'Lenny has died'. It is never useful to use terms like 'kicked the bucket' or 'gone to meet his maker' because they have little meaning for those experiencing learning difficulties. I once used such terminology when I was working in Taiwan; although the person I was talking to spoke very good English, he was utterly confused by my expression and got the 'wrong end of the stick'. I use 'wrong end of the stick' here to illustrate the point ... English is full of such expressions, metaphor, similes, euphemisms ... As many individuals will take them literally, they should be avoided.
Straight talking does not mean bluntness and a lack of consideration and empathy. "He's died. You'll have to deal with it", is not what straight talking, in this instance means, at all. We can be gentle, kind and considerate and still not couch our language in metaphors which will be difficult if not impossible for the individual to comprehend.
"To die, to sleep;To sleep: perchance to dream: ay, there's the rub; For in that sleep of death what dreams may come
when we have shuffled off this mortal coil." Shakespeare Hamlet
We all find talking about death difficult. It is probably one of the reasons that there are so many euphemisms for the term: for example such things as 'passed on', 'gone away', gone to a better place, suffering ended ... However, while we might comprehend just substitutions Individuals experiencing difficulties will not and they will only be further confused by them. While we might have good intentions and believe that we are shielding the individual from the harsh realities of life we are actually not helping the individual to come to terms with the loss. What is required is a clear and simple use of language and not substitutions within indirect references.
The most extreme form of shielding is not to inform the individual at all, after all, 'out of sight is out of mind', isn't it? Actually, it isn't! If there is a loss, the individual is likely to be aware of it at some level. We cannot judge at what level that may be and assumptions of a lack of understanding on the part of the individual are not helpful.
Thus, it is not 'Lenny has passed away' it is 'Lenny has died'. It is never useful to use terms like 'kicked the bucket' or 'gone to meet his maker' because they have little meaning for those experiencing learning difficulties. I once used such terminology when I was working in Taiwan; although the person I was talking to spoke very good English, he was utterly confused by my expression and got the 'wrong end of the stick'. I use 'wrong end of the stick' here to illustrate the point ... English is full of such expressions, metaphor, similes, euphemisms ... As many individuals will take them literally, they should be avoided.
Straight talking does not mean bluntness and a lack of consideration and empathy. "He's died. You'll have to deal with it", is not what straight talking, in this instance means, at all. We can be gentle, kind and considerate and still not couch our language in metaphors which will be difficult if not impossible for the individual to comprehend.
"To die, to sleep;To sleep: perchance to dream: ay, there's the rub; For in that sleep of death what dreams may come
when we have shuffled off this mortal coil." Shakespeare Hamlet
Preparation for Loss
We are all human and it is the human condition to want to shield the 'vulnerable' from sadness, grief and things that are unpleasant. However, in such practice we may be doing more harm than good. It is really important that we prepare individuals for loss such that they are are more able to cope with it when it happens and happen it will; it is no good putting it off or pretending that everything will be well for ever.
Thus, we need to think about all the forms of loss that may affect an individual from time to time (Death is but one form of loss but nevertheless an important issue with which we must deal) and prepare the individual for it. Once we have listed those forms of loss that may affect the individual it is easier to consider ways in which significant others (staff, relatives, etc) can help and inform the individual. Preparation is crucial. Coping with loss without being prepared is so much more difficult and stressful. Having some understanding of what has happened, knowing what to do, to whom to turn, and to whom we can talk is very important. Preparation for loss should follow the distal to proximal principle....
Thus, we need to think about all the forms of loss that may affect an individual from time to time (Death is but one form of loss but nevertheless an important issue with which we must deal) and prepare the individual for it. Once we have listed those forms of loss that may affect the individual it is easier to consider ways in which significant others (staff, relatives, etc) can help and inform the individual. Preparation is crucial. Coping with loss without being prepared is so much more difficult and stressful. Having some understanding of what has happened, knowing what to do, to whom to turn, and to whom we can talk is very important. Preparation for loss should follow the distal to proximal principle....
Distal To Proximal Principle
The distal (far away) to proximal (very near) principle for loss suggests that we introduce an individual to loss by beginning with items that are distal to the individual which s/he will not find too distressing. For example, Children's first experience of death may be during a walk in the woods and coming across a dead animal with their parents or when the cat brings home a dead creature that it has caught or when an insect or spider invades the house and someone kills it. All these times and others like them are opportunities to introduce the concept of death and dying in a distal fashion. The individual needs to come to understand that all life ceases when death occurs and that the dead creature does not come back to life and the process is a one way affair. We are actually surrounded by death. We cannot eat a piece of meat without it meaning the death of a living creature, we cannot wear an item of leather or sit on leather furniture without something having to die to make this provision for us. We do not normally think in these ways about such things as it is uncomfortable but, nevertheless, it is a fact. Furthermore, there are books (even for children) in which one of the main characters dies (For example, Charlotte's Web by E.B. White and I'll always love you by Hans Wilhelm) which could also be used as an opportunity to discuss the topic of loss. Indeed, there are many opportunities to discuss the concept of death such that individuals are aware of the concept before meeting it head on with the loss of a significant other. It is important to ensure that the individual understands that although everything living has to die, death normally comes at the end of a long life and that loved ones are not suddenly going to be taken away.
If someone famous dies and it is announced in the media. This presents an opportunity to talk about the concept of death and what death means to us. It need not be a real person and, as such, even more distal is the death of someone fictitious in a soap opera or a story for example. However, distal is a relative term. While the death of someone famous who the individual does not really know may be distal, the death of someone from a favourite TV program may be proximal! Natural disasters occur all to frequently and are usually well reported in the media.Such disasters are often accompanied by loss of homes and of work and sadly, of life. Such disasters, especially those in overseas countries, can be a means of introducing the concepts of loss to an individual. It may be that the individual or group of individual can do something to raise money for the disaster fund for example which action, in itself, can be a source to raise awareness of particular issues surrounding this topic in a distal manner. A visit to a cemetery to look at the graves can be an educational experience. For example, the architecture of the head stones, the dates and the histories of those who are there. However, a visit to a cemetary need not be a specially organised thing, if you happen to be passing one and are not in a particular rush to get somewhere and the weather is fine, cemetaries can be a beautiful place to be. Of course, they also provide an opportunity to discuss the purpose of such a place...
Significant others must decide what is distal and what is proximal. In the preparation for loss, it is recommended that distal items are selected for use as tools with which the individual can gradually begin to understand some of the concepts involved. Remember, one single talk on the concept of death is not enough. Although difficult, it must be revisited as appropriate.
Can something be too distal? Perhaps! If the individual has profound difficulties and the chosen item is so far removed from their reality that it has no meaning then it may not be a useful choice. However, it is a beginning on which we can build and with which certain topics can be introduced. A staff member may talk about their loss to an individual. The 'ownership' is the staff member's and not the individual's and, thus, is distal. As long as the staff member feels comfortable about this and can talk about the loss without too great an emotional reaction then it may be a good beginning. This introduces another important point: early preparation should keep emotions distal too. While we may be talking about how others are feeling and introducing concepts of empathy it should not be our intent to create strong emotional reactions too soon although emotions do play an important role and we should not attempt to hide them. The reason for the staff member not having too strong a reaction to talking about the death of a close person is not to protect the individual but rather to assist the staff member in the task. If they feel comfortable with a possible strong reaction then the decision is theirs. However, the distal to proximal principle still applies!
As we move from distal to proximal over a period of time (which will differ from individual to individual) then we must be aware that emotions will play a greater and greater role. However, the purpose of the Distal To Proximal Principle technique is to equip the individual with the knowledge, understanding, communication, experience and the strategies to be better able to cope with the increasing emotions.
A more proximal event concerning death is the death of a pet ...
If someone famous dies and it is announced in the media. This presents an opportunity to talk about the concept of death and what death means to us. It need not be a real person and, as such, even more distal is the death of someone fictitious in a soap opera or a story for example. However, distal is a relative term. While the death of someone famous who the individual does not really know may be distal, the death of someone from a favourite TV program may be proximal! Natural disasters occur all to frequently and are usually well reported in the media.Such disasters are often accompanied by loss of homes and of work and sadly, of life. Such disasters, especially those in overseas countries, can be a means of introducing the concepts of loss to an individual. It may be that the individual or group of individual can do something to raise money for the disaster fund for example which action, in itself, can be a source to raise awareness of particular issues surrounding this topic in a distal manner. A visit to a cemetery to look at the graves can be an educational experience. For example, the architecture of the head stones, the dates and the histories of those who are there. However, a visit to a cemetary need not be a specially organised thing, if you happen to be passing one and are not in a particular rush to get somewhere and the weather is fine, cemetaries can be a beautiful place to be. Of course, they also provide an opportunity to discuss the purpose of such a place...
Significant others must decide what is distal and what is proximal. In the preparation for loss, it is recommended that distal items are selected for use as tools with which the individual can gradually begin to understand some of the concepts involved. Remember, one single talk on the concept of death is not enough. Although difficult, it must be revisited as appropriate.
Can something be too distal? Perhaps! If the individual has profound difficulties and the chosen item is so far removed from their reality that it has no meaning then it may not be a useful choice. However, it is a beginning on which we can build and with which certain topics can be introduced. A staff member may talk about their loss to an individual. The 'ownership' is the staff member's and not the individual's and, thus, is distal. As long as the staff member feels comfortable about this and can talk about the loss without too great an emotional reaction then it may be a good beginning. This introduces another important point: early preparation should keep emotions distal too. While we may be talking about how others are feeling and introducing concepts of empathy it should not be our intent to create strong emotional reactions too soon although emotions do play an important role and we should not attempt to hide them. The reason for the staff member not having too strong a reaction to talking about the death of a close person is not to protect the individual but rather to assist the staff member in the task. If they feel comfortable with a possible strong reaction then the decision is theirs. However, the distal to proximal principle still applies!
As we move from distal to proximal over a period of time (which will differ from individual to individual) then we must be aware that emotions will play a greater and greater role. However, the purpose of the Distal To Proximal Principle technique is to equip the individual with the knowledge, understanding, communication, experience and the strategies to be better able to cope with the increasing emotions.
A more proximal event concerning death is the death of a pet ...
Pets and death
One way in which children typically learn about death early in life is through the death of an animal or a pet. A child is likely to come across a dead animal or insect at some point early in life maybe while out walking in the woods or the family's cat bringing home its prey or someone swatting an insect that has intruded on the family home. While we understand that the creature involved has died and what that entails, the individual may not. Any of these events present an opportunity to discuss the issues surrounding death with an individual without too great an emotional reaction.
Distal pet deaths are easier to talk about than proximal. Thus, if an opportunity arises in which someone's pet has died (perhaps an aunt's or a friend at school or ...) then specific issues can be addressed without too great an emotional involvement.
However, depending on the ability of the individual to communicate, it should be realised that there may be difficult questions to answer. This is a serious issue and responses should never be flippant, dismissive or humourous. While jokes and humour might seem a good way of resolving a difficult issue they are generally not helpful and will not help the individual to cope with their own losses when they arise. It is also important to ensure that the individual understands that although death is a universal feature of all life, it usually comes at the end of a long life and loved family members are not going to be taken away.
Keeping a pet or having a school/establishment pet is a good idea. It need not be a dog or a cat, it could be a few fish in a fish tank for example. When one of the fish dies, the issue should not be hidden but made public such that it is a topic for discussion in situ. In such situations everyone will feel the loss and all can be supportive of each other.
The death of a loved pet can be a very traumatic time and, as such, is not a distal event but one that, for the individual, is proximal. The loss should be treated with respect, care, and empathy.
Distal pet deaths are easier to talk about than proximal. Thus, if an opportunity arises in which someone's pet has died (perhaps an aunt's or a friend at school or ...) then specific issues can be addressed without too great an emotional involvement.
However, depending on the ability of the individual to communicate, it should be realised that there may be difficult questions to answer. This is a serious issue and responses should never be flippant, dismissive or humourous. While jokes and humour might seem a good way of resolving a difficult issue they are generally not helpful and will not help the individual to cope with their own losses when they arise. It is also important to ensure that the individual understands that although death is a universal feature of all life, it usually comes at the end of a long life and loved family members are not going to be taken away.
Keeping a pet or having a school/establishment pet is a good idea. It need not be a dog or a cat, it could be a few fish in a fish tank for example. When one of the fish dies, the issue should not be hidden but made public such that it is a topic for discussion in situ. In such situations everyone will feel the loss and all can be supportive of each other.
The death of a loved pet can be a very traumatic time and, as such, is not a distal event but one that, for the individual, is proximal. The loss should be treated with respect, care, and empathy.
All living things die
If a collection is made of items from the natural world which were once living such as fruits, leaves, shells, branches, vegetables and flowers, etc. these can be displayed on a table top and can form the basis of a discussion about change from one state (living) to another state (dead). The Learners can be encouraged to explore such items using their active senses: to see, feel, hear, taste (such things as fruits) and smell. Staff can ask prompting questions such as, "Is this item alive?", "Was it alive?", "What did it look like when it was alive?", "How do we know that it is no longer alive?". Fresh fruit, dried fruit, and petrified fruit can be compared and contrasted.
Lots of sensory experiences are available to those with the most significant Learning Disabilities:
- Feel a shell. Hold a sea shell to your ear - what can you hear?
- Crush dry leaves in your hands; listen to the sound they make. Compare with live leaves.
- Make a collage from dry leaves.
- Taste a fresh fruit and then taste the dried fruit but only look at and smell the rotten fruit.
- Notice that new fruits are smooth but old fruit is wrinkly;
- Make a rubbing of a piece of bark;
- Feel a potato, peel a potato, cook a potato, eat pieces of cooked potato - at what point is it living and at what point is it dead?
- Make potato prints;
- Make a shell picture;
- Create dried flowers, make pictures and cards using dried flowers and other natural items such as seeds.
The natural world provides lots of opportunities to develop some awareness of life and death with possibilities for all levels of ability.
Lots of sensory experiences are available to those with the most significant Learning Disabilities:
- Feel a shell. Hold a sea shell to your ear - what can you hear?
- Crush dry leaves in your hands; listen to the sound they make. Compare with live leaves.
- Make a collage from dry leaves.
- Taste a fresh fruit and then taste the dried fruit but only look at and smell the rotten fruit.
- Notice that new fruits are smooth but old fruit is wrinkly;
- Make a rubbing of a piece of bark;
- Feel a potato, peel a potato, cook a potato, eat pieces of cooked potato - at what point is it living and at what point is it dead?
- Make potato prints;
- Make a shell picture;
- Create dried flowers, make pictures and cards using dried flowers and other natural items such as seeds.
The natural world provides lots of opportunities to develop some awareness of life and death with possibilities for all levels of ability.
LSBs... Creating Life Story Books
A Life Story Book (LSB) is a record (a form of Memory Book) of a person's (or pet's) life that is accessible to an individual with learning difficulties. It need not, therefore, be written material but might be a PowerPoint presentation that can be controlled by a single switch. Indeed, these days, with the easy availability of electronic material (sounds and videos) from digital cameras and recorders, having an accessible electronic form (perhaps in addition to a had crafted form) of LSB is recommended.
LSBs are a means for an individual with learning difficulties to keep precious memories of a Lost Loved One (LLO) alive in an easily accessible form. They also provide a means of assisting the individual to learn about the life cycle of all living things and therefore should contain images of the LLO as a baby, as a child, during teenage years, getting married, with children, and at significant moments in their life, etc.
Note: It may not be desirable to paste some items into an LSB. However, plastic pockets can easily be sourced which can both display and hold items which may need to be removed from time to time.
An LSB contains materials that are relevant to the individual and therefore will differ considerably from person to person. An LSB may contain:
- Symbols:
There may be a need to include symbols to support the understanding of some individuals. Symbols can be used to make requests
("Will you read this page to me?"), to act as annotations to entries ("Rover as a puppy, July 2000"), to give directions ("turn the
page", "go back a page"), to provide emotional feedback (I am sad, angry, happy, worried, ...), etc. The symbols should be of such
a size to make them easily accessible to the individual for whatever means of access they may have to use (remember this may
change over time). Similar symbols may need to appear on every page to avoid the issues of having to turn back OR a separate
board can be constructed for use in communication with the LSB. It must be kept with the LSB so that it is available at all times
that the LSB is used.
- Written materials:
Although the individual may be illiterate, it does not follow that all written material such be excluded: for example, a hand written
letter from a lost loved one could be included which will be treasured. Even though the individual cannot read it for him/herself, s/he
will know what it says and will always be able to ask others to read it for them (there should even be a little symbol sticker on the
page containing such materials which says please read this to me. An individual may make lots of requests for such a reading.
It should not be denied.
If an individual is illiterate, written information should be kept simple and clear. It should be supported by symbols such that the
individual can access it without the need for additional help.
- Pictures:
Individual with LLO; (life cycle pictures of LLO as a baby, child, adult, etc.). If the photo is a valued item for others too and therefore
cannot be kept (even in a plastic pocket inside the LSB) then a reproduction can be made via a digital scan (for example) which can
be used instead.
- Mementoes and Memory Boxes:
We should not choose what items are important for an individual to keep but allow the individual to choose for him/herself. Not all
mementoes will fit inside a LSB and such items can be kept in a safe and accessible (to the individual) place where they can be
easily retrieved should they be required. Photographs can be taken of such items which can then be added to the LSB. If available,
photographs of the LLO with the memento should also be included
Not all mementos can be pasted into an LSB. However, digital images can be taken of such items and they can be added. The
actual mementos can be kept in a safe and accessible place (Memory Box) which, itself, may be recorded in the LSB to
remind the individual where to go.
- Memories:
Some memories may not be available in a photograph or a memento but nevertheless should still be included. For example, an
individual may list the things that s/he remembers about the LLO (Dad used to like to play dominoes at the pub). In this instance,
any image of the memory (a picture of someone playing dominoes from the internet) can be used annotated with an appropriate
message (Dad loved dominoes at the pub). When the individual is ready and willing then s/he may want to share memories of a
LLO with a significant other. The significant other can help the individual to capture those memories for ever in the LSB.
In some instances, where a person is aware that they are not going to live for much longer, it may be possible for them to prepare
such a book for an individual and share it with them before they die such that the individual has already something to treasure and
on which they can build further.
As a complement to the Memory Book, a Memory Box of momentoes is an excellent idea. The box contains things which
belonged to the LLO or remind the individual of the LLO or are comforting in some way. See Momentoes above.
- Other:
There is no wrong thing that either should be kept out of an LSB unless they simply do not fit. If the individual thinks it important
then it should be included. It is not for us to judge. Videos and recordings can also be represented in an LSB. A still from a video
can act as a reminder that there is a film or video available of a particular event. The annotation can state where the video is located
and how it may be accessed.
It is really important that the individual him or herself be involved in creating the LSB. This activity itself is a part of the healing process and the resulting item will become long time treasured material. As such, it may be used over and over and over. To withstand such continued use,an LSB should never be made cheaply: access for the individual should always be considered and the need for durability built into its creation. It would also be useful to have the option to add or remove pages at any point should that become desirable.
LSBs are a means for an individual with learning difficulties to keep precious memories of a Lost Loved One (LLO) alive in an easily accessible form. They also provide a means of assisting the individual to learn about the life cycle of all living things and therefore should contain images of the LLO as a baby, as a child, during teenage years, getting married, with children, and at significant moments in their life, etc.
Note: It may not be desirable to paste some items into an LSB. However, plastic pockets can easily be sourced which can both display and hold items which may need to be removed from time to time.
An LSB contains materials that are relevant to the individual and therefore will differ considerably from person to person. An LSB may contain:
- Symbols:
There may be a need to include symbols to support the understanding of some individuals. Symbols can be used to make requests
("Will you read this page to me?"), to act as annotations to entries ("Rover as a puppy, July 2000"), to give directions ("turn the
page", "go back a page"), to provide emotional feedback (I am sad, angry, happy, worried, ...), etc. The symbols should be of such
a size to make them easily accessible to the individual for whatever means of access they may have to use (remember this may
change over time). Similar symbols may need to appear on every page to avoid the issues of having to turn back OR a separate
board can be constructed for use in communication with the LSB. It must be kept with the LSB so that it is available at all times
that the LSB is used.
- Written materials:
Although the individual may be illiterate, it does not follow that all written material such be excluded: for example, a hand written
letter from a lost loved one could be included which will be treasured. Even though the individual cannot read it for him/herself, s/he
will know what it says and will always be able to ask others to read it for them (there should even be a little symbol sticker on the
page containing such materials which says please read this to me. An individual may make lots of requests for such a reading.
It should not be denied.
If an individual is illiterate, written information should be kept simple and clear. It should be supported by symbols such that the
individual can access it without the need for additional help.
- Pictures:
Individual with LLO; (life cycle pictures of LLO as a baby, child, adult, etc.). If the photo is a valued item for others too and therefore
cannot be kept (even in a plastic pocket inside the LSB) then a reproduction can be made via a digital scan (for example) which can
be used instead.
- Mementoes and Memory Boxes:
We should not choose what items are important for an individual to keep but allow the individual to choose for him/herself. Not all
mementoes will fit inside a LSB and such items can be kept in a safe and accessible (to the individual) place where they can be
easily retrieved should they be required. Photographs can be taken of such items which can then be added to the LSB. If available,
photographs of the LLO with the memento should also be included
Not all mementos can be pasted into an LSB. However, digital images can be taken of such items and they can be added. The
actual mementos can be kept in a safe and accessible place (Memory Box) which, itself, may be recorded in the LSB to
remind the individual where to go.
- Memories:
Some memories may not be available in a photograph or a memento but nevertheless should still be included. For example, an
individual may list the things that s/he remembers about the LLO (Dad used to like to play dominoes at the pub). In this instance,
any image of the memory (a picture of someone playing dominoes from the internet) can be used annotated with an appropriate
message (Dad loved dominoes at the pub). When the individual is ready and willing then s/he may want to share memories of a
LLO with a significant other. The significant other can help the individual to capture those memories for ever in the LSB.
In some instances, where a person is aware that they are not going to live for much longer, it may be possible for them to prepare
such a book for an individual and share it with them before they die such that the individual has already something to treasure and
on which they can build further.
As a complement to the Memory Book, a Memory Box of momentoes is an excellent idea. The box contains things which
belonged to the LLO or remind the individual of the LLO or are comforting in some way. See Momentoes above.
- Other:
There is no wrong thing that either should be kept out of an LSB unless they simply do not fit. If the individual thinks it important
then it should be included. It is not for us to judge. Videos and recordings can also be represented in an LSB. A still from a video
can act as a reminder that there is a film or video available of a particular event. The annotation can state where the video is located
and how it may be accessed.
It is really important that the individual him or herself be involved in creating the LSB. This activity itself is a part of the healing process and the resulting item will become long time treasured material. As such, it may be used over and over and over. To withstand such continued use,an LSB should never be made cheaply: access for the individual should always be considered and the need for durability built into its creation. It would also be useful to have the option to add or remove pages at any point should that become desirable.
Visiting the Sick

There are times when people die very quickly but there equally times when people have a period of illness prior to their death. It is important not to shield such events from an individual for whatever reason (he will be too upset, she will be difficult to take there, he won't understand, she will not want to come away, ...). The individual should be given opportunities to visit the sick person (if they choose/want to do so) and to be able to communicate with them to the best of their abilities. When we become sick we generally believe that we are going to get well and return to our normal life. It is therefore not appropriate to talk to an individual about the possibility of death. However, in some rare instances, people know in advance that there is a strong probability that they will not survive. In such instances, if the person feels capable, it might be of great help to the individual if the person can talk about it and say what they think might happen to them after they have died. If they have strong beliefs they might explain about going to Heaven and being with Jesus and how happy they will be. However, they should also make it clear that when death comes they will not be able to come back and see them and, that they are not going away because the individual has done something wrong or because they have stopped caring about them. Individuals should not be excluded from visits simply because of their disability not to protect them from 'pain' unless this has been generally applied to all relatives of the same age for some specific reason.
It is also vitally important that visits be organised if the individual's previous experiences of someone going into hospital was that they died and didn't come home. In this instance, the individual might reasonably believe that another member of his/her family is going to die and not come home even if the hospital stay is for some relatively trivial matter. Being prepared for and visits during can allay feelings of loss within any period of absence by any significant other. It is easy for an individual to confuse matters if they are 'protected' from seeing and told half truths (or complete fabrications) or euphemisms are used in place of straight (but considerate) talk.
It is also vitally important that visits be organised if the individual's previous experiences of someone going into hospital was that they died and didn't come home. In this instance, the individual might reasonably believe that another member of his/her family is going to die and not come home even if the hospital stay is for some relatively trivial matter. Being prepared for and visits during can allay feelings of loss within any period of absence by any significant other. It is easy for an individual to confuse matters if they are 'protected' from seeing and told half truths (or complete fabrications) or euphemisms are used in place of straight (but considerate) talk.
Talking of Death. Talking of Loss. Good Practice Guide

Telling the individual experiencing Learning Difficulties about a death can be a difficult thing to do. However, it is better that it is done than the individual hears about it from someone else who will not inform them with kindness. It should not be assumed that not telling them is better because the individual is likely to notice that a loved person is missing and we cannot know how they will 'understand' this.
- ensure that all significant others and ALL other staff (including those on separate shifts) are aware of the situation and treat the individual concerned with care and empathy.
- If there is no close member of the family who is coming to tell the individual about the loss there should be a nominated member of staff appointed to do so. This should be someone with whom the individual has a close and caring relationship rather than some person whom s/he has never met previously or who has just a casual working relationship.
- There should be no delay in information about the loss other than the time it takes to prepare your thoughts and consider how to tell the truth in a kind and considerate manner. Never withhold the information from an individual simply because you feel 'they will not understand' or 'it may upset them too much' or because you find it too difficult a subject. Individuals have a right to know, have a right to grieve... need to know, need to grieve...
- Vocabulary used should always match the individual's level of comprehension. It may be augmented by the use of symbols, drawings, pictures and or photographs.
- Communicate with individuals directly, irrespective of whoever they may have with them. Let the individual know that you understand the experience is very sad and painful for them.
- Always begin by preparing the individual for the bad news. 'You know that Rover has not been eating and walking very well lately... well I have some very sad news ...'
- Never pretend that a dead person is still alive.
- If there is likely to be strong reaction ensure that support is on hand and that the individual's reaction will not put them into physical danger.
- Reactions may not occur immediately: ensure that for the first few days following the news that extra care is provided to ensure the ability to cope with any delayed response. Indeed, reactions may take weeks if not longer to appear. Be prepared to deal with them as they arise with great empathy and consideration. Do not say, 'Oh that was ages ago, it is time to move on'!
- Do not use indirect language; 'we have lost Grandpa' is confusing, 'Grandpa has died' is much better. Provide information relating to the why of the loss.
- Do not try to use humour to 'deflect' the situation. Do not try to 'jolly' the person along following the loss. All people need time to grieve.
- Under no circumstances should individuals be teased about any loss either directly or indirectly. Such behaviour amounts to abuse / mental cruelty.
- Encourage questioning. Always try to answer questions honestly.
- Ensure that the individual understands that the death was not as a result of something s/he had previously done.
- If there was suffering, do not dwell on this fact but do not neglect it either. It is important that the individual understands that death is not the same as suffering. For example, you might say something like, 'You know that Rover had a bad stomach and could not walk very well. It was not nice for him. We are all sad and we will all miss him but it is good that he has not got to be in pain any more'. Thus, death becomes an end of suffering and not a cause of suffering.
- Do not hide your own grief. Let the individual see that it OK and natural to feel sad, to cry, to ask questions about the loss ...
- Share your own feelings about the loss. Tell the individual how you are feeling. If the individual is capable of understanding, tell them how grief can affect the body in some people so that are prepared for any changes if they occur. Tell them also what to do if such things should happen to them. Let them know that it is natural and OK to react in these ways.
- Ask the individual to tell you how they are feeling. Let them know that it is OK to feel sad. Be aware that behaviour and body language may show that a person. Monitor the person for a period of days to see if there is a change in behaviour that might show that the loss has affected him/her more than s/he is saying. Are they quieter than normal? Do they want to spend more time alone in their room? Are they feeling ill? Are there untypical reactions to everyday events?
- Prepare the individual for the 'strangers' who will be coming to their home in connection with the funeral. For example, the funeral director, church minister, or even the police. Ensure that such people are also prepared for the individual and that they are told to involve them in all that is happening (they may need guidance on 'how' best to do this) and not to talk 'over' them to the others who are present.
- Allow the individual to choose if they wish to attend the funeral. Do not force them to go (or to stay away) if they do not wish to. Prepare them for what they will see and experience. Following the distal to proximal principle, try to ensure that the individual has had prior experiences of funerals, cremations and burials such that they will know what to expect. Having a small ceremony for the death of a pet, for example, is a good idea. Attending the funerals of distant relatives whom the individual did not know is also a good idea. It provides experiences and an opportunity to discuss the issue of death.
- Ensure that the individual understands that there will always be someone to whom they can turn for comfort and communication of their feelings. Ensure that they know where to go and what to do. Ensure that all Significant Others are aware of the situation and are prepared for the situation.
- If there is denial then do not keep trying to convince the individual of the loss. The individual will accept it in time and at that point there will be a reaction. Be prepared. Ensure that no Significant Other supports the individual's denial but informs them in a kind and considerate manner that what they have been told is true and they are prepared to discuss it with them if they want and when they want.
- Always ask the individual if s/he would like you to read the letters, cards, etc of sympathy from others that arrived. If the individual does not want you to do this then, at least, ensure that s/he has access to this material and knows that they can 'ask' you or another significant other to assist them with it at any time.
- Ensure that the individual is involved and represented in arrangements for the funeral. For example, they may wish to buy flowers once they are aware this is a common practice. Flowers should never be purchased on 'their behalf' without their involvement. The individual should be involved as much as is practical in selecting the flowers to be purchased and in all other aspects of the funeral process.
- Individuals should be able to choose how they grieve. If they wish to be alone then they should have this opportunity. If they wish to look at photographs with a member of staff then this should happen. If they wish to continue a particular response to a loss for a long period then, that too, should be respected. Only if a reaction poses a significant threat to the individual's physical well being should it be addressed. If it is felt that a continuing reaction poses a threat to psychological well being then the assistance of a qualified health professional should be sought to verify this belief and to decide whether a particular course of action is necessary.
- Staff should assist individuals to keep in touch with 'lost' friends whenever possible by phone, by letter, by e-mail, by Skype, social networking or any other means. There is no reason these days why a particular friend cannot maintain regular contact even if they move to another country.
- Individuals are likely to feel a loss even more at anniversaries and special times such as Christmas when families typically get together. Staff should be especially sensitive at these times.
- Individuals should always be allowed to keep mementoes of people they have lost and to talk about these and the deceased whenever they choose to do so. The use of Life Story Books (See below) is recommended.
- Individuals should be involved in the decisions on what happens to the property of the deceased relation.
- Individuals should always be consulted on what they would like to happen following the death of a member or a primary carer. Their wishes should be respected and, whenever possible, acted upon.
- Staff should always respect the anniversaries of a death of a significant other.
- Talk about the topics of loss (see the following section)
- ensure that all significant others and ALL other staff (including those on separate shifts) are aware of the situation and treat the individual concerned with care and empathy.
- If there is no close member of the family who is coming to tell the individual about the loss there should be a nominated member of staff appointed to do so. This should be someone with whom the individual has a close and caring relationship rather than some person whom s/he has never met previously or who has just a casual working relationship.
- There should be no delay in information about the loss other than the time it takes to prepare your thoughts and consider how to tell the truth in a kind and considerate manner. Never withhold the information from an individual simply because you feel 'they will not understand' or 'it may upset them too much' or because you find it too difficult a subject. Individuals have a right to know, have a right to grieve... need to know, need to grieve...
- Vocabulary used should always match the individual's level of comprehension. It may be augmented by the use of symbols, drawings, pictures and or photographs.
- Communicate with individuals directly, irrespective of whoever they may have with them. Let the individual know that you understand the experience is very sad and painful for them.
- Always begin by preparing the individual for the bad news. 'You know that Rover has not been eating and walking very well lately... well I have some very sad news ...'
- Never pretend that a dead person is still alive.
- If there is likely to be strong reaction ensure that support is on hand and that the individual's reaction will not put them into physical danger.
- Reactions may not occur immediately: ensure that for the first few days following the news that extra care is provided to ensure the ability to cope with any delayed response. Indeed, reactions may take weeks if not longer to appear. Be prepared to deal with them as they arise with great empathy and consideration. Do not say, 'Oh that was ages ago, it is time to move on'!
- Do not use indirect language; 'we have lost Grandpa' is confusing, 'Grandpa has died' is much better. Provide information relating to the why of the loss.
- Do not try to use humour to 'deflect' the situation. Do not try to 'jolly' the person along following the loss. All people need time to grieve.
- Under no circumstances should individuals be teased about any loss either directly or indirectly. Such behaviour amounts to abuse / mental cruelty.
- Encourage questioning. Always try to answer questions honestly.
- Ensure that the individual understands that the death was not as a result of something s/he had previously done.
- If there was suffering, do not dwell on this fact but do not neglect it either. It is important that the individual understands that death is not the same as suffering. For example, you might say something like, 'You know that Rover had a bad stomach and could not walk very well. It was not nice for him. We are all sad and we will all miss him but it is good that he has not got to be in pain any more'. Thus, death becomes an end of suffering and not a cause of suffering.
- Do not hide your own grief. Let the individual see that it OK and natural to feel sad, to cry, to ask questions about the loss ...
- Share your own feelings about the loss. Tell the individual how you are feeling. If the individual is capable of understanding, tell them how grief can affect the body in some people so that are prepared for any changes if they occur. Tell them also what to do if such things should happen to them. Let them know that it is natural and OK to react in these ways.
- Ask the individual to tell you how they are feeling. Let them know that it is OK to feel sad. Be aware that behaviour and body language may show that a person. Monitor the person for a period of days to see if there is a change in behaviour that might show that the loss has affected him/her more than s/he is saying. Are they quieter than normal? Do they want to spend more time alone in their room? Are they feeling ill? Are there untypical reactions to everyday events?
- Prepare the individual for the 'strangers' who will be coming to their home in connection with the funeral. For example, the funeral director, church minister, or even the police. Ensure that such people are also prepared for the individual and that they are told to involve them in all that is happening (they may need guidance on 'how' best to do this) and not to talk 'over' them to the others who are present.
- Allow the individual to choose if they wish to attend the funeral. Do not force them to go (or to stay away) if they do not wish to. Prepare them for what they will see and experience. Following the distal to proximal principle, try to ensure that the individual has had prior experiences of funerals, cremations and burials such that they will know what to expect. Having a small ceremony for the death of a pet, for example, is a good idea. Attending the funerals of distant relatives whom the individual did not know is also a good idea. It provides experiences and an opportunity to discuss the issue of death.
- Ensure that the individual understands that there will always be someone to whom they can turn for comfort and communication of their feelings. Ensure that they know where to go and what to do. Ensure that all Significant Others are aware of the situation and are prepared for the situation.
- If there is denial then do not keep trying to convince the individual of the loss. The individual will accept it in time and at that point there will be a reaction. Be prepared. Ensure that no Significant Other supports the individual's denial but informs them in a kind and considerate manner that what they have been told is true and they are prepared to discuss it with them if they want and when they want.
- Always ask the individual if s/he would like you to read the letters, cards, etc of sympathy from others that arrived. If the individual does not want you to do this then, at least, ensure that s/he has access to this material and knows that they can 'ask' you or another significant other to assist them with it at any time.
- Ensure that the individual is involved and represented in arrangements for the funeral. For example, they may wish to buy flowers once they are aware this is a common practice. Flowers should never be purchased on 'their behalf' without their involvement. The individual should be involved as much as is practical in selecting the flowers to be purchased and in all other aspects of the funeral process.
- Individuals should be able to choose how they grieve. If they wish to be alone then they should have this opportunity. If they wish to look at photographs with a member of staff then this should happen. If they wish to continue a particular response to a loss for a long period then, that too, should be respected. Only if a reaction poses a significant threat to the individual's physical well being should it be addressed. If it is felt that a continuing reaction poses a threat to psychological well being then the assistance of a qualified health professional should be sought to verify this belief and to decide whether a particular course of action is necessary.
- Staff should assist individuals to keep in touch with 'lost' friends whenever possible by phone, by letter, by e-mail, by Skype, social networking or any other means. There is no reason these days why a particular friend cannot maintain regular contact even if they move to another country.
- Individuals are likely to feel a loss even more at anniversaries and special times such as Christmas when families typically get together. Staff should be especially sensitive at these times.
- Individuals should always be allowed to keep mementoes of people they have lost and to talk about these and the deceased whenever they choose to do so. The use of Life Story Books (See below) is recommended.
- Individuals should be involved in the decisions on what happens to the property of the deceased relation.
- Individuals should always be consulted on what they would like to happen following the death of a member or a primary carer. Their wishes should be respected and, whenever possible, acted upon.
- Staff should always respect the anniversaries of a death of a significant other.
- Talk about the topics of loss (see the following section)
Topics of loss
Many individuals may have limited or confused notions about loss. It is natural for families, carers and professionals alike to want to shield them from topics that they believe might be upsetting or worrying. However, this can lead to a situation in which the individual is ill-prepared for events that happen in everyone's life and make the situation, when it does occur, much more problematic and traumatic.
It is good practice to introduce topics of loss before a loss occurs. It needs to be done considerately such that the individual is not left worrying about the loss of friends or relations or concerned about what may happen following such a event. It is important that there is one or more people to whom the individual can return to ask any questions at any point. It is good practice to follow the distal to proximal principle in this matter such that the individual is not grieving at the time such issues are discuss and explained. This only adds an additional layer of problems to what is a difficult area.
The following is a non-exhaustive list of topics that ought to be covered:
Definition: What is death?
Causality. What causes death? What is the cycle of life? Why do things die?
Timing: When do people die?
Irreversibility: Can you come back to life once you are dead?
Non-functionality: What ceases to function in a person once death has occurred? Can they still see, feel, hear, smell,
think, talk ...?
Universality: Do all things die? Do all living things die?
Familial: Will my <person> (mother, father, brother, sister) die?
Personal: Will I die? Am I safe? Will the same thing happen to me?
Sequence: What happens after death? What happens to those that are left behind?
Consequence: What will happen to me after ,person. dies? What changes will be happening in my life? Will I be able
to continue as I did before?
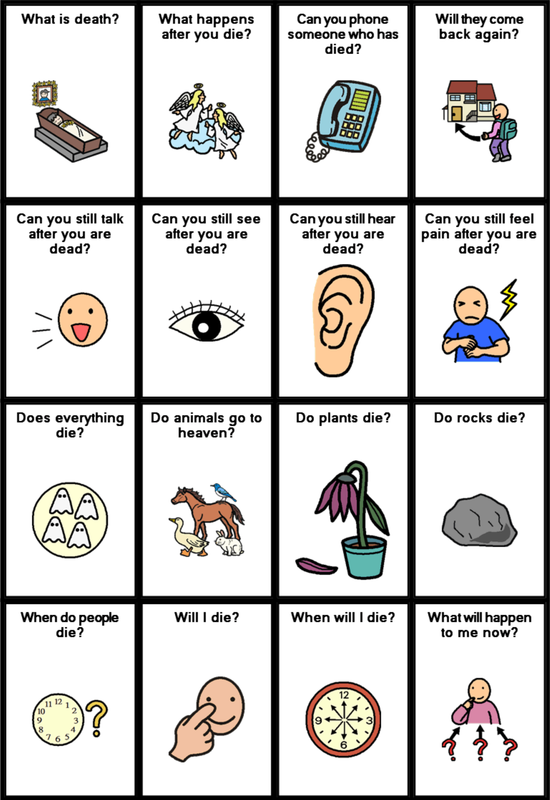
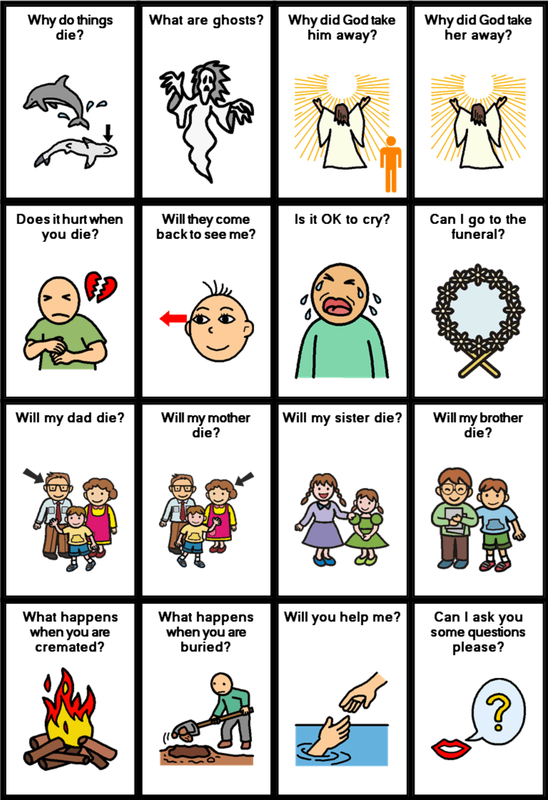
An individual will want to ask questions about such topics and therefore s/he must have a means of doing so with the current communication system or with additional communications boards or pages. Some ideas for such pages are provided below. One size does not fit all needs and therefore the boards are provided as a method of stimulating your thinking on this matter rather than as some form of definitive solution. However,if you think that the communication boards illustrated may be helpful, they are available from Talksense free of charge on request. Please use form at bottom of this page to request boards.
It is good practice to introduce topics of loss before a loss occurs. It needs to be done considerately such that the individual is not left worrying about the loss of friends or relations or concerned about what may happen following such a event. It is important that there is one or more people to whom the individual can return to ask any questions at any point. It is good practice to follow the distal to proximal principle in this matter such that the individual is not grieving at the time such issues are discuss and explained. This only adds an additional layer of problems to what is a difficult area.
The following is a non-exhaustive list of topics that ought to be covered:
Definition: What is death?
Causality. What causes death? What is the cycle of life? Why do things die?
Timing: When do people die?
Irreversibility: Can you come back to life once you are dead?
Non-functionality: What ceases to function in a person once death has occurred? Can they still see, feel, hear, smell,
think, talk ...?
Universality: Do all things die? Do all living things die?
Familial: Will my <person> (mother, father, brother, sister) die?
Personal: Will I die? Am I safe? Will the same thing happen to me?
Sequence: What happens after death? What happens to those that are left behind?
Consequence: What will happen to me after ,person. dies? What changes will be happening in my life? Will I be able
to continue as I did before?
An individual will want to ask questions about such topics and therefore s/he must have a means of doing so with the current communication system or with additional communications boards or pages. Some ideas for such pages are provided below. One size does not fit all needs and therefore the boards are provided as a method of stimulating your thinking on this matter rather than as some form of definitive solution. However,if you think that the communication boards illustrated may be helpful, they are available from Talksense free of charge on request. Please use form at bottom of this page to request boards.
What About Religion?
For many, religion is a great comfort at the time of a loss. The belief that life does not end with death but continues in another form can help us to cope. However, explaining one difficult to comprehend topic by using another one can be a recipe for disaster for the individual experiencing learning difficulties. If the individual understands the concept of God/Allah (or any other deity specific to a particular faith) then it may be a good means to help him/her come to terms with a difficult loss. However, it should not be assumed that, just because individuals have attended church regularly with their family, they understand such concepts. Furthermore, the use of such language as 'He has gone to see God' or 'She is with God now' or 'He has gone to Heaven to be with Jesus' are all phrases with are open to the wrong interpretation by the individual. Ensure that the individual understands that 'going to be with God' or being 'in Heaven' means that the person will not be coming back and they cannot be contacted by phone or by letter or e-mail. Also ensure that the individual understands that the person did not 'go to be be with God' because:
- s/he did not love them;
- s/he did not want to see them any more;
- s/he did something bad that caused God to take the person away;
- the individual did something bad to cause God to take the person away;
- God did not like the person;
- s/he chose God over him/her;
- s/he is punishing him/her.
or any other possible misinterpretation. Also, ensure that the individual understands that God does not 'call' people to his kingdom randomly and, therefore he will not be taking away other loved people for quite some time. The use of religion to explain death or provide comfort is fraught with problems unless it it is thought through, explained carefully and, the individual's thoughts and feeling are explored to avoid confusion and misunderstanding.
Whatever belief system that you have, the beliefs of the individual must be held paramount. If the individual asks what happens after death, it may be best to explain what different people/cultures believe. In doing so, one belief should not be stressed above another, even if you are a really committed Christian, for example. You should explain each of the possibilities (there are, at least, six) in turn and then allow the individual to decide which s/he believes is correct. If you are asked what you believe, then you should state your beliefs and explain why you believe them. Do not attempt to change an individual's mind even if you think they are wrong. Be there for them and tell them that you are prepared to discuss the subject further, at any point, as they wish.
One change should not lead to another
The loss of one person (or other) can lead to other losses. For example, when a parent dies, a son or daughter may no longer be considered able to continue living in the family home and may be moved into residential care. Thus, the individual has not only lost a parent but also lost a home as well as a familiar routines, foods, practices, smells, friends ... Compound losses are the most difficult with which to deal. It is hardly surprising, therefore, when an individual reacts badly to such events, indeed, it would be more surprising if they didn't! Also, at such times, the individual is likely to be performing at a level that is below that which is typical, therefore, performing assessments on moving into residential placements because of the death or incapacity of a parent / carer is not an example of good practice.
Whenever possible, everything should be done to maintain all other things within a person's life such that one loss does not lead to another.
Whenever possible, everything should be done to maintain all other things within a person's life such that one loss does not lead to another.
What happens to me?

It is quite natural for an individual to be concerned about what will happen to them when a parent or carer dies? If they cannot express such feelings and concerns it must be terribly frightening and worrying. Where possible, and as detailed above, one change should not lead to a cascade of changes with which the individual has suddenly to cope. However, if the person who has died was a sole primary carer and there is no other family member to take their place then there will be a need to provide alternative care. It may be that social services can support the individual to continue to live in the family home; it may also be that the individual will need to move into residential care. While families may believe that they will outlive the individual and therefore they will always be there to care, this is not necessarily the case. Many people experiencing learning difficulties will lead a long life and will outlive their parents. Also parents may become infirm and unable to cope as they grow older. Hoping for the best but planning and preparing for the worse is good practice. It provides some peace of mind for all concerned and also better prepares the individual for change should anything happen. Ensuring that an individual is gradually prepared for such changes (if they need to happen) over a period of time is good practice. The individual's concerns can be addressed as they arise and everyone involved can be assured by the process.
As soon as possible following a loss, someone that the individual knows and trusts (family member or carer) should spend some quality time explaining the possible options and answering any questions and concerns that the individual may have. Keep explanations simple and always use straightforward language. If there are varying options, explain each option and ask which the individual would prefer. The choice should be the individual's. Where possible, allow the individual to experience each option in turn such that s/he is better able to state which is preferred. Try not to put words or ideas into the individual's mind, "I think it would be best for you if ...". Rather, ask the individual what s/he thinks would be best and what s/he wants to do. Ensure that the individual understands that:
- all contacts with what has gone before will not be lost;
- friends and relations will still be there for him/her;
- favourite items will not be taken away.
- s/he will always have someone to whom s/he can turn for help, advice and comfort.
As soon as possible following a loss, someone that the individual knows and trusts (family member or carer) should spend some quality time explaining the possible options and answering any questions and concerns that the individual may have. Keep explanations simple and always use straightforward language. If there are varying options, explain each option and ask which the individual would prefer. The choice should be the individual's. Where possible, allow the individual to experience each option in turn such that s/he is better able to state which is preferred. Try not to put words or ideas into the individual's mind, "I think it would be best for you if ...". Rather, ask the individual what s/he thinks would be best and what s/he wants to do. Ensure that the individual understands that:
- all contacts with what has gone before will not be lost;
- friends and relations will still be there for him/her;
- favourite items will not be taken away.
- s/he will always have someone to whom s/he can turn for help, advice and comfort.
Communicating Loss: Creating Communication Boards for Loss
'Life' and 'death', although common to us all are not Core words. That is, they are not contained in the list of those words that we use the most frequently. There is a tendency to believe that, following a death, a page (or pages) or vocabulary should be prepared with which the individual can discuss his or her feeling and aspects of the situation. However, such vocabulary and such pages will, by definition, be new and therefore the symbols and language involved will be unfamiliar and require tuition. Furthermore, typically, the emotional vocabulary of such pages is likely to be one of sadness and sorrow such that, if asked how s/he is feeling, the individual can only respond in a given and predicted manner.
"How are you John?" ... "I am really sad" (frightened, worried, angry, ...)
All of this is poor practice. The provision of vocabulary in response to specific situations as they arise is a poor way to develop communication skills. A much better approach is to provide a vocabulary of core words that are sufficient to discuss any topic (including those of natural disasters which occur all too frequently in the news but are a means of using the distal to proximal principle to develop concepts of and communicative reactions to loss). Of course, it may be necessary to extend the core from time to time but to provide pages of vocabulary that may only be used once every few months is NOT an example of good practice.
While we may want to group symbols into categories such that a particular item is easier to locate, the more categories there are the greater the size of the system. The greater the size of the system the more difficult it is to learn and to navigate. The more frequently we use a word or phrase the easier it is to remember and to locate. We tend to remember that which we use regularly and forget those things which we don't. For example, people will remember their own phone number or those of friends and relations they call frequently but forget the numbers of people to whom they talk only on occasions (which is why we have telephone books and such). Thus, if we can talk about topics using a smaller but frequently used vocabulary set it will be easier to learn and quicker to use. That does not mean we cannot acquire new words and ask that they be added. So do we need to add words such as 'burial', 'crematorium', 'funeral', 'hearse', 'undertaker' etc to a communication system? Permanent addition of such vocabulary will only serve to expand the system and make it more difficult to use. While some dynamic systems can cope with extra pages which will not slow down or otherwise impede the use of the main core vocabulary, it is likely that, unless used frequently, such pages will not be maintained and will be forgotten as existing by the User. Of course, they can be reminded as and when necessary and, as long as the page is not too complex and the symbols are clear, it may be that the individual can cope.
Can we show the individual how to talk about this topic without having all the 'fringe' vocabulary available? For example what other words could we use in place of:
burial place, put, in, under, ground, earth, dead
crematorium place, building, where, take, fire, burn, body, dead
deceased person, who, died, dead, not living
funeral church, service, dead, friends, meet, say, goodbye
hearse big, long, black, car, for, dead
undertaker person who job dead
'Dead' is a useful word. It can be used as an intensifier (it was dead good), an adjective (It is dead), an adverb (he stopped dead in his tracks), as well as a noun (the dead are lying all around). As such, it should be included in most communication systems.
One idea from the Talksense book of ideas for communication systems (not something that is available for general release!) is the 'Topic Button'. Talksense is unaware of any present system that has such a feature but will report any that it finds in the future. The topic button does not go to a specific page but moves to the page which has the fringe vocabulary for the current topic of conversation. If the topic is a natural disaster the button moves to the disaster page, if it is a death in the family then the button moves to the symbols for loss page. How does it know where to go? It doesn't! It has to be told the topic. In other words, it has to be set. One way of teaching it (there are others but one idea will serve the purpose here), the first time it is used, it allows the User to reach the page by normal routes. Once the page is reached, the topic button remembers the pages location and then, when used again, goes directly there using a system of one selection and return to the page from which it came. Thus, if the topic where 'loss' and the 'loss' page where attached to the topic button, it would go there repeatedly for a single item of vocabulary each time it was activated. How would it know when the topic changed? It would stop going to the loss page after a system shutdown or after a set period of time of non use or on a direct command to 'clear topic' (which could be programmed on a functions page or on each fringe page). Using a topic button, an individual could use everyday vocabulary to talk about a specific item and then, as needed, quickly and simply call up and use related fringe words.
As such things as topic buttons do not presently exist it is possible to create a topic board. A topic board presents particular fringe vocabulary from which a person might select but which is not a permanent part of the individual's communication system although it can be requested at any time. A topic board for loss would be used in conjunction with the main communication system by both parties to teach concepts in the area and to communicate.
"How are you John?" ... "I am really sad" (frightened, worried, angry, ...)
All of this is poor practice. The provision of vocabulary in response to specific situations as they arise is a poor way to develop communication skills. A much better approach is to provide a vocabulary of core words that are sufficient to discuss any topic (including those of natural disasters which occur all too frequently in the news but are a means of using the distal to proximal principle to develop concepts of and communicative reactions to loss). Of course, it may be necessary to extend the core from time to time but to provide pages of vocabulary that may only be used once every few months is NOT an example of good practice.
While we may want to group symbols into categories such that a particular item is easier to locate, the more categories there are the greater the size of the system. The greater the size of the system the more difficult it is to learn and to navigate. The more frequently we use a word or phrase the easier it is to remember and to locate. We tend to remember that which we use regularly and forget those things which we don't. For example, people will remember their own phone number or those of friends and relations they call frequently but forget the numbers of people to whom they talk only on occasions (which is why we have telephone books and such). Thus, if we can talk about topics using a smaller but frequently used vocabulary set it will be easier to learn and quicker to use. That does not mean we cannot acquire new words and ask that they be added. So do we need to add words such as 'burial', 'crematorium', 'funeral', 'hearse', 'undertaker' etc to a communication system? Permanent addition of such vocabulary will only serve to expand the system and make it more difficult to use. While some dynamic systems can cope with extra pages which will not slow down or otherwise impede the use of the main core vocabulary, it is likely that, unless used frequently, such pages will not be maintained and will be forgotten as existing by the User. Of course, they can be reminded as and when necessary and, as long as the page is not too complex and the symbols are clear, it may be that the individual can cope.
Can we show the individual how to talk about this topic without having all the 'fringe' vocabulary available? For example what other words could we use in place of:
burial place, put, in, under, ground, earth, dead
crematorium place, building, where, take, fire, burn, body, dead
deceased person, who, died, dead, not living
funeral church, service, dead, friends, meet, say, goodbye
hearse big, long, black, car, for, dead
undertaker person who job dead
'Dead' is a useful word. It can be used as an intensifier (it was dead good), an adjective (It is dead), an adverb (he stopped dead in his tracks), as well as a noun (the dead are lying all around). As such, it should be included in most communication systems.
One idea from the Talksense book of ideas for communication systems (not something that is available for general release!) is the 'Topic Button'. Talksense is unaware of any present system that has such a feature but will report any that it finds in the future. The topic button does not go to a specific page but moves to the page which has the fringe vocabulary for the current topic of conversation. If the topic is a natural disaster the button moves to the disaster page, if it is a death in the family then the button moves to the symbols for loss page. How does it know where to go? It doesn't! It has to be told the topic. In other words, it has to be set. One way of teaching it (there are others but one idea will serve the purpose here), the first time it is used, it allows the User to reach the page by normal routes. Once the page is reached, the topic button remembers the pages location and then, when used again, goes directly there using a system of one selection and return to the page from which it came. Thus, if the topic where 'loss' and the 'loss' page where attached to the topic button, it would go there repeatedly for a single item of vocabulary each time it was activated. How would it know when the topic changed? It would stop going to the loss page after a system shutdown or after a set period of time of non use or on a direct command to 'clear topic' (which could be programmed on a functions page or on each fringe page). Using a topic button, an individual could use everyday vocabulary to talk about a specific item and then, as needed, quickly and simply call up and use related fringe words.
As such things as topic buttons do not presently exist it is possible to create a topic board. A topic board presents particular fringe vocabulary from which a person might select but which is not a permanent part of the individual's communication system although it can be requested at any time. A topic board for loss would be used in conjunction with the main communication system by both parties to teach concepts in the area and to communicate.
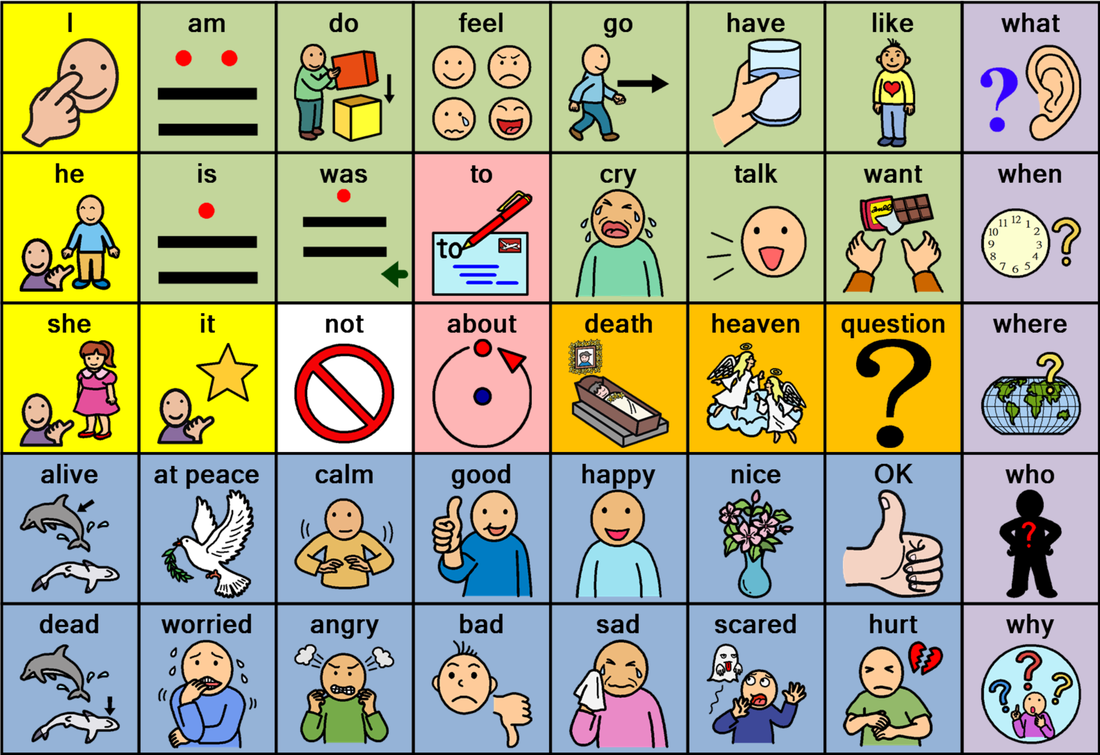
The above is one example of a communication board for loss. It is NOT a recommended system for all-comers! It is neither good nor bad. There will be some who think that there are obvious words missing and some who think that it is too complex. The board is not supposed to be THE solution but, rather, an idea to promote thought about how such a system could be set up to assist an individual in your care. It may be that such vocabulary is already contained in the individual's existing communication system. However, such vocabulary may not all be together on one page and, thus, the current system might make it difficult for the individual to talk about things that are concerning him/her.
Questions:
- Is the board too simple or too complex?
- Does it contain the necessary vocabulary? What words are missing?
- Is it set out in such a manner that makes it easy for the individual to access?
- What symbols should be used?
- Where is the board to be kept? (Will it be added to the existing communication system, for example?);
- Will the individual understand the vocabulary? Can we teach the individual about the vocabulary?
- Will we need additional boards for specific events such as a funeral?
- Are all significant others prepared to work with the individual with the board? What training have they had?
- Will it be used? If not, why do all the work? What is the alternative?
You will notice that the majority of the words on the board depicted are commonly used and, as such, should be contained in any communication system. There are a few however which would be used rarely: for example, the combination 'at peace' may be OK for construction such phrases as 'he is at peace' but would not be used in general conversation. However, the words 'at' and 'peace' as separate units would be used more generally and could be brought together when needed to form the example phrase. While we may believe that we talk about 'heaven' a lot, I would doubt that even committed Christians use the word daily in conversation: it may not even be used in conversation in church on a Sunday although it is likely to be sung in hymns and mentioned during prayers. Likewise with 'death'. Could we cope with just the word 'dead' which could be used flexibly? Does the individual actually need all the varying forms (dead, death, dying, die, dies, deathly, ...) in order to get a message across?
The above board is about a specific type of loss; it may be better to create a generic board for all loss that can be used in distal times of disaster as well as for those occasions that are proximal. The more frequently a system is used, the more useful to the individual it is likely to be when proximal events occur.
Note: If it is considered appropriate, the above board is available free of charge, on request, as a word document, for non-commercial use.
Questions:
- Is the board too simple or too complex?
- Does it contain the necessary vocabulary? What words are missing?
- Is it set out in such a manner that makes it easy for the individual to access?
- What symbols should be used?
- Where is the board to be kept? (Will it be added to the existing communication system, for example?);
- Will the individual understand the vocabulary? Can we teach the individual about the vocabulary?
- Will we need additional boards for specific events such as a funeral?
- Are all significant others prepared to work with the individual with the board? What training have they had?
- Will it be used? If not, why do all the work? What is the alternative?
You will notice that the majority of the words on the board depicted are commonly used and, as such, should be contained in any communication system. There are a few however which would be used rarely: for example, the combination 'at peace' may be OK for construction such phrases as 'he is at peace' but would not be used in general conversation. However, the words 'at' and 'peace' as separate units would be used more generally and could be brought together when needed to form the example phrase. While we may believe that we talk about 'heaven' a lot, I would doubt that even committed Christians use the word daily in conversation: it may not even be used in conversation in church on a Sunday although it is likely to be sung in hymns and mentioned during prayers. Likewise with 'death'. Could we cope with just the word 'dead' which could be used flexibly? Does the individual actually need all the varying forms (dead, death, dying, die, dies, deathly, ...) in order to get a message across?
The above board is about a specific type of loss; it may be better to create a generic board for all loss that can be used in distal times of disaster as well as for those occasions that are proximal. The more frequently a system is used, the more useful to the individual it is likely to be when proximal events occur.
Note: If it is considered appropriate, the above board is available free of charge, on request, as a word document, for non-commercial use.

distraught sad unhappy not sure better happy fantastic

furious angry annoyed worried concerned afraid terrified
The emoticons above, designed to allow someone to communicate just how they are feeling are also available, free of charge, as a Word document (other formats are available too) on request. They are also available as separate switch caps for use either on jelly bean type of switches or on BIGreds or BIGmacks. If you would like any of these things, please state the size and please use the form at the bottom of the page.
Symbols for Loss

This website has a page of symbols that can be used for aspects of loss. The symbols are free for non-commercial usage. Click on the symbol to the left to move to the loss symbols page.
If the symbol(s) that are sought cannot be found on that page, please contact us and we will add into the set for the benefit of all.
If the symbol(s) that are sought cannot be found on that page, please contact us and we will add into the set for the benefit of all.
Cuddles are not abuse
It seems sometimes that political correctness is taken too far and that, in a laudable effort to protect individuals from abuse (and staff from accusations of abuse) we also 'shield' them from any close physical contact. Using hand under hand techniques to facilitate communication, for example, is not necessarily abuse providing that the facilitator is guiding the hand to create a message that is not of the individual's choosing or intent and has informed the individual of the nature of the interaction and has concent. Likewise, giving a cuddle to a person who is in a state of grief is not abuse providing that we are not taking an adult out of a wheelchair and sitting him/her in our lap in order to do so. Yes, there is a fine line between physical and emotional support and abuse but it is not one of which staff should be fearful providing they have been given adequate training into what might be considered/interpreted as abuse.
Good Grief: No Right Way
There is no one right way to grieve. Some cultures grieve in the open and others tend to grieve in private. Each must find his or her own path. Simply because we belong to one culture, it should not be assumed that an individual has to grieve in this way. "Pull yourself together", "Got to be strong and carry on", "You are an adult now and adults don't behave like that" and other such similar comments from others are generally not helpful. Individuals have a right to grieve. Indeed, it is important that they do but in their own way and in their own time. They should not be 'forced' to grieve neither prevented form grieving.
It does not follow because there is no one right way to grieve that, conversely, there is no wrong way. If someone choose to take their grief out on an entire population by committing genocide for example, the overwhelming majority of us would consider that to be wrong. If an individual chooses a pathway which is potentially harmful then, unless you are an expert in such matters, it is best to seek advice from a professional with lots of experience on the matter. There are many sources of useful information on the web and support groups that may be able to provide advice.
For some, actions speak louder than words, and doing something to honour the Lost Loved One (LLO) is a means of helping the healing process. For example, making a donation to a particular charity in the LLO's name, or sponsoring an item or event in their name, building an Life Story Book; it really does not matter what it is; as long as the individual elects to do it, it should help with grief management.
It does not follow because there is no one right way to grieve that, conversely, there is no wrong way. If someone choose to take their grief out on an entire population by committing genocide for example, the overwhelming majority of us would consider that to be wrong. If an individual chooses a pathway which is potentially harmful then, unless you are an expert in such matters, it is best to seek advice from a professional with lots of experience on the matter. There are many sources of useful information on the web and support groups that may be able to provide advice.
For some, actions speak louder than words, and doing something to honour the Lost Loved One (LLO) is a means of helping the healing process. For example, making a donation to a particular charity in the LLO's name, or sponsoring an item or event in their name, building an Life Story Book; it really does not matter what it is; as long as the individual elects to do it, it should help with grief management.
Life must go on
What do we need to do in the days, weeks, months and years following a loss to support an individual experiencing a learning difficulty?
- Does the individual know to whom s/he can go to ask questions or just to talk?
- Does the individual have access to a place where s/he can be on his/her own?
- Does the individual have access to a Life Story Book and or a Memory Box?
- Does the individual have easy access to media files?
- Has the individual been asked if s/he would like a photograph of the LLO displayed
prominently in their room?
- Has the individual a means of visiting the grave of the LLO as desired?
- Has the individual a means of visiting a place of faith as desired?
- Has the individual been asked if s/he wishes to commemorate the date of the loss in
some way? Have they been involved in what will happen?
- Has the individual some way to indicate to all staff that s/he is upset/grieving even many
weeks or months after the event?
- Are all staff/significant others aware of the anniversary of a loss?
- Is the an establishment policy and procedure document available for staff to consult on aspects of loss?
- Have aspects of the LLO's will that concern the individual been explained? Have their wishes been honoured?
- Have any future transitions/changes been explained to the individual? Has s/he been prepared adequately to cope with them?
- Have the individual's concerns and questions on the topics of loss been addressed?
- Has the individual been assisted to write messages / cards, send e-mails, etc to others concerned with the loss?
- How is the individual's loss / reaction to the loss affecting peers? Have their needs also been met?
- Does the individual know to whom s/he can go to ask questions or just to talk?
- Does the individual have access to a place where s/he can be on his/her own?
- Does the individual have access to a Life Story Book and or a Memory Box?
- Does the individual have easy access to media files?
- Has the individual been asked if s/he would like a photograph of the LLO displayed
prominently in their room?
- Has the individual a means of visiting the grave of the LLO as desired?
- Has the individual a means of visiting a place of faith as desired?
- Has the individual been asked if s/he wishes to commemorate the date of the loss in
some way? Have they been involved in what will happen?
- Has the individual some way to indicate to all staff that s/he is upset/grieving even many
weeks or months after the event?
- Are all staff/significant others aware of the anniversary of a loss?
- Is the an establishment policy and procedure document available for staff to consult on aspects of loss?
- Have aspects of the LLO's will that concern the individual been explained? Have their wishes been honoured?
- Have any future transitions/changes been explained to the individual? Has s/he been prepared adequately to cope with them?
- Have the individual's concerns and questions on the topics of loss been addressed?
- Has the individual been assisted to write messages / cards, send e-mails, etc to others concerned with the loss?
- How is the individual's loss / reaction to the loss affecting peers? Have their needs also been met?

Further Reading, Bibliography and References
If you know of an additional source of information on this topic; a book or an article or other, please let Talksense know so that we may add it to this list. Thank you.
Arthur, A.R. (2003). The emotional lives of people with learning disability, British Journal of Learning Disabilities, volume 31, pp. 25-30
Bennett, D. (2003). Death and people with learning disabilities: Empowering carers. British Journal of Learning Disabilities, Volume 31, pp. 118 - 122.
Bihm, E. & Elliott, I. (1982). Conceptions of death in mentally retarded persons. Journal of Psychology, Volume 3, pp. 205-210.
Blackman, N. (Ed)(1999). Living with loss: Helping people with learning disabilities cope with loss and bereavement. Brighton: Pavilion
Blackman, N. (2003). Loss and learning disability. London: Worth Publishers.
Blackman, N. (2008). The development of an assessment tool for the bereavement needs of people with earning disabilities. British Journal of Learning Disability, Volume 36. pp. 165 – 170.
Bonell-Pascual, E., Huline-Dickens, S., Hollins, S., et al (1999), Bereavement and grief in adults with learning disabilities. A follow-up study. British Journal of Psychiatry, Volume 175, pp. 348 - 350.
Boss, P., & Yeats, J.R. (2014). Ambiguous loss: A complicated type of grief when loved ones disappear. Bereavement Care, Volume 33(2), pp. 63 – 69
Boulden, J., & Boulden, J. (1992). Saying Goodbye. Weaverville, CA: Boulden Publications
Bowlby, J. (1962). Pathological mourning and childhood mourning. Journal of the American Psychoanalytical Association, Volume II, pp. 500 - 541.
Bowlby, J. (1969). Attachment and loss: Volume I, attachment. New York: Basic Books.
Bowlby, J. (1973). Attachment and loss: Volume 2, separation. New York: Basic Books.
Bowlby, J. (1980). Attachment and loss: Volume 3, loss, sadness, and depression. New York: Basic Books.
Bowling, S. & Hollins S. (2003 ), Coping with Bereavement: the Dynamics of Intervention, In Davidson, P., Prasher, V., Janicki, M., (Eds). Mental Health, Intellectual Disabilities, and the Aging Process, Wiley
Braza, K. (1992). Memory Book for Bereaved Children. Salt Lake City, UT: Healing Resources
Brelstaff, K. (1984) Reactions to death: can the mentally handicapped grieve? Some experiences of those who did. Journal of National Association of Teachers of Mentally Handicapped People. May 1984, pp. 10 - 17
Brock, A. & Shute, R. (2001). Group coping skills program for parents of children with dyslexia and other learning disabilities, Australian Journal of Learning Disabilities, Volume 6 (4)
Brown, E. (1996) Religious Education for All. David Fulton Publishers
Brown, E. (1999). Loss, Change and Grief: An Educational Perspective, David Fulton Publishers
Brown, E. (2007). Supporting the Child and the Family in Paediatric Palliative Care, Jessica Kingsley Publishers
Brown M., Duff, H.,Karatzias, T., and Horsburgh, D. (2011). A review of the literature relating to psychological interventions and people with intellectual disabilities: Issues for research, policy, education and clinical practice, Journal of Intellectual Disabilities, March 2011, volume 15, (1), pp. 31-45
Çağan, O., & Ünsal, A. (2014). Depression and loneliness in disabled adults, 4th World Conference on Psychology, Counselling and Guidance, Procedia - Social and Behavioral Sciences, Volume 114, pp. 754 – 760
Carder, M. (1987). Journey into understanding mentally retarded people's experiences around death, The Journal Of Pastoral Care, Volume 41 (1), pp. 18 - 31
Cathcart, F. (1991). Bereavement and Mental Handicap, Bereavement Care, Volume 10 (1), pp. 9 - 11
Cathcart, F. (1994). Understanding Death and Dying: Your Feelings. British Institute of Learning Disabilities, Kidderminster.
Cathcart, F. (2000). Death and people with learning disabilities: Interventions to support clients and carers, British Journal of Clinical Psychology, Volume 34 (2), pp. 165 – 175
Clute, M.A. (2006). A Grounded Theory Study Of The Bereavement ExperienceFor Adults With Developmental Disabilities Following The Death Of A Parent Or Loved One: Perceptions Of Bereavement Counselors, 19th National Symposium on Doctoral Research in Social Work
Conboy-Hill, S. (1992) Grief, loss and people with learning disabilities. In Waitman A., & Conboy-Hill S. (eds). Psychotherapy and mental handicap. London, UK, Sage: pp. 150 – 70.
Cook, A.S., & Dworkin, D.S. (1992). Helping the Bereaved: Therapeutic Intervention for Children, Adolescents, and Adults. New York: basic Books
CYMRU Wales, (2010), Supporting people with a learning disability when they experience a loss or bereavement: A guide for carers, Aneurin Bevan Health Board, January 2010
Diets, B. (1988). Life After Loss: A Personal Guide Dealing with Death, Divorce, Job Chnage and Relocation. Tucson, Az: Fisher Books
Dell’Aquila, S. (1996). Developmental disability and grief: Assessing the impact of life events. Unpublished master’s thesis, Wilfred Luarier University, Waterloo, Ontario, Canada.
Deutsch, H. (1985). Grief counseling with the mentally retarded clients, Psychiatric Aspects of Mental Retardation Reviews, Vol. 4 (5), pp. 17 - 20
Dodd, P., Dowling, S., & Hollins S. (2005). A review of the emotional, psychiatric and behavioural responses to bereavement in people with intellectual disabilities, Journal of Intellectual Disability Research, Volume 49 (7), pp. 537–543, July
Dodd, P., McEvoy, J., Guerin, S., McGovern, E., Smith, E. & Hillery, J. (2005). Attitudes to Bereavement and Intellectual Disabilities in an Irish Context, Journal of Applied Research in Intellectual Disabilities, Volume 18 (3), September 2005 , pp. 237-243
Dodd, P., Guerin, S., McEvoy, J., Buckley, S., Tyrrell, J. & Hillery, J. (2008), A study of complicated grief symptoms in people with intellectual disabilities, Journal of Intellectual Disability Research, Volume 52 (5), pp. 415–425, May
Dodd, P., & Blackman, N. (2014). Complicated grief. In S. Read (Ed.), Supporting people with intellectual disabilities experiencing loss and bereavement: Theory and compassionate practice (pp. 56 – 67). London, Kingsley
Doka, K.J. (Ed.)(1996). Living with Grief After a Sudden Loss. Washington, DC: Hospice Foundation of America
Doka, K.J. (2002). Disenfranchised Grief: New Directions, Challenges, and Strategies for Practice. Research Press, Champaign IL.
Doka, K.J. (2010). Grief, multiple loss and dementia. Bereavement Care, Volume 29(3), pp.15 – 20.
Dougy Centre (1990). Waving Goodbye: An Activities Manual for Children in Grief. Portland, OR: Dougy Centre
Dowling, S., Hubert, J., White, S., and Hollins, S. (2006). Bereaved adults with intellectual disabilities: a combined randomized controlled trial and qualitative study of two community-based interventions, Journal of Intellectual Disability Research, Volume 50 (4), pp. 277–287, April 2006
Duff, R., La Rocca, J., Lizzet, A., Martin, P., Pearce, L., Williams, M., & Peck, C. (1981). A comparison of the fears of mildly retarded adults with children of their mental age and chronological age matched controls. Journal of Behaviour Therapy and Experimental Psychiatry, Volume 12, pp. 121 – 124.
Elliot, D. (1995). Helping people with learning disabilities to handle grief, Nursing Times, Volume 91 (43), pp. 27-29.
Emerson, P. (1977). Covert grief reaction in mentally retarded clients, Mental Retardation, Volume 15 (6), pp. 46 - 47
Flower, D. (1983) Susan's Story. London: The Royal Society for Mentally Handicapped Chidren and Adults
French, J. & Kuczaj, E. (1992). Working Through Loss and Change With People With Learning Difficulties, Journal of the British Institute of Mental Handicap (APEX), Volume 20 (3), pp.108–111, September 1992
Gault, J. (2003). Bereavement: helping a patient with a learning disability to cope, Nursing Times, Volume 99 (1), pp. 26
Gilrane-McGarry, U. and Taggart, L. (2007). An exploration of the support received by people with intellectual disabilities who have been bereaved, Journal of Research in Nursing, March 2007, Volume 12 (2), pp. 129-144
Goldberg, D., Magrill, L., Hale, J., Damaskinidou, K., Paul, J. & Tham, S. (1995). Protection and loss: working with learning-disabled adults and their families, Journal of Family Therapy, Volume 17 (3), pp. 263–280, August
Goldman, L. (2005). Children also grieve: Talking About Death and Healing, Jessica Kingsley Publishers
Gullone, E., Cummins, R.A., & King, N.J. (1996). Self-reported fears: A comparison study of youths with and without an intellectual disability. Journal of Intellectual Disability Research, Volume 40, pp. 227 – 240.
Harper, D.C., Wadsworth, J., & Fowler, C. (1991). Griefand loss with older adults with mental retardation: A pilot study of current status and needs. Paper presented at the SIG/Aging Conference, October, Lexington, KY.
Harper, D.C. & Wadsworth, J.S. (1993). Grief in adults with mental retardation, Research in Developmental Disabilities, Volume 14 (4), pp. 313 - 330
Hastings, R.P., Hatton, C., Taylor, J.L., & Maddison, C. (2004). Life events and psychiatric symptoms in adults with intellectual disabilities, Journal of Intellectual Disability Research, Volume 48 (1), pp. 42–46, January 2004
Heath, M.A., & Cole, B.V. (2012). Strengthening classroom emotional support for children following a family member’s death. School Psychology International, Volume 33(3), pp. 243 - 262
Hedger, C.J., & Dyer-Smith, M.J. (1993). Death education for older adults with developmental disabilities; A life cycle therapeutic recreation approach. Activities, Adaptation, and Aging. Volume 18 (1), pp. 29 - 36
Heegaard, M. (1988). When Someone Very Special Dies: Children can Learn to Cope with Grief. Minneapolis, MN: Woodland Press.
Heegaard, M. (1992). The Drawing Out Feelings Series. USA: Woodland Press.
Hedger, C.J. & Dyer Smith, M.J. (1993). Death education for older adults with developmental disabilities: A life cycle therapeutic reaction approach, Activiities, Adaptation and Aging, Volume 18 (1), pp. 29 - 36
Hill, S. & & Johnson C. (2012). A Grief Group Therapy Model for Adults with Intellectual Disabilities, The Baddour Center, Senatobia, MS. A PowerPoint presentation
Hobson R.J., Outson, J., & Lee, A. (1989) Recognition of emotion by mentally retarded adolescents and young adults. American Journal of Mental Retardation, Volume 93. pp. 434 – 443.
Hogg. J., Juhlberg. K., & Lambe, L. (2006). Development and mortality over a 10-year period among people with profound intellectual and multiple disabilities. Journal of Applied Research in Intellectual Disabilities. Volume 19 (3), pp. 262 - 262.
Holland, J. (2003). Supporting schools with loss: ‘Lost for Words’, in Hull. British Journal of Special Education, 30 (2), pp76-78.
Hollins, S. (1987), How do people with Mental retardation cope with loss? Paper presented at the ICPS conference, Sydney Sussex College, Cambridge, 23rd - 27th March, 1987
Hollins, S. (1995), Managing Grief Better: People With Intellectual Disabilities, The Habilitative Mental Healthcare Newsletter, May/June 1995, Volume 14, No. 3.
Hollins, S., Dowling. S., & Blackman, N. (1995) When Somebody Dies. Books Beyond Words, London.
Hollins, S. and Esterhuyzen, A. (1997). Bereavement and grief in adults with learning disabilities. British Journal of Psychiatry, Volume 170, pp. 497-501.
Hollins, S. and Sireling, L. (1991). When Dad Died: working through loss with people who have learning disabilities or with children. Windsor: NFER-Nelson.
Hollins, S. and Sinason, V. (2000). Psychotherapy, learning disabilities and trauma: new perspectives, The British Journal of Psychiatry, Volume 176, pp. 32-36
Holmes, T. (2012). Forgotten Grief: Helping People with Developmental Disabilities Manage Personal Loss, Alberta Counsellor, Volume 32(1), pp.3 - 26
Howell, M. C. (ed.)(1989), Serving the underserved: caring for people who and both old and mentally retarded, Boston: Exceptional Parent Press
James, I. A. (1995). Helping People with Learning Disability to Cope with Bereavement. British Journal of Learning Disabilities, 23, pp
74-78.
Jewett, C. (1982). Helping Children Cope with Separation and Loss. Havard, MA: The Havard Common Press
Kauffman, J. (1994). Mourning and mental retardation, Death Studies, Volume 18, pp 257 - 271
Kauffman, J. (2005). Guidebook on helping persons with mental retardation mourn. Amityville, NY: Baywood Publishing Company, Inc.
Kauffman, J., & Gaventa, B. (2008). Good grief does not depend on I.Q., ARC newsletter, Summer 2008
Kennedy, E. (2000). The impact of cognitive development and socialization factors on the concept of death among adults with mental retardation. Unpublished doctoral dissertation. Akron, Ohio: University of Akron.
King's Fund (1980). The right to grieve. Leaflet
King's Fund (1981). Bereavement and mentally handicapped people.
Kitching, N. (1987), Helping people with mental handicaps cope with bereavement: A case study with discussion , Journal of the British Institute of Mental Handicap (APEX), Volume 15 (2), pp. 60–63, June 1987
Kloeppel, D.A. & Hollins, S. (1989). Double handicap: mental retardation and death in the family, Death Studies, Volume 13 (1), pp. 31 - 38
Kuekes, J. (1996). Parents’ perception of their adult developmentally disabled children’s understanding of death. Unpublished doctoral dissertation, California School of Professional Psychology, Los Angeles, California
Levelle, E. (1997). Conceptual knowledge of a normative life event: The impact of intellectual ability, age, experience and attachment on the concept of death. Unpublished doctoral dissertation, West Virginia University, Morgantown, West Virginia.
Lindemann, E. (1944). Symptomatology and mangement of acute grief. American Journal of Psychiatry, Volume 101, pp. 141 - 148
Lipe-Goodson, P. S. and Goebel, B. L. (1983). Perception of age and death in mentally retarded adults. Mental Retardation, Volume 21, pp. 68 - 75.
Luchterhand, C. (1998). Mental retardation and grief following a death loss, www.thearc.org
Luchterhand, C. & Murphy, N. (1998). Helping adults with mental retardation grieve a death loss, Bristol PA, Accelerated Development
Lyons, C.A. (2000). Studying grief in adults with learning disabilities, The British Journal of Psychiatry, Volume 176, pp. 297-298
MacHale, R. & Carey, S. (2002). An investigation of the effects of bereavement on mental health and challenging behaviour in adults with learning disability, British Journal of Learning Disabilities, Volume 30 (3), pp. 113–117
MacHale, R., McEvoy, J. & Tierney, E. (2009). Caregiver Perceptions of the Understanding of Death and Need for Bereavement Support in Adults with Intellectual Disabilities, Journal of Applied Research in Intellectual Disabilities, Volume 22 (6), November 2009 , pp. 574-581
Mappin, R., & Hanlon, D. (2005). Description and evaluation of a bereavement group for people with learning disabilities. British Journal of Learning Disability, Volume 33. pp. 106 – 112.
Markell, M. & Hoover, J. (2010). Children with developmental disabilities, death and grief, IN - Corr, C. & Balk, D. (Eds.) Children's Encounters With Death, Bereavement, and Coping, Chapter 20, Springer Publishing
Marquardt, H.A. (1989), Funeral and memorial services, In Howell, M. C. (ed.), Serving the underserved: caring for people who and both old and mentally retarded, pp. 346 - 348. Boston: Exceptional Parent Press
McCarthy, J. (2001). Post-traumatic stress disorder in people with learning disability, Advances in Psychiatric Treatment, Volume 7: pp. 163-169
McDaniel, B.A. (1989). A group work experience with mentally retarded adults on the issues of death and dying, Journal of Gerontological Social Work, Volume 13 (3/4), pp. 187 - 191
McEvoy, J., (1989) Investingating the concept of death in adults who are mentally handicapped, The British Journal of Mental Subnormality, Volume 35, part 2, No. 69
McEvoy, J., Reid, Y., and Guerin, S. (2002). Emotion recognition and concept of death in people with learning disabilities, The British Journal of Developmental Disabilities, Volume 48 (95), pp. 83-89
McEvoy, J. & Smith, E. (2005). Families Perceptions of the Grieving Process and Concept of Death in Individuals with Intellectual Disabilities, The British Journal of Development Disabilities, Volume 51 (100), January 2005 , pp. 17-25
McEvoy, J., Guerin, S., Dodd, P. & Hillery, J. (2010). Supporting Adults with an Intellectual Disability During Experiences of Loss and Bereavement: Staff Views, Experiences and Suggestions for Training, Journal of Applied Research in Intellectual Disabilities, Volume 23 (6), November 2010 , pp. 585-596
McEvoy, J., MacHale, R., & Tierney, E. (2012). Concept of death and perceptions of bereavement in adults with intellectual disabilities. Journal of Intellectual Disability Research, Volume 56(2), pp. 191 – 203.
McLoughlin, I.J.. (1986), Bereavement in the Mentally Handicapped, British Journal Of Hospital Medicine, 36 (4), pp 256 - 260
McLaughlin, I.J., & Bhate, M.S. (1987). A case of affective psychosis following bereavement in a mentally handicapped woman. British Journal of Psychiatry, Volume 151, pp. 552 - 554.
Melvin, D., & Lukeman, D. (2000). Bereavement: A Framework for those Working with Children, Clinical Child Psychology and Psychiatry, Volume 5(4), pp. 521 - 539
Moise, L.E. (1978), In sickness and death, Mental Retardation, Volume 16 (6), pp. 397 - 398
Murray, G.C., McKenzie, K., and Quigley, A. (2000). An Examination of the Knowledge and Understanding of Health and Social Care Staff about the Grieving Process in Individuals with a Learning Disability, Journal of Intellectual Disabilities, March 2000, Volume 4 (1), pp. 77 - 90
Murray Parkes, C. (1965), Bereavement and mental illness, British Journal of Medical Psychology, Volume 38 (1), pp. 13–26, March 1965
Murray Parkes, C. (1998), Facing loss, British Medical Journal. 1998 May 16; Volume 316(7143): pp. 1521–1524.
Myreddi V., & Narayan, J. (1993), The concept of death among people with mental handicap, International Journal of Rehabilitation Research: December 1993 - Volume 16(4) , pp 328-330
Oswin, M. (1981). Bereavement and Mentally Handicapped People, London: King's Fund Centre.
Oswin, M. (1882). Nobody for me to look after, Parents' Voice, March 1982, 10
Oswin, M. ( 1985). Bereavement, In Mental Handicap: a multi-disciplinary approach. Chapter 17. Eds. Craft, M., Bicknell, J., & Hollins, S.
London: Bailliere Tindall
Oswin, M. (1989). Bereavement and mentally handicapped people. In T. Philpot (Ed.), Last things: Social work with the dying and bereaved (pp. 92 - 105). Wellington, Surrey, Great Britian: Community Care.
Oswin, M. (1991). Am I Allowed to Cry? A Study of Bereavement amongst people who have Learning Disabilities. London: Human
Horizons Series. Souvenir Press.
Phillip, M., Lambe, L., & Hogg, J. (2005). The Well Being Workshop: Recognising the Emotional and Mental Well-being of People with Profound and Multiple Learning Disabilities. Foundation for People with Learning Disabilities, London.
Pima Council on Developmental Disabilities (1994). More years more tears: How grief and loss experiences affect adults with mental retardation. Video Tape. Tuscon Arizona
Raji, O., Hollins, S., & Drinnan, A. (2003) How far are people with learning disabilities involved in funeral rites? British Journal of Learning Disabilities, Volume 31, pp. 42-45.
Rando, T.A. (1993). Treatment of Complicated Mourning. Champaign, IL: Research Press
Read, S. (1998). Breaking bad news to people with learning disability. British Journal of Nursing, Volume 7 (2), pp. 86-91.
Read, S. (1999). Bereavement and people with learning disabilities. London: E-Map healthcare Ltd., Nursing Times Monograph No. 30.
Read, S. (1999). Creative ways of working when exploring the bereavement counselling process. IN: N. Blackman (ed) (1999). Living with loss: Helping people with learning disabilities cope with loss and bereavement (pp. 9-13). Brighton: Pavilion Publ.
Read, S. (2000). Bereavement and people with learning disabilities. Nursing and Residential Care, Volume 2 (50), pp. 230-234.
Read, S. (2001). A Year in the Life of a Bereavement Counselling and Support Service for People with Learning Disabilities, Journal of Intellectual Disabilities, March 2001, Volume 5 (1), pp.19-33
Read, S. (2003). Bereavement and loss. In: A. Markwick & A.Parrish (2003). Learning disabilities: Themes and perspectives. Edinburgh: Butterworth Hinemann.
Read, S. & Elliot, D. (2003). Death and learning disability: A vulnerability perspective. Journal of Adult Protection, Volume 5 (1), pp. 5-14.
Read, S. & Papakosta-Harvey, V. (2004). Using workshops on loss for adults with learning disabilities: A second study. Journal of Learning Disabilities, 8 (2), pp. 191 - 208.
Read, S., & Bowler, C. (2007). Life story work and bereavement: Shared reflections on its usefulness. Learning Disability Practice, Volume 10(4), pp.10 – 15.
Read, S., & Elliott, D. (2007). Exploring a continuum of support for bereaved people with intellectual disabilities. Journal of Learning Disabilities, Volume 11(2), pp. 167 – 181.
Read, S. (Ed.) (2014). Supporting people with intellectual disabilities experiencing loss and bereavement: Theory and compassionate practice. London, Kingsley
Reilly, D., Hastings, R., Vaughan, F., & Huws, J.C. (2008) Parental bereavement and the loss of a child with intellectual disabilities: a review of the literature. Intellectual and Developmental Disabilities. Volume 46 (1), pp. 27 - 43.
Reynolds, S., Guerin, S., McEvoy, J. & Dodd, P. (2008). Evaluation of a Bereavement Training Program for Staff in an Intellectual Disabilities Service, Journal of Policy and Practice in Intellectual Disabilities, Volume 5 (1), March 2008 , pp. 1-5
Riches, V. (2008). Unrecognised and Unsupported: Grief among People with Intellectual Disability, Grief Matters: The Australian Journal of Grief and Bereavement, Volume 11 (2), pp. 48 - 53
Rojahn, J., Lederer, M., & Tasse, M.J. (1995) Facial emotion recognition by persons with mental retardation: a review of the experimental literature. Research in Developmental Disability, Volume 16, pp. 393 – 414.
Rosenblatt, P.C. (1988). Grief: The social context of private feelings. Journal of Social issues, Volume 44(3), pp. 67 - 78
Rosenblatt, P.C., & Elde, C. (1990). Shared reminiscence about a deceased parent: Implications for grief education and grief counseling. Family Relations, Voume 39, pp. 206 - 210
Rothenberg, E.D. (1994). Bereavement intervention with vulnerable populations: A case report on group work with the developmentally disabled, Social Work with Groups, Volume 17 (3), pp. 61 - 75
Ryan, K., Guerin, S., Dodd, P., & McEvoy, J. (2011). End-of-life care for people with intellectual disabilities: Paid carer perspectives. Journal of Applied Research in Intellectual Disabilities, Volume 24, pp. 199 – 207.
Slaughter, V., & Griffiths, M. (2007). Death understanding and fear of death in young children. Clinical Child Psychology and Psychiatry, Volume 12, pp. 525 – 535
Smith, Debra et al. (2000). Life After Death: Preparing People with Intellectual Disability for Bereavement and Loss. Fyshwick, ACT : Australian Institute on Intellectual Disability, A resource guide for families and caregivers.
Sormanti, M. & Ballan, M. (2011). Strengthening grief support for children with developmental disabilities, School Psychology International, April 2011, Volume 32 (2), pp. 179-193
Stancliffe, R.J., Wiese, M.Y., Read, S., Jeltes, G., & Clayton, J.M. (2016). Knowing, planning for and fearing death: Do adults with intellectual disability and disability staff differ? Research in Developmental Disabilities, Volume 49–50, pp. 47 – 59
Staudacher, C. (1991). Men and Grief: A guide for men surviving the death of a loved one - A resource for caregivers and mental health professionals. Oakland, CA: New Harbinger Publications
St. Thomas, B., & Johnson, P. (2007). Empowering Children through Art and Expression: Culturally Sensitive Ways of Healing Trauma and Grief, Jessica Kingsley
Stickney, D. (2004). Water Bugs and Dragonflies: Explaining Death to Young Children, Pilgrim Press (Revised Edition)
Stoddart, K. and McDonnell, J. (1999). Addressing grief and loss in adults with developmental disabilities. Journal of Developmental Disabilities, Volume 6, pp. 51-65.
Stoddart, K., Burke, L., & Temple, V. (2002). Outcome Evaluation of Bereavement Groups for Adults with Intellectual Disabilities, Journal of Applied Research in Intellectual Disabilities, Volume 15 (1), pp. 28–35, March
Strachan, J. (1981) Reaction to bereavement: a study of a group of mentally handicapped hospital residents. Apex, 9(1), pp 20 - 21
Stroebe, M.S., Storebe, W. & Hansson, R.O. (1993). Handbook of Bereavement. Cambridge: Cambridge University Press.
Strohmer, D.C. & Prout, H.T. (eds) (1994). Counselling and psychotherapy for persons with mental retardation and borderline intelligence. Vermont: Clinical Psychology Publishing Co.
Summers, S.J. (2003) Psychological intervention for people with learning disabilities who have experienced bereavement: a case study illustration. British Journal of Learning Disability, Volume 31, pp. 37 – 41.
Tatelbaum, J. (1980). The Courage to Grieve. New York: Harper and Row
Tatelbaum, J. (1989). You Don't Have to Suffer: A handbook for Moving Beyond Life's Crises. New York: Harper and Row
Todd, S. & Shearn, J. (1997). Family Dilemmas and Secrets: Parents' disclosure of information to their adult offspring with learning disabilities, Disability & Society, Volume 12 (3)
Todd, S. (2007). Silenced grief: living with the death of a child with learning disabilities. Journal of Intellectual Disability Research. Volume 51 (8), pp. 637 - 648.
Todd, S., Bernal, J., & Forrester-Jones, R. (2013). Editorial: Death, dying and intellectual disability research. Journal of Applied Research in Intellectual Disabilities, Volume 26(3), pp. 183 – 185
Tuffrey-Wijne, I., & McEnhill, L. (2008). Communication difficulties and intellectual disability in end-of-life care. International Journal of Palliative Nursing, Volume 14, pp. 189 – 195.
Tuffrey-Wijne, I., Giatras, N., Butler, G., Cresswell, A., Manners, P., & Bernal, J. (2013). Developing guidelines for disclosure or non-disclosure of bad news around life-limiting illness and death to people with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, Volume 26, pp. 231 – 242.
Turner, J.C., & Graffam, J.H.(1987),Deceased loved ones in the dreams of mentally retarded adults, American Journal of Mental Deficiency, Volume 92, pp. 282- 289
Turner, M. (2006). Talking with children and young people about death and dying. Second Edition. Jessica Kingsley Publishers
Van Dyke, L. (2003). Lessons in grief & death: Supporting people with developmental disabilities in the healing process. Homewood, Ill: High Tide Press.
Vredeveld, R. (1985). The crisis of death: Dimensions of pastoral care in the death of a person with mental retardation. Paper presented at the Annual Convention of the American Association for Mental Deficiency, May, Philadelphia, PA.
Wadsworth, J.S. & Harper, D.C. (1991). Grief and Bereavement in mantal retardation: A need for new understanding. Death Studies, Volume 15, pp. 281 - 292
Wiese, M.Y., Stancliffe, R.J., Balandin, S., Howarth, G., & Dew, A. (2012). End-of-life care and dying: Issues raised by staff supporting older people with intellectual disability in community living services. Journal of Applied Research in Intellectual Disabilities, Volume 25(6), pp. 571 – 583.
Wiese, M.Y., Dew, A., Stancliffe, R. J., Howarth, G., & Balandin, S. (2013a). ‘‘If and when?’’: The beliefs and experiences of community living staff in supporting older people with intellectual disability to know about dying. Journal of Intellectual Disability Research, Volume 57(10), pp. 980 – 992.
Wiese, M.Y., Stancliffe, R.J., Dew, A., Balandin, S., & Howarth, G. (2013b). What is talked about? Community living staff experiences of talking with older people with intellectual disability about dying and death. Journal of Intellectual Disability Research, Volume 58(7), pp. 679 – 690.
Wiese, M.Y. (2014). End-of-life care of people with intellectual disabilities in community living services. Sydney: The University of Sydney (Unpublished PhD Thesis).
Wiese, M.Y., Stancliffe, R.J., Clayton, J., Read, S., & Jeltes, G. (2014). End-of-life planning scale. Sydney: Centre for Disability Research and Policy, The University of Sydney.
Wiese, M., Stancliffe, R.J., Read, S., Jeltes, G., & Clayton, J. (2015). Learning about dying, death and end-of-life planning: Current issues informing future actions. Journal of Intellectual & Developmental Disability, Volume 40(2), pp. 230 – 235
Worden, J.W. (1983). Grief Counselling and Grief Therapy. London: Tavistock.
www.bereavementanddisability.org.uk
Yanok, J. & Addis Beifus, J. (1993). Communicating about loss and mourning: Death education for individuals with mental retardation, Mental Retardation, Volume 31 (3), pp. 144 - 147
If you are aware of other sources of information on this topic please let Talksense know. There is a form provided below that can be used for this purpose.
Tell Talksense your story
Talksense would love to hear your experiences of this topic (good or bad). Please let us know if it is OK to share such information or if it's OK to share but you would like to remain annonymous (for example). Talksense will always respect your wishes. You may use the contact from below or e-mail ([email protected]) directly.
Talksense would like to hear your thoughts and opinions on this page even if they disagree with any of the suggestions made. Again, please indicate if you will allow your opinions to be published and if you wish to remaiin annonymous.
Talksense would like to hear your thoughts and opinions on this page even if they disagree with any of the suggestions made. Again, please indicate if you will allow your opinions to be published and if you wish to remaiin annonymous.
Return to Home Page
Click on the Left Arrow below to retrun to the choice page or hit the Up Arrow to return to the top of this page.
 Return To Home Page |
 Return to Top of Page |
